
Influence of Physical Activity during Pregnancy on Birth Weight: Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Population
2.3. Intervention (Exposure)
2.4. Comparison
3. Outcome
4. Data Sources
- English: (physical activity OR exercise OR training OR physical exercise OR fitness OR (strength training) OR physical intervention OR Pilates OR Yoga OR strengthening OR aerobic OR resistance training OR pelvic floor muscle training) AND (pregnancy OR maternal OR antenatal OR pregnant AND (birth weight OR macrosomia OR low birth weight OR large gestational age OR small gestational age) AND (randomized clinical trial OR randomized controlled trial OR RCT).
- Spanish: (actividad física O ejercicio O entrenamiento O ejercicio físico O fitness O entrenamiento de fuerza O intervención de actividad física O Pilates O Yoga O fortalecimiento O aeróbico O entrenamiento de resistencia O fortalecimiento del suelo pélvico) Y (embarazo O materno O antenatal O embarazada Y peso de nacimiento O macrosomía O bajo peso al nacer O gran edad gestacional O pequeña edad gestacional) Y (ensayo clínico aleatorizado O ensayo controlado aleatorizado O ECA).
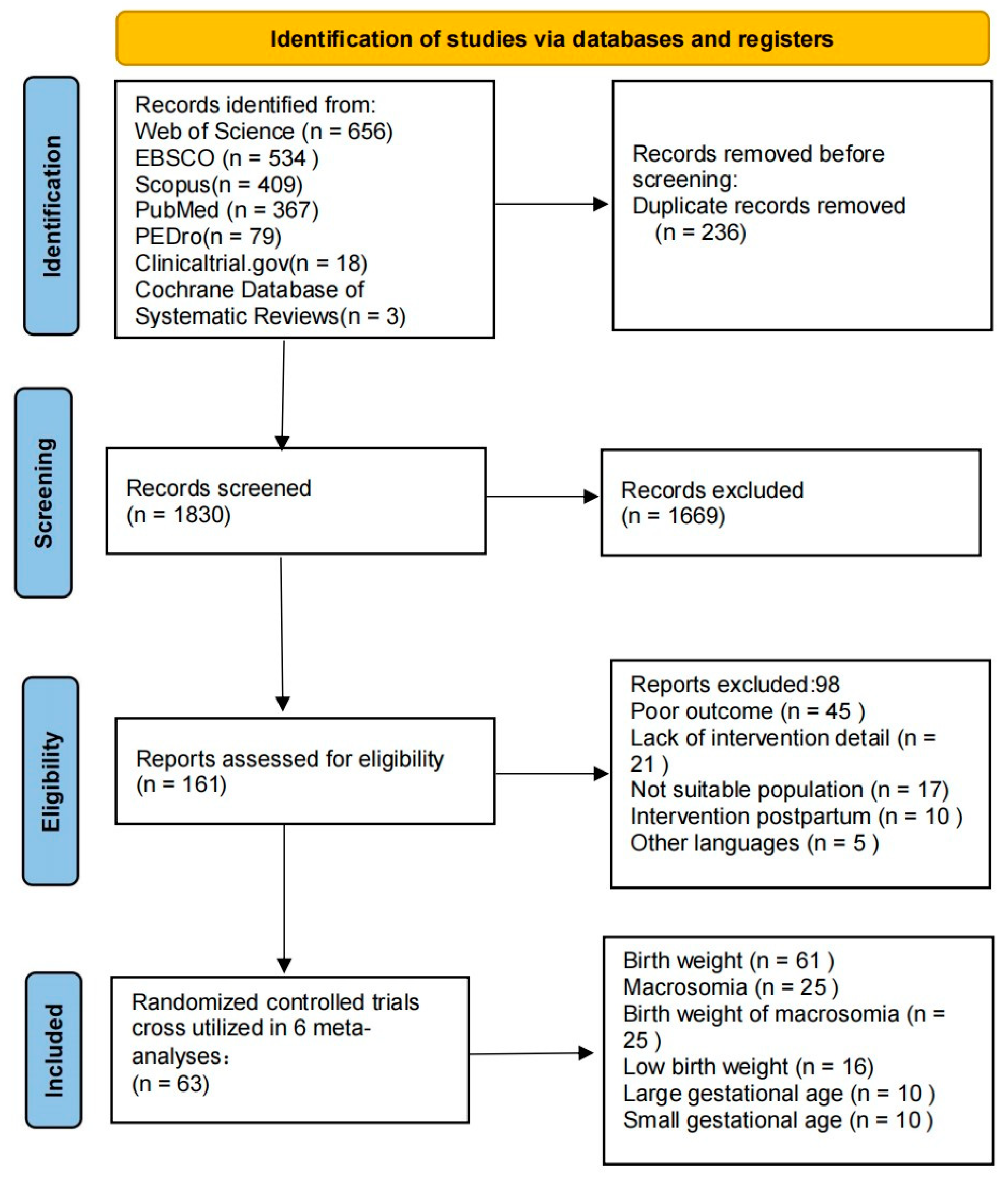
5. Study Selection and Data Extraction
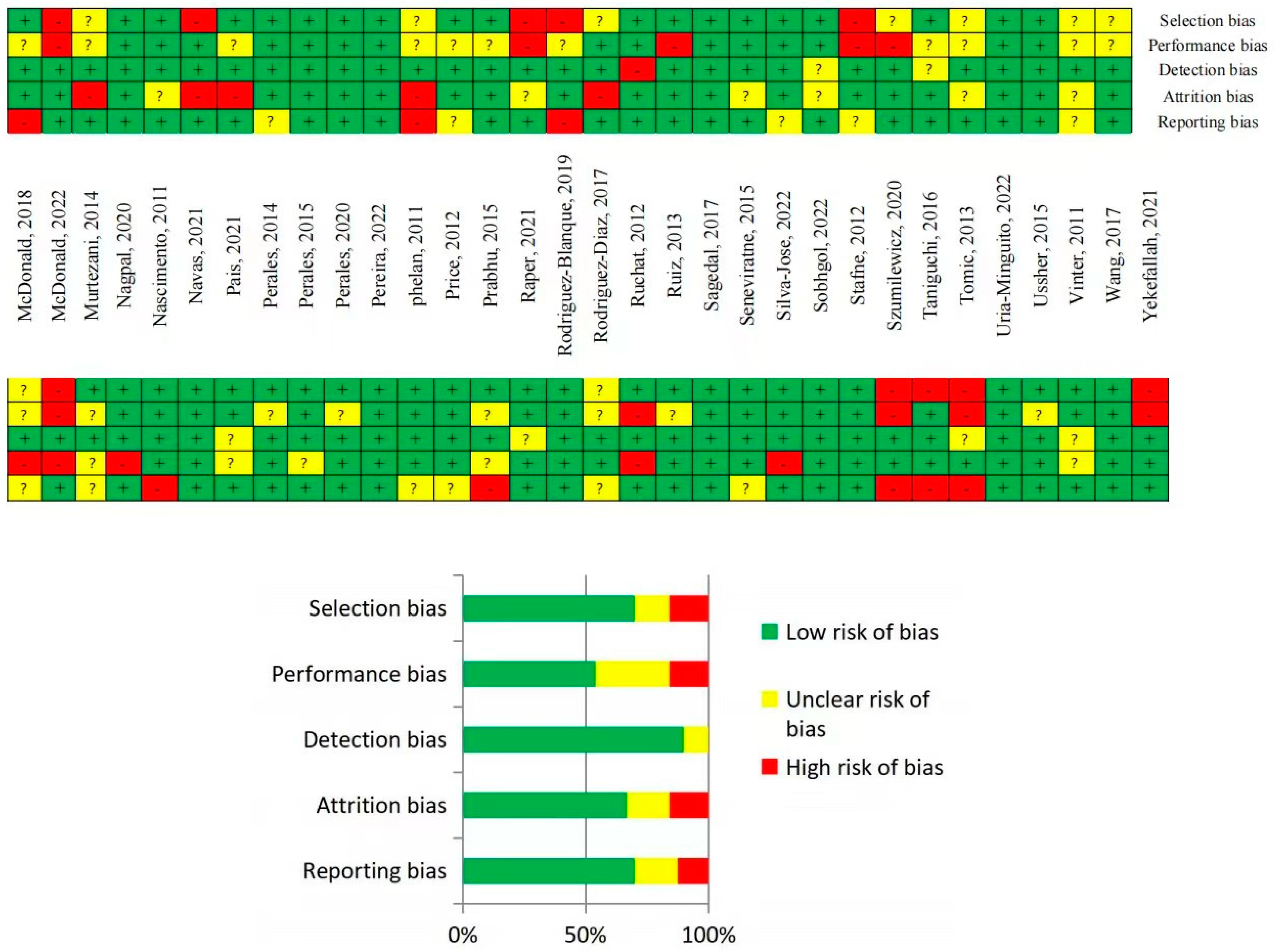
6. Quality of Evidence and Risk of Bias Assessments
7. Statistical Analysis
8. Results
8.1. Study Characteristics
8.2. Risk of Bias Assessment
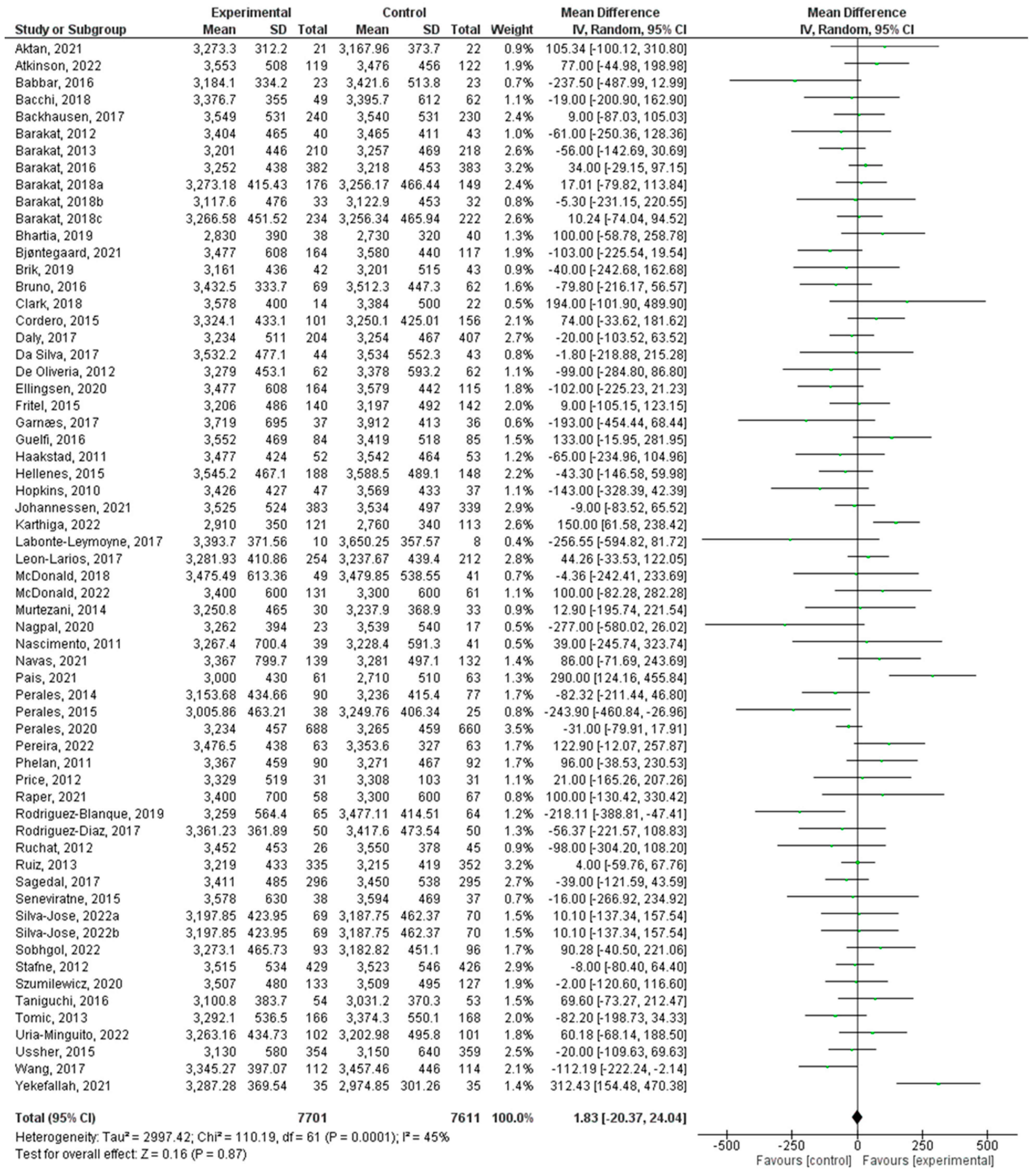
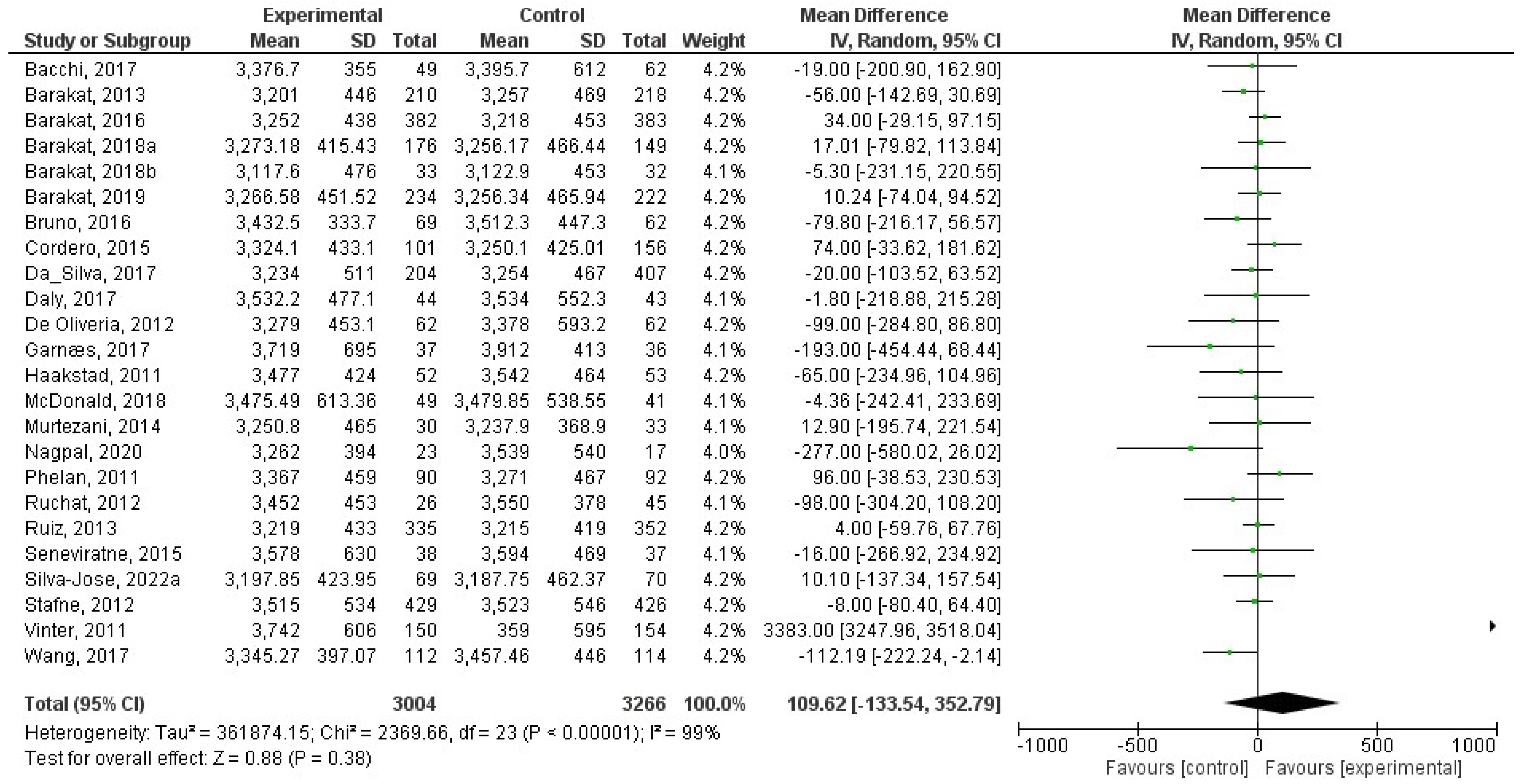
8.3. Effect of Physical Activity during Pregnancy on Birth weight
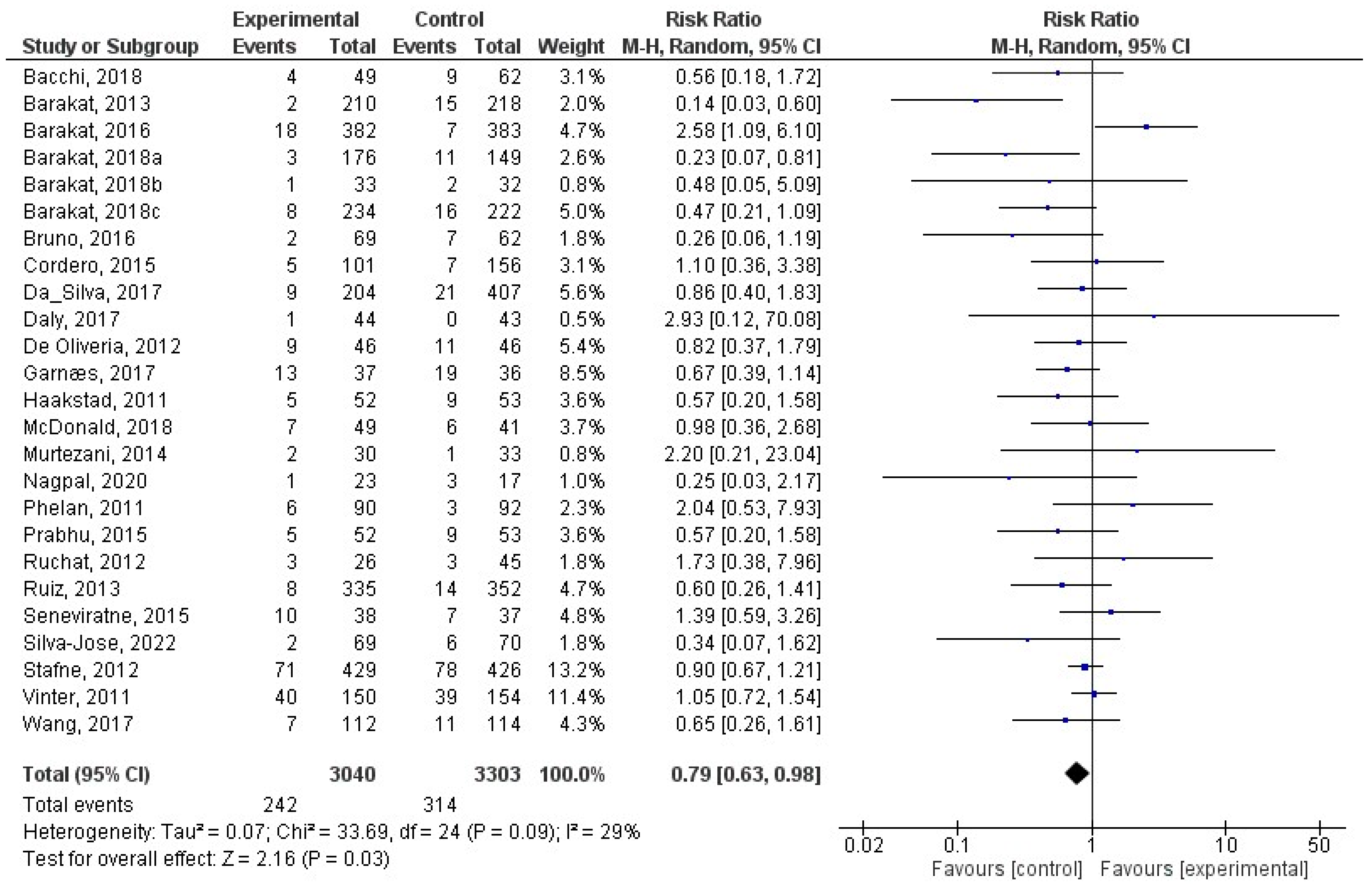
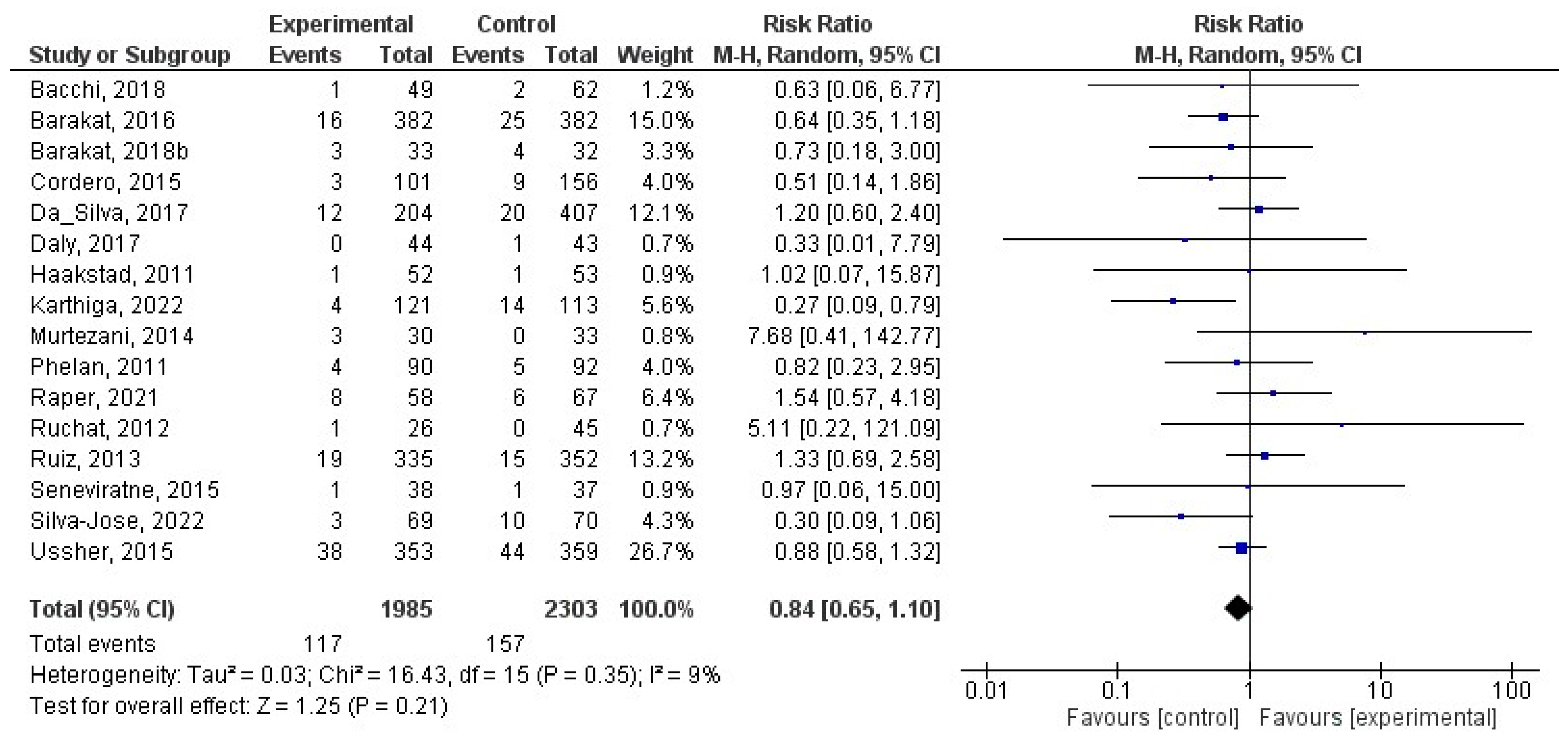
8.4. Effect of Physical Activity during Pregnancy on Macrosomia
8.5. Effect of Physical Activity during Pregnancy on Low Birth Weight
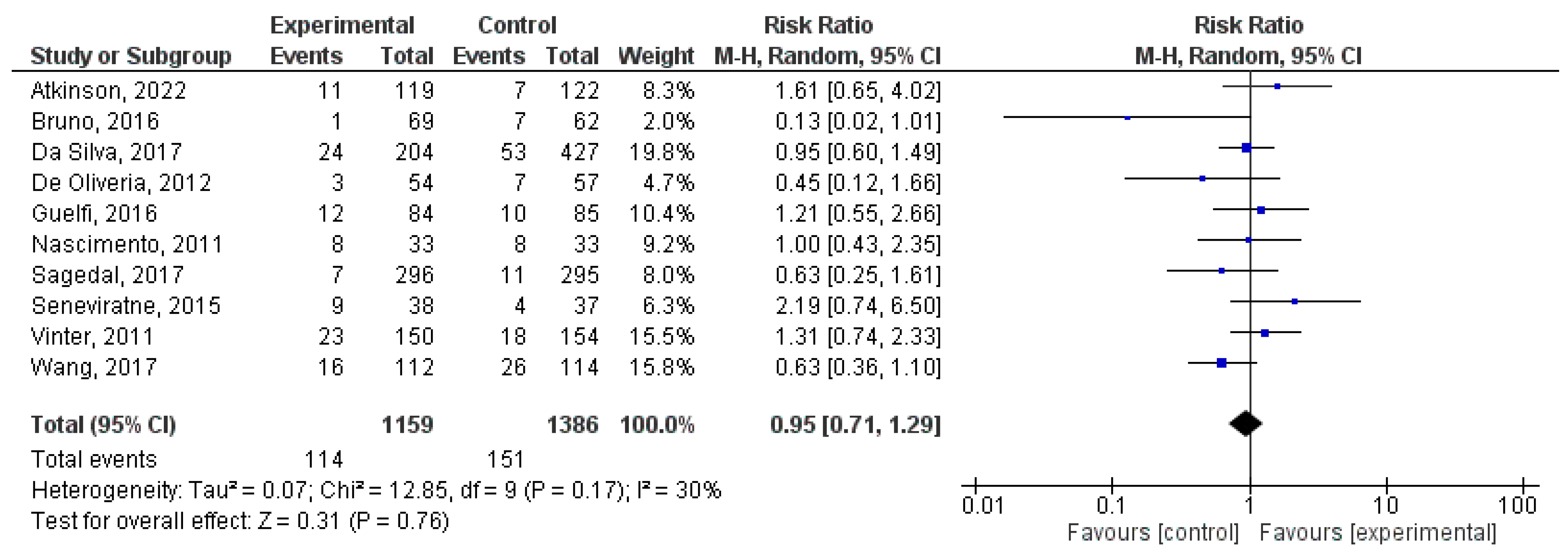
8.6. Effect of Physical Activity during Pregnancy on Large for Gestational Age
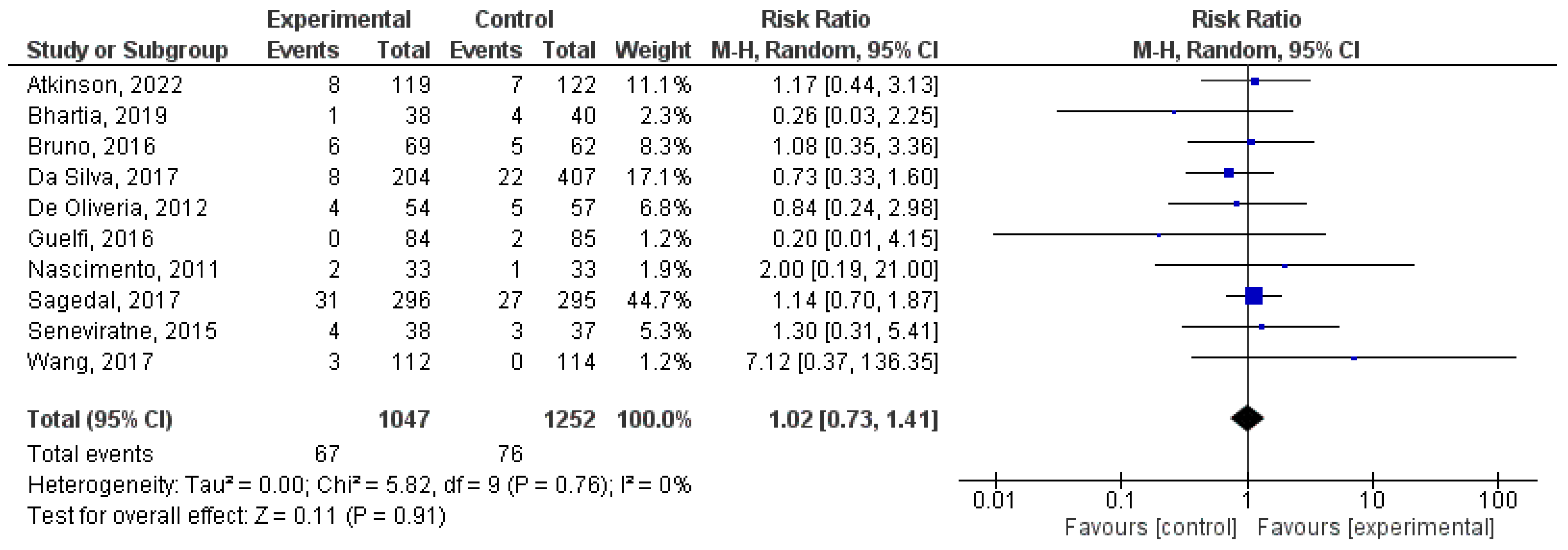
8.7. Effect of Physical Activity during Pregnancy on Small for Gestational Age
9. Discussion
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chiavaroli, V.; Derraik, J.G.; Hofman, P.L.; Cutfield, W.S. Born large for gestational age: Bigger is not always better. J. Pediatr. 2016, 170, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Sebayang, S.K.; Dibley, M.J.; Kelly, P.J.; Shankar, A.V.; Shankar, A.H.; Group, S.S. Determinants of low birthweight, small-for-gestational-age and preterm birth in Lombok, Indonesia: Analyses of the birthweight cohort of the SUMMIT trial. Trop. Med. Int. Health 2012, 17, 938–950. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, R.P.; Naik, G.; Choudhary, T.S.; Chowdhury, R.; Taneja, S.; Bhandari, N.; Martines, J.C.; Bahl, R.; Bhan, M.K. Cognitive and motor outcomes in children born low birth weight: A systematic review and meta-analysis of studies from South Asia. BMC Pediatr. 2019, 19, 35. [Google Scholar] [CrossRef]
- Stålnacke, S.R.; Tessma, M.; Böhm, B.; Herlenius, E. Cognitive development trajectories in preterm children with very low birth weight longitudinally followed until 11 years of age. Front. Physiol. 2019, 10, 307. [Google Scholar] [CrossRef]
- Zamorski, M.A.; Biggs, W.S. Management of suspected fetal macrosomia. Am. Fam. Physician 2001, 63, 302. [Google Scholar]
- Boulet, S.L.; Alexander, G.R.; Salihu, H.M.; Pass, M. Macrosomic births in the United States: Determinants, outcomes, and proposed grades of risk. Am. J. Obstet. Gynecol. 2003, 188, 1372–1378. [Google Scholar] [CrossRef] [PubMed]
- Boulet, S.L.; Salihu, H.M.; Alexander, G.R. Mode of delivery and the survival of macrosomic infants in the United States, 1995–1999. Birth 2006, 33, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Decker, A.; Platt, R.W.; Kramer, M.S. How big is too big? The perinatal consequences of fetal macrosomia. Am. J. Obstet. Gynecol. 2008, 198, 517.e1–517.e6. [Google Scholar] [CrossRef]
- Fuchs, F.; Bouyer, J.; Rozenberg, P.; Senat, M.-V. Adverse maternal outcomes associated with fetal macrosomia: What are the risk factors beyond birthweight? BMC Pregnancy Childbirth 2013, 13, 90. [Google Scholar] [CrossRef]
- Tomić, V.; Bošnjak, K.; Petrov, B.; Đikić, M.; Knežević, D. Macrosomic births at Mostar Clinical Hospital: A 2-year review. Bosn. J. Basic Med. Sci. 2007, 7, 271. [Google Scholar] [CrossRef][Green Version]
- Nagpal, T.S.; Mottola, M.F. Physical activity throughout pregnancy is key to preventing chronic disease. Reproduction 2020, 160, R111. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.-M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; Gray, C.E.; Garcia, A.J. Impact of prenatal exercise on neonatal and childhood outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef]
- Moreno-Fernandez, J.; Ochoa, J.J.; Lopez-Frias, M.; Diaz-Castro, J. Impact of early nutrition, physical activity and sleep on the fetal programming of disease in the pregnancy: A narrative review. Nutrients 2020, 12, 3900. [Google Scholar] [CrossRef]
- Everest, C.; da Silva, D.F.; Puranda, J.; Souza, S.C.; Goudreau, A.D.; Nagpal, T.S.; Edwards, C.M.; Gupta, R.; Adamo, K.B. Physical Activity and Weight Gain Throughout Pregnancy Are Associated With Umbilical Cord Markers. J. Obstet. Gynaecol. Can. 2022, 44, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Gascoigne, E.L.; Webster, C.M.; Honart, A.W.; Wang, P.; Smith-Ryan, A.; Manuck, T.A. Physical activity and pregnancy outcomes: An expert review. Am. J. Obstet. Gynecol. MFM 2023, 5, 100758. [Google Scholar] [CrossRef]
- Forczek, W.; Curylo, M.; Forczek, B. Physical activity assessment during gestation and its outcomes: A review. Obstet. Gynecol. Surv. 2017, 72, 425–444. [Google Scholar] [CrossRef] [PubMed]
- Menke, B.R.; Duchette, C.; Tinius, R.A.; Wilson, A.Q.; Altizer, E.A.; Maples, J.M. Physical Activity during Pregnancy and Newborn Body Composition: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 7127. [Google Scholar] [CrossRef]
- Perkins, C.C.; Pivarnik, J.M.; Paneth, N.; Stein, A.D. Physical activity and fetal growth during pregnancy. Obstet. Gynecol. 2007, 109, 81–87. [Google Scholar] [CrossRef]
- Teede, H.J.; Bailey, C.; Moran, L.J.; Khomami, M.B.; Enticott, J.; Ranasinha, S.; Rogozińska, E.; Skouteris, H.; Boyle, J.A.; Thangaratinam, S. Association of antenatal diet and physical activity–based interventions with gestational weight gain and pregnancy outcomes: A systematic review and meta-analysis. JAMA Intern. Med. 2022, 182, 106–114. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee Opinion No. 650: Physical Activity and Exercise During Pregnancy and the Postpartum Period. Obstet. Gynecol. 2015, 126, e135–e142.
- Davies, G.A.; Wolfe, L.A.; Mottola, M.F.; MacKinnon, C. Joint SOGC/CSEP clinical practice guideline: Exercise in pregnancy and the postpartum period. Can. J. Appl. Physiol. 2003, 28, 329–341. [Google Scholar] [CrossRef]
- Aktan, B.; Kayıkçıoğlu, F.; Akbayrak, T. The comparison of the effects of clinical Pilates exercises with and without childbirth training on pregnancy and birth results. Int. J. Clin. Pract. 2021, 75, e14516. [Google Scholar] [CrossRef]
- Atkinson, S.A.; Maran, A.; Dempsey, K.; Perreault, M.; Vanniyasingam, T.; Phillips, S.M.; Hutton, E.K.; Mottola, M.F.; Wahoush, O.; Xie, F. Be Healthy in Pregnancy (BHIP): A randomized controlled trial of nutrition and exercise intervention from early pregnancy to achieve recommended gestational weight gain. Nutrients 2022, 14, 810. [Google Scholar] [CrossRef] [PubMed]
- Babbar, S.; Hill, J.B.; Williams, K.B.; Pinon, M.; Chauhan, S.P.; Maulik, D. Acute feTal behavioral Response to prenatal Yoga: A single, blinded, randomized controlled trial (TRY yoga). Am. J. Obstet. Gynecol. 2016, 214, 399.e1–399.e8. [Google Scholar] [CrossRef]
- Bacchi, M.; Mottola, M.F.; Perales, M.; Refoyo, I.; Barakat, R. Aquatic activities during pregnancy prevent excessive maternal weight gain and preserve birth weight: A randomized clinical trial. Am. J. Health Promot. 2018, 32, 729–735. [Google Scholar] [CrossRef]
- Backhausen, M.G.; Tabor, A.; Albert, H.; Rosthøj, S.; Damm, P.; Hegaard, H.K. The effects of an unsupervised water exercise program on low back pain and sick leave among healthy pregnant women–A randomised controlled trial. PLoS ONE 2017, 12, e0182114. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Lopez, C.; Montejo, R.; Coteron, J. Exercise during pregnancy reduces the rate of cesarean and instrumental deliveries: Results of a randomized controlled trial. J. Matern. Fetal. Neonatal. Med. 2012, 25, 2372–2376. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Lopez, C.; Lucia, A.; Ruiz, J.R. Exercise during pregnancy and gestational diabetes-related adverse effects: A randomized controlled trial. Br. J. Sports Med. 2013, 47, 630–636. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obstet. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Franco, E.; Perales, M.; Lopez, C.; Mottola, M.F. Exercise during pregnancy is associated with a shorter duration of labor. A randomized clinical trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Vargas, M.; Brik, M.; Fernandez, I.; Gil, J.; Coteron, J.; Santacruz, B. Does Exercise During Pregnancy Affect Placental Weight?: A Randomized Clinical Trial. Eval. Health Prof. 2018, 41, 400–414. [Google Scholar] [CrossRef]
- Barakat, R.; Refoyo, I.; Coteron, J.; Franco, E. Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Braz. J. Phys. Ther. 2018, 23, 148–155. [Google Scholar] [CrossRef]
- Bhartia, N.; Jain, S.; Shankar, N.; Rajaram, S.; Gupta, M. Effects of antenatal yoga on maternal stress and clinical outcomes in north indian women: A randomised controlled trial. J. Indian Acad. Clin. Med. 2019, 20, 10–14. [Google Scholar]
- Bjontegaard, K.A.; Stafne, S.N.; Morkved, S.; Salvesen, K.A.; Evensen, K.A.I. Body mass index and physical activity in seven-year-old children whose mothers exercised during pregnancy: Follow-up of a multicentre randomised controlled trial. BMC Pediatr. 2021, 21, 496. [Google Scholar] [CrossRef]
- Brik, M.; Fernández-Buhigas, I.; Martin-Arias, A.; Vargas-Terrones, M.; Barakat, R.; Santacruz, B. Does exercise during pregnancy impact on maternal weight gain and fetal cardiac function? A randomized controlled trial. Ultrasound Obstet. Gynecol. 2019, 53, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Bruno, R.; Petrella, E.; Bertarini, V.; Pedrielli, G.; Neri, I.; Facchinetti, F. Adherence to a lifestyle programme in overweight/obese pregnant women and effect on gestational diabetes mellitus: A randomized controlled trial. Matern. Child Nutr. 2017, 13, e12333. [Google Scholar] [CrossRef]
- Clark, E.; Isler, C.; Strickland, D.; McMillan, A.G.; Fang, X.; Kuehn, D.; Ravisankar, S.; Strom, C.; May, L.E. Influence of aerobic exercise on maternal lipid levels and offspring morphometrics. Int. J. Obes. 2019, 43, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Cordero, Y.; Mottola, M.F.; Vargas, J.; Blanco, M.; Barakat, R. Exercise Is Associated with a Reduction in Gestational Diabetes Mellitus. Med. Sci. Sports Exerc. 2015, 47, 1328–1333. [Google Scholar] [CrossRef]
- da Silva, S.G.; Hallal, P.C.; Domingues, M.R.; Bertoldi, A.D.; Silveira, M.F.d.; Bassani, D.; da Silva, I.C.M.; da Silva, B.G.C.; Coll, C.d.V.N.; Evenson, K. A randomized controlled trial of exercise during pregnancy on maternal and neonatal outcomes: Results from the PAMELA study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 175. [Google Scholar] [CrossRef]
- Daly, N.; Farren, M.; McKeating, A.; O’Kelly, R.; Stapleton, M.; Turner, M.J. A Medically Supervised Pregnancy Exercise Intervention in Obese Women: A Randomized Controlled Trial. Obstet. Gynecol. 2017, 130, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- de Oliveria Melo, A.S.; Silva, J.L.P.; Tavares, J.S.; Barros, V.O.; Leite, D.F.; Amorim, M.M. Effect of a physical exercise program during pregnancy on uteroplacental and fetal blood flow and fetal growth: A randomized controlled trial. Obstet. Gynecol. 2012, 120, 302–310. [Google Scholar] [CrossRef]
- Ellingsen, M.S.; Pettersen, A.; Stafne, S.N.; Morkved, S.; Salvesen, K.A.; Evensen, K. Neurodevelopmental outcome in 7-year-old children is not affected by exercise during pregnancy: Follow up of a multicentre randomised controlled trial. BJOG 2020, 127, 508–517. [Google Scholar] [CrossRef]
- Fritel, X.; De Tayrac, R.; Bader, G.; Savary, D.; Gueye, A.; Deffieux, X.; Fernandez, H.; Richet, C.; Guilhot, J.; Fauconnier, A. Preventing urinary incontinence with supervised prenatal pelvic floor exercises: A randomized controlled trial. Obstet. Gynecol. 2015, 126, 370–377. [Google Scholar] [CrossRef]
- Garnaes, K.K.; Nyrnes, S.A.; Salvesen, K.Å.; Salvesen, Ø.; Mørkved, S.; Moholdt, T. Effect of supervised exercise training during pregnancy on neonatal and maternal outcomes among overweight and obese women. Secondary analyses of the ETIP trial: A randomised controlled trial. PLoS ONE 2017, 12, e0173937. [Google Scholar] [CrossRef] [PubMed]
- Guelfi, K.J.; Ong, M.J.; Crisp, N.A.; Fournier, P.A.; Wallman, K.E.; Grove, J.R.; Doherty, D.A.; Newnham, J.P. Regular Exercise to Prevent the Recurrence of Gestational Diabetes Mellitus: A Randomized Controlled Trial. Obstet. Gynecol. 2016, 128, 819–827. [Google Scholar] [CrossRef]
- Haakstad, L.A.; Bø, K. Exercise in pregnant women and birth weight: A randomized controlled trial. BMC Pregnancy Childbirth 2011, 11, 66. [Google Scholar] [CrossRef]
- Hellenes, O.M.; Vik, T.; Løhaugen, G.C.; Salvesen, K.Å.; Stafne, S.N.; Mørkved, S.; Evensen, K.A.I. Regular moderate exercise during pregnancy does not have an adverse effect on the neurodevelopment of the child. Acta Paediatr. 2015, 104, 285–291. [Google Scholar] [CrossRef]
- Hopkins, S.A.; Baldi, J.C.; Cutfield, W.S.; McCowan, L.; Hofman, P.L. Exercise training in pregnancy reduces offspring size without changes in maternal insulin sensitivity. J. Clin. Endocrinol. Metab. 2010, 95, 2080–2088. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, H.H.; Froshaug, B.E.; Lysaker, P.J.G.; Salvesen, K.A.; Lukasse, M.; Morkved, S.; Stafne, S.N. Regular antenatal exercise including pelvic floor muscle training reduces urinary incontinence 3 months postpartum-Follow up of a randomized controlled trial. Acta Obstet. Gynecol. Scand. 2021, 100, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Karthiga, K.; Pal, G.K.; Dasari, P.; Nanda, N.; Velkumary, S.; Chinnakali, P.; Renugasundari, M.; Harichandrakumar, K.T. Effects of yoga on cardiometabolic risks and fetomaternal outcomes are associated with serum nitric oxide in gestational hypertension: A randomized control trial. Sci. Rep. 2022, 12, 11732. [Google Scholar] [CrossRef]
- Labonte-Lemoyne, E.; Curnier, D.; Ellemberg, D. Exercise during pregnancy enhances cerebral maturation in the newborn: A randomized controlled trial. J. Clin. Exp. Neuropsychol. 2017, 39, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Leon-Larios, F.; Corrales-Gutierrez, I.; Casado-Mejia, R.; Suarez-Serrano, C. Influence of a pelvic floor training programme to prevent perineal trauma: A quasi-randomised controlled trial. Midwifery 2017, 50, 72–77. [Google Scholar] [CrossRef]
- McDonald, S.M.; Yeo, S.; Liu, J.; Wilcox, S.; Sui, X.; Pate, R.R. Associations between maternal physical activity and fitness during pregnancy and infant birthweight. Prev. Med. Rep. 2018, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.M.; Mouro, S.; Wisseman, B.; Isler, C.; DeVente, J.; Newton, E.; Hildebrand, J.; Kuehn, D.; Kelley, G.; Chasan-Taber, L. Influence of prenatal exercise on the relationship between maternal overweight and obesity and select delivery outcomes. Sci. Rep. 2022, 12, 17343. [Google Scholar] [CrossRef]
- Murtezani, A.; Paçarada, M.; Ibraimi, Z.; Nevzati, A.; Abazi, N. The impact of exercise during pregnancy on neonatal outcomes: A randomized controlled trial. J. Sports Med. Phys. Fitness 2014, 54, 802–808. [Google Scholar]
- Nagpal, T.S.; Prapavessis, H.; Campbell, C.G.; de Vrijer, B.; Bgeginski, R.; Hosein, K.; Paplinskie, S.; Manley, M.; Mottola, M.F. Sequential introduction of exercise first followed by nutrition improves program adherence during pregnancy: A randomized controlled trial. Int. J. Behav. Med. 2020, 27, 108–118. [Google Scholar] [CrossRef]
- Nascimento, S.L.; Surita, F.G.; Parpinelli, M.A.; Siani, S.; Pinto e Silva, J.L. The effect of an antenatal physical exercise programme on maternal/perinatal outcomes and quality of life in overweight and obese pregnant women: A randomised clinical trial. BJOG 2011, 118, 1455–1463. [Google Scholar] [CrossRef]
- Navas, A.; Carrascosa, M.d.C.; Artigues, C.; Ortas, S.; Portells, E.; Soler, A.; Yañez, A.M.; Bennasar-Veny, M.; Leiva, A. Effectiveness of moderate-intensity aerobic water exercise during pregnancy on quality of life and postpartum depression: A multi-center, randomized controlled trial. J. Clin. Med. 2021, 10, 2432. [Google Scholar] [CrossRef]
- Pais, M.; Pai, M.V.; Kamath, A.; Bhat, R.; Bhat, P.; Joisa, G.H. A Randomized Controlled Trial on the Efficacy of Integrated Yoga on Pregnancy Outcome. Holist. Nurs. Pract. 2021, 35, 273–280. [Google Scholar] [CrossRef]
- Perales, M.; Refoyo, I.; Coteron, J.; Bacchi, M.; Barakat, R. Exercise during pregnancy attenuates prenatal depression: A randomized controlled trial. Eval. Health Prof. 2015, 38, 59–72. [Google Scholar] [CrossRef]
- Perales Santaella, M.; Mateos, S.; Vargas, M.; Sanz, I.; Lucía Mulas, A.; Barakat Carballo, R.O. Fetal and maternal heart rate responses to exercise in pregnant women. A randomized Controlled Trial. Arch. Med. Deporte 2015, 170, 361–367. [Google Scholar]
- Perales, M.; Valenzuela, P.L.; Barakat, R.; Cordero, Y.; Pelaez, M.; Lopez, C.; Ruilope, L.M.; Santos-Lozano, A.; Lucia, A. Gestational Exercise and Maternal and Child Health: Effects until Delivery and at Post-Natal Follow-up. J. Clin. Med. 2020, 9, 379. [Google Scholar] [CrossRef]
- Pereira, I.B.; Silva, R.; Ayres-de-Campos, D.; Clode, N. Physical exercise at term for enhancing the spontaneous onset of labor: A randomized clinical trial. J. Matern. Fetal. Neonatal. Med. 2022, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Phelan, S.; Phipps, M.G.; Abrams, B.; Darroch, F.; Schaffner, A.; Wing, R.R. Randomized trial of a behavioral intervention to prevent excessive gestational weight gain: The Fit for Delivery Study. Am. J. Clin. Nutr. 2011, 93, 772–779. [Google Scholar] [CrossRef]
- Price, B.B.; Amini, S.B.; Kappeler, K. Exercise in pregnancy: Effect on fitness and obstetric outcomes-a randomized trial. Med. Sci. Sports Exerc. 2012, 44, 2263–2269. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, N. Effect of a exercise by pregnant women and birth weight: A randomized controlled trial. J. Evol. Med. Dent. Sci. 2015, 4, 1509–1517. [Google Scholar] [CrossRef]
- Raper, M.J.; McDonald, S.; Johnston, C.; Isler, C.; Newton, E.; Kuehn, D.; Collier, D.; Broskey, N.T.; Muldrow, A.; May, L.E. The influence of exercise during pregnancy on racial/ethnic health disparities and birth outcomes. BMC Pregnancy Childbirth 2021, 21, 258. [Google Scholar] [CrossRef]
- Rodriguez-Blanque, R.; Sanchez-Garcia, J.C.; Sanchez-Lopez, A.M.; Exposito-Ruiz, M.; Aguilar-Cordero, M.J. Randomized Clinical Trial of an Aquatic Physical Exercise Program During Pregnancy. J. Obstet. Gynecol. Neonatal. Nurs. 2019, 48, 321–331. [Google Scholar] [CrossRef]
- Rodríguez-Díaz, L.; Ruiz-Frutos, C.; Vázquez-Lara, J.M.; Ramírez-Rodrigo, J.; Villaverde-Gutiérrez, C.; Torres-Luque, G. Effectiveness of a physical activity programme based on the Pilates method in pregnancy and labour. Enferm. Clín. 2017, 27, 271–277. [Google Scholar] [CrossRef]
- Ruchat, S.-M.; Davenport, M.H.; Giroux, I.; Hillier, M.; Batada, A.; Sopper, M.M.; Hammond, J.; Mottola, M.F. Nutrition and exercise reduce excessive weight gain in normal-weight pregnant women. Med. Sci. Sports Exerc. 2012, 44, 1419–1426. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Perales, M.; Pelaez, M.; Lopez, C.; Lucia, A.; Barakat, R. Supervised exercise–based intervention to prevent excessive gestational weight gain: A randomized controlled trial. Mayo Clin. Proc. 2013, 88, 1388–1397. [Google Scholar] [CrossRef]
- Sagedal, L.; Øverby, N.; Bere, E.; Torstveit, M.; Lohne-Seiler, H.; Småstuen, M.; Hillesund, E.; Henriksen, T.; Vistad, I. Lifestyle intervention to limit gestational weight gain: The Norwegian Fit for Delivery randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Seneviratne, S.N.; Jiang, Y.; Derraik, J.; McCowan, L.; Parry, G.K.; Biggs, J.B.; Craigie, S.; Gusso, S.; Peres, G.; Rodrigues, R.O.; et al. Effects of antenatal exercise in overweight and obese pregnant women on maternal and perinatal outcomes: A randomised controlled trial. BJOG 2016, 123, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Silva-Jose, C.; Sánchez-Polán, M.; Barakat, R.; Díaz-Blanco, Á.; Mottola, M.F.; Refoyo, I. A Virtual Exercise Program throughout Pregnancy during the COVID-19 Pandemic Modifies Maternal Weight Gain, Smoking Habits and Birth Weight—Randomized Clinical Trial. J. Clin. Med. 2022, 11, 4045. [Google Scholar] [CrossRef] [PubMed]
- Sobhgol, S.S.; Smith, C.A.; Thomson, R.; Dahlen, H.G. The effect of antenatal pelvic floor muscle exercise on sexual function and labour and birth outcomes: A randomised controlled trial. Women Birth 2022, 35, e607–e614. [Google Scholar] [CrossRef]
- Stafne, S.N.; Salvesen, K.A.; Romundstad, P.R.; Eggebo, T.M.; Carlsen, S.M.; Morkved, S. Regular exercise during pregnancy to prevent gestational diabetes: A randomized controlled trial. Obstet. Gynecol. 2012, 119, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Szumilewicz, A.; Kuchta, A.; Kranich, M.; Dornowski, M.; Jastrzebski, Z. Prenatal high-low impact exercise program supported by pelvic floor muscle education and training decreases the life impact of postnatal urinary incontinence: A quasiexperimental trial. Medicine 2020, 99, e18874. [Google Scholar] [CrossRef]
- Taniguchi, C.; Sato, C. Home-based walking during pregnancy affects mood and birth outcomes among sedentary women: A randomized controlled trial. Int. J. Nurs. Pract. 2016, 22, 420–426. [Google Scholar] [CrossRef]
- Tomic, V.; Sporis, G.; Tomic, J.; Milanovic, Z.; Zigmundovac-Klaic, D.; Pantelic, S. The effect of maternal exercise during pregnancy on abnormal fetal growth. Croat. Med. J. 2013, 54, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Uria-Minguito, A.; Silva-Jose, C.; Sanchez-Polan, M.; Diaz-Blanco, A.; Garcia-Benasach, F.; Carrero Martinez, V.; Alzola, I.; Barakat, R. The Effect of Online Supervised Exercise throughout Pregnancy on the Prevention of Gestational Diabetes in Healthy Pregnant Women during COVID-19 Pandemic: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 14104. [Google Scholar] [CrossRef]
- Ussher, M.; Lewis, S.; Aveyard, P.; Manyonda, I.; West, R.; Lewis, B.; Marcus, B.; Riaz, M.; Taylor, A.H.; Barton, P.; et al. The London Exercise And Pregnant smokers (LEAP) trial: A randomised controlled trial of physical activity for smoking cessation in pregnancy with an economic evaluation. Health Technol. Assess. 2015, 19, 1–135. [Google Scholar] [CrossRef] [PubMed]
- Vinter, C.A.; Jensen, D.M.; Ovesen, P.; Beck-Nielsen, H.; Jørgensen, J.S. The LiP (Lifestyle in Pregnancy) study: A randomized controlled trial of lifestyle intervention in 360 obese pregnant women. Diabetes Care 2011, 34, 2502–2507. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wei, Y.; Zhang, X.; Zhang, Y.; Xu, Q.; Sun, Y.; Su, S.; Zhang, L.; Liu, C.; Feng, Y.; et al. A randomized clinical trial of exercise during pregnancy to prevent gestational diabetes mellitus and improve pregnancy outcome in overweight and obese pregnant women. Am. J. Obstet. Gynecol. 2017, 216, 340–351. [Google Scholar] [CrossRef]
- Yekefallah, L.; Namdar, P.; Dehghankar, L.; Golestaneh, F.; Taheri, S.; Mohammadkhaniha, F. The effect of yoga on the delivery and neonatal outcomes in nulliparous pregnant women in Iran: A clinical trial study. BMC Pregnancy Childbirth 2021, 21, 351. [Google Scholar] [CrossRef]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE approach in systematic reviews and guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019; pp. 205–228. [Google Scholar]
- Hedges, L.V.; Tipton, E.; Johnson, M.C. Robust variance estimation in meta-regression with dependent effect size estimates. Res. Synth. Methods 2010, 1, 39–65. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.6; John Wiley & Sons: Chichester, UK, 2011. [Google Scholar]
- Saigal, S.; Stoskopf, B.; Streiner, D.; Paneth, N.; Pinelli, J.; Boyle, M. Growth trajectories of extremely low birth weight infants from birth to young adulthood: A longitudinal, population-based study. Pediatr. Res. 2006, 60, 751–758. [Google Scholar] [CrossRef]
- Bisson, M.; Lavoie-Guénette, J.; Tremblay, A.; Marc, I. Physical activity volumes during pregnancy: A systematic review and meta-analysis of observational studies assessing the association with infant’s birth weight. Am. J. Perinatol. Rep. 2016, 6, e170–e197. [Google Scholar] [CrossRef] [PubMed]
- Most, J.; Marlatt, K.L.; Altazan, A.D.; Redman, L.M. Advances in assessing body composition during pregnancy. Eur. J. Clin. Nutr. 2018, 72, 645–656. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Gao, E.; Wu, J.; Zhou, J.; Yang, Q.; Walker, M.; Mbikay, M.; Sigal, R.; Nair, R.; Wen, S. Fetal macrosomia and adolescence obesity: Results from a longitudinal cohort study. Int. J. Obes. 2009, 33, 923–928. [Google Scholar] [CrossRef]
- Sauder, K.A.; Ritchie, N.D. Reducing intergenerational obesity and diabetes risk. Diabetologia 2021, 64, 481–490. [Google Scholar] [CrossRef]
- Beall, M.H.; El Haddad, M.; Gayle, D.; Desai, M.; Ross, M.G. Adult obesity as a consequence of in utero programming. Clin. Obstet. Gynecol. 2004, 47, 957–966. [Google Scholar] [CrossRef]
- Sarr, O.; Yang, K.; Regnault, T.R. In utero programming of later adiposity: The role of fetal growth restriction. J. Pregnancy 2012, 2012, 134758. [Google Scholar] [CrossRef]
- Silveira, P.P.; Portella, A.K.; Goldani, M.Z.; Barbieri, M.A. Developmental origins of health and disease (DOHaD). J. Pediatr. 2007, 83, 494–504. [Google Scholar] [CrossRef]
- Santos, P.C.; Leirós-Rodríguez, R.; Abreu, S.; Ferreira, M.; Alves, O.; Mota, J. Physical activity during pregnancy and its effects on neonatal outcomes. Placenta 2022, 128, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Jantunen, H.; Wasenius, N.; Salonen, M.K.; Perälä, M.-M.; Kautiainen, H.; Simonen, M.; Pohjolainen, P.; Kajantie, E.; von Bonsdorff, M.; Eriksson, J. Relationship between physical activity and physical performance in later life in different birth weight groups. J. Dev. Orig. Health Dis. 2018, 9, 95–101. [Google Scholar] [CrossRef]
- Walasik, I.; Kwiatkowska, K.; Kosińska Kaczyńska, K.; Szymusik, I. Physical activity patterns among 9000 pregnant women in poland: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 1771. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.-M.; Poitras, V.J.; Garcia, A.J.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Ruchat, S.-M.; Mottola, M.F.; Skow, R.J.; Nagpal, T.S.; Meah, V.L.; James, M.; Riske, L.; Sobierajski, F.; Kathol, A.J.; Marchand, A.-A. Effectiveness of exercise interventions in the prevention of excessive gestational weight gain and postpartum weight retention: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Currie, L.M.; Woolcott, C.G.; Fell, D.B.; Armson, B.A.; Dodds, L. The association between physical activity and maternal and neonatal outcomes: A prospective cohort. Matern. Child Health J. 2014, 18, 1823–1830. [Google Scholar] [CrossRef] [PubMed]
- Mou, S.S.; Gillies, C.; Hu, J.; Danielli, M.; Al Wattar, B.H.; Khunti, K.; Tan, B.K. Association between HbA1c Levels and Fetal Macrosomia and Large for Gestational Age Babies in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of 17,711 Women. J. Clin. Med. 2023, 12, 3852. [Google Scholar] [CrossRef]
- International Weight Management in Pregnancy (i-WIP). Collaborative Group. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: Meta-analysis of individual participant data from randomised trials. BMJ 2017, 358, j3119. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Type | N | EG | CG | Intervention Physical Exercise Program | Main Variables Analyzed | Secondary Variables Analyzed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Freq | Intensity | Duration of Program | Type of Exercise | Superv. Class | Duration of Class | Adh. | |||||||||
| Aktan [24] | 2021 | Turkey | RCT | 43 | 21 | 22 | 2 | Mod | 8 w | Clinical Pilates exercise | Yes | 60 min | - | General anxiety, gestational weight gain | Type of delivery, birth weight |
| Atkinson [25] | 2022 | Canada | RTC | 241 | 119 | 122 | 3–4 | Mod | 22 w | Walking | No | 25–40 min | 80% | Gestational weight gain | Depression, type of delivery, and birth weight |
| Babbar [26] | 2016 | USA | RCT | 46 | 23 | 23 | 3 | Mod | 8 w | Yoga | Yes | 60 min | 80% | Umbilical artery, type of delivery, birth weight | Gestational weight gain |
| Bacchi [27] | 2018 | Argentina | RTC | 111 | 49 | 62 | 3 | Low–Mod | 28 w | Aquatic activities | Yes | 55–60 min | 80% | Gestational weight gain and birth weight | - |
| Backhausen [28] | 2017 | Denmark | RCT | 516 | 258 | 258 | 2 | Low | 12 w | Water exercise | No | 70 min | 76% | Low back pain, birth weight | Type of delivery |
| Barakat [29] | 2012 | Spain | RCT | 290 | 138 | 152 | 3 | Mod | 28 w | Aerobic exercise | Yes | 40–45 min | - | Type of delivery | Gestational weight gain and birth weight |
| Barakat [30] | 2013 | Spain | RCT | 510 | 255 | 255 | 3 | Mod | 28 w | Aerobic, strength, and flexibility exercise | Yes | 50–55 min | 95% | Gestational diabetes | Gestational weight gain and birth weight |
| Barakat [31] | 2016 | Spain | RCT | 765 | 382 | 383 | 3 | Mod | 28 w | Aerobic, strength, and flexibility exercise | Yes | 50–55 min | 80% | Hypertension | Type of delivery, gestational weight gain, birth weight |
| Barakat [32] | 2018a | Spain | RCT | 429 | 227 | 202 | 3 | Mod | 28 w | Aerobic exercise | Yes | 55–60 min | 80% | Duration of labor | Type of delivery, use of epidural, birth weight |
| Barakat [33] | 2018b | Spain | RCT | 65 | 33 | 32 | 3 | Mod | 28 w | Aerobic, pelvic floor strength, and flexibility exercise | Yes | 55–60 min | 85% | Placenta weight | Gestational age, type of delivery, birth weight |
| Barakat [34] | 2018c | Spain | RCT | 456 | 234 | 222 | 3 | Mod | 28 w | Aerobic exercise | Yes | 50–55 min | 80% | Gestational weight gain | Gestational age, type of delivery, birth weight |
| Bhartia [35] | 2019 | India | RCT | 78 | 38 | 40 | 1 | Mod | 12 w | Yoga | Yes | 50 min | - | Maternal stress, type of delivery, birth weight | - |
| 2 | No | ||||||||||||||
| Bjøntegaard [36] | 2021 | Norway | RCT | 281 | 164 | 117 | 1 | Mod | 12 w | Aerobic, strength, and balance exercise | Yes | 60 min | - | Type of delivery, birth weight | Physical activity of children at age of seven |
| 2 | No | 45 min | |||||||||||||
| Brik [37] | 2019 | Spain | RTC | 85 | 42 | 43 | 3 | 55–60% Max HR | 29 w | Aerobic, strength, coordination and balance, and pelvic floor exercise | Yes | 60 min | 70% | Gestational weight gain, fetal cardiac function | Type of delivery, birth weight, gestational age |
| Bruno [38] | 2016 | Italy | RTC | 131 | 69 | 62 | 3 | Mod | 16 w | Walking, dietary counselling | No | 30 min | - | Gestational diabetes | Gestational weight gain, type of delivery, birth weight |
| Clark [39] | 2018 | USA | RTC | 36 | 14 | 22 | 3 | Mod | 20 w | Aerobic | Yes | 60 min | - | Gestational weight gain | Type of delivery, birth weight |
| Cordero [40] | 2015 | Spain | RCT | 257 | 101 | 156 | 2 | 50–55% Max HR | 26 w | Aerobics in gym hall | Yes | 50–60 min | 80% | Gestational diabetes | Gestational weight gain, type of delivery, birth weight |
| 1 | Aquatic activity | ||||||||||||||
| Da Silva [41] | 2017 | Brazil | RTC | 639 | 213 | 426 | 3 | Mod | 16 w | Aerobic, strength training | Yes | 60 min | 70% | Preterm birth and pre-eclampsia | Gestational weight gain, birth weight |
| Daly [42] | 2017 | Ireland | RCT | 88 | 44 | 44 | 3 | Mod | 26 w | Aerobic, pelvic floor exercise | Yes | 50–60 min | 80% | Maternal fasting plasma glucose | Type of delivery and birth weight |
| De Oliveria [43] | 2012 | Brazil | RTC | 111 | 54 | 57 | 3 | 60–80% Max HR | 25 w | Walking | Yes | 15–40 min | 85% | VO2max, birth weight and gestational age | - |
| Ellingsen [44] | 2020 | Norway | RTC | 279 | 164 | 115 | 1 | Mod | 12 w | Aerobic activity and strength exercise | Yes | 60 min | - | Neurodevelopment in 7-year-old children | Gestational age, birth weight, type of delivery |
| 2 | No | 45 min | |||||||||||||
| Fritel [45] | 2015 | France | RCT | 282 | 140 | 142 | 1 | Low | 8 w | Pelvic floor training | Yes | 20–30 min | - | Urinary incontinence | Type of delivery and birth weight |
| Garnaes [46] | 2017 | Norway | RCT | 74 | 38 | 36 | 3 | Mod | 20 w | Aerobic, strength training | Yes | 60 min | - | Birth weight | Type of delivery, perineal tears, gestational age |
| 2 | - | No | 50 min | ||||||||||||
| 7 | Pelvic floor training | No | 1 min | ||||||||||||
| Guelfi [47] | 2016 | Australia | RCT | 172 | 85 | 87 | 3 | Mod | 14 w | Home-based stationary cycling program | Yes | 20–60 min | - | Gestational diabetes | Type of delivery, birth weight |
| Haakstad [48] | 2011 | Norway | RCT | 105 | 52 | 53 | 2 | Mod | 12 w | Aerobic dance and strength training | Yes | 60 min | 80% | Birth weight | Gestational age, type of delivery |
| 1 | No | 30 min | |||||||||||||
| Hellenes [49] | 2015 | Norway | RCT | 336 | 188 | 148 | 1 | Mod | 16 w | Aerobic activity | Yes | 30 + min | - | Cognitive, language and motor domains of children | Gestational age, birth weight, and type of delivery |
| 2 | No | ||||||||||||||
| Hopkins [50] | 2010 | New Zealand | RCT | 84 | 47 | 37 | 5 | 65% VO2max | 16 w | Stationary cycling program | No | 40 min | - | Birth weight, gestational age | - |
| Johannessen [51] | 2021 | Norway | RCT | 722 | 383 | 339 | 1 | Mod | 12 w | Aerobic, strength and pelvic floor exercise | Yes | 55–70 min | - | Urinary incontinence at 3 months postpartum | Type of delivery, episiotomy, epidural, duration of labor, birth weight |
| 2 | No | 45 min | |||||||||||||
| Karthiga [52] | 2022 | India | RCT | 234 | 121 | 113 | 7 | Mod | 20 w | Yoga 5 sessions of Yoga techniques | No | 60 min | - | Gestational hypertension | Type of delivery, duration of labor, birth weight |
| Labonte-Leymoyne [53] | 2017 | Canada | RCT | 18 | 10 | 8 | 3 | 55% VO2max | 24 w | Aerobic exercise | Yes | 20 + min | - | Neuroelectric response of the neonatal brain | Maternal weight gain, birth weight |
| Leon-Larios [54] | 2017 | Spain | RCT | 466 | 254 | 212 | 5 | Low | 6 w | Perineal massage and pelvic floor exercise | No | 18–23 min | - | Perineal tear and episiotomy | Type of delivery, duration of labor, birth weight, and epidural analgesia |
| McDonald [55] | 2018 | USA | RCT | 90 | 49 | 41 | 5 | 55–69% Max HR | 20 w | Walking program | No | 40 min | - | Preeclampsia and pathophysiological progress of preeclampsia | Gestational weight gain and birth weight |
| McDonald [56] | 2022 | USA | RCT | 192 | 131 | 61 | 3 | Mod | 24 w | Aerobic and resistance training | Yes | 50 min | 80% | Gestational weight gain, type of delivery and birth weight | - |
| Murtezani [57] | 2014 | Republic of Kosovo | RCT | 63 | 30 | 33 | 3 | Mod | 20 w | Aerobic and strength exercise | Yes | 40–45 min | 85% | Birth weight and gestational age | - |
| Nagpal [58] | 2020 | Canada | RCT | 40 | 23 | 17 | 3 | Mild | 11 w | Walking program + nutrition | Yes | 25–40 min | 80.2% | Scoring women on meeting the intervention goals | Gestational weight gain, birth weight, macrosomia, and low birth weight |
| Nascimento [59] | 2011 | Brazil | RCT | 80 | 39 | 41 | 5 | Low–Mod | 17 w | Aerobic exercise Walking | No | 40 min | 62.5% | Gestational weight gain | Birth weight |
| Navas [60] | 2021 | Spain | RCT | 294 | 148 | 146 | 3 | 55–65% Max HR | 20 w | Aquatic exercise | Yes | 45 min | - | Postpartum depression, quality of life, and quality of sleep | Gestational age, birth weight |
| Pais [61] | 2021 | India | RCT | 124 | 61 | 63 | 7 | Low | 20 w | Yoga One-to-one Yoga session for 7 days | No | 45 min | - | Preeclampsia and gestational diabetes | Gestational age, duration of labor, type of delivery, birth weight |
| Perales [62] | 2014 | Spain | RCT | 167 | 90 | 77 | 3 | 55–60% Max HR | 29 w | Aerobic activity | Yes | 55–60 min | - | Prenatal depression | Gestational weight gain, birth weight, and type of delivery |
| Perales [63] | 2015 | Spain | RCT | 63 | 38 | 25 | 3 | 55–60% Max HR | 28 w | Aerobic dance, pelvic floor muscle training | Yes | 55–60 min | 80% | Fetal and maternal heart rate | Gestational weight gain, birth weight, type of delivery |
| Perales [64] | 2020 | Spain | RCT | 1348 | 688 | 660 | 3 | Light–Mod | 30 w | Aerobic, pelvic floor exercise | Yes | 50–55 min | 95% | Gestational weight gain, hypertension, and gestational diabetes | Type of delivery, birth weight, gestational age |
| Pereira [65] | 2022 | Portugal | RCT | 126 | 63 | 63 | 3 | 55–69% Max HR | 3 w | Walking | Yes | 30 min | - | Rate of labor induction | Type of delivery, birth weight |
| Phelan [66] | 2011 | USA | RCT | 363 | 179 | 184 | 7 | Low | 26 w | Walking | No | 30 min | - | Gestational weight gain | Gestational hypertension, birth weight, and type of delivery |
| Price [67] | 2012 | USA | RCT | 62 | 31 | 31 | 4 | Mod | 23 w | Aerobic exercise | Yes | 45–60 min | - | Birth weight | Duration of labor, type of delivery |
| Prabhu [68] | 2015 | India | RCT | 105 | 52 | 53 | 2 | Mod | 12 w | Aerobic dance | Yes | 45 min | 80% | Birth weight | - |
| 1 | No | 30 min | |||||||||||||
| Raper [69] | 2021 | USA | RCT | 125 | 58 | 67 | 3 | Mod | 24 w | Aerobic | Yes | 50 min | 80% | Gestational diabetes, type of delivery, and birth weight | - |
| Rodriguez-Blanque [70] | 2019 | Spain | RTC | 129 | 65 | 64 | 3 | Mod | 17 w | Aquatic physical exercise | Yes | 60 min | - | Laceration and episiotomy rates | Type of delivery, birth weight, and anesthesia |
| Rodriguez-Diaz [71] | 2017 | Spain | RCT | 100 | 50 | 50 | 2 | Mod | 8 w | Pilates | Yes | 40–45 min | 90% | Gestational weight gain, blood pressure, strength, flexibility, and spinal curvature | Type of delivery, episiotomy, analgesia, and birth weight |
| Ruchat [72] | 2012 | Canada | RCT | 71 | 26 | 45 | 1 | Mod | 22 w | Walking | Yes | 25–40 min | - | Gestational weight gain, birth weight | - |
| 2–3 | No | ||||||||||||||
| Ruiz [73] | 2013 | Spain | RCT | 962 | 481 | 481 | 3 | Light–Mod | 28 w | Aerobic and resistance exercise | Yes | 50–55 min | 97% | Gestational weight gain | Birth weight, type of delivery |
| Sagedal [74] | 2017 | Norway | RCT | 591 | 296 | 295 | 2 | Mod | 24 w | Aerobic, strength training. Dietary counselling | Yes | 60 min | - | Gestational weight gain, birth weight | Gestational age, perineal tear |
| Seneviratne [75] | 2015 | New Zealand | RCT | 75 | 38 | 37 | 3–5 | Mod | 16 w | Stationary cycling program | No | 15–30 min | - | Birth weight, type of delivery | Gestational weight gain, gestational age |
| Silva-Jose [76] | 2022 | Spain | RCT | 139 | 69 | 70 | 3 | 55–65% Max HR | 30 w | Aerobic exercise | Yes | 55–60 min | 80% | Gestational weight gain | Birth weight, type of delivery |
| Sobhgol [77] | 2022 | Australia | RCT | 200 | 100 | 100 | 7 | Low | 16 w | Pelvic floor muscle exercise | No | 30 min | 50% | Female sexual function | Type of delivery, perineal tear, episiotomy, duration of labor, and birth weight |
| Stafne [78] | 2012 | Norway | RCT | 761 | 396 | 365 | 2 | Mod–High | 12 w | Aerobic, strength, pelvic floor training | Yes | 60 min | 55% | Urinary and anal incontinence | Type of delivery, birth weight |
| 1 | No | 45 min | |||||||||||||
| Szumilewicz [79] | 2020 | Poland | RCT | 260 | 133 | 127 | 3 | Low–Mod | 24 w | Aerobic, resistance, pelvic floor muscle training | Yes | 60 min | - | Urinary incontinence 2 months and 1 year postpartum | Type of delivery, birth weight, duration of labor, analgesia |
| Taniguchi [80] | 2016 | Japan | RCT | 118 | 60 | 58 | 3 | Mod | 6 + w | Walk briskly | Yes | 30 min | 80% | Type of delivery, birth weight | - |
| Tomic [81] | 2013 | Croatia | RCT | 334 | 166 | 168 | 3 | 60–75% Max HR | 28 w | Aerobic exercise | Yes | 50 min | 80% | Macrosomia, birth weight, type of delivery, gestational weight gain | - |
| Uria-Minguito [82] | 2022 | Spain | RCT | 203 | 102 | 101 | 3 | 65–70% Max HR | 28 w | Aerobic exercise | Yes | 50–60 min | - | Gestational diabetes | Gestational weight gain, type of delivery, birth weight |
| Ussher [83] | 2015 | UK | RCT | 789 | 394 | 395 | 3–4 | Low | 6 w | Exercise on a treadmill | Yes | 20 min | 88.8% | Continuous smoking abstinence | Type of delivery, birth weight |
| Vinter [84] | 2011 | Denmark | RCT | 304 | 150 | 154 | 7 | Mod | 24 w | Aerobic exercise, dietary counselling | No | 30–60 min | - | Gestational weight gain | Birth weight |
| Wang [85] | 2017 | China | RCT | 226 | 112 | 114 | 3 | 55–65% Max HR | 24 w | Stationary cycling program | Yes | 45–60 min | 75% | Gestational diabetes | Birth weight, macrosomia |
| Yekefallah [86] | 2021 | Iran | RCT | 70 | 35 | 35 | 2 | Low–Mod | 11 w | Yoga | Yes | 75 min | - | Episiotomy, perineal tear, type of delivery | Birth weight, gestational age, duration of labor |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Nagpal, T.S.; Silva-José, C.; Sánchez-Polán, M.; Gil-Ares, J.; Barakat, R. Influence of Physical Activity during Pregnancy on Birth Weight: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 5421. https://doi.org/10.3390/jcm12165421
Zhang D, Nagpal TS, Silva-José C, Sánchez-Polán M, Gil-Ares J, Barakat R. Influence of Physical Activity during Pregnancy on Birth Weight: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2023; 12(16):5421. https://doi.org/10.3390/jcm12165421
Chicago/Turabian StyleZhang, Dingfeng, Taniya S. Nagpal, Cristina Silva-José, Miguel Sánchez-Polán, Javier Gil-Ares, and Rubén Barakat. 2023. "Influence of Physical Activity during Pregnancy on Birth Weight: Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 12, no. 16: 5421. https://doi.org/10.3390/jcm12165421
APA StyleZhang, D., Nagpal, T. S., Silva-José, C., Sánchez-Polán, M., Gil-Ares, J., & Barakat, R. (2023). Influence of Physical Activity during Pregnancy on Birth Weight: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 12(16), 5421. https://doi.org/10.3390/jcm12165421