
Unicompartmental Knee Arthroplasty Provides Superior Clinical and Radiological Outcomes Compared to High Tibial Osteotomy at a Follow-Up of 5–8 Years

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Hypotheses
2.3. Statistics
3. Results
3.1. Patients
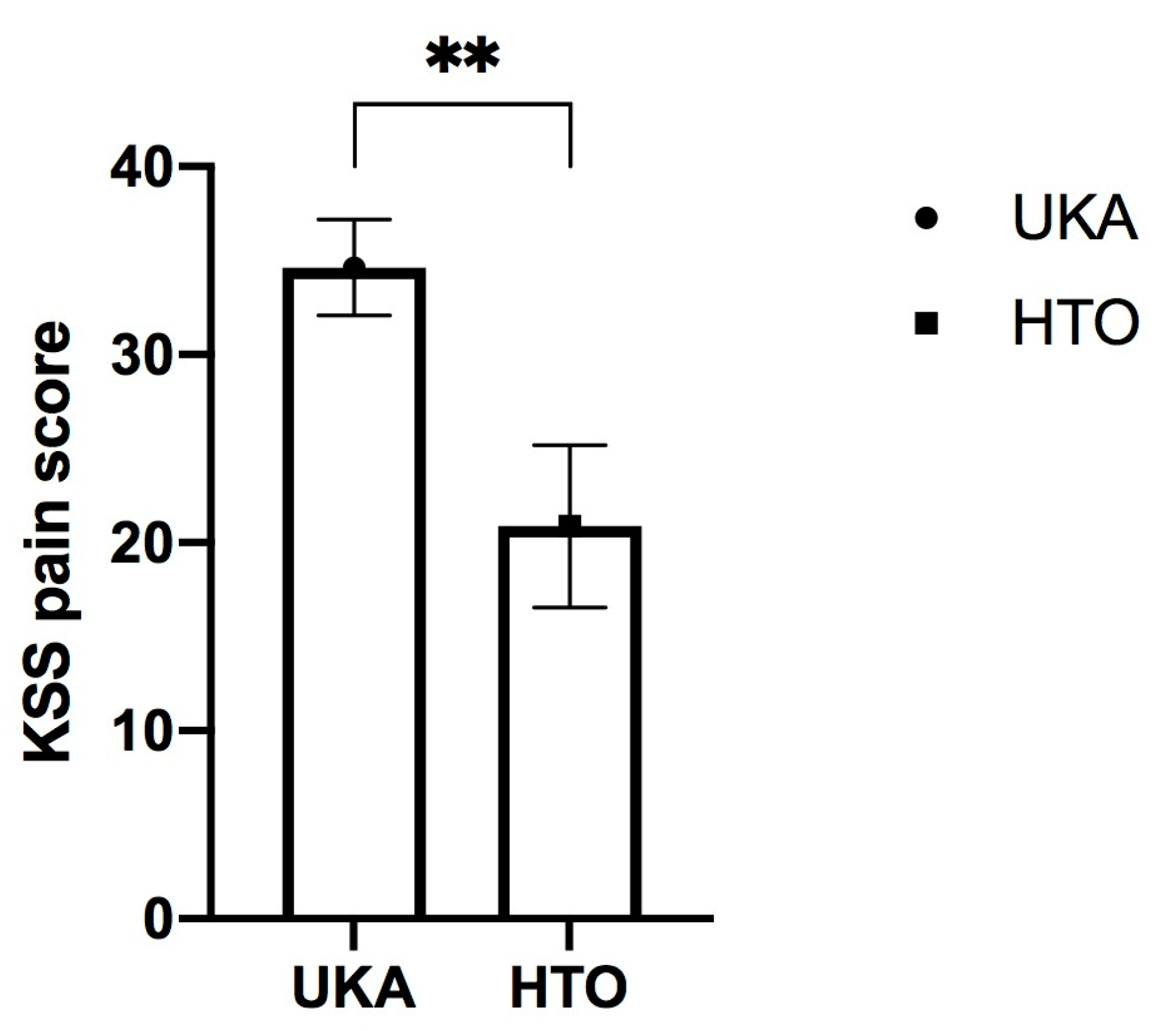
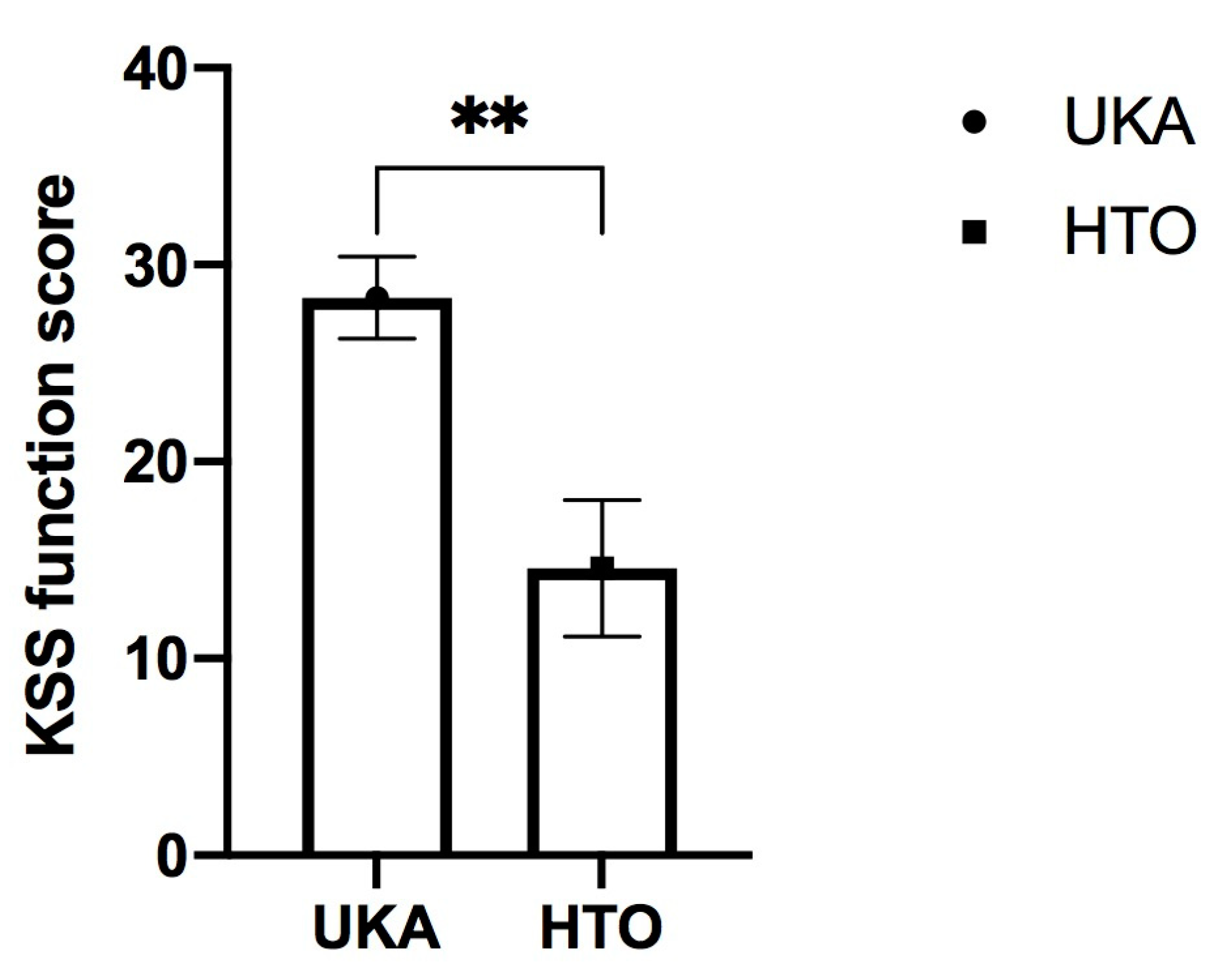
3.2. Clinical Scores
3.3. Radiological Outcome/OA Progression
3.4. Survivorship/Revision
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ledingham, J.; Regan, M.; Jones, A.; Doherty, M. Radiographic patterns and associations of osteoarthritis of the knee in patients referred to hospital. Ann. Rheum. Dis. 1993, 52, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Willis-Owen, C.A.; Brust, K.; Alsop, H.; Miraldo, M.; Cobb, J.P. Unicondylar knee arthroplasty in the UK National Health Service: An analysis of candidacy, outcome and cost efficacy. Knee 2009, 16, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Stoddart, J.C.; Dandridge, O.; Garner, A.; Cobb, J.; van Arkel, R. The compartmental distribution of knee osteoarthritis—A systematic review and meta-analysis. Osteoarthr. Cartil. 2021, 29, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Nehrer, S.; Neubauer, M.; Stotter, C. Osteoarthritis and/or Sports. Dtsch. Z. Sportmed. 2019, 70, 169–174. [Google Scholar] [CrossRef]
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis Rheum. 2008, 58, 26–35. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Koo, S.; Scanlan, S.F. Gait Mechanics Influence Healthy Cartilage Morphology and Osteoarthritis of the Knee. J. Bone Jt. Surg. Am. 2009, 91 (Suppl. S1), 95–101. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Mündermann, A.; Smith, R.L.; Alexander, E.J.; Dyrby, C.O.; Koo, S. A Framework for the in Vivo Pathomechanics of Osteoarthritis at the Knee. Ann. Biomed. Eng. 2004, 32, 447–457. [Google Scholar] [CrossRef]
- Goodell, P.B.; Johansen, P.M.; Bartels, D.W.; Sherman, S.L.; Amanatullah, D.F. Comparing Unicompartmental Knee Arthroplasty and High Tibial Osteotomy for Isolated Medial Compartment Knee Osteoarthritis. JBJS Rev. 2023, 11, e22. [Google Scholar] [CrossRef]
- Dettoni, F.; Bonasia, D.E.; Castoldi, F.; Bruzzone, M.; Blonna, D.; Rossi, R. High tibial osteotomy versus unicompartmental knee arthroplasty for medial compartment arthrosis of the knee: A review of the literature. Iowa Orthop. J. 2010, 30, 131. [Google Scholar]
- Cao, Z.; Mai, X.; Wang, J.; Feng, E.; Huang, Y. Unicompartmental Knee Arthroplasty vs High Tibial Osteotomy for Knee Osteoarthritis: A Systematic Review and Meta-Analysis. J. Arthroplast. 2018, 33, 952–959. [Google Scholar] [CrossRef]
- Yadav, A.K.; Parihar, M.; Mariani, I.; Giorgino, R.; Mangiavini, L.; Ursino, N.; D’Ambrosi, R. High tibial osteotomy with an external fixator or unicompartmental knee arthroplasty for varus knee in young patients? J. Orthop. 2022, 34, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Liddle, A.D.; Judge, A.; Pandit, H.; Murray, D.W. Adverse outcomes after total and unicompartmental knee replacement in 101 330 matched patients: A study of data from the National Joint Registry for England and Wales. Lancet 2014, 384, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Pandit, H.; Jenkins, C.; Gill, H.S.; Barker, K.; Dodd, C.A.F.; Murray, D.W. Minimally invasive Oxford phase 3 unicompartmental knee replacement: Results of 1000 cases. J. Bone Jt. Surg. Ser. B 2011, 93, 198–204. [Google Scholar] [CrossRef]
- Niama Natta, D.D.; Thienpont, E.; Bredin, A.; Salaun, G.; Detrembleur, C. Rasch analysis of the Forgotten Joint Score in patients undergoing knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1984–1991. [Google Scholar] [CrossRef]
- Kozinn, S.C.; Marx, C.; Scott, R.D. Unicompartmental knee arthroplasty: A 4.5–6-year follow-up study with a metal-backed tibial component. J. Arthroplast. 1989, 4, S1–S9. [Google Scholar] [CrossRef] [PubMed]
- Carlson, V.R.; Post, Z.D.; Orozco, F.R.; Davis, D.M.; Lutz, R.W.; Ong, A.C. When Does the Knee Feel Normal Again: A Cross-Sectional Study Assessing the Forgotten Joint Score in Patients After Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 700–703. [Google Scholar] [CrossRef]
- Kayani, B.; Konan, S.; Tahmassebi, J.; Rowan, F.E.; Haddad, F.S. An assessment of early functional rehabilitation and hospital discharge in conventional versus robotic-arm assisted unicompartmental knee arthroplasty. Bone Jt. J. 2019, 101B, 24–33. [Google Scholar] [CrossRef]
- Spahn, G.; Hofmann, G.O.; von Engelhardt, L.V.; Li, M.; Neubauer, H.; Klinger, H.M. The impact of a high tibial valgus osteotomy and unicondylar medial arthroplasty on the treatment for knee osteoarthritis: A meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 96–112. [Google Scholar] [CrossRef]
- Richmond, J.C. Surgery for Osteoarthritis of the Knee. Rheum. Dis. Clin. N. Am. 2013, 34, 815–825. [Google Scholar] [CrossRef]
- Jackson, J.P.; Waugh, W. Tibial osteotomy for osteoarthritis of the knee. J. Bone Jt. Surg. 1961, 43-B, 746–751. [Google Scholar] [CrossRef]
- Coventry, M.B. Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee: A preliminary report. J. Bone Jt. Surg. 2001, 83, 1426. [Google Scholar] [CrossRef]
- Rossi, R.; Bonasia, D.E.; Amendola, A. The Role of High Tibial Osteotomy in the Varus Knee. J. Am. Acad. Orthop. Surg. 2011, 19, 590–599. [Google Scholar] [CrossRef] [PubMed]
- W-Dahl, A.; Toksvig-Larsen, S. Cigarette smoking delays bone healingA prospective study of 200 patients operated on by the hemicallotasis technique. Acta Orthop. Scand. 2004, 75, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Amendola, A.; Bonasia, D.E. Results of high tibial osteotomy: Review of the literature. Int. Orthop. 2010, 34, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Krych, A.J.; Reardon, P.; Sousa, P.; Pareek, A.; Stuart, M.; Pagnano, M. Unicompartmental Knee Arthroplasty Provides Higher Activity and Durability Than Valgus-Producing Proximal Tibial Osteotomy at 5 to 7 Years. J. Bone Jt. Surg. 2017, 99, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Song, S.J.; Bae, D.K.; Kim, K.I.; Park, C.H. Long-term survival is similar between closed-wedge high tibial osteotomy and unicompartmental knee arthroplasty in patients with similar demographics. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1310–1319. [Google Scholar] [CrossRef]
- Brouwer, R.W.; Huizinga, M.R.; Duivenvoorden, T.; van Raaij, T.M.; Verhagen, A.P.; Bierma-Zeinstra, S.M.; Verhaar, J.A. Osteotomy for treating knee osteoarthritis. Cochrane Database Syst. Rev. 2014, 12. [Google Scholar] [CrossRef]
- Petersen, W.; Metzlaff, S. Open wedge high tibial osteotomy (HTO) versus mobile bearing unicondylar medial joint replacement: Five years results. Arch. Orthop. Trauma Surg. 2016, 136, 983–989. [Google Scholar] [CrossRef]
- Lysholm, J.; Tegner, Y. Knee injury rating scales. Acta Orthop. 2007, 78, 445–453. [Google Scholar] [CrossRef]
- Okimura, S.; Suzuki, T.; Matsumura, T.; Ikeda, Y.; Shiwaku, K.; Teramoto, A.; Yamashita, T. Patient-reported outcome measures after mobile-bearing unicompartmental knee arthroplasty were better than medial opening-wedge high tibial osteotomy in early elderly patients with severe osteoarthritis. Arch. Orthop. Trauma Surg. 2023, 1–6. [Google Scholar] [CrossRef]
- Karamitev, S.S.; Stavrev, V.P.; Chifligarov, A.G. Comparative Analysis of the results obtained after Unicondylar Knee Arthroplasty and High Tibial Osteotomy in Isolated Gonarthrosis. Folia Med. 2014, 56, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.; Li, G.; Chen, K.; Zhao, Y.; Hua, Y.; Cai, Z. Comparison of high tibial osteotomy and unicompartmental knee arthroplasty in the treatment of unicompartmental osteoarthritis. A meta-analysis. J. Arthroplast. 2013, 28, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Akagi, R.; Ninomiya, T.; Yamashita, T.; Tahara, M.; Kimura, S.; Ono, Y.; Yamaguchi, S.; Ohtori, S.; Sasho, T. Comparison of joint awareness after medial unicompartmental knee arthroplasty and high tibial osteotomy: A retrospective multicenter study. Arch. Orthop. Trauma Surg. 2022, 142, 1133–1140. [Google Scholar] [CrossRef]
- Parente, A.; Legnani, C.; Bargagliotti, M.; Marullo, M.; Romagnoli, S. Unicompartmental vs. total knee replacement in patients with failed high tibial osteotomy. Arch. Orthop. Trauma Surg. 2022, 142, 2051–2056. [Google Scholar] [CrossRef]
- Shen, G.; Shen, D.; Fang, Y.; Li, X.; Cui, L.; Wei, B.; Wu, L. Clinical Outcomes of Revision Total Knee Arthroplasty after High Tibial Osteotomy and Unicompartmental Knee Arthroplasty: A Systematic Review and Meta-Analysis. Orthop. Surg. 2022, 14, 1549–1557. [Google Scholar] [CrossRef] [PubMed]
- Serbin, P.A.; Do, D.-H.; Hinkle, A.; Wukich, D.; Huo, M.; Sambandam, S. Comparative Analysis of Unicompartmental Total Knee Arthroplasty and High Tibial Osteotomy: Time to Total Knee Arthroplasty and Other Outcome Measures. Arthroplast. Today 2023, 20, 101107. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, B.P.; Limberg, A.K.; Tibbo, M.E.; Perry, K.I.; Pagnano, M.W.; Abdel, M.P. Total Knee Arthroplasty After High Tibial Osteotomy Results in Excellent Long-Term Survivorship and Clinical Outcomes. J. Bone Jt. Surg. 2019, 101, 970–978. [Google Scholar] [CrossRef]
- Kuriyama, S.; Watanabe, M.; Sekiguchi, K.; Nakamura, S.; Nishitani, K.; Ito, H.; Matsuda, S. Differences in impact on adjacent compartments in medial unicompartmental knee arthroplasty versus high tibial osteotomy with identical valgus alignment. Knee 2021, 29, 241–250. [Google Scholar] [CrossRef]
- Smith, W.B.; Steinberg, J.; Scholtes, S.; Mcnamara, I.R. Medial compartment knee osteoarthritis: Age-stratified cost-effectiveness of total knee arthroplasty, unicompartmental knee arthroplasty, and high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 924–933. [Google Scholar] [CrossRef]
- Lee, D.C.; Byun, S.J. High Tibial Osteotomy. Knee Surg. Relat. Res. 2012, 24, 61–69. [Google Scholar] [CrossRef]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States. J. Bone Jt. Surg. Am. Vol. 2014, 97, 1386–1397. [Google Scholar] [CrossRef] [PubMed]
- Borus, T.; Thornhill, T. Unicompartmental Knee Arthroplasty. J. Am. Acad. Orthop. Surg. 2008, 16, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Kozinn, S.C.; Scott, R. Unicondylar knee arthroplasty. J. Bone Jt. Surg. 1989, 71, 145–150. [Google Scholar] [CrossRef]
- Swienckowski, J.J.; Pennington, D.W. Unicompartmental Knee Arthroplasty in Patients Sixty Years of Age or Younger. J. Bone Jt. Surg. 2004, 86, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Dell’Isola, A.; Allan, R.; Smith, S.L.; Marreiros, S.S.P.; Steultjens, M. Identification of clinical phenotypes in knee osteoarthritis: A systematic review of the literature. BMC Musculoskelet. Disord. 2016, 17, 425. [Google Scholar] [CrossRef]
- Hunter, D.J.; Collins, J.E.; Deveza, L.; Hoffmann, S.C.; Kraus, V. Biomarkers in osteoarthritis: Current status and outlook—The FNIH Biomarkers Consortium PROGRESS OA study. Skeletal Radiol. 2023, 1–17. [Google Scholar] [CrossRef]
- Minas, T.; Gomoll, A.H.; Solhpour, S.; Rosenberger, R.; Probst, C.; Bryant, T. Autologous Chondrocyte Implantation for Joint Preservation in Patients with Early Osteoarthritis. Clin. Orthop. Relat. Res. 2010, 468, 147–157. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| UKA | HTO | ||
|---|---|---|---|
| n | 61 | 25 | |
| age | Mean | 57.418 | 52.017 |
| SEM | ±0.7267 | ±1.1972 | |
| p-value (∆ at baseline) | 0.000 * | ||
| BMI | mean | 30.23 | 28.84 |
| SEM | ±0.705 | ±1.008 | |
| p-value (∆ at baseline) | 0.279 | ||
| Sex | m:f | 21:40 | 19:6 |
| % m:f | 34.4%:65.6% | 76.0%:24.0% | |
| p-value (∆ at baseline) | 0.000 * | ||
| UKA | HTO | p-Value | Favors | ||||
|---|---|---|---|---|---|---|---|
| Category | Mean | SEM | Mean | SEM | |||
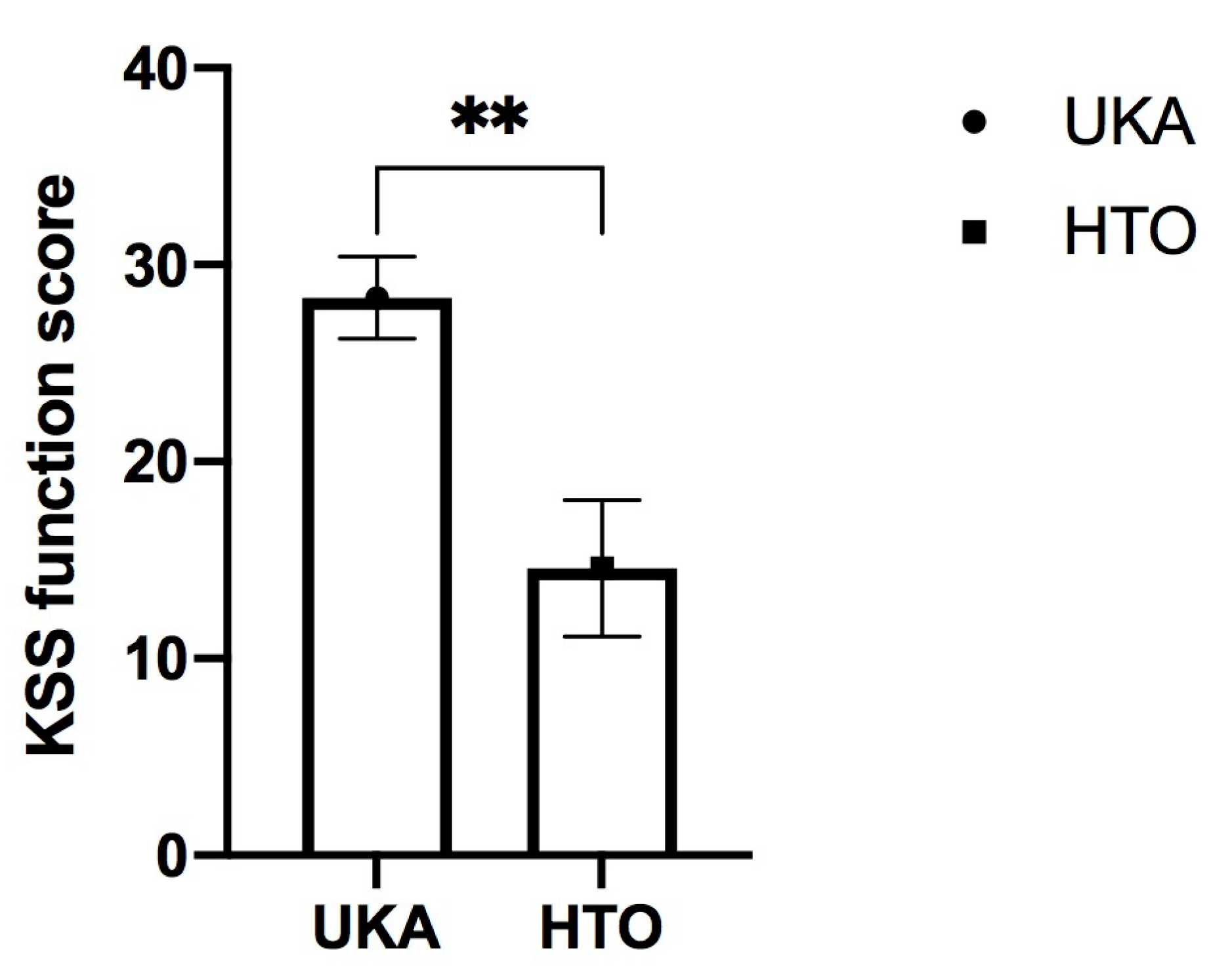
| KSS | ∆KSS function | 28.3333 | ±2.0913 | 14.5833 | ±3.4567 | 0.001 * | UKA |
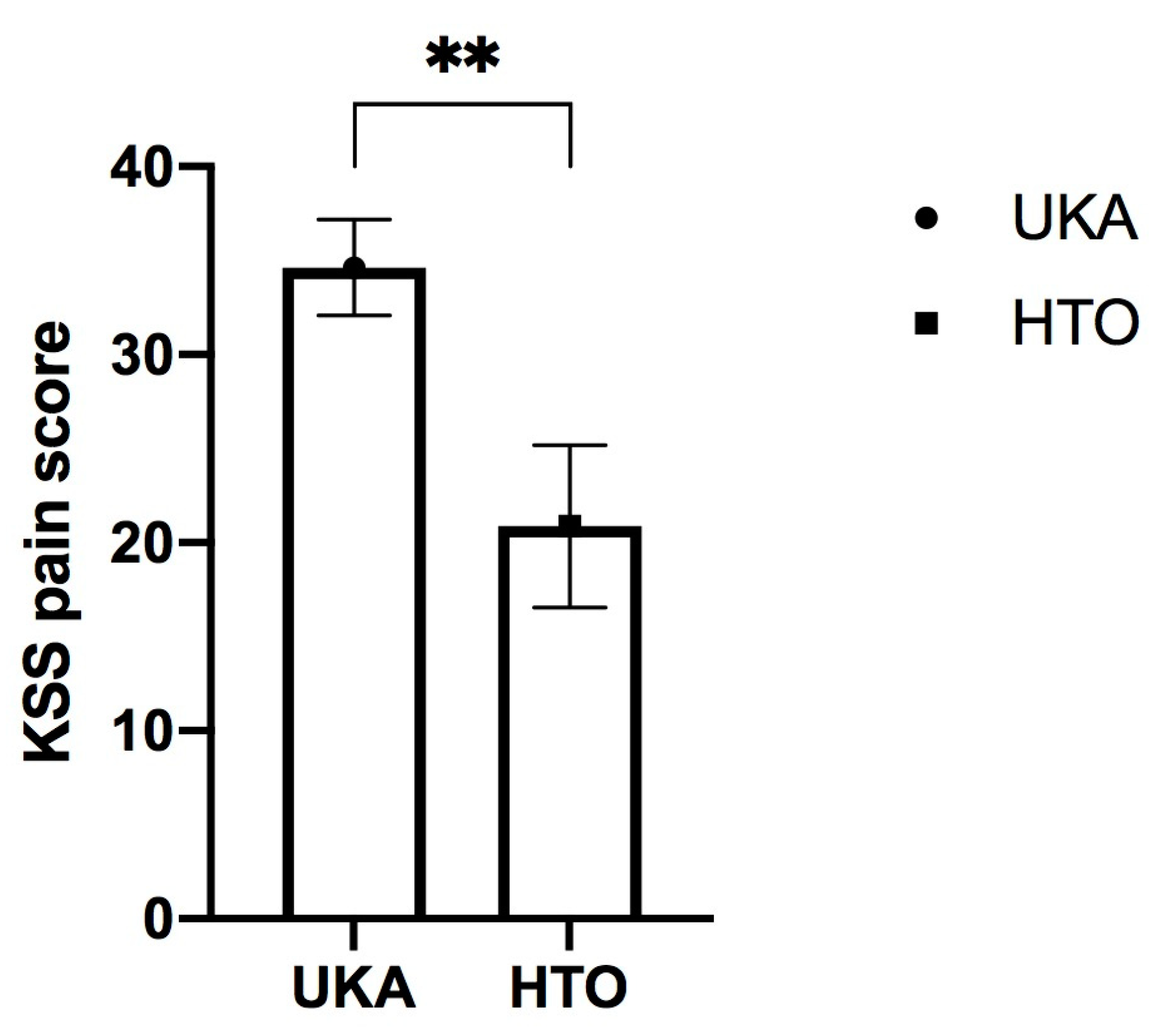
| ∆KSS pain | 34.6271 | ±2.5539 | 20.8750 | ±4.3181 | 0.006 * | UKA | |
| ROM (post OP) | ROM flexion | 120.16 | ±1.248 | 125.00 | ±2.102 | 0.056 | n.s. |
| SF36 (post OP) | KSK | 45.674869 | ±1.1122 | 46.982712 | ±1.8764 | 0.537 | n.s. |
| PSK | 48.298241 | ±1.4709 | 52.580000 | ±2.0149 | 0.092 | n.s. | |
| Tegner | 4.16 | ±0.139 | 4.76 | ±0.296 | 0.077 | n.s. |
| Category | UKA | HTO | p-Value | Favors | ||
|---|---|---|---|---|---|---|
| OA Progression (KL-Based) | Yes | No | Yes | No | ||
| n | 22 | 37 | 14 | 7 | 0.02 * | UKA |
| % intra-group | 37.3 | 62.7 | 66.7 | 33.3 | ||
| Category | UKA | HTO | p-Value | Favors | ||
|---|---|---|---|---|---|---|
| Revision | Yes | No | Yes | No | ||
| n | 4 | 57 | 6 | 18 | 0.018 * | UKA |
| % intra-group | 6.6 | 93.4 | 25.0 | 75.0 | ||
| revision method | 3 × TKR, 1 × PE | 5 × TKR, 1 × UKA | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neubauer, M.; Reinberger, E.-M.; Dammerer, D.; Moser, L.B.; Neugebauer, J.; Gottsauner-Wolf, F.; Nehrer, S. Unicompartmental Knee Arthroplasty Provides Superior Clinical and Radiological Outcomes Compared to High Tibial Osteotomy at a Follow-Up of 5–8 Years. J. Clin. Med. 2023, 12, 5387. https://doi.org/10.3390/jcm12165387
Neubauer M, Reinberger E-M, Dammerer D, Moser LB, Neugebauer J, Gottsauner-Wolf F, Nehrer S. Unicompartmental Knee Arthroplasty Provides Superior Clinical and Radiological Outcomes Compared to High Tibial Osteotomy at a Follow-Up of 5–8 Years. Journal of Clinical Medicine. 2023; 12(16):5387. https://doi.org/10.3390/jcm12165387
Chicago/Turabian StyleNeubauer, Markus, Eva-Maria Reinberger, Dietmar Dammerer, Lukas B. Moser, Johannes Neugebauer, Florian Gottsauner-Wolf, and Stefan Nehrer. 2023. "Unicompartmental Knee Arthroplasty Provides Superior Clinical and Radiological Outcomes Compared to High Tibial Osteotomy at a Follow-Up of 5–8 Years" Journal of Clinical Medicine 12, no. 16: 5387. https://doi.org/10.3390/jcm12165387
APA StyleNeubauer, M., Reinberger, E.-M., Dammerer, D., Moser, L. B., Neugebauer, J., Gottsauner-Wolf, F., & Nehrer, S. (2023). Unicompartmental Knee Arthroplasty Provides Superior Clinical and Radiological Outcomes Compared to High Tibial Osteotomy at a Follow-Up of 5–8 Years. Journal of Clinical Medicine, 12(16), 5387. https://doi.org/10.3390/jcm12165387