

Development of a Novel Prediction Model for Red Blood Cell Transfusion Risk in Cardiac Surgery

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- -
- Sociodemographic and anthropometric characteristics: age, sex, weight, height, body mass index (BMI) and body surface area (BSA).
- -
- Clinical and personal history: comorbidities and toxic habits.
- -
- Cardiovascular risk factors: diabetes mellitus, arterial hypertension, dyslipidemia and EuroSCORE I. EuroSCORE II, which is the current risk metric for surgery-related mortality within 30 days, was not used in this study as our objective was to compare against the current transfusion risk model [8].
- -
- Variables included in EuroSCORE I: chronic obstructive pulmonary disease (COPD), previous cardiac surgery, extracardiac arteriopathy, neurological dysfunction, serum creatinine >200 μmol/L, active infectious endocarditis, unstable angina, left ventricle ejection fraction (LVEF), recent myocardial infarction, pulmonary hypertension, surgery other than CABG, surgery on the thoracic aorta and post-infarct septal rupture.
- -
- Variables related to the surgical intervention: time of extracorporeal circulation, complications. The surgical procedure was classified into three categories: one procedure, when patients underwent valvular surgery or CABG surgery; combined procedures when patients underwent a combined procedure like valve–valve surgery or valve–CABG surgery and other cardiac procedures, including other cardiothoracic procedures.
- -
- Other variables related to transfusion control: need for transfusion of red blood cell concentrates, number of concentrates transfused, other blood products, pro-hemostatic and ACTA–PORT score.
3. Results
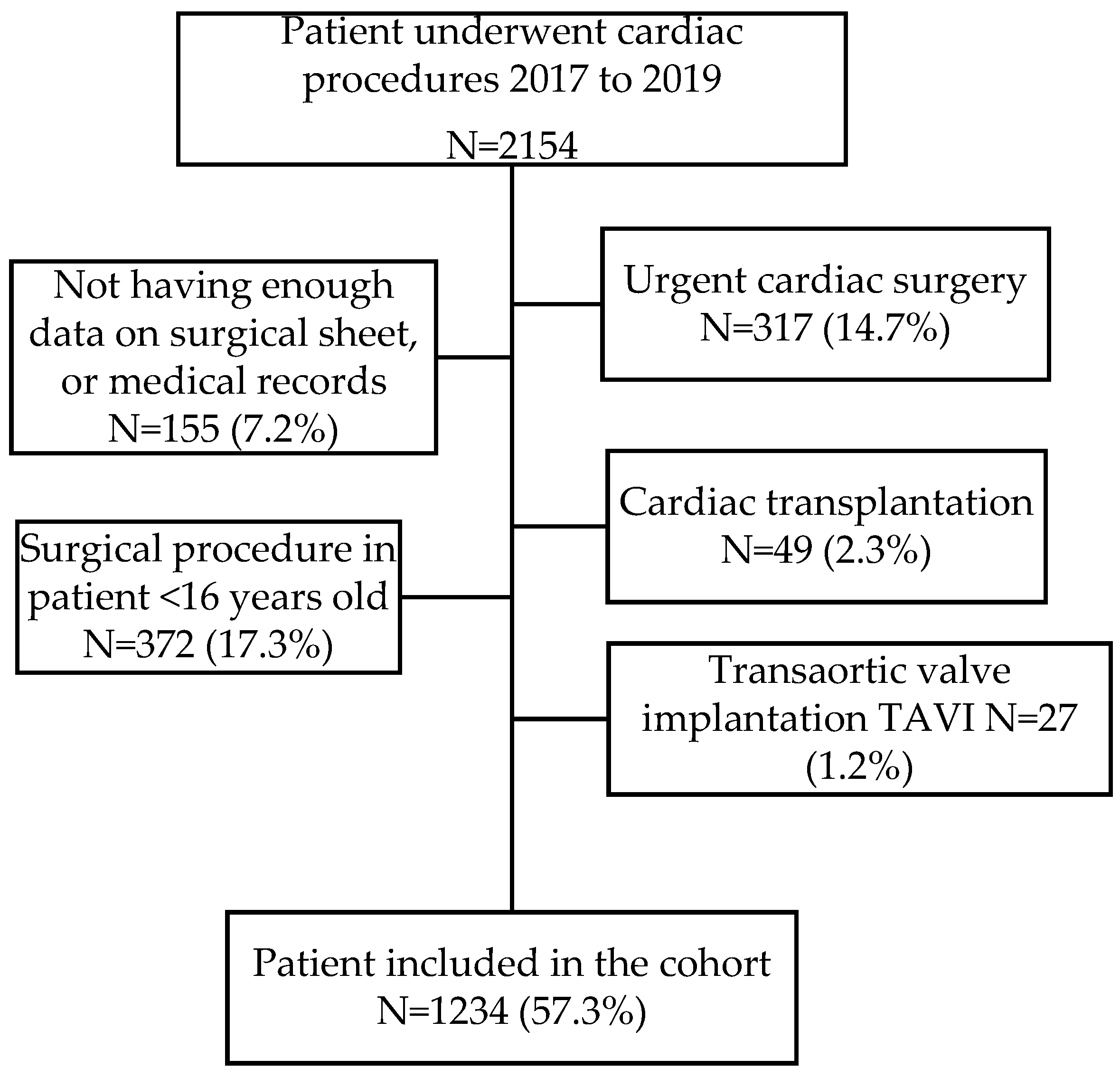
3.1. Characteristics of the Cohort
3.2. Risk Factors Associated with Red Blood Cell Transfusion in Cardiac Surgery
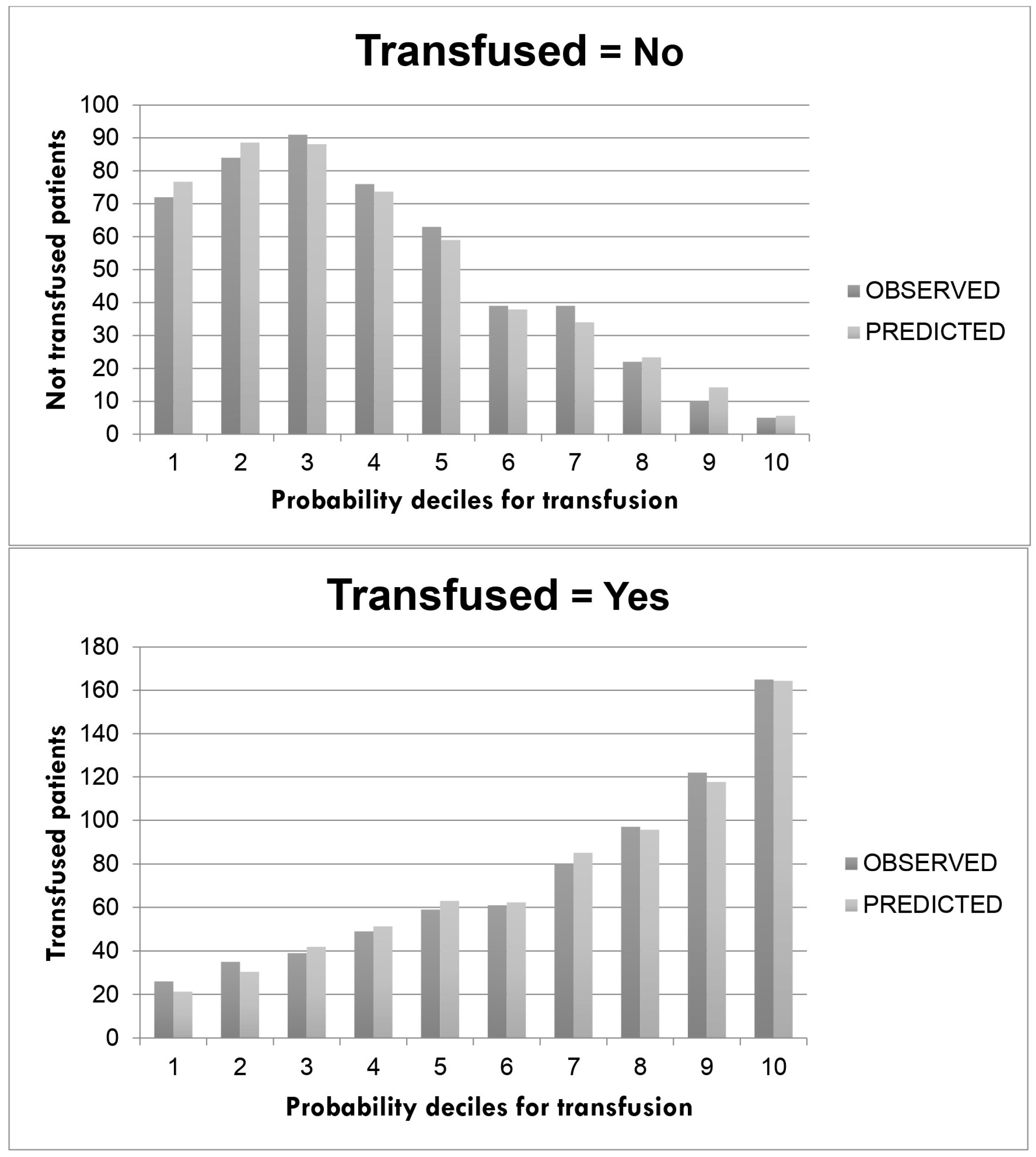
3.3. Prediction Model of the Risk of Red Blood Cell Transfusion in Cardiac Surgery
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raphael, J.; Mazer, C.D.; Wilkey, A.; Subramani, S.; Schroeder, A.; Abdalla, M.; Ferreira, R.; Roman, P.E.; Welsby, I.; Greilich, P.E.; et al. Corrigendum to ‘Society of Cardiovascular Anesthesiologists (SCA) Clinical Practice Improvement (CPI) Advisory for Management of Perioperative Bleeding and Hemostasis in Cardiac Surgery Patients. J. Cardiothorac. Vasc. Anesth. 2020, 34, 840–841. [Google Scholar] [CrossRef]
- Engoren, M.C.; Habib, R.H.; Zacharias, A.; Schwann, T.A.; Riordan, C.J.; Durham, S.J. Effect of blood transfusion on long-term survival after cardiac operation. Ann. Thorac. Surg. 2002, 74, 1180–1186. [Google Scholar] [CrossRef]
- Shaw, R.E.; Johnson, C.K.; Ferrari, G.; Brizzio, M.E.; Sayles, K.; Rioux, N.; Zapolanski, A.; Grau, J.B. Blood transfusion in cardiac surgery does increase the risk of 5-year mortality: Results from a contemporary series of 1714 propensity-matched patients. Transfusion 2014, 54, 1106–1113. [Google Scholar] [CrossRef]
- Horvath, K.A.; Acker, M.A.; Chang, H.; Bagiella, E.; Smith, P.K.; Iribarne, A.; Kron, I.L.; Lackner, P.; Argenziano, M.; Ascheim, D.D.; et al. Blood transfusion and infection after cardiac surgery. Ann. Thorac. Surg. 2013, 95, 2194–2201. [Google Scholar] [CrossRef]
- Johnson, D.J.; Scott, A.V.; Barodka, V.M.; Park, S.; Wasey, J.O.; Ness, P.M.; Gniadek, T.; Frank, S.M. Morbidity and Mortality after High-dose Transfusion. Anesthesiology 2016, 124, 387–395. [Google Scholar] [CrossRef]
- Al-Khabori, M.; Al-Riyami, A.Z.; Mukaddirov, M.; Al-Sabti, H. Transfusion indication predictive score: A proposed risk stratification score for perioperative red blood cell transfusion in cardiac surgery. Vox Sang. 2014, 107, 269–275. [Google Scholar] [CrossRef]
- Goudie, R.; Sterne, J.A.C.; Verheyden, V.; Bhabra, M.; Ranucci, M.; Murphy, G.J. Risk scores to facilitate preoperative prediction of transfusion and large volume blood transfusion associated with adult cardiac surgery. Br. J. Anaesth. 2015, 114, 757–766. [Google Scholar] [CrossRef]
- Klein, A.; Collier, T.; Yeates, J.; Miles, L.; Fletcher, S.; Evans, C.; Richards, T. The ACTA PORT-score for predicting perioperative risk of blood transfusion for adult cardiac surgery. Br. J. Anaesth. 2017, 119, 394–401. [Google Scholar] [CrossRef]
- Pajares, A.; Larrea, L.; Zarragoikoetexea, I.; Tur, A.; Vicente, R.; Argente, P. Patient blood management in cardiac surgery: Results. Rev. Española Anestesiol. Reanim. (English Ed.) 2018, 65, 196–203. [Google Scholar] [CrossRef]
- Alghamdi, A.A.; Davis, A.; Brister, S.; Corey, P.; Logan, A. Development and validation of Transfusion Risk Understanding Scoring Tool (TRUST) to stratify cardiac surgery patients according to their blood transfusion needs. Transfusion 2006, 46, 1120–1129. [Google Scholar] [CrossRef]
- Ranucci, M.; Castelvecchio, S.; Frigiola, A.; Scolletta, S.; Giomarelli, P.; Biagioli, B. Predicting transfusions in cardiac surgery: The easier, the better: The Transfusion Risk and Clinical Knowledge score. Vox Sang. 2009, 96, 324–332. [Google Scholar] [CrossRef]
- Da Cunha, C.B.C.; Monteiro, V.S.; de Magalhães Ferraz, D.L.; Tchaick, R.M.; de Carvalho Júnior, J.D.; Silva, I.T.C.; Figueira, F.A.M.D.S.; Andrade, L.B. Validation of Blood Transfusion Risk Scores (TRACK and TRUST) in a Cardiac Surgery Service in Brazil. Braz. J. Cardiovasc. Surg. 2023, 38, 227–234. [Google Scholar] [CrossRef]
- Madhu Krishna, N.R.; Nagaraja, P.S.; Singh, N.G.; Nanjappa, S.N.; Kumar, K.N.; Prabhakar, V.; Manjunatha, N. Evaluation of Risk Scores in Predicting Perioperative Blood Transfusions in Adult Cardiac Surgery. Ann. Card. Anaesth. 2019, 22, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lemeshow, S.; Gauducheau, E.; Roques, F.; Nashef, S.A.M.; Michel, P.; Salamon, R. European system for cardiac operative risk eval-uation (EuroSCORE). Eur. J. Cardio-Thoracic. Surg. 1999, 16, 9–13. [Google Scholar]
- Vlot, E.A.; Vernooij, L.M.; Loer, S.A.; van Dongen, E.P.; Noordzij, P.G. External Validation of the ACTA-PORT Transfusion Risk Score in Older Cardiac Surgery Patients at Risk of Frailty. J. Cardiothorac. Vasc. Anesth. 2022, 36, 2983–2990. [Google Scholar] [CrossRef] [PubMed]
- Leff, J.; Romano, C.A.; Gilbert, S.; Nair, S. Validation Study of the Transfusion Risk and Clinical Knowledge (TRACK) Tool in Cardiac Surgery Patients: A Retrospective Analysis. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2669–2675. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, J.; Bithell, J. Bootstrap Confidence Intervals: When, Which, What? A Practical Guide for Medical Statisticians. Stat. Med. 2000, 19, 1141–1164. [Google Scholar] [CrossRef]
- Kleinbaum, D.G.; Kleinbaum, D.G. Applied Regression Analysis and Other Multivariable Methods; Cengage Learning: Boston, MA, USA, 2008; ISBN 9780495384960. [Google Scholar]
- Bulus, M. Pwrss: Statistical Power and Sample Size Calculation Tools. R Package Version 0.3.1. 2023. Available online: https://CRAN.R-project.org/package=pwrss (accessed on 1 August 2023).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 1 August 2023).
- Karkouti, K.; Yau, T.M.; Scott Beattie, W.; Callum, J.; Cheng, D.; Dupuis, J.-Y.; Kent, B.; Laflamme, C.; Légaré, J.-F.; Mazer, D.; et al. Prediction of massive blood transfusion in cardiac surgery. Can. J. Anesth. 2006, 53, 781–794. [Google Scholar] [CrossRef]
- Hardy, J.-F.; Perrault, J.; Tremblay, N.; Robitaille, D.; Blain, R.; Carrier, M. The stratification of cardiac surgical procedures according to use of blood products: A retrospective analysis of 1480 cases. Can. J. Anaesth. 1991, 38, 511–517. [Google Scholar] [CrossRef]
- Reid, C.; Billah, B.; Dinh, D.; Smith, J.; Skillington, P.; Yii, M.; Seevanayagam, S.; Mohajeri, M.; Shardey, G. An Australian risk prediction model for 30-day mortality after isolated coronary artery bypass: The AusSCORE. J. Thorac. Cardiovasc. Surg. 2009, 138, 904–910. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhang, L.; Li, X.; Hu, S. SinoSCORE: A logistically derived additive prediction model for post-coronary artery bypass grafting in-hospital mortality in a Chinese population. Front. Med. China 2013, 7, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Moorthy, V.; Liu, W.; Chew, S.T.H.; Ti, L.K. Impact of diabetes on outcomes of cardiac surgery in a multiethnic Southeast Asian population. Diabetes Vasc. Dis. Res. 2019, 16, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Aronson, S.; Dyke, C.M.; Stierer, K.A.; Levy, J.H.; Cheung, A.T.; Lumb, P.D.; Kereiakes, D.J.; Newman, M.F. The ECLIPSE trials: Comparative studies of clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for acute hypertension treatment in cardiac surgery patients. Obstet. Anesth. Dig. 2008, 107, 1110–1121. [Google Scholar] [CrossRef] [PubMed]
- Vuylsteke, A.; Pagel, C.; Gerrard, C.; Reddy, B.; Nashef, S.; Aldam, P.; Utley, M. The Papworth Bleeding Risk Score: A stratification scheme for identifying cardiac surgery patients at risk of excessive early postoperative bleeding. Eur. J. Cardio-Thoracic Surg. 2011, 39, 924–930. [Google Scholar] [CrossRef]
- Semple, J.W.; Rebetz, J.; Kapur, R. Transfusion-associated circulatory overload and transfusion-related acute lung injury. Blood Am. Soc. Hematol. 2019, 133, 1840–1853. [Google Scholar] [CrossRef]
- Koch, C.G.; Li, L.; Sessler, D.I.; Figueroa, P.; Hoeltge, G.A.; Mihaljevic, T.; Blackstone, E.H. Duration of Red-Cell Storage and Complications after Cardiac Surgery. N. Engl. J. Med. 2008, 358, 1229–1239. [Google Scholar] [CrossRef]
- Voorhuis, F.T.R.; Dieleman, J.M.; de Vooght, K.M.K.; van Dijk, D.; van Herwerden, L.A.; Peelen, L.M.; van Klei, W.A. Storage time of red blood cell concentrates and adverse outcomes after cardiac surgery: A cohort study. Ann. Hematol. 2013, 92, 1701–1706. [Google Scholar] [CrossRef]
- Xiao, K.; Zhao, F.; Liu, Q.; Jiang, J.; Chen, Z.; Gong, W.; Zheng, Z.; Le, A. Effect of red blood cell storage duration on outcomes of isolated traumatic brain injury. Med. Sci. Monit. 2020, 26, e923448-1–e923448-9. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total N = 1234 | |
|---|---|
| Age (years), median, (IQR) | 66 (58.0; 73.0) |
| Sex male, n (%) | 789 (63.9) |
| BMI, median, (IQR) | 28.2 (25.3; 31.8) |
| BSA median, (IQR) | 1.8 (1.7; 2.0) |
| Preoperative Hb (g/dL), median, (IQR) | 13.0 (11.7; 14.2) |
| Serum creatinine (μmol/L), preoperative median, (IQR) | 0.9 (0.8; 1.1) |
| EuroSCORE I median, (IQR) | 4.4 (2.4; 7.0) |
| Current smoker | 227 (18.4) |
| High blood pressure, n (%) | 803 (65.1) |
| Diabetes mellitus, n (%) | 387 (31.4) |
| Dyslipidemia, n (%) | 629 (51.0) |
| Surgery, n (%) | |
| One procedure | 857 (69.4) |
| Combined surgery | 119 (9.6) |
| Other procedures | 258 (20.9) |
| Patient transfused, n (%) | 733 (59.4) |
| Median number of transfusions | 1 (0; 2) |
| ACTA–PORT score median, (IQR) | 15 (10; 18) |
| Median time of extracorporeal circulation (min), (IQR) | 109 (85; 140) |
| Median time of ICU stay (days) (IQR) | 3 (2; 4) |
| Median time of hospital stay median (days) (IQR) | 14 (9; 24) |
| Mortality, n (%) | 57 (4.6) |
| One Procedure N = 857 | Combined Procedure N = 119 | Other Procedures N = 258 | |||||
|---|---|---|---|---|---|---|---|
| N (%) | CI 95.0% | N (%) | CI 95.0% | N (%) | CI 95.0% | p-Value | |
| Age (years), median, (IQR) | 66 (59; 73) | (66; 68) | 69 (64; 75) | (67; 72) | 60 (46; 69) | (56; 63) | <0.001 |
| Sex male, n (%) | 554 (64.6) | (61.4; 67.8) | 74 (62.2) | (53.3; 70.5) | 161 (62.4) | (56.4; 68.1) | 0.738 |
| BMI, median, (IQR) | 28.2 (25.3; 27.9) | (27.9; 28.7) | 28.2 (25.3; 31.9) | (27.5; 29.4) | 28.3 (25; 31.9) | (27.6; 29.4) | 0.904 |
| BSA, median | 1.8 (1.7; 2.0) | (1.8; 1.8) | 1.8 (1.7; 2.0) | (1.8; 1.9) | 1.9 (1.7; 2.0) | (1.8; 1.9) | 0.143 |
| Preoperative Hb (g/dL), median, (IQR) | 13.0 (11.8; 14.2) | (12.9; 13.2) | 12.2 (11; 13.5) | (11.9; 12.6) | 13.5 (12; 14.6) | (13.3; 13.8) | <0.001 |
| Serum creatinine (μmol/L), preoperative median, (IQR) | 0.95 (0.8; 1.15) | (0.94; 0.97) | 0.96 (0.82; 1.15) | (0.9; 1.04) | 0.92 (0.79; 1.10) | (0.89; 0.97) | 0.129 |
| EuroSCORE I median, (IQR) | 3.90 (2.27; 6.30) | (3.73; 4.09) | 4.99 (3.29; 7.88) | (4.2; 5.5) | 5.48 (3.29; 10.36) | (5.41; 6.35) | <0.001 |
| Current smoker | 165 (19.3) | (16.7; 22.0) | 18 (15.1) | (9.6; 22.4) | 44 (17.1) | (12.8; 22.0) | 0.249 |
| High blood pressure, n (%) | 585 (68.3) | (65.1; 71.3) | 85 (71.4) | (62.9; 79.0) | 133 (51.6) | (45.4; 57.6) | <0.001 |
| Diabetes mellitus, n (%) | 304 (35.5) | (32.3; 38.7) | 62 (52.1) | (43.2; 60.9) | 21 (8.1) | (5.3; 11.9) | <0.001 |
| Dyslipidemia, n (%) | 472 (55.1) | (51.8; 58.4) | 79 (66.4) | (57.6; 74.4) | 78 (30.2) | (24.9; 36.0) | <0.001 |
| Patient transfused, n (%) | 491 (57.3) | (54; 60.6) | 103 (86.6) | (79.6; 91.8) | 139 (53.9) | (47.8; 59.9) | <0.001 |
| Median number of transfusions | 1 (0; 2) | (1; 2) | 2 (1; 3) | (2; 3) | 0 (0; 2) | . | <0.001 |
| ACTA–PORT score median, (IQR) | 15 (11; 18) | (15; 16) | 19 (15; 23) | (18; 21) | 12 (8; 16) | (11; 13) | <0.001 |
| Median time of extracorporeal circulation (min), (IQR) | 100 (81; 127) | (98; 103) | 133.5 (113; 156) | (125; 140) | 133.5 (94; 178) | (125; 145) | <0.001 |
| Median time of ICU stay (days) (IQR) | 3 (2; 4) | (3; 4) | 4 (2; 5) | (4; 5) | 3 (2; 5) | (3; 4) | 0.002 |
| Median time of hospital stay median (days) (IQR) | 14 (9; 24) | (13; 15) | 17 (12; 28) | (16; 22) | 12 (9; 22) | (11; 15) | <0.001 |
| Mortality n (%) | 30 (3.5) | (2.4; 4.9) | 12 (10.1) | (5.6; 16.4) | 15 (5.8) | (3.43; 9.2) | 0.004 |
| Total N = 1234 | Not Transfused N = 501 | Transfused N = 733 | p-Value | |
|---|---|---|---|---|
| Age (years), median, (IQR) | 66 (58.0; 73.0) | 63 (54; 71) | 67 (61; 74) | <0.001 |
| Sex male, n (%) | 789 (63.9) | 382(76.2) | 407 (55) | <0.001 |
| BMI, median, (IQR) | 28.2 (25.3; 31.8) | 29 (25.8; 32) | 28.01 (25.0; 31.6) | 0.013 |
| BSA, median | 1.8 (1.7; 2.0) | 1.94 (1.80; 2.07) | 1.83 (1.69; 1.99) | <0.001 |
| Preoperative Hb (g/dL), median, (IQR) | 13.0 (11.7; 14.2) | 14.1 (13.2; 15) | 12.2 (11; 13.3) | <0.001 |
| Serum creatinine (μmol/L), preoperative median, (IQR) | 0.9 (0.8; 1.1) | 0.92 (0.79; 1.18) | 0.97 (0.79; 1.18) | 0.028 |
| EuroSCORE I median, (IQR) | 4.4 (2.4; 7.0) | 3.51 (2.1; 5.5) | 5.13 (3.13; 8.1) | <0.001 |
| Current smoker | 227 (18.4) | 95 (19.0) | 132 (18.0) | 0.671 |
| High blood pressure, n (%) | 803 (65.1) | 284 (56.7) | 519 (70.8) | <0.001 |
| Diabetes mellitus, n (%) | 387 (31.4) | 124 (24.8) | 263 (35.9) | <0.001 |
| Dyslipidemia, n (%) | 629 (51.0) | 223 (44.5) | 406 (55.5) | <0.001 |
| Surgery, n (%) | <0.001 | |||
| One procedure | 857 (69.4) | 366 (73.1) | 491 (67.0) | |
| Combined surgery | 119 (9.6) | 16 (3.2) | 103 (14.1) | |
| Other procedures | 258 (20.9) | 119 (23.8) | 139 (19.0) | |
| ACTA–PORT score, median, (IQR) | 15 (10; 18) | 11 (9; 14) | 17 (13; 20) | <0.001 |
| Median time of extracorporeal circulation (min), (IQR) | 109 (85; 140) | 100 (78; 128) | 118 (89; 148) | <0.001 |
| Median time of ICU stay (days), (IQR) | 3 (2; 4) | 2 (2; 4) | 3 (2; 5) | <0.001 |
| Median time of hospital stay median (days), (IQR) | 14 (9; 24) | 10 (9; 15) | 19 (11; 28) | <0.001 |
| Mortality, n (%) | 57 (4.6) | 0 (0) | 57 (7.8) | <0.001 |
| β | Standard Error | OR | CI 95% | p Value | |
|---|---|---|---|---|---|
| Hb preoperative | |||||
| ≥14 g/dL | 1 | <0.001 | |||
| 13–13.9 g/dL | 0.74 | 0.17 | 2.11 | 1.50; 2.97 | <0.001 |
| 12–12.9 g/dL | 1.58 | 0.19 | 4.88 | 3.34; 7.10 | <0.001 |
| 11–11.9 g/dL | 2.38 | 0.25 | 10.89 | 6.69; 17.72 | <0.001 |
| <11 g/dL | 3.94 | 0.43 | 51.41 | 21.97; 120.27 | <0.001 |
| Surgery | |||||
| One procedure | 1 | ||||
| Combined surgery | 1.38 | 0.30 | 3.97 | (2.19; 7.17) | <0.001 |
| BMI | |||||
| BMI <30 | 1 | ||||
| BMI ≥30 | 0.38 | 0.14 | 1.46 | (1.10; 1.93) | <0.001 |
| Sex | |||||
| Men | 1 | ||||
| Women | 0.51 | 0.15 | 1.67 | (1.24; 2.24) | 0.001 |
| Age | |||||
| <60 | 1 | ||||
| ≥60 | 0.31 | 0.15 | 1.37 | (1.02; 1.83) | 0.033 |
| Constant | −1.46 | 0.18 | 0.23 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Tuñón, O.; Bertomeu-Cornejo, M.; Castillo-Cantero, I.; Borrego-Domínguez, J.M.; García-Cabrera, E.; Bejar-Prado, L.; Vilches-Arenas, A. Development of a Novel Prediction Model for Red Blood Cell Transfusion Risk in Cardiac Surgery. J. Clin. Med. 2023, 12, 5345. https://doi.org/10.3390/jcm12165345
Alonso-Tuñón O, Bertomeu-Cornejo M, Castillo-Cantero I, Borrego-Domínguez JM, García-Cabrera E, Bejar-Prado L, Vilches-Arenas A. Development of a Novel Prediction Model for Red Blood Cell Transfusion Risk in Cardiac Surgery. Journal of Clinical Medicine. 2023; 12(16):5345. https://doi.org/10.3390/jcm12165345
Chicago/Turabian StyleAlonso-Tuñón, Ordoño, Manuel Bertomeu-Cornejo, Isabel Castillo-Cantero, José Miguel Borrego-Domínguez, Emilio García-Cabrera, Luis Bejar-Prado, and Angel Vilches-Arenas. 2023. "Development of a Novel Prediction Model for Red Blood Cell Transfusion Risk in Cardiac Surgery" Journal of Clinical Medicine 12, no. 16: 5345. https://doi.org/10.3390/jcm12165345
APA StyleAlonso-Tuñón, O., Bertomeu-Cornejo, M., Castillo-Cantero, I., Borrego-Domínguez, J. M., García-Cabrera, E., Bejar-Prado, L., & Vilches-Arenas, A. (2023). Development of a Novel Prediction Model for Red Blood Cell Transfusion Risk in Cardiac Surgery. Journal of Clinical Medicine, 12(16), 5345. https://doi.org/10.3390/jcm12165345