
Teeth Damage during General Anesthesia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Pico
2.1.1. Patient, Population, or Problem
- -
- Adult patients undergoing general anesthesia and teeth damage.
2.1.2. Intervention or Exposure
- -
- To see how many times patients got injured with the air way method.
2.1.3. Comparison
- -
- Intubation vs. Insertion supraglottic device.
2.1.4. Outcome
- -
- Frequency of oral injury.
2.2. Research Strategy
2.3. Eligibility Criteria
2.4. Study Selection and Data Collection
2.5. Risk of Bias in Included Studies
2.6. Synthesis of Evidence
3. Results
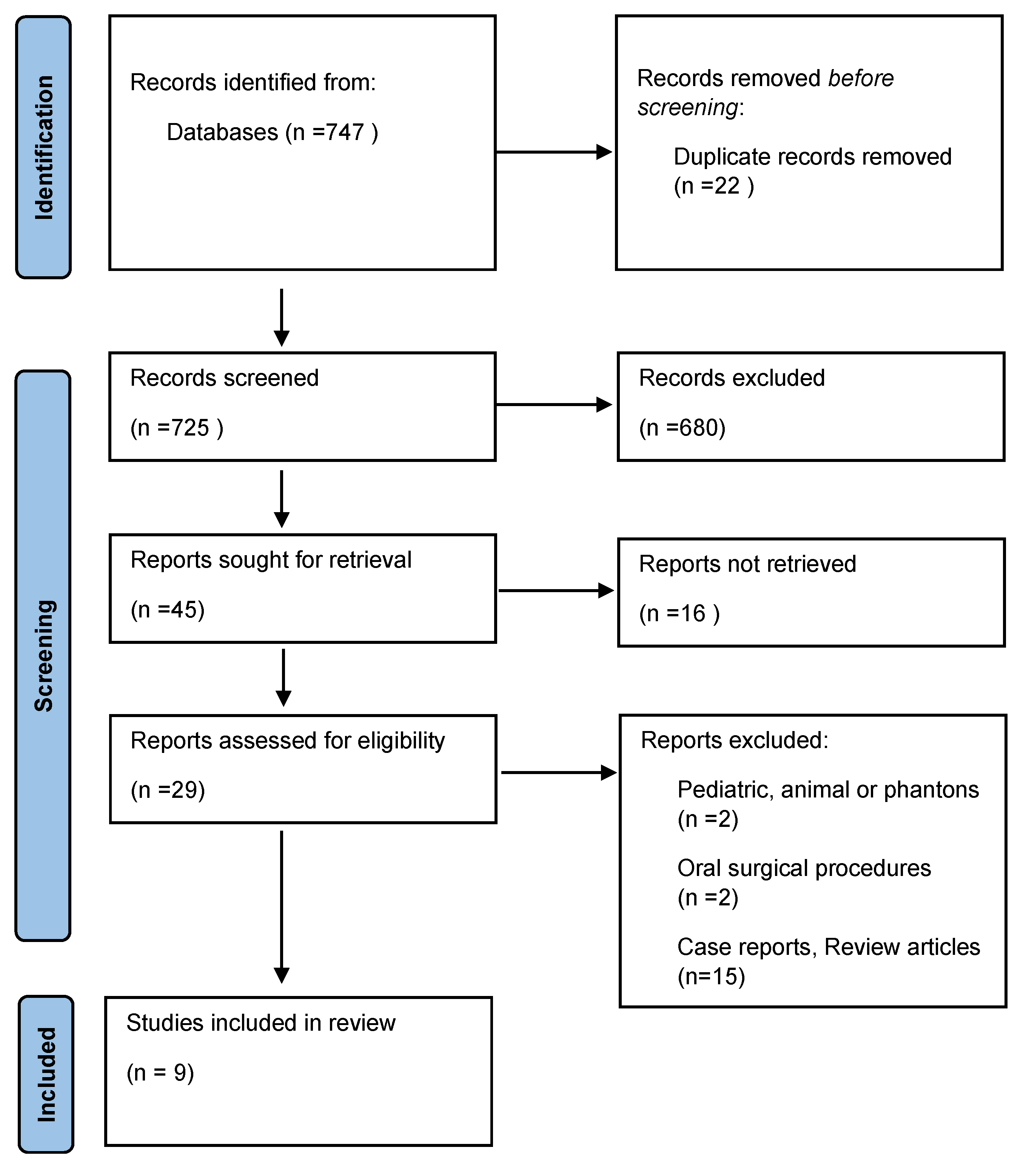
3.1. Search Strategy
3.2. Types of Tooth Injury
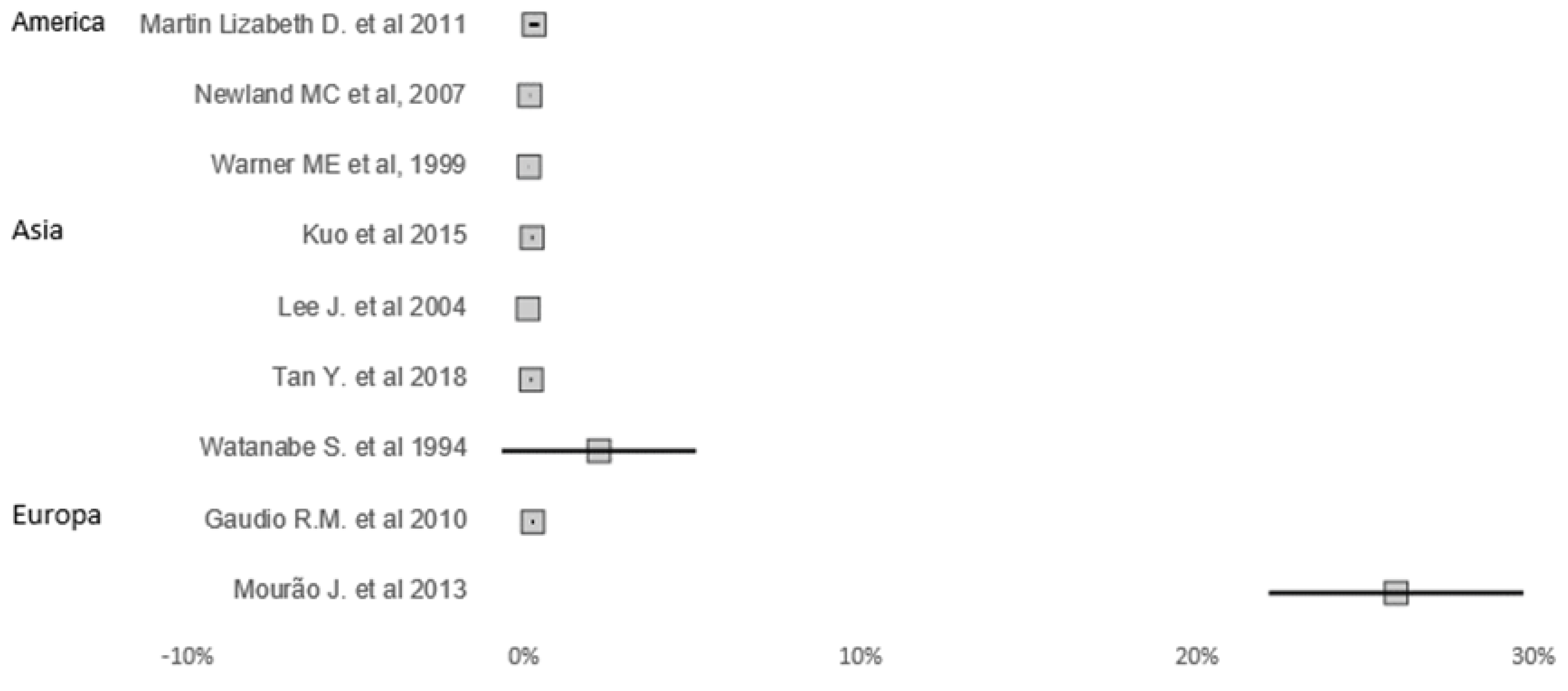
3.3. Types of Airways Management and Teeth Damage
3.4. Teeth Affected
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ansari, S.; Rajpurohit, V.; Dev, V. Dental Trauma due To Intubating during General Anaesthesia: Incidence, Risks Factors, and Prevention. Oral Health Dent. Manag. 2016, 15, 377. [Google Scholar]
- Sahni, V. Dental considerations in anaesthesia. JRSM Open 2016, 7, 2054270416675082. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Divaris, K. Hidden consequences of dental trauma: The social and psychological effects. Pediatr. Dent. 2009, 31, 96–101. [Google Scholar]
- Zitzmann, N.; Krastl, G.; Weiger, R.; Kühl, S.; Sendi, P. Cost-effectiveness of Anterior Implants versus Fixed Dental Prostheses. J. Dent. Res. 2013, 92 (Suppl. 12), 183S–188S. [Google Scholar] [CrossRef]
- Talwar, J.S.; Gaiser, R.R. Dental injury during general anesthesia and those who seek financial compensation: A retrospective study. J. Clin. Anesth. 2020, 63, 109757. [Google Scholar] [CrossRef]
- de Sousa, J.M.; Mourão, J.I. Tooth injury in anaesthesiology. Braz. J. Anesthesiol. 2015, 65, 511–518. [Google Scholar] [PubMed]
- Nuzzolese, E.; Innocenzi, F.; Santovito, D.; Lupariello, F. Dental Injuries During General Anesthesia: Risk Management and Forensic Perspectives. In Proceedings of the 74th AAFS Annual Scientific Meeting, Seattle, WA, USA, 21–25 February 2022; pp. 707–708. [Google Scholar]
- Yasny, J.S. Perioperative Dental Considerations for the Anesthesiologist. Obstet. Anesth. Dig. 2009, 108, 1564–1573. [Google Scholar] [CrossRef]
- Silva, D.; Miranda, R.; Ferreira, I.; Braga, A.; Mourão, J.; Pina-Vaz, I. Validation of a Suggested Pre-Operative Protocol for the Prevention of Traumatic Dental Injuries during Oroendotracheal Intubation: A Pilot Study. Appl. Sci. 2023, 13, 2091. [Google Scholar] [CrossRef]
- Fukuda, T.; Sugimoto, Y.; Yamashita, S.; Toyooka, H.; Tanaka, M. Forces applied to the maxillary incisors during tracheal intubation and dental injury risks of intubation by beginners: A manikin study. Acta Anaesthesiol. Taiwanica 2011, 49, 12–15. [Google Scholar] [CrossRef]
- Diakonoff, H.; De Rocquigny, G.; Tourtier, J.; Guigon, A. Medicolegal issues of peri-anaesthetic dental injuries: A 21-years review of liability lawsuits in France. Dent. Traumatol. 2022, 38, 391–396. [Google Scholar] [CrossRef]
- Burton, J.F.; Baker, A.B. Dental Damage during Anaesthesia and Surgery. Anaesth. Intensiv. Care 1987, 15, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kim, S.-Y.; Park, K.-M.; Yang, S.; Kim, K.-D.; Park, W. Evaluation of dental status using a questionnaire before administration of general anesthesia for the prevention of dental injuries. J. Dent. Anesth. Pain. Med. 2023, 23, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessment. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Mourão, J.; Neto, J.; Luís, C.; Moreno, C.; Barbosa, J.; Carvalho, J.; Tavares, J. Dental injury after conventional direct laryngoscopy: A prospective observational study. Anaesthesia 2013, 68, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Newland, M.C.; Ellis, S.J.; Peters, K.R.; Simonson, J.A.; Durham, T.M.; Ullrich, F.A.; Tinker, J.H. Dental injury associated with anesthesia: A report of 161,687 anesthetics given over 14 years. J. Clin. Anesth. 2007, 19, 339–345. [Google Scholar] [CrossRef]
- Warner, M.E.; Benenfeld, S.M.; Warner, M.A.; Schroeder, D.R.; Maxson, P.M. Perianesthetic dental injuries: Frequency, outcomes, and risk factors. Anesthesiologists 1999, 90, 1302–1305. [Google Scholar] [CrossRef]
- Martin, L.D.; Mhyre, J.M.; Shanks, A.M.; Tremper, K.K.; Kheterpal, S. 3423 emergency tracheal intubations at a university hospital: Airway outcomes and complications. Anesthesiology 2011, 114, 42–48. [Google Scholar] [CrossRef]
- Tan, Y.; Loganathan, N.; Thinn, K.K.; Liu, E.H.C.; Loh, N.-H.W. Dental injury in anaesthesia: A tertiary hospital’s experience. BMC Anesthesiol. 2018, 18, 108. [Google Scholar] [CrossRef]
- Lee, J.; Choi, J.H.; Lee, Y.K.; Kim, E.S.; Kwon, O.K.; Hastings, R.H. The callander laryngoscope blade modification is associated with a decreased risk of dental contact. Can. J. Anaesth. 2004, 51, 181–184. [Google Scholar] [CrossRef]
- Watanabe, S.; Suga, A.; Asakura, N.; Takeshima, R.; Kimura, T.; Taguchi, N.; Kumagai, M. Determination of the distance between the laryngoscope blade and the upper incisors during direct laryngoscopy: Comparisons of a curved, an angulated straight, and two straight blades. Anesth. Analg. 1994, 79, 638–641. [Google Scholar] [CrossRef]
- Kuo, Y.W.; Lu, I.C.; Yang, H.Y.; Chiu, S.L.; Hsu, H.T.; Cheng, K.I. Quality improvement program reduces perioperative dental injuries—A review of 64,718 anesthetic patients. J. Chin. Med. Assoc. 2016, 79, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Rosa Maria, G.; Paolo, F.; Stefania, B.; Letizia, T.; Martina, A.; Massimiliano, D.; Carlo, O.; Maria, A.F. Traumatic dental injuries during anaesthesia: Part I: Clinical evaluatio. Dent. Traumatol. 2010, 26, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Nouette-Gaulain, K.; Lenfant, F.; Jacquet-Francillon, D.; Belbachir, A.; Bournigault-Nuquet, A.; Choquet, O.; Claisse, A.; Dujarric, F.; Francon, D.; Gentili, M.; et al. French clinical guidelines for prevention of perianaesthetic dental injuries: Long text. Ann. Fr. Anesth. Reanim. 2012, 31, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.E.; Baekgaard, J.S.; Rasmussen, L.S. Dental injuries in relation to general anaesthesia—A retrospective study. Acta Anaesthesiol. Scand. 2019, 63, 993–1000. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Author, Year of Publication | Title | Aim of the Study | Type of Airway Management | Total Quality Score | Types of Tooth Injury | Most Tooth Affected | Conclusions |
|---|---|---|---|---|---|---|---|
| Newland MC et al., 2007 [8] | Dental injury associated with anesthesia: a report of 161,687 anesthetics given over 14 years | Determine the frequency, outcomes, and risk factors for dental injury related to anesthesia. | Mask only; Oral intubation; Nasal intubation; LMA; Tracheostomy |  | Enamel fracture; Subluxation; Luxation; Avulsion; Crown Fracture; Crown and root fracture; Missing tooth/teeth; Other injury | Upper central incisors | Dental injury is one of the most common adverse events reported in association with anesthesia. Risk factors include preexisting poor dentition or reconstructive work and moderately difficult to difficult intubation [8]. |
| Warner ME et al., 1999 [9] | Perianesthetic dental injuries: frequency, outcomes, and risk factors | Determine the frequency, outcomes, and risk factors for perianesthetic dental injuries | Laryngoscopy, tracheal intubation | | Crown fractures, Partial dislocations | Upper incisors | Based on these data from a large surgical population at a single training institution, approximately 1:4500 patients who receive anesthesia services sustain a dental injury that required repair or extraction. Patients most at risk for perianesthetic dental injury include those with preexisting poor dentition who have one or more risk factors for difficult laryngoscopy and tracheal intubation [9]. |
| Martin Lizabeth D. et al., 2011 [10] | 3423 Emergency Tracheal Intubations at a University Hospital Airway Outcomes and Complications | Evaluate the incidence of difficult intubation and complication rates and to determine predictors of complications in this setting | Aspiration, Esophageal intubation, and Oropharyngeal |  | During emergent nonoperative intubation, specific clinical situations are associated with an increased risk of airway complication and may provide a starting point for allocation of experienced first responders [10]. | ||
| Tan Y. et al., 2018 [11] | Dental injury in anesthesia: a tertiary hospital’s experience | Evaluate the incidence, risk factors, and local practices in the management of perioperative dental injuries in Singapore | three types of Supraglottic airway devices (SADs): all videolaryngoscopy was carried out using the McGrath Mac laryngoscopy |  | Avulsion and Crown Fractured | Upper right and left incisors | Videolaryngoscopy with the McGrath MAC is associated with an increased likelihood of dental injury. This could be either because videolarygoscopes were used when increased risk of dental trauma was anticipated, or due to incorrect technique of laryngoscopy. Future studies should be performed to establish the causality. The management of dental injuries could be improved with development of departmental guidelines [11]. |
| Mourão J. et al., 2013 [12] | Dental injury after conventional direct laryngoscopy: a prospective observational study | Overcome some of the previous limitations and determine a more accurate incidence of dental damage and risk factors after conventional direct laryngoscopy for tracheal intubation | Laryngoscopy for tracheal intubation | | Enamel Fracture, Avulsed | Upper central incisor | Finally, given the high rate of reported injury with conventional laryngoscopy, it would be important to repeat our methodology using other intubation devices, such as videolaryngoscopes, to assess if the rate of injury is different [12]. |
| Lee J. et al., 2004 [13] | The Callander laryngoscope blade modification is associated with a decreased risk of dental contact | Determine whether preoperative examination could predict the risk of contacting the teeth with the laryngoscope and to evaluate the effectiveness of a modified Macintosh blade on reducing dental 7 contact | Laryngoscopy | | Airway characteristics correlate with the risk of hitting the upper teeth during laryngoscopy. The modified Macintosh blade reduces the risk of contacting the teeth [13]. | ||
| Watanabe S. et al., 1994 [14] | Determination of the distance Between the Laryngoscope Blade and the Upper Incisors During Direct Laryngoscopy: Comparisons of a Curved, an Angulated Straight, and Two Straight Blades | Compare the heel-tooth distance when the optimum visibility of the glottis was obtained using the four different types of laryngoscope blade: a Miller, a Wisconsin with a higher heel than a Miller, a Macintosh, and a Belscope blade | Laryngoscopy | | Fracture and Subluxation | Central incisor | In conclusion, a low-heeled angulated straight blade, the Belscope blade, provides a significantly greater field of view between the posterior end of the blade and the upper teeth than other types of blades. It may therefore contribute to a reduced likelihood of upper dental injuries during laryngoscopy [14]. |
| Kuo et al., 2015 [15] | Quality improvement program reduces perioperative dental injuries e A review of 64,718 anesthetic patients | Reduce the incidence of perioperative dental injury. | LMA | | Subluxation; Luxation; Avulsion; Crown Fracture; Damage to fixed partial denture, Missing tooth, other injury | Upper central incisor | Dental injury incidence was significantly reduced and remained at low levels after implementation of the quality improvement program. We suggest the implementation of a standardized dental examination into the preoperative evaluation system adding pathologic teeth fixed or protected devices to minimize dental injury associated with anesthesia [15]. |
| Gaudio R.M. et al., 2010 [16] | Traumatic dental injuries during anesthesia: part I: clinical evaluation | Investigate the main characteristics of the dental injuries identified by an anesthesiology incident reporting and constituting a body of malpractice claims. | Tracheal intubation | | Avulsions, damage to crowns and bridgeworks, Luxation, Teeth fractures, Bulk fractures | Upper central incisor | Even though the majority of anesthesiologists were trained enough in the use of airway devices and aware of the potential damage while using excessive forces, some unexpected difficulties may have led to lesions. It is known that damage to teeth can occur even in the absence of negligence [16]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neto, J.M.; Teles, A.R.; Barbosa, J.; Santos, O. Teeth Damage during General Anesthesia. J. Clin. Med. 2023, 12, 5343. https://doi.org/10.3390/jcm12165343
Neto JM, Teles AR, Barbosa J, Santos O. Teeth Damage during General Anesthesia. Journal of Clinical Medicine. 2023; 12(16):5343. https://doi.org/10.3390/jcm12165343
Chicago/Turabian StyleNeto, João M., Ana Rita Teles, Joselina Barbosa, and Orquídea Santos. 2023. "Teeth Damage during General Anesthesia" Journal of Clinical Medicine 12, no. 16: 5343. https://doi.org/10.3390/jcm12165343
APA StyleNeto, J. M., Teles, A. R., Barbosa, J., & Santos, O. (2023). Teeth Damage during General Anesthesia. Journal of Clinical Medicine, 12(16), 5343. https://doi.org/10.3390/jcm12165343