
Outcome of Facial Burn Injuries Treated by a Nanofibrous Temporary Epidermal Layer
 , ,
, ,  , ,
, , 
Abstract
1. Background
2. Materials and Methods
2.1. Study Design
2.2. Preparation and Application of SpinCare™
2.3. Outcome Assessment
3. Results
3.1. Data
3.1.1. Patients
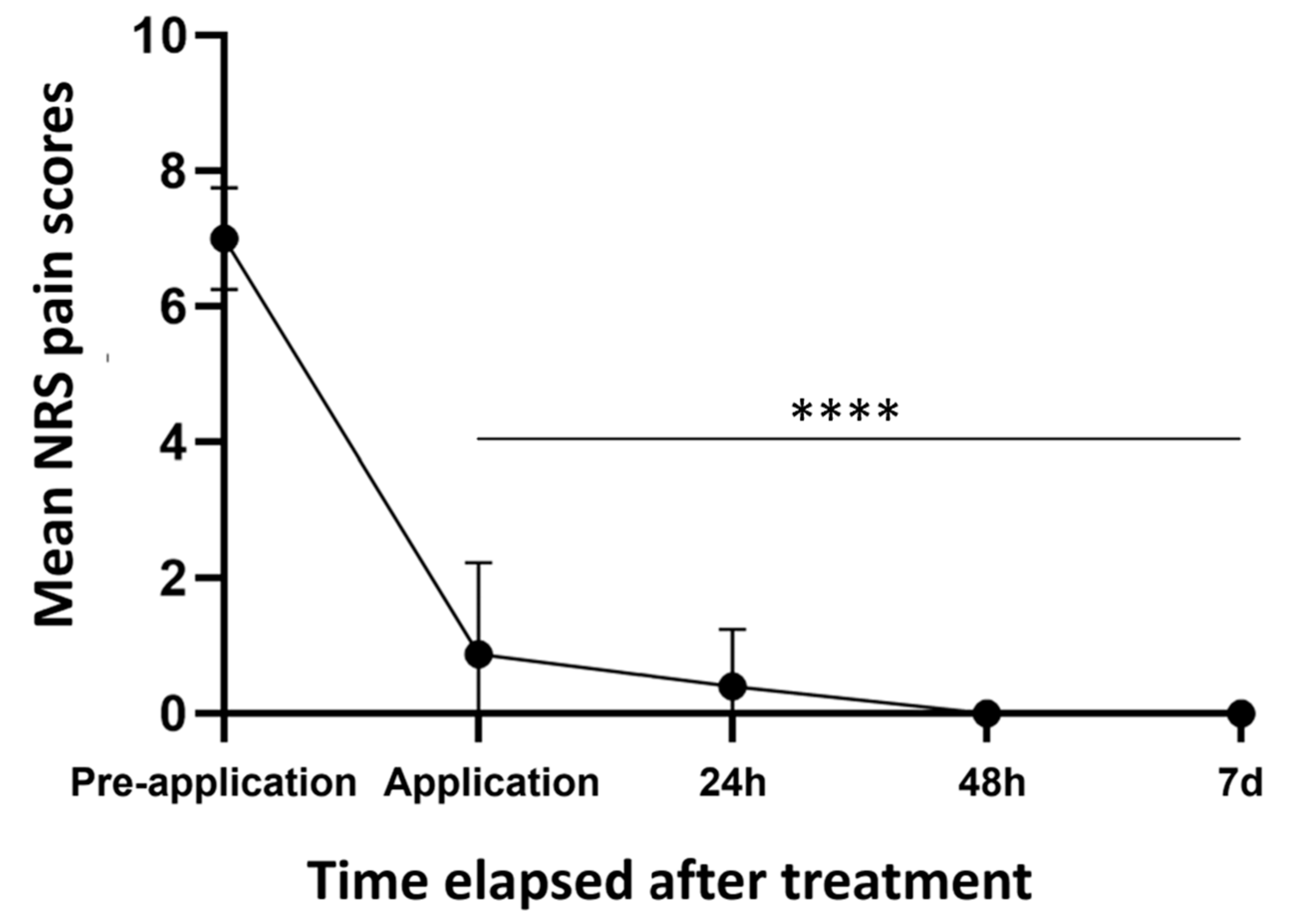
3.1.2. Pain Scores
3.1.3. Healing Time
3.1.4. Functional and Aesthetic Outcomes
3.1.5. Application and Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clark, C.; Ledrick, D.; Moore, A. Facial Burns; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hoogewerf, C.J.; van Baar, M.E.; Hop, M.J.; Bloemen, M.C.; Middelkoop, E.; Nieuwenhuis, M.K. Burns to the head and neck: Epidemiology and predictors of surgery. Burns 2013, 39, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Hoogewerf, C.J.; van Baar, M.E.; Middelkoop, E.; van Loey, N.E. Impact of facial burns: Relationship between depressive symptoms, self-esteem and scar severity. Gen. Hosp. Psychiatry 2014, 36, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Duteille, F.; Perrot, P. Management of 2nd-degree facial burns using the Versajet((R)) hydrosurgery system and xenograft: A prospective evaluation of 20 cases. Burns 2012, 38, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.M.; Lee, A.; Stoddard, F.J., Jr.; Li, N.C.; Schneider, J.C.; Shapiro, G.D.; Griggs, C.L.; Wang, C.; Palmieri, T.; Meyer, W.J., 3rd; et al. The Effect of Facial Burns on Long-Term Outcomes in Young Adults: A 5-Year Study. J. Burn Care Res. 2018, 39, 497–506. [Google Scholar] [CrossRef]
- Ren, Z.; Chang, W.C.; Zhou, Q.; Wang, Y.; Wang, H.; Hu, D. Recovery of lost face of burn patients, perceived changes, and coping strategies in the rehabilitation stage. Burns 2015, 41, 1855–1861. [Google Scholar] [CrossRef]
- Greenhalgh, D.G. Management of facial burns. Burns Trauma 2020, 8, tkaa023. [Google Scholar] [CrossRef]
- Friedstat, J.S.; Klein, M.B. Acute management of facial burns. Clin. Plast. Surg. 2009, 36, 653–660. [Google Scholar] [CrossRef]
- Arno, A.; Barret, J.P.; Harrison, R.A.; Jeschke, M.G. Face allotransplantation and burns: A review. J. Burn Care Res. 2012, 33, 561–576. [Google Scholar] [CrossRef]
- Leon-Villapalos, J.; Jeschke, M.G.; Herndon, D.N. Topical management of facial burns. Burns 2008, 34, 903–911. [Google Scholar] [CrossRef]
- Yildirim, R.; Guner, A.; Cekic, A.B.; Usta, M.A.; Ulusahin, M.; Turkyilmaz, S. Outcomes of the Use of Hyaluronic Acid-Based Wound Dressings for the Treatment of Partial-Thickness Facial Burns. J. Burn Care Res. 2023, 44, 551–554. [Google Scholar] [CrossRef]
- Bujang-Safawi, E.; Halim, A.S.; Khoo, T.L.; Dorai, A.A. Dried irradiated human amniotic membrane as a biological dressing for facial burns—A 7-year case series. Burns 2010, 36, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Longinotti, C. The use of hyaluronic acid based dressings to treat burns: A review. Burns Trauma 2014, 2, 162–168. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Aretz, F.G.; Fuchs, P.C.; Lefering, R.; Yary, P.; Oplander, C.; Schulz, A.; Daniels, M. Comparison of Long-Term Skin Quality and Scar Formation in Partial-Thickness Burn Wounds Treated with Suprathel((R)) and epicite(hydro(R)) Wound Dressings. Medicina 2022, 58, 1550. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Fuchs, P.C.; Heitzmann, W.; Kanho, C.H.; Schiefer, J.L. Our Initial Experience In The Customized Treatment Of Donor Site And Burn Wounds With A New Nanofibrous Temporary Epidermal Layer. Ann. Burns Fire Disasters 2021, 34, 58–66. [Google Scholar] [PubMed]
- Chen, S.; Li, R.; Li, X.; Xie, J. Electrospinning: An enabling nanotechnology platform for drug delivery and regenerative medicine. Adv. Drug Deliv. Rev. 2018, 132, 188–213. [Google Scholar] [CrossRef]
- Nanomedic. Spincare. 2020. Available online: https://nanomedic.com/research/#research_pest (accessed on 1 January 2020).
- Nedomansky, J.; Oramary, A.; Nickl, S.; Fuchs, G.; Radtke, C.; Haslik, W.; Fochtmann-Frana, A. Treatment of partial thickness burns of the face with Acticoat7: A retrospective single center study. Wien. Klin. Wochenschr. 2021, 133, 202–208. [Google Scholar] [CrossRef]
- Jeschke, M.G.; van Baar, M.E.; Choudhry, M.A.; Chung, K.K.; Gibran, N.S.; Logsetty, S. Burn injury. Nat. Rev. Dis. Primers 2020, 6, 11. [Google Scholar] [CrossRef]
- Greenhalgh, D.G. Management of Burns. New Engl. J. Med. 2019, 380, 2349–2359. [Google Scholar] [CrossRef]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef]
- Beausang, E.; Floyd, H.; Dunn, K.W.; Orton, C.I.; Ferguson, M.W. A new quantitative scale for clinical scar assessment. Plast. Reconstr. Surg. 1998, 102, 1954–1961. [Google Scholar] [CrossRef]
- Hoogewerf, C.J.; Hop, M.J.; Nieuwenhuis, M.K.; Oen, I.M.; Middelkoop, E.; Van Baar, M.E. Topical treatment for facial burns. Cochrane Database Syst. Rev. 2020, 7, CD008058. [Google Scholar] [CrossRef]
- Tang, H.; Lv, G.; Fu, J.; Niu, X.; Li, Y.; Zhang, M.; Zhang, G.; Hu, D.; Chen, X.; Lei, J.; et al. An open, parallel, randomized, comparative, multicenter investigation evaluating the efficacy and tolerability of Mepilex Ag versus silver sulfadiazine in the treatment of deep partial-thickness burn injuries. J. Trauma Acute Care Surg. 2015, 78, 1000–1007. [Google Scholar] [CrossRef]
- Heyneman, A.; Hoeksema, H.; Vandekerckhove, D.; Pirayesh, A.; Monstrey, S. The role of silver sulphadiazine in the conservative treatment of partial thickness burn wounds: A systematic review. Burns 2016, 42, 1377–1386. [Google Scholar] [CrossRef]
- Chaganti, P.; Gordon, I.; Chao, J.H.; Zehtabchi, S. A systematic review of foam dressings for partial thickness burns. Am. J. Emerg. Med. 2019, 37, 1184–1190. [Google Scholar] [CrossRef] [PubMed]
- Schiefer, J.L.; Rath, R.; Ahrens, E.; Grigutsch, D.; Graff, I.; Stromps, J.P.; Fuchs, P.C.; Schulz, A. Evaluation of scar quality after treatment of superficial burns of the hands and face with Dressilk or Biobrane-An intra-individual comparison. Burns 2018, 44, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Singer, A.J.; McClain, S.A. The effects of a high-potency topical steroid on cutaneous healing of burns in pigs. Acad. Emerg. Med. 2002, 9, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Haik, J.; Kornhaber, R.; Blal, B.; Harats, M. The Feasibility of a Handheld Electrospinning Device for the Application of Nanofibrous Wound Dressings. Adv. Wound Care 2017, 6, 166–174. [Google Scholar] [CrossRef]
- Gao, C.; Zhang, L.; Wang, J.; Jin, M.; Tang, Q.; Chen, Z.; Cheng, Y.; Yang, R.; Zhao, G. Electrospun nanofibers promote wound healing: Theories, techniques, and perspectives. J. Mater. Chem. B 2021, 9, 3106–3130. [Google Scholar] [CrossRef]
- Mi, H.Y.; Salick, M.R.; Jing, X.; Crone, W.C.; Peng, X.F.; Turng, L.S. Electrospinning of unidirectionally and orthogonally aligned thermoplastic polyurethane nanofibers: Fiber orientation and cell migration. J. Biomed. Mater. Res. A 2015, 103, 593–603. [Google Scholar] [CrossRef]
- Dubsky, M.; Kubinova, S.; Sirc, J.; Voska, L.; Zajicek, R.; Zajicova, A.; Lesny, P.; Jirkovska, A.; Michalek, J.; Munzarova, M.; et al. Nanofibers prepared by needleless electrospinning technology as scaffolds for wound healing. J. Mater. Sci. Mater. Med. 2012, 23, 931–941. [Google Scholar] [CrossRef]
- Mosier, M.J.; Gibran, N.S. Surgical excision of the burn wound. Clin. Plast. Surg. 2009, 36, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Engrav, L.H.; Heimbach, D.M. Early reconstruction of facial burns. West J. Med. 1991, 154, 203–204. [Google Scholar] [PubMed]
- Engrav, L.H.; Heimbach, D.M.; Walkinshaw, M.D.; Marvin, J.A. Excision of burns of the face. Plast. Reconstr. Surg. 1986, 77, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.K.; Engrav, L.H.; Heimbach, D.M.; Gibran, N.S.; Costa, B.A.; Nakamura, D.Y.; Moore, M.L.; Blayney, C.B.; Hoover, C.L. Early excision and grafting of face and neck burns in patients over 20 years. Plast. Reconstr. Surg. 2002, 109, 1266–1273. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Score | |
|---|---|---|
| Color | Perfect | 1 |
| Slight mismatch | 2 | |
| Obvious mismatch | 3 | |
| Gross mismatch | 4 | |
| Finish | Matte | 1 |
| Shiny | 2 | |
| Contour | Flush with surrounding skin | 1 |
| Slightly proud/indented | 2 | |
| Hypertrophic | 3 | |
| Keloid | 4 | |
| Distortion | None | 1 |
| Mild | 2 | |
| Moderate | 3 | |
| Severe | 4 |
| Case | Age | Gender | Burn Degree | TBSA (Facial) | Hospitalization (Days) | Follow Up (Months) | NRS Score Pre-Treatment | NRS Score (24 h, 48 h, 72 h) | Scar Score (MSS) | Functional Outcome | Aesthetic Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 68 | Male | Superficial PT | 18 (3.5) | 37 | 27 | n/a | 2, 0, 0 | 4.83 | 10 | 10 |
| 2 | 42 | Male | Superficial PT | 11.5 (1) | 16 | 31.5 | 7 | 2, 0, 0 | 4 | 10 | 10 |
| 3 | 25 | Male | Superficial/deep PT | 5.5 (2.5) | 12 | 6.5 | 6 | 0, 0, 0 | 4.8 | 10 | 10 |
| 4 | 26 | Male | Superficial/deep PT | 16.5 (2) | 11 | 7.5 | 7 | 0, 0, 0 | 4 | 10 | 10 |
| 5 | 23 | Male | Superficial PT | 3.5 (3) | 5 | 30 | 6 | 0, 0, 0 | 4.8 | 10 | 10 |
| 6 | 16 | Male | Superficial PT | 24 (4) | 25 | 18 | n/a | 0, 0, 0 | 5.4 | 10 | 10 |
| 7 | 31 | Female | Superficial PT | 10.5 (4) | 7 | 3 | 8 | 0, 0, 0 | 5.2 | n/a | n/a |
| 8 | 40 | Male | Superficial PT | 35 (4) | 89 | 3 | 7 | 0, 0, 0 | 8.8 | n/a | n/a |
| 9 | 45 | Male | Superficial PT | 17 (4) | 26 | 29 | 7 | 0, 0, 0 | 4.4 | 10 | 10 |
| 10 | 72 | Male | Superficial PT | 23 (4) | 22 | 8.5 | 8 | 0, 0, 0 | 4.6 | 10 | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasella, M.; Cirebea, J.; Gousopoulos, E.; Wang, A.; Schweizer, R.; Waldner, M.; Grieb, G.; Buehler, P.; Plock, J.A.; Kim, B.-S. Outcome of Facial Burn Injuries Treated by a Nanofibrous Temporary Epidermal Layer. J. Clin. Med. 2023, 12, 5273. https://doi.org/10.3390/jcm12165273
Vasella M, Cirebea J, Gousopoulos E, Wang A, Schweizer R, Waldner M, Grieb G, Buehler P, Plock JA, Kim B-S. Outcome of Facial Burn Injuries Treated by a Nanofibrous Temporary Epidermal Layer. Journal of Clinical Medicine. 2023; 12(16):5273. https://doi.org/10.3390/jcm12165273
Chicago/Turabian StyleVasella, Mauro, Jan Cirebea, Epameinondas Gousopoulos, Anna Wang, Riccardo Schweizer, Matthias Waldner, Gerrit Grieb, Philipp Buehler, Jan Alexander Plock, and Bong-Sung Kim. 2023. "Outcome of Facial Burn Injuries Treated by a Nanofibrous Temporary Epidermal Layer" Journal of Clinical Medicine 12, no. 16: 5273. https://doi.org/10.3390/jcm12165273
APA StyleVasella, M., Cirebea, J., Gousopoulos, E., Wang, A., Schweizer, R., Waldner, M., Grieb, G., Buehler, P., Plock, J. A., & Kim, B.-S. (2023). Outcome of Facial Burn Injuries Treated by a Nanofibrous Temporary Epidermal Layer. Journal of Clinical Medicine, 12(16), 5273. https://doi.org/10.3390/jcm12165273