
Is Exercise during Pregnancy a Risk for Gestational Age and Preterm Delivery? Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Intervention
2.3. Comparison
2.4. Outcomes
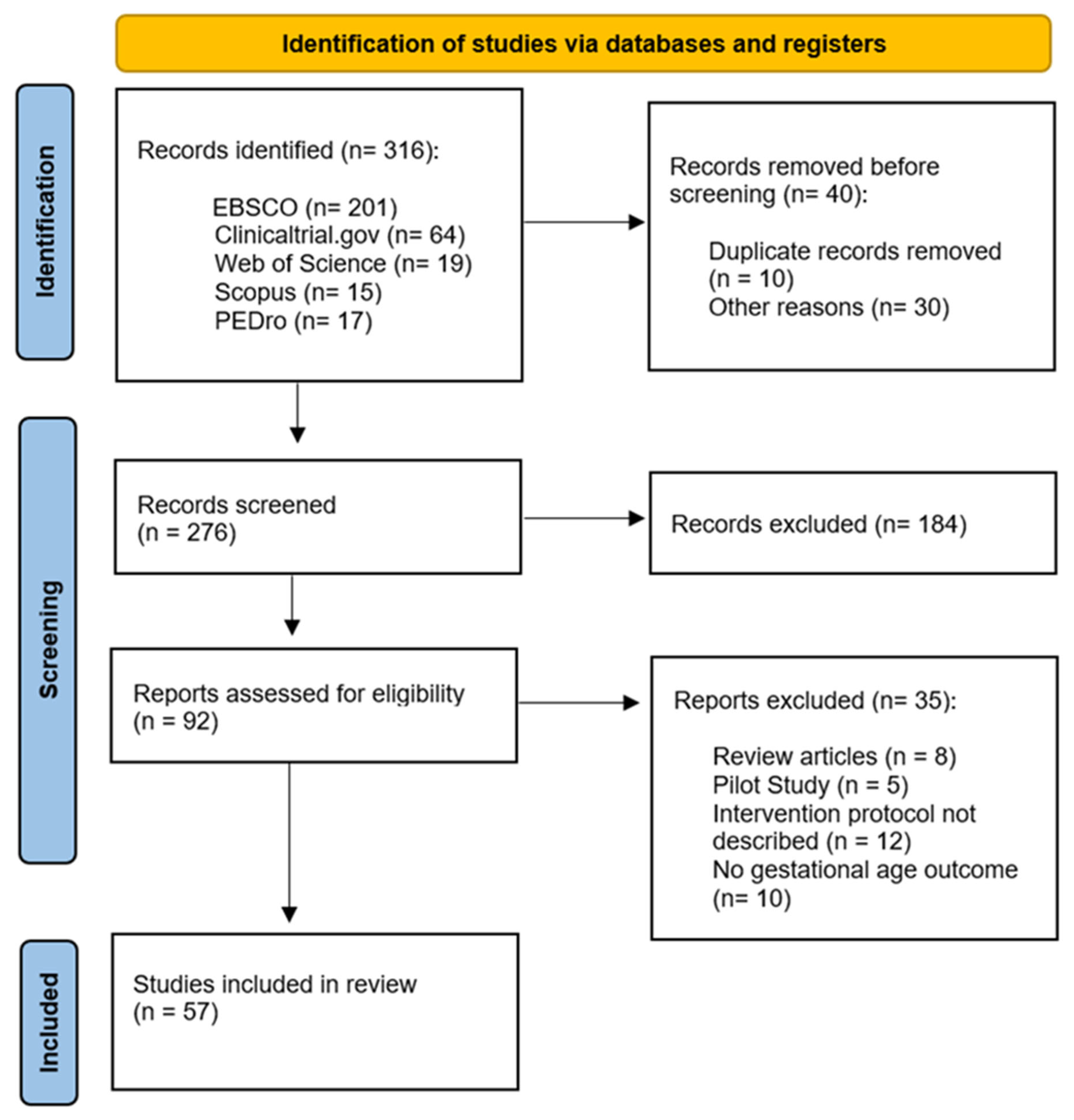
2.5. Study Design and Selection Process
- English: physical activity OR exercise OR physical exercise OR fitness OR strength training OR physical intervention OR cointervention AND pregnancy OR pregnant OR maternal OR antenatal AND randomized clinical trial OR RCT OR non-randomized clinical trial AND gestational age OR preterm birth OR preterm delivery.
- Spanish: actividad física OR ejercicio OR ejercicio físico OR fitness OR entrenamiento de fuerza OR intervención física OR co-intervención AND embarazo OR embarazada OR maternal OR prenatal AND ensayo clínico aleatorizado OR ensayo clínico no aleatorizado AND edad gestacional OR nacimiento a pretérmino OR parto pretérmino.
2.6. Statistical Analysis, Quality of Evidence Assessment, and Risk of Bias

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | N | EG | CG | Intervention Features | Main Variables Analysed | Secondary Variables Analysed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Freq | Intensity | PT | Type | Superv. Class | Duration | Adh. | ||||||||
| Babbar [21] | 2016 | US | 46 | 23 | 23 | 3 | Mod | 8 w | Yoga | Yes | 60 min | - | Gestational age, type of delivery, birth weight | Gestational weight gain |
| Bacchi [22] | 2018 | Argentina | 111 | 49 | 62 | 3 | Low–mod | 26 w | Aquatic activities | Yes | 55–60 min | 80% | Gestational weight gain, gestational age | Birth weight |
| Backhausen [23] | 2017 | Denmark | 516 | 258 | 258 | 2 | Low | 12 w | Aerobic | No | 70 min | - | Low back pain, birth weight | Gestational age, type of delivery |
| Barakat [24] | 2011 | Spain | 80 | 40 | 40 | 3 | Low–mod | 28 w | Aerobic and light strength training | Yes | 35–45 min | Maternal health status | Gestational age, type of delivery | |
| Barakat [25] | 2012 a | Spain | 290 | 138 | 152 | 3 | Mod | 28 w | Aerobic exercise | Yes | 40–45 min | - | Type of delivery | Gestational age and birth weight |
| Barakat [26] | 2012 b | Spain | 83 | 40 | 43 | 3 | Low–mod | 28–33 w | Land aerobic and aquatic activity | Yes | 35–45 min | - | Gestational weight gain and gestational diabetes | Gestational age, type of delivery, birth weight |
| Barakat [27] | 2013 | Spain | 510 | 255 | 255 | 3 | Mod | 28 w | Aerobic, strength, and flexibility exercise | Yes | 50–55 min | - | Gestational diabetes, gestational age | Gestational weight gain and birth weight |
| Barakat [28] | 2014 a | Spain | 290 | 138 | 152 | 3 | 60–75% Max HR | 28–31 w | Aerobic exercise | Yes | 55–60 min | 80% | Gestational age | Gestational diabetes, gestational weight gain |
| Barakat [29] | 2014 b | Spain | 200 | 107 | 93 | 3 | Mod | 26–31 w | Aerobic exercise | Yes | 55–60 min | 80% | Gestational age, gestational weight gain, type of delivery, gestational diabetes | Birth weight, head circumference |
| Barakat [30] | 2016 | Spain | 765 | 382 | 383 | 3 | Mod | 28 w | Aerobic, strength, and flexibility exercise | Yes | 50–55 min | 80% | Hypertension | Type of delivery, gestational age, birth weight |
| Barakat [31] | 2018 a | Spain | 429 | 227 | 202 | 3 | Mod | 28 w | Aerobic exercise | Yes | 55–60 min | 80% | Duration of labour, gestational age | Type of delivery, use of epidural, birth weight |
| Barakat [32] | 2018 b | Spain | 65 | 33 | 32 | 3 | Mod | 28 w | Aerobic, pelvic floor strength, and flexibility exercises | Yes | 55–60 min | - | Placenta’s weight | Gestational age, type of delivery, birth weight |
| Barakat [33] | 2019 | Spain | 456 | 234 | 222 | 3 | Mod | 28 w | Aerobic exercise | Yes | 50–55 min | - | Gestational weight gain | Gestational age, type of delivery, birth weight |
| Bhartia [34] | 2019 | India | 78 | 38 | 40 | 1 2 | Mod | 12 w | Yoga | Yes No | 50 min | - | Maternal stress, type of delivery, birth weight | Gestational age |
| Bjøntegaard [35] | 2021 | Norway | 281 | 164 | 117 | 1–2 | Mod–high | 12 w | Endurance, strength training and balance exercises | Yes No | 60 min 45 min | - | Type of delivery, birth weight, gestational age | PA of children at age of seven |
| Brik [36] | 2019 | Spain | 85 | 42 | 43 | 3 | Light–mod | 29 w | Aerobic, strength, and pelvic floor exercises | Yes | 60 min | 70% | Gestational weight gain | Type of delivery, birth weight, gestational age |
| Carrascosa [37] | 2021 | Spain | 286 | 145 | 141 | 3–5 | 55–65% Max HR | 20 w | Water aerobic exercise | Yes | 45 min | - | Use of epidural analgesia during labour | Type of delivery, time of active labour, episiotomy, gestational age |
| Clark [38] | 2018 | USA | 36 | 14 | 22 | 3 | Mod | 20 w | Aerobic | Yes | 60 min | - | Gestational weight gain, gestational age | Type of delivery, birth weight |
| Cordero [39] | 2012 | Spain | 55 | 25 | 30 | 3 | 50–55% Max HR | 28–33 w | Aerobic and strength training | Yes | 50 min | 80% | Gestational weight gain, gestational diabetes, | Gestational age |
| Cordero [40] | 2015 | Spain | 342 | 122 | 220 | 3 | Mod | 24 w | Aerobics in a gym hall and aquatic activity | Yes | 50–60 min | 80% | Gestational diabetes, gestational age | Gestational weight gain, type of delivery, birth weight |
| Da Silva [41] | 2017 | Brazil | 639 | 213 | 426 | 3 | Mod | 16+ w | Aerobic, strength and stretching training | Yes | 60 min | 70% | Gestational age, preterm birth, and pre-eclampsia | Gestational weight gain, birth weight |
| Daly [42] | 2017 | Ireland | 88 | 44 | 44 | 3 | Mod | 8 w | Aerobic pelvic floor exercises | Yes | 50–60 min | - | Maternal fasting plasma glucose, gestational age | Type of delivery and birth weight |
| de Barros [43] | 2010 | Brazil | 64 | 32 | 32 | 1–2 | Mod | 12 w | Resistance exercise | Yes No | 30 min | - | Gestational diabetes, gestational age | - |
| Dias [44] | 2011 | Norway | 42 | 21 | 21 | 1 | Low | 16 w | Pelvic floor muscle training | Yes | 30 min | 75% | Type of delivery, birth weight, gestational age | Pelvic floor muscle strength |
| Ellingsen [45] | 2020 | Norway | 279 | 164 | 115 | 1–2 | Mod | 12 w | Aerobic activity and strength exercises | Yes No | 60 min 45 min | - | Neurodevelopmental in 7-year-old children | Gestational age, birth weight, type of delivery |
| Fernández-Buhigas [46] | 2020 | Spain | 92 | 41 | 51 | 3 | 50–60% Max HR | 23–27 w | Aerobic, strength, coordination and balance, pelvic floor exercises | Yes | 60 min | 80% | Blood pressure, gestational weight gain | Gestational age |
| Ghodsi [47] | 2014 | Iran | 80 | 40 | 40 | 3 | 50–60% Max HR | 12–18 w | Stationary cycling | No | 15 min | - | Gestational age, type of delivery, perineal tear | - |
| Guelfi [48] | 2016 | Australia | 169 | 84 | 85 | 3 | 65–75% Max HR | 14 w | Home-based stationary cycling program | Yes | 60 min | - | Gestational diabetes | Gestational age, type of delivery, birth weight |
| Haakstad [49] | 2011 | Norway | 105 | 52 | 53 | 2–1 | Mod | 12 w | Aerobic dance and strength training | Yes No | 60 min 30 min | - | Birth weight | Gestational age, type of delivery |
| Halse [50] | 2015 | Australia | 40 | 20 | 20 | 3 | 55–65% Max HR | 6 w | Stationary cycling | No | 45 min | - | Maternal attitude and intentions of exercise | Gestational age, gestational weight gain |
| Hellenes [51] | 2015 | Norway | 336 | 188 | 148 | 1–3 | Mod | 16 w | Aerobic activity | Yes No | 30+ min | - | Cognitive, language and motor domains of children | Gestational age, birth weight, and type of delivery |
| Kong [52] | 2014 | USA | 37 | 18 | 19 | 5 | Mod | 20 w | Treadmill walking | No | 30 min | - | Postpartum weight retention | Gestational weight gain, gestational age, birth weight |
| Leão [53] | 2022 | Brazil | 424 | 141 | 283 | 3 | Mod | 16 w | Aerobic and strength training | Yes | 60 min | 70% | Childhood neurodevelopment | Gestational age |
| McDonald [54] | 2021 | USA | 192 | 131 | 61 | 3 | Mod | 24+ w | Aerobic and resistance training | Yes | 50 min | - | Infant Morphometry | Gestational age |
| McMillan [55] | 2019 | USA | 60 | 33 | 27 | 3 | Mod | 20 w | Aerobic activity | Yes | 50 min | Infant neuromotor skills | Gestational weight gain, gestational age | |
| Murtezani [56] | 2014 | Repub. of Kosovo | 63 | 30 | 33 | 3 | Mod | 20 w | Aerobic and strength exercises | Yes | 40–45 min | - | Birth weight, gestational age | - |
| Nascimento [57] | 2011 | Brazil | 82 | 40 | 42 | 1–5 | Low–mod | 22 w | Aerobic exercise, walking | Yes No | 40 min | - | Gestational weight gain, gestational age | Birth weight |
| Nobles [58] | 2015 | USA | 251 | 124 | 127 | 5 | Mod | 12 w | Aerobic activity | No | 30 min | - | Gestational diabetes | Birth weight, gestational age |
| Pais [59] | 2021 | India | 132 | 66 | 66 | 7 | Low | 14–18 w | Yoga | No | 45 min | - | Preeclampsia and gestational diabetes | Gestational age, analgesia, duration of labour, type of delivery, birth weight |
| Perales [60] | 2015 | Spain | 63 | 38 | 25 | 3 | 55–60% Max HR | 26–31 w | Aerobic dance, pelvic floor muscle training | Yes | 55–60 min | - | Foetal and maternal heart rate | Gestational weight gain, gestational age, birth weight, type of delivery |
| Perales [61] | 2016 | Spain | 166 | 83 | 83 | 3 | 55–60% Max HR | 28–31 w | Aerobic and strength exercises | Yes | 55–60 min | - | Duration of labour, gestational age, type of delivery, birth weight | - |
| Perales [62] | 2020 | Spain | 1348 | 668 | 660 | 3 | Light–mod | 30 w | Aerobic, pelvic floor exercises | Yes | 50–55 min | - | Gestational weight gain, hypertension and gestational diabetes | Type of delivery, birth weight, gestational age, preterm delivery |
| Raper [63] | 2021 | USA | 125 | 58 | 67 | 3 | Mod | 22 w | Aerobic | Yes | 50 min | 80% | Gestational diabetes, type of delivery and birth weight | Gestational age |
| Renault [64] | 2014 | Denmark | 283 | 142 | 141 | 7 | Low | 22–26 w | 11,000 daily steps | No | 60+ min | - | Gestational weight gain, miscarriage | Gestational age |
| Ruchat [65] | 2012 | Canada | 71 | 26 | 45 | 2–3 | Mod | 22 w | Walking | Yes No | 25–40 min | - | Gestational weight gain, birth weight, gestational age | - |
| Ruiz [66] | 2013 | Spain | 96 | 48 | 48 | 3 | Light–mod | 29–30 w | Aerobic and resistance exercises | Yes | 50–55 min | - | Gestational weight gain, gestational age | Birth weight, type of delivery |
| Sagedal [67] | 2017 | Norway | 591 | 296 | 295 | 2 | Mod | 24 w | Strength training and cardiovascular exercise | Yes | 60 min | - | Gestational weight gain, birth weight | Gestational age |
| Sanda [68] | 2018 | Norway | 589 | 295 | 294 | 2–3 | Mod | 22 w | Aerobic exercises | Yes No | 60 min 30 min | - | Gestational age, duration of labour, type of delivery | - |
| Seneviratne [69] | 2015 | New Zealand | 75 | 38 | 37 | 3–5 | Mod | 16 w | Stationary cycling program | No | 15–30 min | - | Birth weight, type of delivery | Gestational weight gain, gestational age |
| Silva-Jose [70] | 2022 | Spain | 157 | 78 | 79 | 3 | Mod | 28–31 w | Aerobic exercise | Yes | 55–60 min | 80% | Gestational weight gain, gestational age | Type of delivery, birth weight |
| Stafne [71] | 2012 | Norway | 761 | 396 | 365 | 1–3 | Mod | 12 w | Aerobics, strength, pelvic floor exercises | Yes No | 60 min 45 min | - | Urinary and anal incontinence | Type of delivery, birth weight, gestational age |
| Taniguchi [72] | 2016 | Japan | 118 | 60 | 58 | 3 | Mod | 6+ w | Walk briskly | Yes | 30 min | 80% | Type of delivery, birth weight | Gestational age |
| Tomic [73] | 2013 | Croatia | 334 | 166 | 168 | 3 | 60–75% Max HR | 28–30 w | Aerobic exercise | Yes | 50 min | 80% | Macrosomia, birth weight, type of delivery, gestational weight gain | Gestational age |
| Uria-Minguito [74] | 2022 | Spain | 203 | 102 | 101 | 3 | 65–70% Max HR | 28–31 w | Aerobic exercise | Yes | 50–60 min | - | Gestational diabetes, gestational age | Gestational weight gain, type of delivery, birth weight |
| Ussher [75] | 2015 | UK | 789 | 394 | 395 | 3–4 | Low | 6 w | Exercise on treadmill | Yes | 20 min | - | Continuous smoking abstinence | Type of delivery, birth weight |
| Wang [76] | 2017 | China | 300 | 150 | 150 | 3 | 55–65% Max HR | 18 w | Stationary cycling program | Yes | 60 min | 75% | Gestational diabetes | Birth weight, macrosomia, gestational age |
| Yekefallah [77] | 2021 | Iran | 70 | 35 | 35 | 2 | Low–mod | 11 w | Yoga | Yes | 75 min | - | Episiotomy, type of delivery | Birth weight, gestational age, duration of labour |
3. Results
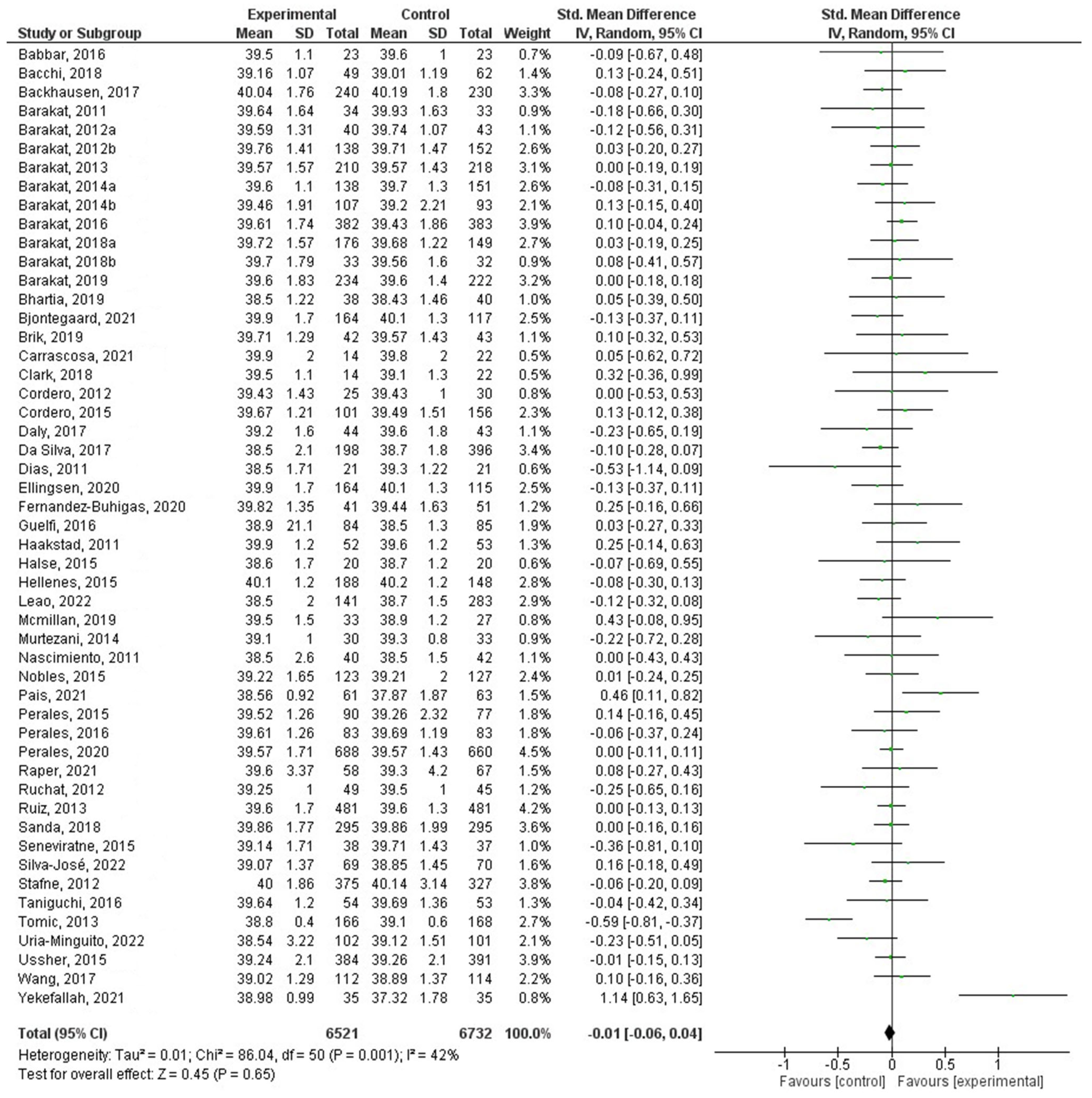
3.1. Effect of PA on Gestational Age
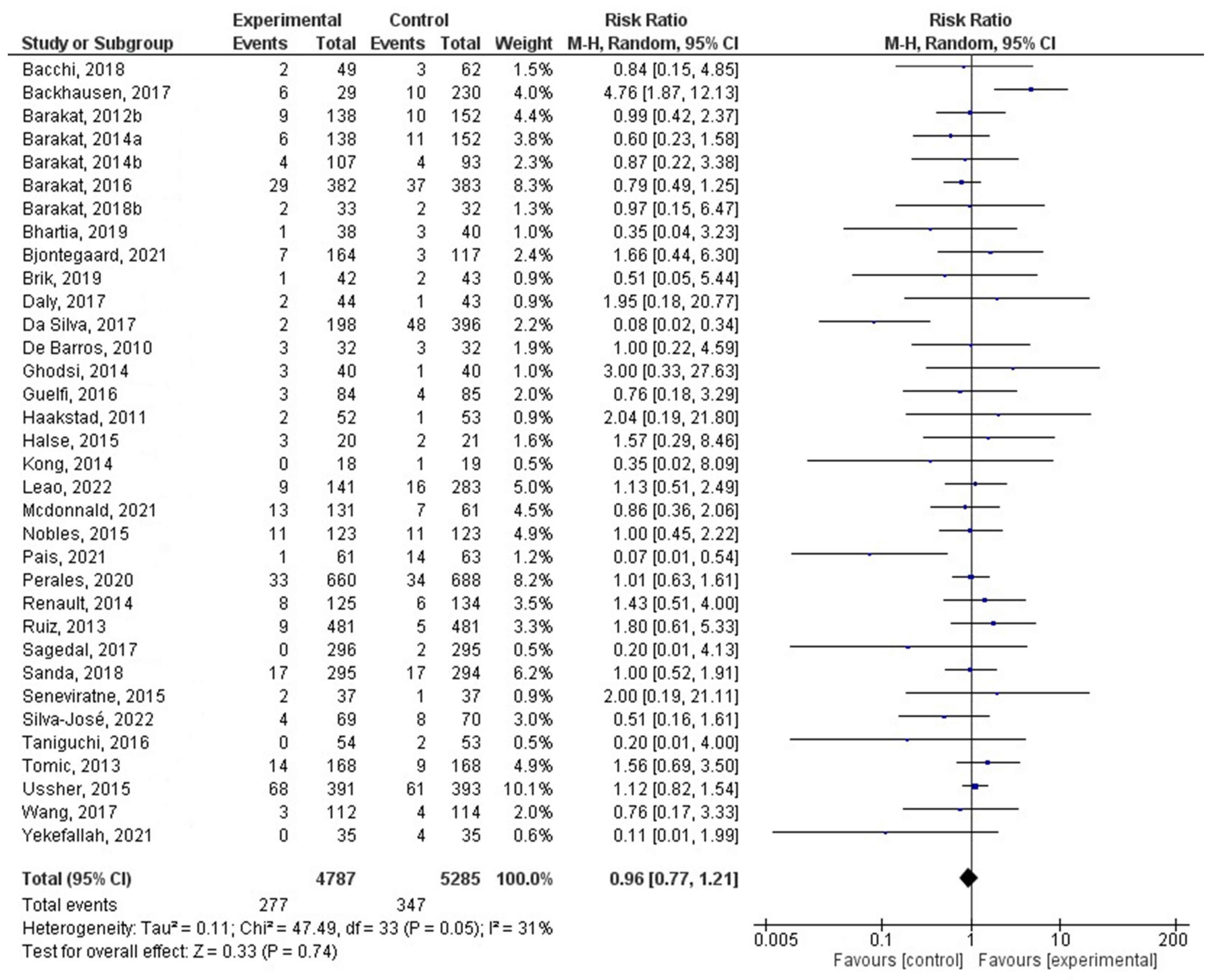
3.2. Effect of PA on the Risk of Preterm Delivery
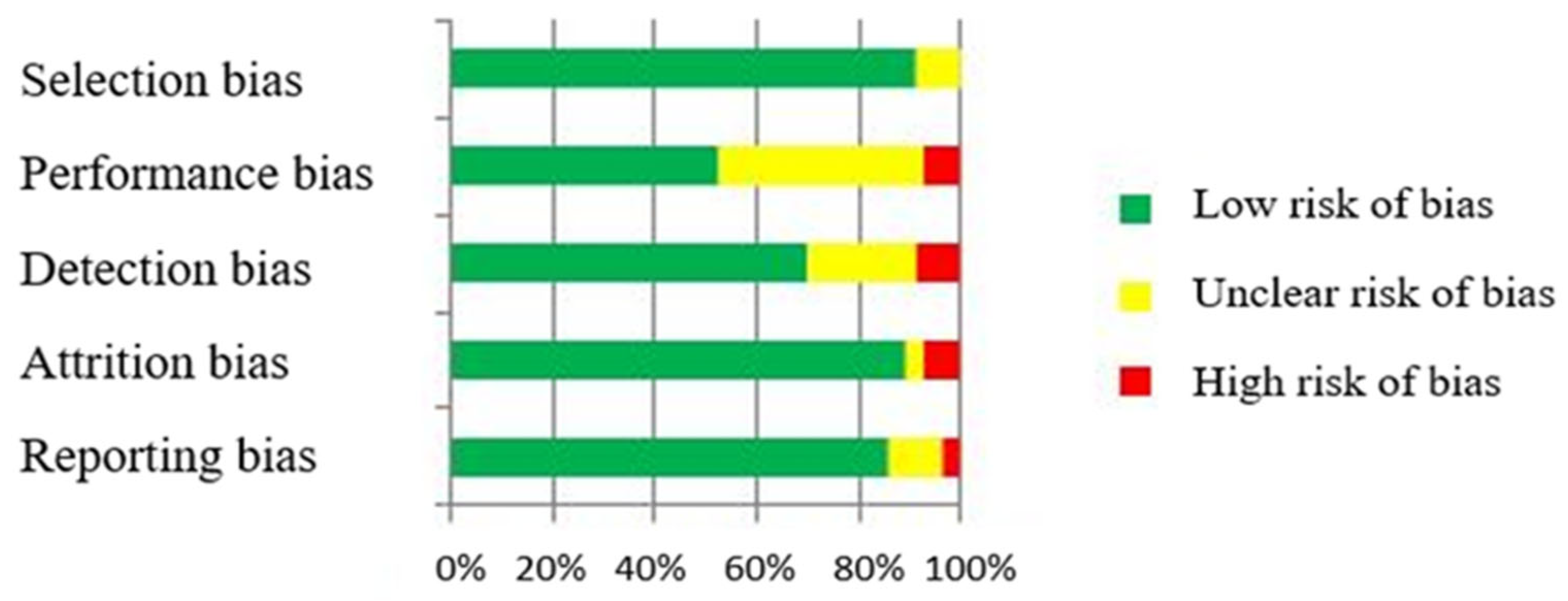
3.3. Risk of Bias Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barakat, R. Pregnancy. In Encyclopedia of Exercise Medicine in Health and Disease; Mooren, F.-C., Ed.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 722–726. [Google Scholar]
- Khaire, A.; Wadhwani, N.; Madiwale, S.; Joshi, S. Maternal fats and pregnancy complications: Implications for long-term health. Prostaglandins Leukot. Essent. Fatty Acids 2020, 157, 102098. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Perales, M. Resistance Exercise in Pregnancy and Outcome. Clin. Obstet. Gynecol. 2016, 59, 591–599. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Källén, K.; Serenius, F.; Westgren, M.; Maršál, K.; EXPRESS Group. Impact of obstetric factors on outcome of extremely preterm births in Sweden: Prospective population-based observational study (EXPRESS). Acta Obstet. Gynecol. Scand. 2015, 94, 1203–1214. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Polán, M.; Silva-Jose, C.; Franco, E.; Nagpal, T.S.; Gil-Ares, J.; Lili, Q.; Barakat, R.; Refoyo, I. Prenatal Anxiety and Exercise. Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5501. [Google Scholar] [CrossRef]
- Mottola, M.F. Components of Exercise Prescription and Pregnancy. Clin. Obstet. Gynecol. 2016, 59, 552–558. [Google Scholar] [CrossRef]
- Ornoy, A. Prenatal origin of obesity and their complications: Gestational diabetes, maternal overweight and paradoxical effects of fetal growth restriction and macrosomia. Reprod. Toxicol. 2011, 32, 205–212. [Google Scholar] [CrossRef]
- Ribeiro, M.M.; Andrade, A.; Nunes, I. Physical exercise in pregnancy: Benefits, risks and prescription. J. Perinat. Med. 2021, 50, 4–17. [Google Scholar] [CrossRef]
- Perales, M.; Valenzuela, P.L.; Barakat, R.; Alejo, L.B.; Cordero, Y.; Peláez, M.; Lucia, A. Obesity can offset the cardiometabolic benefits of gestational exercise. Int. J. Obes. 2021, 45, 342–347. [Google Scholar] [CrossRef]
- Owe, K.M.; Nystad, W.; Skjaerven, R.; Stigum, H.; Bø, K. Exercise during pregnancy and the gestational age distribution: A cohort study. Med. Sci. Sports Exerc. 2012, 44, 1067–1074. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; et al. Impact of prenatal exercise on neonatal and childhood outcomes: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Tipton, E.; Johnson, M.C. Robust variance estimation in meta-regression with dependent effect size estimates. Res. Synth. Methods 2010, 1, 39–65. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.; Riaz, M.; Lewis, S.; Aveyard, P.; Coleman, T.; Manyonda, I.; West, R.; Lewis, B.; Marcus, B.; Taylor, A.; et al. PA for antenatal and postnatal depression in women attempting to quit smoking: Randomised controlled trial. BMC Pregnancy Childbirth 2018, 18, 156. [Google Scholar] [CrossRef]
- Ferreira González, I.; Urrútia, G.; Alonso-Coello, P. Systematic Reviews and Meta-Analysis: Scientific Rationale and Interpretation. Rev. Española Cardiol. 2011, 64, 688–696. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.; Vist, G.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE an Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. Br. Med. J. 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savovíc, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Assessing Risk of Bias in a Randomized Trial. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.1; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2020; pp. 1539–1558. [Google Scholar]
- Babbar, S.; Hill, J.B.; Williams, K.B.; Pinon, M.; Chauhan, S.P.; Maulik, D. Acute fetal behavioral response to prenatal Yoga: A single, blinded, randomized controlled trial (TRY yoga). Am. J. Obstet. Gynecol. 2016, 214, 399.e1–399.e8. [Google Scholar] [CrossRef]
- Bacchi, M.; Mottola, M.F.; Perales, M.; Refoyo, I.; Barakat, R. Aquatic Activities During Pregnancy Prevent Excessive Maternal Weight Gain and Preserve Birth Weight: A Randomized Clinical Trial. Am. J. Health Promot. 2018, 32, 729–735. [Google Scholar] [CrossRef]
- Backhausen, M.G.; Tabor, A.; Albert, H.; Rosthøj, S.; Damm, P.; Hegaard, H.K. The effects of an unsupervised water exercise program on low back pain and sick leave among healthy pregnant women—A randomised controlled trial. PLoS ONE 2017, 12, e0182114. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Pelaez, M.; Montejo, R.; Luaces, M.; Zakynthinaki, M. Exercise during pregnancy improves maternal health perception: A randomized controlled trial. Am. J. Obstet. Gynecol. 2011, 204, 402.e1–402.e7. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Cordero, Y.; Coteron, J.; Luaces, M.; Montejo, R. Exercise during pregnancy improves maternal glucose screen at 24–28 weeks: A randomised controlled trial. Br. J. Sports Med. 2012, 46, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Pelaez, M.; Lopez, C.; Montejo, R.; Coteron, J. Exercise during pregnancy reduces the rate of cesarean and instrumental deliveries: Results of a randomized controlled trial. J. Matern. Fetal Neonatal. Med. 2012, 25, 2372–2376. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Pelaez, M.; Lopez, C.; Lucia, A.; Ruiz, J.R. Exercise during pregnancy and gestational diabetes-related adverse effects: A randomised controlled trial. Br. J. Sports Med. 2013, 47, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Pelaez, M.; Montejo, R.; Refoyo, I.; Coteron, J. Exercise throughout pregnancy does not cause preterm delivery: A randomized, controlled trial. J. PA Health 2014, 11, 1012–1017. [Google Scholar] [CrossRef]
- Barakat, R.; Perales, M.; Bacchi, M.; Coteron, J.; Refoyo, I. A program of exercise throughout pregnancy. Is it safe to mother and newborn? Am. J. Health Promot. 2014, 29, 2–8. [Google Scholar] [CrossRef]
- Barakat, R.; Pelaez, M.; Cordero, Y.; Perales, M.; Lopez, C.; Coteron, J.; Mottola, M.F. Exercise during pregnancy protects against hypertension and macrosomia: Randomized clinical trial. Am. J. Obstet. Gynecol. 2016, 214, 649.e1–649.e8. [Google Scholar] [CrossRef]
- Barakat, R.; Franco, E.; Perales, M.; López, C.; Mottola, M.F. Exercise during pregnancy is associated with a shorter duration of labor. A randomized clinical trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 33–40. [Google Scholar] [CrossRef]
- Barakat, R.; Vargas, M.; Brik, M.; Fernandez, I.; Gil, J.; Coteron, J.; Santacruz, B. Does Exercise During Pregnancy Affect Placental Weight?: A Randomized Clinical Trial. Eval. Health Prof. 2018, 41, 400–414. [Google Scholar] [CrossRef]
- Barakat, R.; Refoyo, I.; Coteron, J.; Franco, E. Exercise during pregnancy has a preventative effect on excessive maternal weight gain and gestational diabetes. A randomized controlled trial. Braz. J. Phys. Ther. 2019, 23, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Bhartia, N.; Jain, S.; Shankar, N.; Rajaram, S.; Manish, G. Effects of Antenatal Yoga on Maternal Stress and Clinical Outcomes in North Indian Women: A Randomised controlled trial. JIACM 2019, 20, 10–14. [Google Scholar]
- Bjøntegaard, K.A.; Stafne, S.N.; Mørkved, S.; Salvesen, K.Å.; Evensen, K.A.I. Body mass index and PA in seven-year-old children whose mothers exercised during pregnancy: Follow-up of a multicentre randomised controlled trial. BMC Pediatr. 2021, 21, 496. [Google Scholar] [CrossRef]
- Brik, M.; Fernández-Buhigas, I.; Martin-Arias, A.; Vargas-Terrones, M.; Barakat, R.; Santacruz, B. Does exercise during pregnancy impact on maternal weight gain and fetal cardiac function? A randomized controlled trial. Ultrasound. Obstet. Gynecol. 2019, 53, 583–589. [Google Scholar] [CrossRef]
- Carrascosa, M.D.C.; Navas, A.; Artigues, C.; Ortas, S.; Portells, E.; Soler, A.; Bennasar-Veny, M.; Leiva, A.; Aquanatal Trial. Effect of aerobic water exercise during pregnancy on epidural use and pain: A multi-centre, randomised, controlled trial. Midwifery 2021, 103, 103105. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.; Isler, C.; Strickland, D.; McMillan, A.G.; Fang, X.; Kuehn, D.; Ravisankar, S.; Strom, C.; May, L.E. Influence of aerobic exercise on maternal lipid levels and offspring morphometrics. Int. J. Obes. 2019, 43, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Cordero, Y.; Peláez, M.; De Miguel, M.; Perales, M.; Barakat, R. ¿Puede el ejercicio físico moderado durante el embarazo actuar como un factor de prevención de la Diabetes Gestacional. RICYDE. Rev. Int. Cienc. Deporte 2012, 27, 3–19. [Google Scholar] [CrossRef]
- Cordero, Y.; Mottola, M.F.; Vargas, J.; Blanco, M.; Barakat, R. Exercise Is Associated with a Reduction in Gestational Diabetes Mellitus. Med. Sci. Sports Exerc. 2015, 47, 1328–1333. [Google Scholar] [CrossRef]
- Da Silva, S.G.; Hallal, P.C.; Domingues, M.R.; Bertoldi, A.D.; Silveira, M.F.D.; Bassani, D.; da Silva, I.C.M.; da Silva, B.G.C.; Coll, C.V.N.; Evenson, K. A randomized controlled trial of exercise during pregnancy on maternal and neonatal outcomes: Results from the PAMELA study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 175. [Google Scholar] [CrossRef]
- Daly, N.; Farren, M.; McKeating, A.; O’Kelly, R.; Stapleton, M.; Turner, M.J. A Medically Supervised Pregnancy Exercise Intervention in Obese Women: A Randomized Controlled Trial. Obstet. Gynecol. 2017, 130, 1001–1010. [Google Scholar] [CrossRef]
- De Barros, M.C.; Lopes, M.A.; Francisco, R.P.; Sapienza, A.D.; Zugaib, M. Resistance exercise and glycemic control in women with gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2010, 203, 556.e1–556.e6. [Google Scholar] [CrossRef] [PubMed]
- Dias, L.A.; Driusso, P.; Aita, D.L.; Quintana, S.M.; Bø, K.; Ferreira, C.H. Effect of pelvic floor muscle training on labour and newborn outcomes: A randomized controlled trial. Rev. Bras. Fisioter. 2011, 15, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Ellingsen, M.S.; Pettersen, A.; Stafne, S.N.; Mørkved, S.; Salvesen, K.Å.; Evensen, K.A. Neurodevelopmental outcome in 7-year-old children is not affected by exercise during pregnancy: Follow up of a multicentre randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Buhigas, I.; Brik, M.; Martin-Arias, A.; Vargas-Terrones, M.; Varillas, D.; Barakat, R.; Santacruz, B. Maternal physiological changes at rest induced by exercise during pregnancy: A randomized controlled trial. Physiol. Behav. 2020, 220, 112863. [Google Scholar] [CrossRef]
- Ghodsi, Z.; Asltoghiri, M. Effects of aerobic exercise training on maternal and neonatal outcome: A randomized controlled trial on pregnant women in Iran. J. Pak. Med. Assoc. 2014, 64, 1053–1056. [Google Scholar]
- Guelfi, K.J.; Ong, M.J.; Crisp, N.A.; Fournier, P.A.; Wallman, K.E.; Grove, J.R.; Doherty, D.A.; Newnham, J.P. Regular Exercise to Prevent the Recurrence of Gestational Diabetes Mellitus: A Randomized Controlled Trial. Obstet. Gynecol. 2016, 128, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Haakstad, L.A.; Bø, K. Exercise in pregnant women and birth weight: A randomized controlled trial. BMC Pregnancy Childbirth 2011, 11, 66. [Google Scholar] [CrossRef]
- Halse, R.E.; Wallman, K.E.; Dimmock, J.A.; Newnham, J.P.; Guelfi, K.J. Home-Based Exercise Improves Fitness and Exercise Attitude and Intention in Women with GDM. Med. Sci. Sports Exerc. 2015, 47, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Hellenes, O.M.; Vik, T.; Løhaugen, G.C.; Salvesen, K.Å.; Stafne, S.N.; Mørkved, S.; Evensen, K.A. Regular moderate exercise during pregnancy does not have an adverse effect on the neurodevelopment of the child. Acta Paediatr. 2015, 104, 285–291. [Google Scholar] [CrossRef]
- Kong, K.L.; Campbell, C.G.; Foster, R.C.; Peterson, A.D.; Lanningham-Foster, L. A pilot walking program promotes moderate-intensity PA during pregnancy. Med. Sci. Sports Exerc. 2014, 46, 462–471. [Google Scholar] [CrossRef]
- Leão, O.A.A.; Domingues, M.R.; Bertoldi, A.D.; Ricardo, L.I.C.; Müller, W.A.; Tornquist, L.; Martins, R.C.; Murray, J.; Silveira, M.F.; Crochemore-Silva, I.; et al. Effects of Regular Exercise during Pregnancy on Early Childhood Neurodevelopment: The PA for Mothers Enrolled in Longitudinal Analysis Randomized Controlled Trial. J. Phys. Act. Health 2022, 19, 203–210. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.M.; Isler, C.; Haven, K.; Newton, E.; Kuehn, D.; Kelley, G.; Chasan-Taber, L.; May, L.E. Moderate intensity aerobic exercise during pregnancy and 1-month infant Morphometry. Birth Defects Res. 2021, 113, 238–247. [Google Scholar] [CrossRef] [PubMed]
- McMillan, A.G.; May, L.E.; Gaines, G.G.; Isler, C.; Kuehn, D. Effects of Aerobic Exercise during Pregnancy on 1-Month Infant Neuromotor Skills. Med. Sci. Sports Exerc. 2019, 51, 1671–1676. [Google Scholar] [CrossRef]
- Murtezani, A.; Paçarada, M.; Ibraimi, Z.; Nevzati, A.; Abazi, N. The impact of exercise during pregnancy on neonatal outcomes: A randomized controlled trial. J. Sports Med. Phys. Fitness. 2014, 54, 802–808. [Google Scholar] [PubMed]
- Nascimento, S.L.; Surita, F.G.; Parpinelli, M.Â.; Siani, S.; Pinto e Silva, J.L. The effect of an antenatal physical exercise programme on maternal/perinatal outcomes and quality of life in overweight and obese pregnant women: A randomised clinical trial. BJOG 2011, 118, 1455–1463. [Google Scholar] [CrossRef]
- Nobles, C.; Marcus, B.H.; Stanek, E.J., 3rd; Braun, B.; Whitcomb, B.W.; Solomon, C.G.; Manson, J.E.; Markenson, G.; Chasan-Taber, L. Effect of an exercise intervention on gestational diabetes mellitus: A randomized controlled trial. Obstet. Gynecol. 2015, 125, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Pais, M.; Pai, M.V.; Kamath, A.; Bhat, R.; Bhat, P.; Joisa, G.H. A Randomized Controlled Trial on the Efficacy of Integrated Yoga on Pregnancy Outcome. Holist. Nurs. Pract. 2021, 35, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Perales, M.; Refoyo, I.; Coteron, J.; Bacchi, M.; Barakat, R. Exercise during pregnancy attenuates prenatal depression: A randomized controlled trial. Eval. Health Prof. 2015, 38, 59–72. [Google Scholar] [CrossRef]
- Perales, M.; Calabria, I.; Lopez, C.; Franco, E.; Coteron, J.; Barakat, R. Regular Exercise throughout Pregnancy Is Associated with a Shorter First Stage of Labor. Am. J. Health Promot. 2016, 30, 149–154. [Google Scholar] [CrossRef]
- Perales, M.; Valenzuela, P.L.; Barakat, R.; Cordero, Y.; Peláez, M.; López, C.; Ruilope, L.M.; Santos-Lozano, A.; Lucia, A. Gestational Exercise and Maternal and Child Health: Effects until Delivery and at Post-Natal Follow-up. J. Clin. Med. 2020, 9, 379. [Google Scholar] [CrossRef]
- Raper, M.J.; McDonald, S.; Johnston, C.; Isler, C.; Newton, E.; Kuehn, D.; Collier, D.; Broskey, N.T.; Muldrow, A.; May, L.E. The influence of exercise during pregnancy on racial/ethnic health disparities and birth outcomes. BMC Pregnancy Childbirth 2021, 21, 258. [Google Scholar] [CrossRef] [PubMed]
- Renault, K.M.; Nørgaard, K.; Nilas, L.; Carlsen, E.M.; Cortes, D.; Pryds, O.; Secher, N.J. The Treatment of Obese Pregnant Women (TOP) study: A randomized controlled trial of the effect of PA intervention assessed by pedometer with or without dietary intervention in obese pregnant women. Am. J. Obstet. Gynecol. 2014, 210, 134.e1–134.e9. [Google Scholar] [CrossRef] [PubMed]
- Ruchat, S.M.; Davenport, M.H.; Giroux, I.; Hillier, M.; Batada, A.; Sopper, M.M.; Hammond, J.M.; Mottola, M.F. Nutrition and exercise reduce excessive weight gain in normal-weight pregnant women. Med. Sci. Sports Exerc. 2012, 44, 1419–1426. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Perales, M.; Pelaez, M.; Lopez, C.; Lucia, A.; Barakat, R. Supervised exercise-based intervention to prevent excessive gestational weight gain: A randomized controlled trial. Mayo Clin. Proc. 2013, 88, 1388–1397. [Google Scholar] [CrossRef] [PubMed]
- Sagedal, L.R.; Øverby, N.C.; Bere, E.; Torstveit, M.K.; Lohne-Seiler, H.; Småstuen, M.; Hillesund, E.R.; Henriksen, T.; Vistad, I. Lifestyle intervention to limit gestational weight gain: The Norwegian Fit for Delivery randomised controlled trial. BJOG 2017, 124, 97–109. [Google Scholar] [CrossRef]
- Sanda, B.; Vistad, I.; Sagedal, L.R.; Haakstad, L.A.H.; Lohne-Seiler, H.; Torstveit, M.K. What is the effect of PA on duration and mode of delivery? Secondary analysis from the Norwegian Fit for Delivery trial. Acta Obstet. Gynecol. Scand. 2018, 97, 861–871. [Google Scholar] [CrossRef]
- Seneviratne, S.N.; Jiang, Y.; Derraik, J.; McCowan, L.; Parry, G.K.; Biggs, J.B.; Craigie, S.; Gusso, S.; Peres, G.; Rodrigues, R.O.; et al. Effects of antenatal exercise in overweight and obese pregnant women on maternal and perinatal outcomes: A randomised controlled trial. BJOG 2016, 123, 588–597. [Google Scholar] [CrossRef]
- Silva-Jose, C.; Sánchez-Polán, M.; Barakat, R.; Díaz-Blanco, Á.; Mottola, M.F.; Refoyo, I. A Virtual Exercise Program throughout Pregnancy during the COVID-19 Pandemic Modifies Maternal Weight Gain, Smoking Habits and Birth Weight-Randomized Clinical Trial. J. Clin. Med. 2022, 11, 4045. [Google Scholar] [CrossRef]
- Stafne, S.N.; Salvesen, K.Å.; Romundstad, P.R.; Eggebø, T.M.; Carlsen, S.M.; Mørkved, S. Regular exercise during pregnancy to prevent gestational diabetes: A randomized controlled trial. Obstet. Gynecol. 2012, 119, 29–36. [Google Scholar] [CrossRef]
- Taniguchi, C.; Sato, C. Home-based walking during pregnancy affects mood and birth outcomes among sedentary women: A randomized controlled trial. Int. J. Nurs. Pract. 2016, 22, 420–426. [Google Scholar] [CrossRef]
- Tomić, V.; Sporiš, G.; Tomić, J.; Milanović, Z.; Zigmundovac-Klaić, D.; Pantelić, S. The effect of maternal exercise during pregnancy on abnormal fetal growth. Croat. Med. J. 2013, 54, 362–368. [Google Scholar] [CrossRef]
- Uria-Minguito, A.; Silva-José, C.; Sánchez-Polán, M.; Díaz-Blanco, Á.; García-Benasach, F.; Carrero Martínez, V.; Alzola, I.; Barakat, R. The Effect of Online Supervised Exercise throughout Pregnancy on the Prevention of Gestational Diabetes in Healthy Pregnant Women during COVID-19 Pandemic: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 14104. [Google Scholar] [CrossRef] [PubMed]
- Ussher, M.; Lewis, S.; Aveyard, P.; Manyonda, I.; West, R.; Lewis, B.; Marcus, B.; Riaz, M.; Taylor, A.H.; Barton, P.; et al. The London Exercise And Pregnant smokers (LEAP) trial: A randomised controlled trial of PA for smoking cessation in pregnancy with an economic evaluation. Health Technol. Assess. 2015, 19, 1–135. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wei, Y.; Zhang, X.; Zhang, Y.; Xu, Q.; Sun, Y.; Su, S.; Zhang, L.; Liu, C.; Feng, Y.; et al. A randomized clinical trial of exercise during pregnancy to prevent gestational diabetes mellitus and improve pregnancy outcome in overweight and obese pregnant women. Am. J. Obstet. Gynecol. 2017, 216, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Yekefallah, L.; Namdar, P.; Dehghankar, L.; Golestaneh, F.; Taheri, S.; Mohammadkhaniha, F. The effect of yoga on the delivery and neonatal outcomes in nulliparous pregnant women in Iran: A clinical trial study. BMC Pregnancy Childbirth 2021, 21, 351. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. ACOG Committee Opinion No. 650: Physical activity and exercise during pregnancy and the postpartum period; Committee opinion no. 650. Obstet. Gynecol 2015, 126, e135–e142. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on PA and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for PA throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef]
- Liao, Z.; Cai, L.; Liu, C.; Li, J.; Hu, X.; Lai, Y.; Shen, L.; Sui, C.; Zhang, H.; Qian, K. Nomogram for predicting the risk of preterm delivery after IVF/ICSI treatment: An analysis of 11,513 singleton births. Front. Endocrinol. 2023, 14, 1065291. [Google Scholar] [CrossRef]
- Delcroix, M.H.; Delcroix-Gomez, C.; Marquet, P.; Gauthier, T.; Thomas, D.; Aubard, Y. Active or passive maternal smoking increases the risk of low birth weight or preterm delivery: Benefits of cessation and tobacco control policies. Tob. Induc. Dis. 2023, 21, 72. [Google Scholar] [CrossRef]
- Tersigni, C.; Neri, C.; D’Ippolito, S.; Garofalo, S.; Martino, C.; Lanzone, A.; Scambia, G.; Di Simone, N. Impact of maternal obesity on the risk of preterm delivery: Insights into pathogenic mechanisms. J. Matern. Fetal. Neonatal. Med. 2022, 35, 3216–3221. [Google Scholar] [CrossRef] [PubMed]
- Campolong, K.; Jenkins, S.; Clark, M.M.; Borowski, K.; Nelson, N.; Moore, K.M.; Bobo, W.V. The association of exercise during pregnancy with trimester-specific and postpartum quality of life and depressive symptoms in a cohort of healthy pregnant women. Arch. Womens Ment. Health 2018, 21, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Polán, M.; Franco, E.; Silva-José, C.; Gil-Ares, J.; Pérez-Tejero, J.; Barakat, R.; Refoyo, I. Exercise During Pregnancy and Prenatal Depression: A Systematic Review and Meta-Analysis. Front. Physiol. 2021, 12, 640024. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barakat, R.; Zhang, D.; Sánchez-Polán, M.; Silva-José, C.; Gil-Ares, J.; Franco, E. Is Exercise during Pregnancy a Risk for Gestational Age and Preterm Delivery? Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 4915. https://doi.org/10.3390/jcm12154915
Barakat R, Zhang D, Sánchez-Polán M, Silva-José C, Gil-Ares J, Franco E. Is Exercise during Pregnancy a Risk for Gestational Age and Preterm Delivery? Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(15):4915. https://doi.org/10.3390/jcm12154915
Chicago/Turabian StyleBarakat, Rubén, Dingfeng Zhang, Miguel Sánchez-Polán, Cristina Silva-José, Javier Gil-Ares, and Evelia Franco. 2023. "Is Exercise during Pregnancy a Risk for Gestational Age and Preterm Delivery? Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 15: 4915. https://doi.org/10.3390/jcm12154915
APA StyleBarakat, R., Zhang, D., Sánchez-Polán, M., Silva-José, C., Gil-Ares, J., & Franco, E. (2023). Is Exercise during Pregnancy a Risk for Gestational Age and Preterm Delivery? Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(15), 4915. https://doi.org/10.3390/jcm12154915