
Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review

 ,
, 
 , ,
, ,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Question and Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
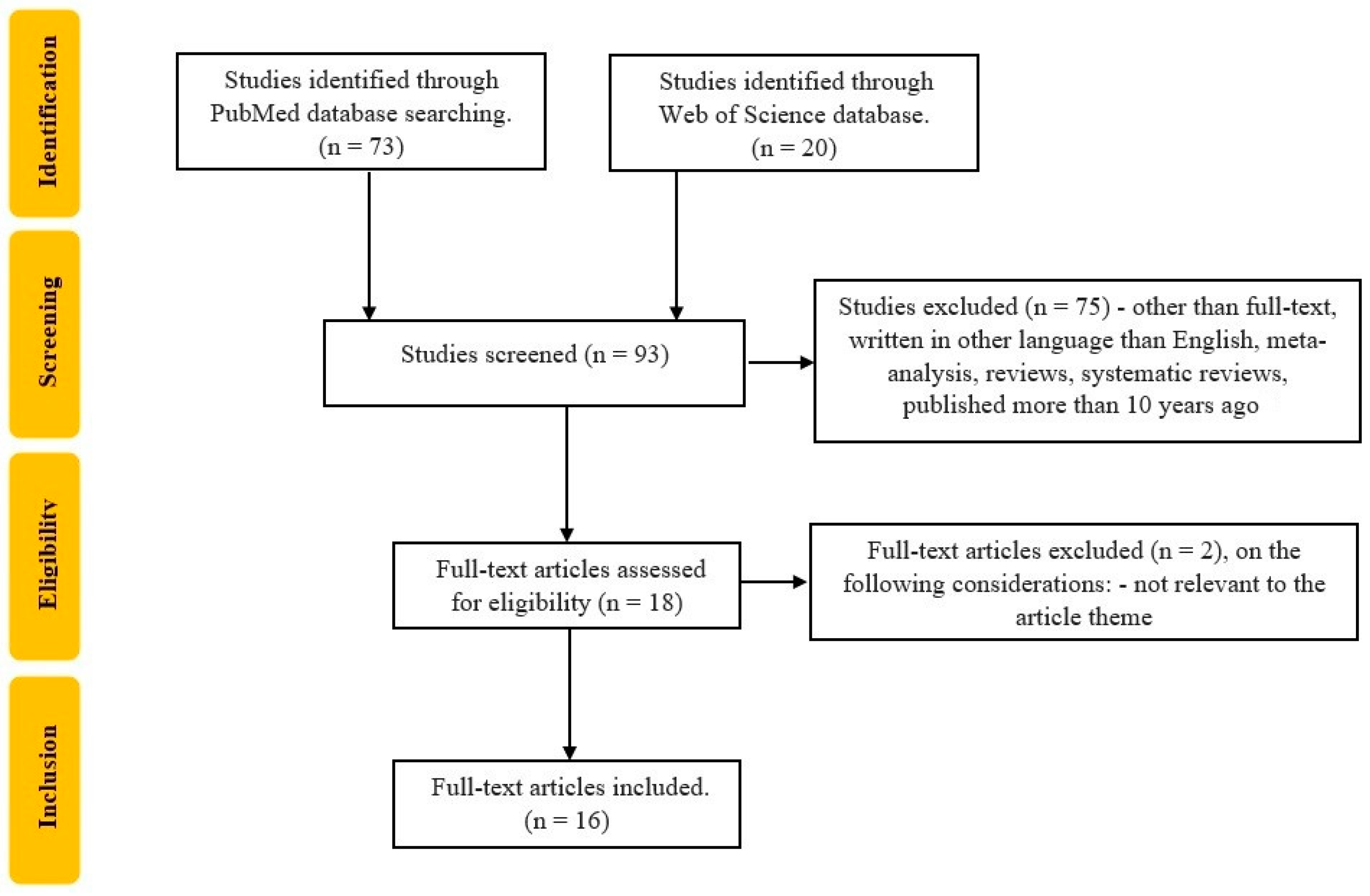
2.4. Selection of Studies
3. Results
Included Studies
4. Discussion
4.1. Assessment of Sarcopenia
4.2. Interventions for Sarcopenia
4.3. Malnutrition, Frailty, and Disability
4.4. Limitations and Future Perspective of Our Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ryan, E.; McNicholas, D.; Creavin, B.; Kelly, M.E.; Walsh, T.; Beddy, D. Sarcopenia and Inflammatory Bowel Disease: A Systematic Review. Inflamm. Bowel Dis. 2019, 25, 67–73. [Google Scholar] [CrossRef]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide Incidence and Prevalence of Inflammatory Bowel Disease in the 21st Century: A Systematic Review of Population-Based Studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Kara, M.; Kaymak, B.; Frontera, W.; Ata, A.M.; Ricci, V.; Ekiz, T.; Chang, K.V.; Han, D.S.; Michail, X.; Quittan, M.; et al. Diagnosing sarcopenia: Functional perspectives and a new algorithm from the ISarcoPRM. J. Rehabil. Med. 2021, 53, 2806. [Google Scholar] [CrossRef]
- Walston, J.D. Sarcopenia in Older Adults. Curr. Opin. Rheumatol. 2012, 24, 623. [Google Scholar] [CrossRef]
- Mukund, K.; Subramaniam, S. Skeletal Muscle: A Review of Molecular Structure and Function, in Health and Disease. Wiley Interdiscip. Rev. Syst. Biol. Med. 2020, 12, e1462. [Google Scholar] [CrossRef]
- Marty, E.; Liu, Y.; Samuel, A.; Or, O.; Lane, J. A Review of Sarcopenia: Enhancing Awareness of an Increasingly Prevalent Disease. Bone 2017, 105, 276–286. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for Clinical Practice and Public Health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Nakamura, S.; Miyazaki, T.; Kakimoto, K.; Fukunishi, S.; Asai, A.; Nishiguchi, S.; Higuchi, K. Inflammatory Bowel Disease and Sarcopenia: Its Mechanism and Clinical Importance. J. Clin. Med. 2021, 10, 4214. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.Q.; Varma, P.; Strauss, B.J.G.; Rajadurai, A.S.; Moore, G.T. Low Muscle Mass at Initiation of Anti-TNF Therapy for Inflammatory Bowel Disease Is Associated with Early Treatment Failure: A Retrospective Analysis. Eur. J. Clin. Nutr. 2017, 71, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, K.; Kapsoritakis, A.; Oikonomou, K.; Manolakis, A.; Tsakiridou, E.; Potamianos, S. Disability in Patients with Inflammatory Bowel Disease: Correlations with Quality of Life and Patient’s Characteristics. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6138105. [Google Scholar] [CrossRef] [PubMed]
- International Classification of Functioning, Disability and Health (ICF). Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 4 March 2023).
- Potcovaru, C.G.; Salmen, T.; Chitu, M.C.; Dima, V.; Mihai, M.B.; Bohiltea, R.E.; Cinteza, D.; Berteanu, M. Assessmen/Ht Tools of Disability Status after Stroke. Rom. J. Neurol. 2022, 21, 208. [Google Scholar] [CrossRef]
- Üstün, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Anderson, A.; Click, B.; Ramos-Rivers, C.; Koutroubakis, I.E.; Hashash, J.G.; Dunn, M.A.; Schwartz, M.; Swoger, J.; Barrie, A.; Regueiro, M.; et al. The Association Between Sustained Poor Quality of Life and Future Opioid Use in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2018, 24, 1380–1388. [Google Scholar] [CrossRef]
- Scaldaferri, F.; Pizzoferrato, M.; Lopetuso, L.R.; Musca, T.; Ingravalle, F.; Sicignano, L.L.; Mentella, M.; Miggiano, G.; Mele, M.C.; Gaetani, E.; et al. Nutrition and IBD: Malnutrition and/or Sarcopenia? A Practical Guide. Gastroenterol. Res. Pract. 2017, 2017, 8646495. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Huang, Y.; Yu, X. A Narrative Review of Gut-Muscle Axis and Sarcopenia: The Potential Role of Gut Microbiota. Int. J. Gen. Med. 2021, 14, 1263–1273. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, M.; Littbrand, H.; Gustafson, Y.; Lundin-Olsson, L.; Lindelöf, N.; Rosendahl, E.; Håglin, L. Effects of High-Intensity Exercise and Protein Supplement on Muscle Mass in ADL Dependent Older People with and without Malnutrition: A Randomized Controlled Trial. J. Nutr. Health Aging 2011, 15, 554–560. [Google Scholar] [CrossRef]
- Marshall, R.N.; Smeuninx, B.; Morgan, P.T.; Breen, L. Nutritional Strategies to Offset Disuse-Induced Skeletal Muscle Atrophy and Anabolic Resistance in Older Adults: From Whole-Foods to Isolated Ingredients. Nutrients 2020, 12, 1533. [Google Scholar] [CrossRef]
- Maltais, M.L.; Ladouceur, J.P.; Dionne, I.J. The Effect of Resistance Training and Different Sources of Postexercise Protein Supplementation on Muscle Mass and Physical Capacity in Sarcopenic Elderly Men. J. Strength Cond. Res. 2016, 30, 1680. [Google Scholar] [CrossRef]
- Subramaniam, K.; Fallon, K.; Ruut, T.; Lane, D.; McKay, R.; Shadbolt, B.; Ang, S.; Cook, M.; Platten, J.; Pavli, P.; et al. Infliximab Reverses Inflammatory Muscle Wasting (Sarcopenia) in Crohn’s Disease. Aliment. Pharmacol. Ther. 2015, 41, 419–428. [Google Scholar] [CrossRef]
- Holt, D.Q.; Moore, G.T.; Strauss, B.J.G.; Hamilton, A.L.; De Cruz, P.; Kamm, M.A. Visceral Adiposity Predicts Post-Operative Crohn’s Disease Recurrence. Aliment. Pharmacol. Ther. 2017, 45, 1255–1264. [Google Scholar] [CrossRef]
- Zhao, J.; Huang, Y.; Yu, X. Effects of Nutritional Supplement and Resistance Training for Sarcopenia in Patients with Inflammatory Bowel Disease: A Randomized Controlled Trial. Medicine 2022, 101, e30386. [Google Scholar] [CrossRef]
- Kang, M.K.; Kim, K.O.; Kim, M.C.; Park, J.G.; Jang, B.I. Sarcopenia Is a New Risk Factor of Nonalcoholic Fatty Liver Disease in Patients with Inflammatory Bowel Disease. Dig. Dis. 2020, 38, 507–514. [Google Scholar] [CrossRef]
- Ciocirlan, M.; Ciocirlan, M.; Iacob, R.; Tanțău, A.; Gheorghe, L.; Gheorghe, C.; Dobru, D.; Constantinescu, G.; Cijevschi, C.; Trifan, A. Malnutrition Prevalence in Newly Diagnosed Patients with Inflammatory Bowel Disease-Data from the National Romanian Database. J. Gastrointest. Liver Dis. 2019, 28, 163–168. [Google Scholar] [CrossRef]
- Bian, D.; Jiang, Y.; Gu, Y.; He, Z.; Chen, Q.; Tang, Y.; Zhong, J.; Shi, Y. Body Mass Index and Disease Activity Are Associated with Moderate to Severe Disability in Crohn’s Disease: A Cross-Sectional Study in Shanghai. Front. Med. 2021, 8, 662488. [Google Scholar] [CrossRef]
- Kochar, B.; Cai, W.; Cagan, A.; Ananthakrishnan, A.N. Frailty is independently associated with mortality in 11 001 patients with inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2020, 52, 311–318. [Google Scholar] [CrossRef]
- Huang, S.; Niu, Y.; Liu, X.; Gu, Z.; Huang, A.; Wu, J. Characteristics of Malnutrition According to Global Leadership Initiative on Malnutrition Criteria in Non-Surgical Patients with Irritable Bowel Disease. Nutrition 2022, 94, 111514. [Google Scholar] [CrossRef] [PubMed]
- Boparai, G.; Kedia, S.; Kandasamy, D.; Sharma, R.; Madhusudhan, K.S.; Dash, N.R.; Sahu, P.; Pal, S.; Sahni, P.; Panwar, R. Combination of Sarcopenia and High Visceral Fat Predict Poor Outcomes in Patients with Crohn’s Disease. Eur. J. Clin. Nutr. 2021, 75, 1491–1498. [Google Scholar] [CrossRef]
- Ge, X.; Xia, J.; Wu, Y.; Ye, L.; Liu, W.; Qi, W.; Cao, Q.; Bai, R.; Zhou, W. Sarcopenia Assessed by Computed Tomography Is Associated with Colectomy in Patients with Acute Severe Ulcerative Colitis. Eur. J. Clin. Nutr. 2022, 76, 410–418. [Google Scholar] [CrossRef]
- Fiorindi, C.; Luceri, C.; Dragoni, G.; Piemonte, G.; Scaringi, S.; Staderini, F.; Nannoni, A.; Ficari, F.; Giudici, F. GLIM Criteria for Malnutrition in Surgical IBD Patients: A Pilot Study. Nutrients 2020, 12, 2222. [Google Scholar] [CrossRef]
- Zhou, Z.; Xiong, Z.; Xie, Q.; Xiao, P.; Zhang, Q.; Gu, J.; Li, J.; Hu, D.; Hu, X.; Shen, Y. Computed Tomography-Based Multiple Body Composition Parameters Predict Outcomes in Crohn’s Disease. Insights Into Imaging 2021, 12, 135. [Google Scholar] [CrossRef] [PubMed]
- Higashiyama, M.; Komoto, S.; Suzuki, Y.; Watanabe, M.; Hibi, T.; Miura, S.; Hokari, R. Relation of Geriatric Nutritional Risk Index with Clinical Risks in Elderly-onset Ulcerative Colitis. J. Gastroenterol. Hepatol. 2021, 36, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Pribadi, R.R.; Simadibrata, M.; Sulaiman, A.S.; Abdullah, M. Role of Thigh Circumference, Calf Circumference, Subjective Global Assessment, and Handgrip Strength as Diagnostic Modalities of Sarcopenia in Women Inflammatory Bowel Disease Patients. JGH Open 2022, 6, 621–624. [Google Scholar] [CrossRef]
- Nardone, O.M.; Ponsiglione, A.; de Sire, R.; Calabrese, G.; Liuzzi, R.; Testa, A.; Guarino, A.D.; Olmo, O.; Rispo, A.; Camera, L. Impact of Sarcopenia on Clinical Outcomes in a Cohort of Caucasian Active Crohn’s Disease Patients Undergoing Multidetector CT-Enterography. Nutrients 2022, 14, 3460. [Google Scholar] [CrossRef]
- Nam, K.; Lee, J.Y.; Ko, Y.; Kim, K.W.; Lee, H.-S.; Hong, S.W.; Park, J.H.; Hwang, S.W.; Yang, D.-H.; Ye, B.D. Impact of Sarcopenia on Clinical Course of Inflammatory Bowel Disease in Korea. Dig. Dis. Sci. 2023, 68, 2165–2179. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Messina, C.; Vitale, J.; Sconfienza, L.M. Imaging of Sarcopenia: Old Evidence and New Insights. Eur. Radiol. 2020, 30, 2199–2208. [Google Scholar] [CrossRef]
- van der Werf, A.; Langius, J.a.E.; de van der Schueren, M.a.E.; Nurmohamed, S.A.; van der Pant, K.a.M.I.; Blauwhoff-Buskermolen, S.; Wierdsma, N.J. Percentiles for Skeletal Muscle Index, Area and Radiation Attenuation Based on Computed Tomography Imaging in a Healthy Caucasian Population. Eur. J. Clin. Nutr. 2018, 72, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Geng, N.; Zhou, Y.; Lin, N.; Song, W.; Xu, M.; Li, S.; Piao, Y.; Han, Z.; Guo, R.; et al. Defining Reference Values for Low Skeletal Muscle Index at the L3 Vertebra Level Based on Computed Tomography in Healthy Adults: A Multicentre Study. Clin. Nutr. 2022, 41, 396–404. [Google Scholar] [CrossRef]
- Yadav, D.P.; Kedia, S.; Madhusudhan, K.S.; Bopanna, S.; Goyal, S.; Jain, S.; Vikram, N.K.; Sharma, R.; Makharia, G.K.; Ahuja, V. Body Composition in Crohn’s Disease and Ulcerative Colitis: Correlation with Disease Severity and Duration. Can. J. Gastroenterol. Hepatol. 2017, 2017, 1215035. [Google Scholar] [CrossRef]
- Jiang, K.; Chen, B.; Lou, D.; Zhang, M.; Shi, Y.; Dai, W.; Shen, J.; Zhou, B.; Hu, J. Systematic Review and Meta-Analysis: Association between Obesity/Overweight and Surgical Complications in IBD. Int. J. Colorectal. Dis. 2022, 37, 1485–1496. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.S.; Malietzis, G.; Lung, P.F.C.; Penez, L.; Yip, W.M.; Gabe, S.; Jenkins, J.T.; Hart, A. The Body Composition Profile Is Associated with Response to Anti-TNF Therapy in Crohn’s Disease and May Offer an Alternative Dosing Paradigm. Aliment. Pharmacol. Ther. 2017, 46, 883–891. [Google Scholar] [CrossRef]
- Adams, D.W.; Gurwara, S.; Silver, H.J.; Horst, S.N.; Beaulieu, D.B.; Schwartz, D.A.; Seidner, D.L. Sarcopenia Is Common in Overweight Patients with Inflammatory Bowel Disease and May Predict Need for Surgery. Inflamm. Bowel Dis. 2017, 23, 1182–1186. [Google Scholar] [CrossRef]
- Singh, A.; Midha, V.; Mahajan, R.; Verma, S.; Kakkar, C.; Grover, J.; Singh, D.; Kaur, R.; Masih, A.; Bansal, N.; et al. Evaluation of Nutritional Characteristics Reveals Similar Prevalence of Malnutrition in Patients with Ulcerative Colitis and Crohn’s Disease. Dig. Dis. Sci. 2023, 68, 580–595. [Google Scholar] [CrossRef]
- Bamba, S.; Inatomi, O.; Takahashi, K.; Morita, Y.; Imai, T.; Ohno, M.; Kurihara, M.; Takebayashi, K.; Kojima, M.; Iida, H.; et al. Assessment of Body Composition from CT Images at the Level of the Third Lumbar Vertebra in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 27, 1435–1442. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the E. G. for E. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Mienche, M.; Setiati, S.; Setyohadi, B.; Kurniawan, J.; Laksmi, P.W.; Ariane, A.; Tirtarahardja, G. Diagnostic Performance of Calf Circumference, Thigh Circumference, and SARC-F Questionnaire to Identify Sarcopenia in Elderly Compared to Asian Working Group for Sarcopenia’s Diagnostic Standard. Acta Med. Indones 2019, 51, 117–127. [Google Scholar] [PubMed]
- Peng, T.-C. Role of Sarcopenia in Nonalcoholic Fatty Liver Disease: Definition Is Crucially Important. Hepatology 2018, 68, 788–789. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.C.; Hwang, S.Y.; Choi, H.Y.; Yoo, H.J.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Baik, S.H.; Choi, D.S.; Choi, K.M. Relationship between Sarcopenia and Nonalcoholic Fatty Liver Disease: The Korean Sarcopenic Obesity Study. Hepatology 2014, 59, 1772–1778. [Google Scholar] [CrossRef]
- Rojas-Feria, M.; Castro, M.; Suárez, E.; Ampuero, J.; Romero-Gómez, M. Hepatobiliary Manifestations in Inflammatory Bowel Disease: The Gut, the Drugs and the Liver. World J. Gastroenterol. 2013, 19, 7327–7340. [Google Scholar] [CrossRef]
- Radu, F.; Potcovaru, C.-G.; Salmen, T.; Filip, P.V.; Pop, C.; Fierbințeanu-Braticievici, C. The Link between NAFLD and Metabolic Syndrome. Diagnostics 2023, 13, 614. [Google Scholar] [CrossRef]
- Diaconu, C.-T.; Guja, C. Nonalcoholic Fatty Liver Disease and Its Complex Relation with Type 2 Diabetes Mellitus—From Prevalence to Diagnostic Approach and Treatment Strategies. J. Clin. Med. 2022, 11, 5144. [Google Scholar] [CrossRef]
- Moon, J.S.; Yoon, J.S.; Won, K.C.; Lee, H.W. The Role of Skeletal Muscle in Development of Nonalcoholic Fatty Liver Disease. Diabetes Metab J. 2013, 37, 278–285. [Google Scholar] [CrossRef]
- Zhao, H.; Cheng, R.; Song, G.; Teng, J.; Shen, S.; Fu, X.; Yan, Y.; Liu, C. The Effect of Resistance Training on the Rehabilitation of Elderly Patients with Sarcopenia: A Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15491. [Google Scholar] [CrossRef]
- Chang, M.C.; Choo, Y.J. Effects of Whey Protein, Leucine, and Vitamin D Supplementation in Patients with Sarcopenia: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 521. [Google Scholar] [CrossRef]
- Dhaliwal, A.; Quinlan, J.I.; Overthrow, K.; Greig, C.; Lord, J.M.; Armstrong, M.J.; Cooper, S.C. Sarcopenia in Inflammatory Bowel Disease: A Narrative Overview. Nutrients 2021, 13, 656. [Google Scholar] [CrossRef]
- Lee, H.J.; Song, J.-K.; Moon, J.; Kim, K.; Park, H.-K.; Kang, G.-W.; Shin, J.-H.; Kang, J.; Kim, B.-G.; Lee, Y.-H.; et al. Health-Related Quality of Life Using WHODAS 2.0 and Associated Factors 1 Year after Stroke in Korea: A Multi-Centre and Cross-Sectional Study. BMC Neurol. 2022, 22, 501. [Google Scholar] [CrossRef]
- Tandon, P.; Low, G.; Mourtzakis, M.; Zenith, L.; Myers, R.P.; Abraldes, J.G.; Shaheen, A.A.M.; Qamar, H.; Mansoor, N.; Carbonneau, M.; et al. A Model to Identify Sarcopenia in Patients with Cirrhosis. Clin. Gastroenterol. Hepatol. 2016, 14, 1473–1480.e3. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Fujita, E.; Thiebaud, R.S.; Loenneke, J.P.; Akamine, T. Ultrasound-Derived Forearm Muscle Thickness Is a Powerful Predictor for Estimating DXA-Derived Appendicular Lean Mass in Japanese Older Adults. Ultrasound Med. Biol. 2016, 42, 2341–2344. [Google Scholar] [CrossRef]
- Perkisas, S.; Bastijns, S.; Baudry, S.; Bauer, J.; Beaudart, C.; Beckwée, D.; Cruz-Jentoft, A.; Gasowski, J.; Hobbelen, H.; Jager-Wittenaar, H.; et al. Application of Ultrasound for Muscle Assessment in Sarcopenia: 2020 SARCUS Update. Eur. Geriatr. Med. 2021, 12, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Fink, J.D.S.; Marcadenti, A.; Rabito, E.I.; Silva, F.M. The New European Society for Clinical Nutrition and Metabolism Definition of Malnutrition: Application for Nutrition Assessment and Prediction of Morbimortality in an Emergency Service. JPEN J. Parenter. Enter. Nutr. 2017, 10, 014860711769524. [Google Scholar] [CrossRef]
- Shafer, L.A.; Walker, J.R.; Chhibba, T.; Ivekovic, M.; Singh, H.; Targownik, L.E.; Peyrin-Biroulet, L.; Gower-Rousseau, C.; Sarter, H.; Bernstein, C.N. Independent Validation of a Self-Report Version of the IBD Disability Index (IBDDI) in a Population-Based Cohort of IBD Patients. Inflamm. Bowel Dis. 2018, 24, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Leong, R.W.L.; Huang, T.; Ko, Y.; Jeon, A.; Chang, J.; Kohler, F.; Kariyawasam, V. Prospective Validation Study of the International Classification of Functioning, Disability and Health Score in Crohn’s Disease and Ulcerative Colitis. J. Crohns Colitis 2014, 8, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.Y.; Shin, J.E.; Park, S.H.; Park, D.I.; Cha, J.M. Disability Due to Inflammatory Bowel Disease Is Correlated with Drug Compliance, Disease Activity, and Quality of Life. Gut Liver 2017, 11, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.C.; Munsell, M.; Harris, M.L. Nationwide Prevalence and Prognostic Significance of Clinically Diagnosable Protein-Calorie Malnutrition in Hospitalized Inflammatory Bowel Disease Patients. Inflamm. Bowel Dis. 2008, 14, 1105–1111. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author (Reference) | Country | Number of Patients (CD/UC) | Mean Age ± SD | Gender (Female), % | BMI (kg/m2) | Sarcopenia Diagnosis (%) | Disease Duration |
|---|---|---|---|---|---|---|---|
| Subramaniam [20], 2015 | Australia | 19 (19/0) | 33.2 ± 10.7 | 58 | 24 ± 4.82 | NR | 101 ± 99.4 Months |
| Holt [21], 2017 | Australia | 34 (34/0) | 37.8 ± 14.2 | 54.5 | 23.5 ± 4.9 | 41 | 5.5 ± 4.0 years |
| Zhao [22], 2022 | China | 28 (−/−) | 44.1 | 32.14 | 21.2 | 100 | NR |
| Kang [23], 2020 | Korea | 433(169/264) | 39.3 | 35.9 | NR | NR | 186.2 months |
| Ciocîrlan [24], 2019 | Romania | 625 (241/365) | 44.1 ± 14.6 | 44.05 | NR | NR | NR |
| Bian [25], 2021 | China | 146 (145/0) | 38.89 ± 10.68 | 33.57 | 19.67 ± 3.37 | 44.41 | 4.99 ± 4.91 years |
| Kochar [26], 2020 | USA | 11,001 (−/−) | 46 | 53 | NR | NR | NR |
| Huang [27], 2021 | China | 72 (48/25) | 36.00 | 28.8 | 20.13 ± 3.04 | NR | 5 years |
| Boparai [28], 2021 | India | 44 (44/0) | 34.4 ± 14.1 | 36.4 | NR | 43 | 48 months |
| Ge X [29], 2021 | China | 254 (0/254) | 43.9 ± 0.9 | 36.6 | 20.8 ± 0.2 | 50 | 62.4 ± 4.1 months |
| Fiorindi [30], 2020 | Italy | 53 (38/15) | 51.08 ± 15.06 | 4//2 | NR | NR | 11 years |
| Zhou [31], 2021 | China | 122 (122/0) | 32.5 ± 12.04 | 22.13 | 18.49 ± 2.80 | 58.85 | 2.19 ± 3.93 years |
| Higashiyama [32], 2021 | Japan | 2778 (0/2778) | NR | NR | NR | NR | NR |
| Pribadi [33], 2022 | Indonesia | 85 (37/48) | 42 | 70.06 | NR | 12.9 | NR |
| Nardone [34], 2022 | Switzerland | 63 (63/0) | 44.2 ± 17.0 | 46 | 21.2 ± 3.6 | 68.3 | 140.0 ± 106.5 months |
| Nam [35], 2022 | Korea | 1027 (854/173) | NR | NR | NR | NR | NR |
| Author (Reference) | Cut-Off Values (cm2/m2) |
|---|---|
| Boparai [28], 2021 | 36.54 ♂ |
| 30.21 ♀ | |
| Ge X [29], 2021 | 42.44 ♂ |
| 33.48 ♀ | |
| Zhou [31], 2021 | NR |
| Nardone [34], 2022 | 52.4 ♂ |
| 38.5 ♀ | |
| Nam [35], 2022 | 49 ♂ |
| 31 ♀ |
| Author (Reference) | Patients with Sarcopenia | Patients without Sarcopenia | p Value | |
|---|---|---|---|---|
| Boparai [28], 2021 CD patients | Number of patients | 19 | 25 | |
| BMI (kg/m2) | 17.2 ± 4.5 | 21.5 ± 3.4 | 0.001 | |
| VF area (cm2) | 77.27 ± 36.9 | 109.2 ± 58.3 | 0.04 | |
| SC area (cm2) | 89.76 ± 65.1 | 141.7 ± 85.9 | 0.03 | |
| VF/SC ratio | 1.26 ± 0.9 | 0.87 ± 0.3 | 0.06 | |
| SMI (cm2/m2) | 27.45 ± 4.9 | 39.55 ± 4.89 | ˂0.001 | |
| Ge X [29], 2021, UC patients | Number of patients | 127 | 127 | |
| BMI (kg/m2) | 20.2 ± 3.5 | 21.3 ± 3.0 | 0.006 | |
| VF area (cm2) | 62.8 ± 40.3 | 66.4 ± 37.2 | 0.457 | |
| SC area (cm2) | 96.2 ± 46.6 | 115.9 ± 50.4 | 0.001 | |
| VF/SC ratio | 0.75 ± 0.49 | 0.61 ± 0.31 | 0.006 | |
| SMI (cm2/m2) | NR | NR | ||
| Nardone [34], 2022, CD patients | Number of patients | 43 | 20 | |
| BMI (kg/m2) | 20.3 ± 3.1 | 23.3 ± 3.8 | 0.002 | |
| VF area (cm2) | 54.0 ± 63.1 | 63.4 ± 62.7 | 0.54 | |
| SC area (cm2) | 94.1 ± 90.4 | 149.9 ± 84.2 | 0.009 | |
| VF/SC ratio | 0.7 ± 0.6 | 0.4 ± 0.4 | 0.04 | |
| SMI (cm2/m2) | NR | NR | ||
| Nam [35], 2022, CD patients | Number of patients | 491 | 363 | |
| BMI (kg/m2) | 20.1 ± 3.3 | 19.2 ± 3.3 | ˂0.0001 | |
| VF area (cm2) | 34.4 ± 28.4 | 49.7 ± 45.0 | ˂0.0001 | |
| SC area (cm2) | 74.0 ± 57.2 | 93.4 ± 70.9 | ˂0.0001 | |
| VF/SC ratio | 0.68 ± 0.78 | 0.69 ± 0.58 | 0.900 | |
| SMI (cm2/m2) | 37.0 ± 7.9 | 52.5 ± 10.2 | ˂0.0001 | |
| Nam [35], 2022, UC patients | Number of patients | 92 | 81 | |
| BMI (kg/m2) | 22.4 ± 3.9 | 21.6 ± 2.7 | ˂0.0001 | |
| VF area (cm2) | 31.6 ± 27.2 | 42.4 ± 36.8 | 0.032 | |
| SC area (cm2) | 63.5 ± 45.6 | 83.2 ± 57.7 | 0.015 | |
| VF/SC ratio | 0.77 ± 1.06 | 0.58 ± 0.36 | 0.108 | |
| SMI (cm2/m2) | 36.9 ± 7.8 | 53.9 ± 0.6 | ˂0.0001 | |
| Patients with adverse outcome | Patients without adverse outcome | |||
| Zhou [31], 2021 | Number of patients | 49 | 73 | |
| BMI (kg/m2) | 17.61 ± 2.41 | 18.85 ± 2.78 | 0.012 | |
| VF area (cm2) | 40.08 ± 42.98 | 57.54 ± 45.59 | 0.036 | |
| SC area (cm2) | 39.18 ± 45.61 | 62.37 ± 51.44 | 0.012 | |
| VF/SC ratio | 8.06 ± 25.98 | 1.22 ± 0.99 | 0.026 | |
| SMI (cm2/m2) | 40.15 ± 6.81 | 42.93 ± 7.86 | 0.046 |
| Author (Reference) | Method Used | Muscle Gain Assessment | Muscle Strength Assessment | Physical Activity Assessment |
| Subramaniam [20] | IFX | Thigh VM | Quadriceps muscle strength at 3 speeds of contraction with an isokinetic dynamometer | IPAQ short form |
| Zhao [22] | WP RT WP + RT | ASM/H2 CC HC Waist/hip ratio | HGS | 5CST 3-m walk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potcovaru, C.-G.; Filip, P.V.; Neagu, O.-M.; Diaconu, L.S.; Salmen, T.; Cinteză, D.; Pantea Stoian, A.; Bobirca, F.; Berteanu, M.; Pop, C. Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review. J. Clin. Med. 2023, 12, 4713. https://doi.org/10.3390/jcm12144713
Potcovaru C-G, Filip PV, Neagu O-M, Diaconu LS, Salmen T, Cinteză D, Pantea Stoian A, Bobirca F, Berteanu M, Pop C. Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review. Journal of Clinical Medicine. 2023; 12(14):4713. https://doi.org/10.3390/jcm12144713
Chicago/Turabian StylePotcovaru, Claudia-Gabriela, Petruța Violeta Filip, Oana-Maria Neagu, Laura Sorina Diaconu, Teodor Salmen, Delia Cinteză, Anca Pantea Stoian, Florin Bobirca, Mihai Berteanu, and Corina Pop. 2023. "Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review" Journal of Clinical Medicine 12, no. 14: 4713. https://doi.org/10.3390/jcm12144713
APA StylePotcovaru, C.-G., Filip, P. V., Neagu, O.-M., Diaconu, L. S., Salmen, T., Cinteză, D., Pantea Stoian, A., Bobirca, F., Berteanu, M., & Pop, C. (2023). Diagnostic Criteria and Prognostic Relevance of Sarcopenia in Patients with Inflammatory Bowel Disease—A Systematic Review. Journal of Clinical Medicine, 12(14), 4713. https://doi.org/10.3390/jcm12144713