
An Observational Study to Develop a Predictive Model for Bacterial Pneumonia Diagnosis in Severe COVID-19 Patients—C19-PNEUMOSCORE
 , , , , ,
, , , , ,  , , , , , , and
, , , , , , and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. Study Setting and Design
2.2. Definitions and Outcomes
2.3. Statistical Analysis
2.4. Microbiological Analysis
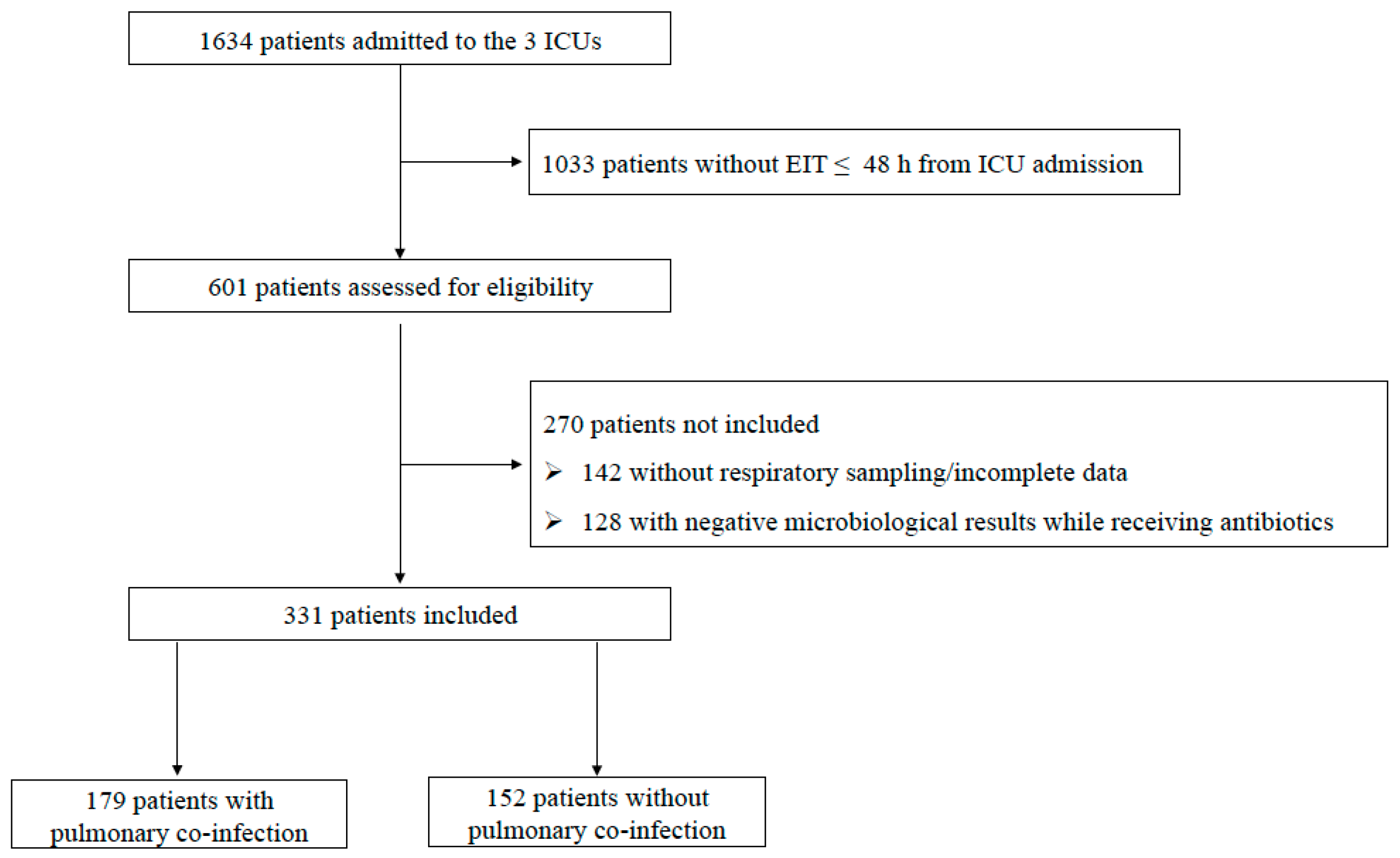
3. Results
3.1. Population Characteristics, Treatments and Outcomes
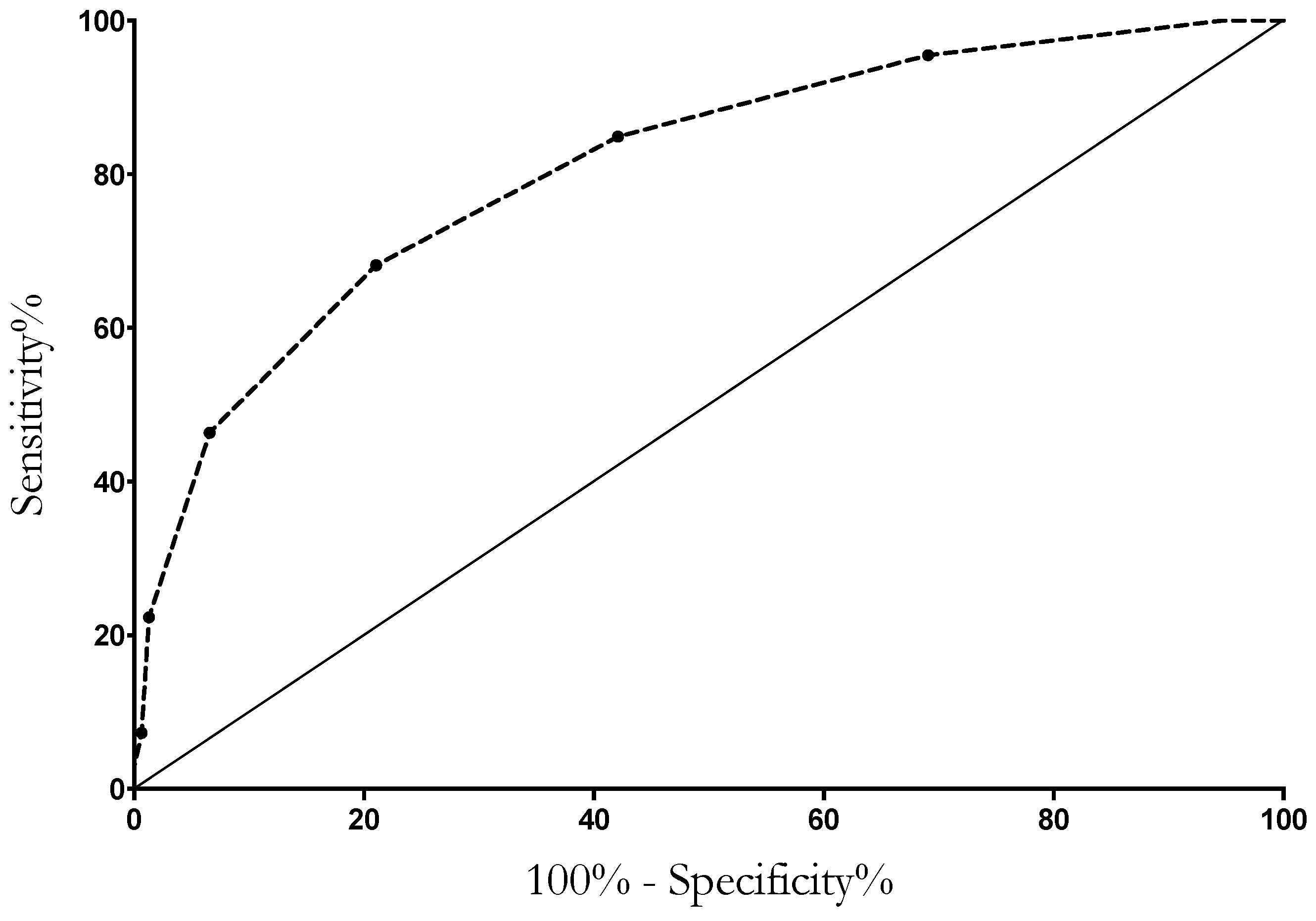
3.2. Factors Associated with Bacterial Pulmonary Co-Infection and Score Development
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Langerbeins, P.; Hallek, M. COVID-19 in patients with hematologic malignancy. Blood 2022, 140, 236–252. [Google Scholar] [CrossRef]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-Y.; Chang, P.-H.; Chen, K.-Y.; Lin, I.-F.; Hsih, W.-H.; Tsai, W.-L.; Chen, J.-A.; Lee, S.S.-J. Coronavirus disease 2019 (COVID-19) associated bacterial coinfection: Incidence, diagnosis and treatment. J. Microbiol. Immunol. Infect. 2022, 55, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhu, Q.; Xiao, Y.; Wu, C.; Jiang, Z.; Liu, L.; Qu, J. Clinical and etiological analysis of co-infections and secondary infections in COVID-19 patients: An observational study. Clin. Respir. J. 2021, 15, 815–825. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Giannella, M.; Rinaldi, M.; Tesini, G.; Gallo, M.; Cipriani, V.; Vatamanu, O.; Campoli, C.; Toschi, A.; Ferraro, G.; Horna, C.S.; et al. Predictive model for bacterial co-infection in patients hospitalized for COVID-19: A multicenter observational cohort study. Infection 2022, 50, 1243–1253. [Google Scholar] [CrossRef]
- Nasir, N.; Rehman, F.; Omair, S.F. Risk factors for bacterial infections in patients with moderate to severe COVID-19: A case-control study. J. Med. Virol. 2021, 93, 4564–4569. [Google Scholar] [CrossRef]
- Santos, A.P.; Gonçalves, L.C.; Oliveira, A.C.C.; Queiroz, P.H.P.; Ito, C.R.M.; Santos, M.O.; Carneiro, L.C. Bacterial Co-Infection in Patients with COVID-19 Hospitalized (ICU and Not ICU): Review and Meta-Analysis. Antibiotics 2022, 11, 894. [Google Scholar] [CrossRef]
- Vaughn, V.M.; Gandhi, T.N.; Petty, L.A.; Patel, P.K.; Prescott, H.C.; Malani, A.N.; Ratz, D.; McLaughlin, E.; Chopra, V.; Flanders, S.A. Empiric Antibacterial Therapy and Community-onset Bacterial Coinfection in Patients Hospitalized with Coronavirus Disease 2019 (COVID-19): A Multi-Hospital Cohort Study. Clin. Infect. Dis. 2021, 72, e533–e541. [Google Scholar] [CrossRef]
- Granata, G.; Schiavone, F.; Pipitone, G.; Taglietti, F.; Petrosillo, N. Antibiotics Use in COVID-19 Patients: A Systematic Literature Review. J. Clin. Med. 2022, 11, 7207. [Google Scholar] [CrossRef]
- Bolker, A.; Coe, K.; Smith, J.; Stevenson, K.; Wang, S.H.; Reed, E. Predictors of respiratory bacterial co-infection in hospitalized COVID-19 patients. Diagn. Microbiol. Infect. Dis. 2022, 102, 115558. [Google Scholar] [CrossRef] [PubMed]
- Kreitmann, L.; Monard, C.; Dauwalder, O.; Simon, M.; Argaud, L. Early bacterial co-infection in ARDS related to COVID-19. Intensive Care Med. 2020, 46, 1787–1789. [Google Scholar] [CrossRef] [PubMed]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Metzelard, M.; Du Cheyron, D.; Lambiotte, F.; Tamion, F.; Labruyere, M.; Geronimi, C.B.; Nieszkowska, A.; et al. Early Bacterial Identification among Intubated Patients with COVID-19 or Influenza Pneumonia: A European Multicenter Comparative Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Le Gall, J.-R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J. The strengthening the reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- De Pascale, G.; Bello, G.; Tumbarello, M.; Antonelli, M. Severe pneumonia in intensive care: Cause, diagnosis, treatment and management: A review of the literature. Curr. Opin. Pulm. Med. 2012, 18, 213–221. [Google Scholar] [CrossRef]
- Ranzani, O.T.; De Pascale, G.; Park, M. Diagnosis of nonventilated hospital-acquired pneumonia: How much do we know? Curr. Opin. Crit. Care 2018, 24, 339–346. [Google Scholar] [CrossRef]
- Borghesi, A.; Zigliani, A.; Golemi, S.; Carapella, N.; Maculotti, P.; Farina, D.; Maroldi, R. Chest X-ray severity index as a predictor of in-hospital mortality in coronavirus disease 2019: A study of 302 patients from Italy. Int. J. Infect. Dis. 2020, 96, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Hanson, K.E.; Caliendo, A.M.; Arias, C.A.; Hayden, M.K.; Englund, J.A.; Lee, M.J.; Loeb, M.; Patel, R.; El Alayli, A.; Altayar, O.; et al. The Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Molecular Diagnostic Testing. Clin. Infect. Dis. 2021, ciab048. [Google Scholar] [CrossRef] [PubMed]
- Posteraro, B.; Cortazzo, V.; Liotti, F.M.; Menchinelli, G.; Ippoliti, C.; De Angelis, G.; La Sorda, M.; Capalbo, G.; Vargas, J.; Antonelli, M.; et al. Diagnosis and Treatment of Bacterial Pneumonia in Critically Ill Patients with COVID-19 Using a Multiplex PCR Assay: A Large Italian Hospital’s Five-Month Experience. Microbiol. Spectr. 2021, 9, e0069521. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and viral co-infections in patients with severe SARS-CoV-2 pneumonia admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Molina, F.J.; Botero, L.E.; Isaza, J.P.; Cano, L.E.; López, L.; Tamayo, L.; Torres, A. Diagnostic concordance between BioFire® FilmArray® Pneumonia Panel and culture in patients with COVID-19 pneumonia admitted to intensive care units: The experience of the third wave in eight hospitals in Colombia. Crit. Care 2022, 26, 130. [Google Scholar] [CrossRef]
- Grasselli, G.; Scaravilli, V.; Mangioni, D.; Scudeller, L.; Alagna, L.; Bartoletti, M.; Bellani, G.; Biagioni, E.; Bonfanti, P.; Bottino, N.; et al. Hospital-Acquired Infections in Critically Ill Patients with COVID-19. Chest 2021, 160, 454–465. [Google Scholar] [CrossRef]
- Greco, M.; De Corte, T.; Ercole, A.; Antonelli, M.; Azoulay, E.; Citerio, G.; Morris, A.C.; De Pascale, G.; Duska, F.; Elbers, P.; et al. Clinical and organizational factors associated with mortality during the peak of first COVID-19 wave: The global UNITE-COVID study. Intensive Care Med. 2022, 48, 690–705, Erratum in Intensive Care Med. 2022, 48, 1130–1131. [Google Scholar] [CrossRef]
- Schouten, J.; De Waele, J.; Lanckohr, C.; Koulenti, D.; Haddad, N.; Rizk, N.; Sjövall, F.; Kanj, S.S. Antimicrobial stewardship in the ICU in COVID times: The known unknowns. Int. J. Antimicrob. Agents 2021, 58, 106409. [Google Scholar] [CrossRef]
- De Waele, J.J.; Derde, L.; Bassetti, M. Antimicrobial stewardship in ICUs during the COVID-19 pandemic: Back to the 90s? Intensive Care Med. 2021, 47, 104–106. [Google Scholar] [CrossRef]
- Bonazzetti, C.; Rinaldi, M.; Giacomelli, A.; Colombo, R.; Ottolina, D.; Rimoldi, S.G.; Pagani, C.; Morena, V.; Ridolfo, A.L.; Vatamanu, O.; et al. Risk factors associated with bacteremia in COVID-19 patients admitted to intensive care unit: A retrospective multicenter cohort study. Infection 2023, 51, 129–136. [Google Scholar] [CrossRef]
- De Pascale, G.; De Maio, F.; Carelli, S.; De Angelis, G.; Cacaci, M.; Montini, L.; Bello, G.; Cutuli, S.L.; Pintaudi, G.; Tanzarella, E.S.; et al. Staphylococcus aureus ventilator-associated pneumonia in patients with COVID-19: Clinical features and potential inference with lung dysbiosis. Crit. Care 2021, 25, 197. [Google Scholar] [CrossRef]
- Grasselli, G.; Zanella, A.; Carlesso, E.; Florio, G.; Canakoglu, A.; Bellani, G.; Bottino, N.; Cabrini, L.; Castelli, G.P.; Catena, E.; et al. Association of COVID-19 Vaccinations with Intensive Care Unit Admissions and Outcome of Critically Ill Patients with COVID-19 Pneumonia in Lombardy, Italy. JAMA Netw. Open 2022, 5, e2238871. [Google Scholar] [CrossRef]
- Espi, M.; Koppe, L.; Fouque, D.; Thaunat, O. Chronic Kidney Disease-Associated Immune Dysfunctions: Impact of Protein-Bound Uremic Retention Solutes on Immune Cells. Toxins 2020, 12, 300. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Li, J.; Wei, W.; Yi, C.; Pu, Y.; Zhang, L.; Cui, T.; Ma, L.; Zhang, J.; Koyner, J.; et al. Kidney health in the COVID-19 pandemic: An umbrella review of meta-analyses and systematic reviews. Front. Public Health 2022, 10, 963667. [Google Scholar] [CrossRef] [PubMed]
- Carbonell, R.; Urgelés, S.; Salgado, M.; Rodríguez, A.; Reyes, L.F.; Fuentes, Y.V.; Serrano, C.C.; Caceres, E.L.; Bodí, M.; Martín-Loeches, I.; et al. Negative predictive value of procalcitonin to rule out bacterial respiratory co-infection in critical COVID-19 patients. J. Infect. 2022, 85, 374–381. [Google Scholar] [CrossRef]
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y.; et al. Prognostic Value of C-Reactive Protein in Patients with Coronavirus 2019. Clin. Infect. Dis. 2020, 71, 2174–2179. [Google Scholar] [CrossRef] [PubMed]
- Houghton, R.; Moore, N.; Williams, R.; El-Bakri, F.; Peters, J.; Mori, M.; Vernet, G.; Lynch, J.; Lewis, H.; Tavener, M.; et al. C-reactive protein-guided use of procalcitonin in COVID-19. JAC-Antimicrob. Resist. 2021, 3, dlab180. [Google Scholar] [CrossRef]
- Fartoukh, M.; Nseir, S.; Mégarbane, B.; Cohen, Y.; Lafarge, A.; Contou, D.; Thille, A.W.; Galerneau, L.M.; Reizine, F.; Cour, M.; et al. Respiratory multiplex PCR and procalcitonin to reduce antibiotic exposure in severe SARS-CoV-2 pneumonia: A multicentre randomized controlled trial. Clin. Microbiol. Infect. 2023, 29, 734–743. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | No. of Patients | No. of Patients | Univariate Analysis | ||
|---|---|---|---|---|---|
| Total Cohort (n = 331) | No Co-Infection (n = 152) | Co-Infection (n = 179) | p Value | OR (95% CI) | |
| Demographics and comorbidities | |||||
| Age, years | 67 [59–74] | 65 [58–72] | 68.5 [60–74] | 0.23 | 1.01 (0.99–1.03) |
| Gender (male) | 233 (70.4) | 101 (66.45) | 132 (73.74) | 0.15 | 1.42 (0.88–2.28) |
| COVID-19 Vaccinated | 24 (7.3) | 3 (2) | 21 (11.73) | 0.003 | 6.6 (1.93–22.59) |
| Recent hospitalization * | 29 (8.8) | 8 (5.3) | 21 (11.7) | 0.04 | 2.39 (1.03–5.57) |
| BMI ≥ 30 kg/m2 | 96 (29.0) | 55 (36.2) | 41 (22.9) | 0.008 | 0.52 (0.32–0.85) |
| CHD ** | 69 (20.8) | 20 (13.2) | 49 (27.4) | 0.002 | 2.49 (1.40–4.42) |
| COPD | 70 (21.1) | 29 (19.1) | 41 (22.9) | 0.39 | 1.26 (0.74–2.15) |
| Non-cardiac vasculopathy | 45 (13.6) | 13 (8.6) | 32 (17.9) | 0.02 | 2.33 (1.17–4.62) |
| Diabetes | 89 (26.9) | 34 (22.4) | 55 (30.7) | 0.09 | 1.54 (0.94–2.53) |
| CKD | 41 (12.4) | 7 (4.6) | 34 (19.0) | <0.001 | 4.86 (2.09–11.31) |
| Immunosuppression *** | 60 (18.0) | 26 (17.0) | 34 (19.0) | 0.51 | 0.83 (0.47–1.46) |
| CLD | 13 (3.9) | 7 (4.6) | 6 (3.4) | 0.56 | 0.72 (0.23–2.19) |
| Charlson index | 3 [2–5] | 3 [2–4] | 4 [2–5] | <0.01 | 1.23 (1.1–1.38) |
| Clinical ICU presenting features | |||||
| SAPS II score | 39 [30–52] | 36 [27–45] | 42 [33–57] | <0.01 | 1.04 (1.03–1.06) |
| SOFA score | 5 [4–7] | 4 [3–6] | 5 [4–7] | <0.01 | 1.24 (1.12–1.36) |
| Pre-ICU Hospital LOS, days | 5 [2–8] | 4 [2–7] | 5 [3–9] | 0.025 | 1.05 (1.01–1.10) |
| Time from symptoms, days | 9 [6–13] | 9 [5–12] | 10 [6–14] | 0.38 | 1.02 (0.98–1.05) |
| Septic Shock | 74 (22.4) | 29 (19.1) | 45 (25.1) | 0.19 | 1.42 (0.84–2.4) |
| Barotrauma | 43 (13.0) | 23 (15.1) | 20 (11.2) | 0.29 | 0.71 (0.37–1.34) |
| Pulmonary embolism | 18 (5.4) | 5 (3.3) | 13 (7.3) | 0.12 | 2.30 (0.80–6.61) |
| MDR colonization **** | 64 (19.3) | 19 (12.5) | 45 (25.1) | 0.004 | 2.35 (1.31–4.23) |
| PaO2/FiO2 | 88 [75–101] | 88 [76–101] | 88 [73–101] | 0.69 | 1.00 (0.99–1.01) |
| Body Temperature, T° | 37.0 [36.5–37.6] | 37.0 [36.4–37.4] | 37.0 [36.5–37.6] | 0.27 | 1.13 (0.91.1.42) |
| Laboratory ICU presenting features | |||||
| WBC (109/L) | 10.60 [7.65–15.11] | 9.50 [6.89–13.05] | 11.51 [8.30–16.36] | 0.72 | 1.00 (0.99–1.02) |
| Neutrophils (109/L) | 9.41 [6.55–13.28] | 8.39 [6.09–11.67] | 10.09 [6.92–14.35] | 0.002 | 1.07 (1.03–1.12) |
| Lymphocytes (109/L) | 0.68 [0.46–0.95] | 0.69 [0.47–1.07] | 0.65 [0.43–0.90] | 0.48 | 0.99 (0.95–1.02) |
| PCT, ng/mL | 0.20 [0.09–0.42] | 0.12 [0.06–0.20] | 0.29 [0.14–0.98] | <0.001 | 39.07 (9.37–162.94) |
| CRP, mg/L | 107.60 [51.7–169.50] | 86.40 [45.15–163.15] | 128.75 [62.75–180.89] | <0.001 | 1.005 (1.003–1.008) |
| Platelets (109/L) | 244 [174–312] | 251 [186–329] | 236 [162–295] | 0.02 | 0.99 (0.99–1.00) |
| D-Dimer, mg/L | 1954 [868–4262] | 1472 [727–3735] | 2142 [965–4895] | 0.94 | 1.00 (1.00–1.00) |
| LDH, U/L | 399 [319–513] | 399 [323–529] | 402 [316–508] | 0.51 | 1.00 (1.00–1.00) |
| Fibrinogen, mg/dL | 531 [416–677] | 530 [416–687] | 535 [414–674] | 0.80 | 1.00 (1.00–1.00) |
| Radiology ICU presenting features | |||||
| Brixia score, total | 9 [6–13] | 8 [5–10] | 10 [8–12] | <0.001 | 1.18 (1.11–1.26) |
| Monolateral consolidation | 114 (34.4) | 46 (30.3) | 68 (38.0) | 0.14 | 1.41 (0.89–2.23) |
| Bilateral consolidation | 76 (22.9) | 28 (18.4) | 48 (26.8) | 0.07 | 1.62 (0.96–2.75) |
| Monolateral effusion | 77 (23.3) | 32 (21.1) | 45 (25.1) | 0.38 | 1.26 (0.75–2.11) |
| Bilateral effusion | 36 (10.9) | 16 (10.5) | 20 (11.2) | 0.85 | 1.07 (0.53–2.14) |
| Treatments at ICU admission | |||||
| Dexamethasone | 281 (84.9) | 128 (84.2) | 153 (85.5) | 0.75 | 1.10 (0.60–2.01) |
| Remdesivir | 160 (48.3) | 75 (49.3) | 85 (47.5) | 0.74 | 0.93 (0.60–1.43) |
| IL-6 inhibitors | 44 (13.3) | 20 (13.2) | 24 (13.4) | 0.95 | 1.02 (0.54–1.93) |
| Outcomes | |||||
| Post-BAL ICU LOS, days | 15 [8–25] | 16 [11–30] | 13 [6–23] | 0.51 | 0.99 (0.98–1.01) |
| Post-BAL Hospital LOS, days | 20 [9–36] | 22 [13–38] | 16 [7–35] | 0.62 | 1.00 (0.99–1.01) |
| Tracheostomy | 109 (32.9) | 54 (35.5) | 55 (30.7) | 0.36 | 0.81 (0.51–1.28) |
| 28-day mortality | 144 (43.5) | 66 (43.4) | 78 (43.6) | 0.98 | 1.01 (0.65–1.56) |
| 90-day mortality | 166 (50.3) | 77 (51.0) | 89 (49.7) | 0.82 | 0.95 (0.62–1.47) |
| Variable | Total (n = 179) |
|---|---|
| Ongoing empiric antimicrobial therapy | 60 (33.5) |
| Cephalosporins | 21 (11.7) |
| β-lactamase + inhibitors | 27 (15.1) |
| Macrolides | 19 (10.6) |
| Fluoroquinolones | 6 (3.4) |
| Linezolid | 6 (3.4) |
| Vancomycin | 5 (2.8) |
| Carbapenems | 4 (2.2) |
| Other antibiotics * | 5 (2.8) |
| Microbiological data | |
| Gram-positive cocci | 102 (57) |
| - Methicillin-sensitive Staphylococcus aureus | 51 (28.5) |
| - Methicillin-resistant Staphylococcus aureus | 29 (16.2) |
| - Streptococcus pneumoniae | 14 (7.8) |
| - Other Gram-positive germs ** | 8 (4.5) |
| Gram-negative bacilli | 113 (63.1) |
| - Pseudomonas aeruginosa | 31 (17.3) |
| - Klebsiella pneumoniae | 25 (13.9) |
| - Haemophilus influenzae | 14 (7.8) |
| - Escherichia coli | 9 (5.0) |
| - Other Klebsiella spp. | 9 (5.0) |
| - Enterobacter cloacae | 7 (3.9) |
| - Stenotrophomonas maltophilia | 6 (3.4) |
| - Other Gram-negative germs *** | 12 (6.7) |
| MDR | 36 (20.1) |
| Polymicrobial **** | 42 (23.5) |
| Concomitant BSI | 32 (17.9) |
| Variables | p Value | OR (95% CI) | β Value | Risk Score Point |
|---|---|---|---|---|
| COVID-19 Vaccinated | 0.006 | 7.01 (1.73–28.39) | 1.95 | 2 |
| CKD | 0.026 | 3.16 (1.15–8.71) | 1.15 | 1 |
| Pre-ICU Hospital LOS ≥ 5, days | 0.021 | 1.94 (1.11–3.4) | 0.74 | 1 |
| Neutrophils, ≥9.4 (109/L) | 0.013 | 1.96 (1.16–3.30) | 0.67 | 1 |
| PCT ≥ 0.2 ng/mL | <0.001 | 5.09 (2.93–8.84) | 1.63 | 2 |
| CRP ≥ 108 mg/L | 0.015 | 1.99 (1.15–3.46) | 0.69 | 1 |
| BRIXIA score ≥ 9 | 0.009 | 2.03 (1.19–3.45) | 0.71 | 1 |
| C19-PNEUMOSCORE | TP | FP | TN | FN | Se (%) | Sp (%) | PPV (%) | NPV (%) | Acc (%) | Youden Index |
|---|---|---|---|---|---|---|---|---|---|---|
| Score ≥ 1 | 179 | 144 | 8 | 0 | 100 | 5.3 | 55.4 | 1 | 56.5 | 0.05 |
| Score ≥ 2 | 171 | 105 | 47 | 8 | 95.5 | 30.9 | 62.0 | 85.5 | 65.9 | 0.26 |
| Score ≥ 3 | 152 | 64 | 88 | 27 | 84.9 | 57.9 | 70.4 | 76.5 | 72.5 | 0.43 |
| Score ≥ 4 | 122 | 32 | 120 | 57 | 68.2 | 78.9 | 79.2 | 67.8 | 73.1 | 0.47 |
| Score ≥ 5 | 83 | 10 | 142 | 96 | 46.4 | 93.4 | 89.2 | 59.7 | 68.0 | 0.4 |
| Score ≥ 6 | 40 | 2 | 150 | 139 | 22.3 | 98.7 | 95.2 | 51.9 | 57.4 | 0.21 |
| Score ≥ 7 | 13 | 1 | 151 | 166 | 7.3 | 99.3 | 92.9 | 47.6 | 49.5 | 0.07 |
| Score ≥ 8 | 5 | 0 | 152 | 174 | 2.8 | 100 | 100 | 46.6 | 47.4 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanzarella, E.S.; Vargas, J.; Menghini, M.; Postorino, S.; Pozzana, F.; Vallecoccia, M.S.; De Matteis, F.L.; Franchi, F.; Infante, A.; Larosa, L.; et al. An Observational Study to Develop a Predictive Model for Bacterial Pneumonia Diagnosis in Severe COVID-19 Patients—C19-PNEUMOSCORE. J. Clin. Med. 2023, 12, 4688. https://doi.org/10.3390/jcm12144688
Tanzarella ES, Vargas J, Menghini M, Postorino S, Pozzana F, Vallecoccia MS, De Matteis FL, Franchi F, Infante A, Larosa L, et al. An Observational Study to Develop a Predictive Model for Bacterial Pneumonia Diagnosis in Severe COVID-19 Patients—C19-PNEUMOSCORE. Journal of Clinical Medicine. 2023; 12(14):4688. https://doi.org/10.3390/jcm12144688
Chicago/Turabian StyleTanzarella, Eloisa Sofia, Joel Vargas, Marco Menghini, Stefania Postorino, Francesca Pozzana, Maria Sole Vallecoccia, Francesco Lorenzo De Matteis, Federico Franchi, Amato Infante, Luigi Larosa, and et al. 2023. "An Observational Study to Develop a Predictive Model for Bacterial Pneumonia Diagnosis in Severe COVID-19 Patients—C19-PNEUMOSCORE" Journal of Clinical Medicine 12, no. 14: 4688. https://doi.org/10.3390/jcm12144688
APA StyleTanzarella, E. S., Vargas, J., Menghini, M., Postorino, S., Pozzana, F., Vallecoccia, M. S., De Matteis, F. L., Franchi, F., Infante, A., Larosa, L., Mazzei, M. A., Cutuli, S. L., Grieco, D. L., Bisanti, A., Carelli, S., Lombardi, G., Piervincenzi, E., Pintaudi, G., Pirronti, T., ... De Pascale, G. (2023). An Observational Study to Develop a Predictive Model for Bacterial Pneumonia Diagnosis in Severe COVID-19 Patients—C19-PNEUMOSCORE. Journal of Clinical Medicine, 12(14), 4688. https://doi.org/10.3390/jcm12144688