
Drug Retention Rates and the Safety of Janus Kinase Inhibitors in Elderly Patients with Rheumatoid Arthritis
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Clinical Evaluations
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Elderly Patients with RA
3.2. Reasons and Rates of Drug Discontinuation
3.3. Drug Discontinuation Rate Due to AEs
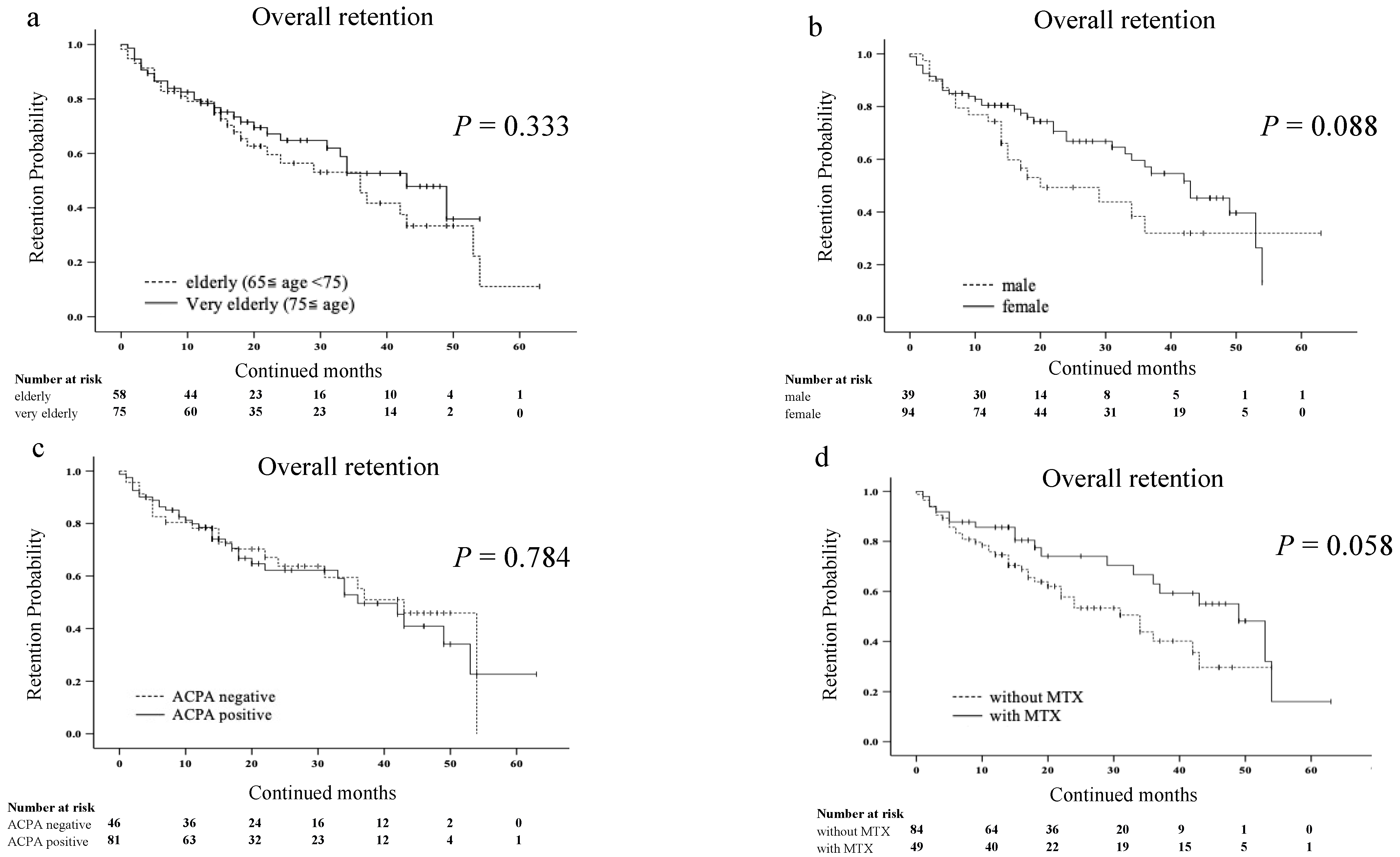
3.4. Drug Retention Rates and Types or Dosage of JAKis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| JAKis | Janus kinase inhibitors |
| RA | Rheumatoid arthritis |
| AEs | adverse events |
| ACPA | anti-citrullinated protein/peptide antibody |
| bDMARD | Biological disease modifying anti rheumatic drug |
| MACE | major adverse cardiovascular events |
| MTX | methotrexate |
| RF | rheumatoid factor |
| CRP: | C-reactive protein |
| GC | glucocorticoid |
References
- Villarino, A.V.; Kanno, Y.; O’Shea, J.J. Mechanisms and consequences of Jak-STAT signaling in the immune system. Nat. Immunol. 2017, 18, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.M.; Kanno, Y.; Villarino, A.; Ward, M.; Gadina, M.; O’Shea, J.J. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat. Rev. Drug Discov. 2017, 17, 78. [Google Scholar] [CrossRef]
- Tanaka, Y.; Luo, Y.; O’Shea, J.J.; Nakayamada, S. Janus kinase-targeting therapies in rheumatology: A mechanisms-based approach. Nat. Rev. Rheumatol. 2022, 18, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.; Xue, L.; Wang, Q.; Lu, W.; Xu, J.; Liu, Z. Comparative efficacy and safety of Janus kinase inhibitors and biological disease-modifying antirheumatic drugs in rheumatoid arthritis: A systematic review and network meta-analysis. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720x21999564. [Google Scholar] [CrossRef] [PubMed]
- Serhal, L.; Lwin, M.N.; Holroyd, C.; Edwards, C.J. Rheumatoid arthritis in the elderly: Characteristics and treatment considerations. Autoimmun. Rev. 2020, 19, 102528. [Google Scholar] [CrossRef]
- Liu, L.; Yan, Y.D.; Shi, F.H.; Lin, H.W.; Gu, Z.C.; Li, J. Comparative efficacy and safety of JAK inhibitors as monotherapy and in combination with methotrexate in patients with active rheumatoid arthritis: A systematic review and meta-analysis. Front. Immunol. 2022, 13, 977265. [Google Scholar] [CrossRef]
- Novella-Navarro, M.; Balsa, A. Difficult-to-Treat Rheumatoid Arthritis in Older Adults: Implications of Ageing for Managing Patients. Drugs Aging 2022, 39, 841–849. [Google Scholar] [CrossRef]
- Adas, M.A.; Alveyn, E.; Cook, E.; Dey, M.; Galloway, J.B.; Bechman, K. The infection risks of JAK inhibition. Expert. Rev. Clin. Immunol. 2022, 18, 253–261. [Google Scholar] [CrossRef]
- Kragstrup, T.W.; Glintborg, B.; Svensson, A.L.; McMaster, C.; Robinson, P.C.; Deleuran, B.; Liew, D.F. Waiting for JAK inhibitor safety data. RMD Open 2022, 8, e002236. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bergstra, S.A.; Kerschbaumer, A.; Sepriano, A.; Aletaha, D.; Caporali, R.; Edwards, C.J.; Hyrich, K.L.; Pope, J.E.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann. Rheum. Dis. 2023, 82, 3–18. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Ebina, K.; Hirano, T.; Maeda, Y.; Yamamoto, W.; Hashimoto, M.; Murata, K.; Onishi, A.; Jinno, S.; Hara, R.; Son, Y.; et al. Factors affecting drug retention of Janus kinase inhibitors in patients with rheumatoid arthritis: The ANSWER cohort study. Sci. Rep. 2022, 12, 134. [Google Scholar] [CrossRef] [PubMed]
- Radner, H.; Yoshida, K.; Tedeschi, S.; Studenic, P.; Frits, M.; Iannaccone, C.; Shadick, N.A.; Weinblatt, M.; Aletaha, D.; Smolen, J.S.; et al. Different Rating of Global Rheumatoid Arthritis Disease Activity in Rheumatoid Arthritis Patients with Multiple Morbidities. Arthritis Rheumatol. 2017, 69, 720–727. [Google Scholar] [CrossRef]
- Sugihara, T. Treatment strategies for elderly-onset rheumatoid arthritis in the new era. Mod. Rheumatol. 2022, 32, 493–499. [Google Scholar] [CrossRef]
- Fleischmann, R.; Alam, J.; Arora, V.; Bradley, J.; Schlichting, D.E.; Muram, D.; Smolen, J.S. Safety and efficacy of baricitinib in elderly patients with rheumatoid arthritis. RMD Open 2017, 3, e000546. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Xie, F.; Yang, S.; Bernatsky, S.; Chen, L.; Yun, H.; Winthrop, K. Risk for Herpes Zoster in Tofacitinib-Treated Rheumatoid Arthritis Patients With and Without Concomitant Methotrexate and Glucocorticoids. Arthritis Care Res. 2019, 71, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Sokolove, J.; Schiff, M.; Fleischmann, R.; Weinblatt, M.E.; Connolly, S.E.; Johnsen, A.; Zhu, J.; Maldonado, M.A.; Patel, S.; Robinson, W.H. Impact of baseline anti-cyclic citrullinated peptide-2 antibody concentration on efficacy outcomes following treatment with subcutaneous abatacept or adalimumab: 2-year results from the AMPLE trial. Ann. Rheum. Dis. 2016, 75, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Drosos, A. Methotrexate intolerance in elderly patients with rheumatoid arthritis: What are the alternatives? Drugs Aging 2003, 20, 723–736. [Google Scholar] [CrossRef]
- Fleischmann, R.; Kremer, J.; Cush, J.; Schulze-Koops, H.; Connell, C.A.; Bradley, J.D.; Gruben, D.; Wallenstein, G.V.; Zwillich, S.H.; Kanik, K.S. Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 495–507. [Google Scholar] [CrossRef]
- Fleischmann, R.; Mysler, E.; Hall, S.; Kivitz, A.J.; Moots, R.J.; Luo, Z.; DeMasi, R.; Soma, K.; Zhang, R.; Takiya, L.; et al. Efficacy and safety of tofacitinib monotherapy, tofacitinib with methotrexate, and adalimumab with methotrexate in patients with rheumatoid arthritis (ORAL Strategy): A phase 3b/4, double-blind, head-to-head, randomised controlled trial. Lancet 2017, 390, 457–468. [Google Scholar] [CrossRef]
- Smolen, J.S.; Pangan, A.L.; Emery, P.; Rigby, W.; Tanaka, Y.; Vargas, J.I.; Zhang, Y.; Damjanov, N.; Friedman, A.; Othman, A.A.; et al. Upadacitinib as monotherapy in patients with active rheumatoid arthritis and inadequate response to methotrexate (SELECT-MONOTHERAPY): A randomised, placebo-controlled, double-blind phase 3 study. Lancet 2019, 393, 2303–2311. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Genovese, M.C.; Haraoui, B.; Li, Z.; Xie, L.; Klar, R.; Pinto-Correia, A.; Otawa, S.; Lopez-Romero, P.; de la Torre, I.; et al. Dose reduction of baricitinib in patients with rheumatoid arthritis achieving sustained disease control: Results of a prospective study. Ann. Rheum. Dis. 2019, 78, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Kawahito, Y.; Morinobu, A.; Kaneko, Y.; Kohno, M.; Hirata, S.; Kishimoto, M.; Seto, Y.; Sugihara, T.; Tanaka, E.; Ito, H.; et al. Drug Treatment Algorithm and Recommendations from the 2020 update of the Japan College of Rheumatology Clinical Practice Guidelines for the Management of Rheumatoid Arthritis-Secondary Publication. Mod. Rheumatol. 2022, 33, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Ytterberg, S.R.; Bhatt, D.L.; Mikuls, T.R.; Koch, G.G.; Fleischmann, R.; Rivas, J.L.; Germino, R.; Menon, S.; Sun, Y.; Wang, C.; et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N. Engl. J. Med. 2022, 386, 316–326. [Google Scholar] [CrossRef]
- Alves, C.; Penedones, A.; Mendes, D.; Marques, F.B. Risk of Cardiovascular and Venous Thromboembolic Events Associated With Janus Kinase Inhibitors in Rheumatoid Arthritis: A Systematic Review and Network Meta-analysis. J. Clin. Rheumatol. 2022, 28, 69–76. [Google Scholar] [CrossRef]
- Xie, W.; Huang, Y.; Xiao, S.; Sun, X.; Fan, Y.; Zhang, Z. Impact of Janus kinase inhibitors on risk of cardiovascular events in patients with rheumatoid arthritis: Systematic review and meta-analysis of randomised controlled trials. Ann. Rheum. Dis. 2019, 78, 1048–1054. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 133 |
|---|---|
| Age (years) | 77.0 ± 7.7 |
| Female, n (%) | 76 (57.1) |
| JAKis use, n | TOF 30, BAR 74, UPA 24, PEF 4, FIL 1 |
| Disease duration (years) | 8.4 ± 10.9 |
| RF-positive, n (%) | 83/127 (65.4) |
| ACPA-positive, n (%) | 81/127 (63.8) |
| CRP (mg/dL) | 3.12 ± 22.2 |
| MMP-3 (ng/mL) | 338.3 ± 493.7 |
| DAS28-CRP | 3.76 ± 1.12 |
| DAS28-ESR | 4.67 ± 1.31 |
| CDAI | 20.7 ± 13.3 |
| eGFR (mL/min) | 71.9 ± 22.1 |
| CKD (eGFR < 60), n (%) | 35 (27.7) |
| Alb (g/dL) | 3.59 ± 0.60 |
| Hypoalbuminemia (Alb < 3.0), n (%) | 25/124 (20.2) |
| Diabetes, n (%) | 25 (18.8) |
| Chronic lung disease, n (%) | 30 (22.6) |
| Interstitial lung disease, n (%) | 18 (13.5) |
| Bronchiolitis, n (%) | 4 (3.0) |
| Bronchiectasis, n (%) | 6 (4.5) |
| Pulmonary emphysema, n (%) | 2 (1.5) |
| MTX use, n (%) | 49 (36.8) |
| MTX dose (mg/week) | 6.5 ± 2.2 |
| GC use, n (%) | 29 (21.8) |
| GC dose (mg/day) | 3.4 ± 22.3 |
| Prior bDMARDs use, n (%) | 49 (36.8) |
| TNFi use, n (%) | 34 (25.7) |
| Anti-IL-6R, n (%) | 27 (20.3) |
| CTLA4-Ig, n (%) | 11 (8.3) |
| Follow up periods (month) | 27.4 ± 15.8 |
| Total | n = 29 |
|---|---|
| Infection | 12 (Pneumonia 8, Pyothorax 1, Upper respiratory infection 1, Herpes Zoster 1, Cholecystitis 1) |
| Malignancy | 9 (Lymphoma 3, Lung 2, Colon 3, Melanoma 1) |
| Hematological disorder | 4 (Anemia 2, Thrombocytopenia 1, Lymphopenia 1) |
| Exacerbation of interstitial pneumonia | 2 |
| Cardiovascular disease | 1 (Cerebral hemorrhage) |
| Renal impairment | 1 |
| AEs n = 29 | Others n = 104 | Univariable Analysis HR (95% CI) p-Value | Multivariate Analysis HR (95% CI) p-Value | |
|---|---|---|---|---|
| Age (years) | 80.0 ± 9.1 | 76.7 ± 7.1 | 1.056 (1.005–1.109) 0.031 * | 1.035 (0.976–1.098) 0.249 |
| Very elderly (age ≥ 75) (%) | 19 (65.5) | 56 (53.8) | 1.412 (0.656–3.038) 0.377 | |
| Female, n (%) | 18 (62.1) | 76 (73.1) | 0.590 (0.277–1.253) 0.169 | |
| RF-positive, n (%) | 15/26 (57.7) | 68/101 (67.3) | 0.893 (0.408–1.957) 0.778 | |
| ACPA-positive, n (%) | 14/26 (53.8) | 67/101 (66.3) | 0.743 (0.343–1.611) 0.452 | |
| CKD (eGFR < 60) (%) | 7 (24.1) | 28 (26.9) | 1.074 (0.455–2.537) 0.870 | |
| CRP (mg/dL) | 3.1 ± 3.5 | 3.3 ± 4.2 | 1.006 (0.908–1.114) 0.915 | |
| Hypoalbuminemia (%) | 11 (37.9) | 14 (13.5) | 3.158 (1.478–6.750) 0.003 * | 2.709 (1.201–6.112) 0.016 * |
| Diabetes, n (%) | 6 (20.7) | 23 (22.1) | 0.951 (0.387–2.339) 0.913 | |
| Chronic lung disease (%) | 11 (37.9) | 19 (18.3) | 2.544 (1.198–5.401) 0.015 * | 2.517 (1.150–5.507) 0.021 * |
| Reduced dose (%) | 12 (41.4) | 43 (41.3) | 0.759 (0.359–1.602) 0.469 | |
| MTX use, n (%) | 7 (24.1) | 42 (40.4) | 0.407 (0.171–0.967) 0.042 * | 0.536 (0.188–1.527) 0.243 |
| GC (≥5 mg/day) use (%) | 5 (17.2) | 13 (12.5) | 2.073 (0.784–5.481) 0.142 | |
| Prior bDMARDs use, n (%) | 12 (41.4) | 37 (35.6) | 1.162 (0.554–2.435) 0.691 |
| Approved Dose (n = 78) | Reduced Dose (n = 55) | p-Value | |
|---|---|---|---|
| Age (years) | 76.1 ± 7.9 | 79.3 ± 6.9 | 0.014 * |
| Female, n (%) | 53 (67.9) | 41 (74.5) | 0.411 |
| Disease duration (years) | 7.8 ± 10.5 | 9.3 ± 11.4 | 0.337 |
| RF-positive, n (%) | 48/74 (64.9) | 35/53 (66.0) | 0.891 |
| ACPA-positive, n (%) | 46/74 (62.2) | 35/53 (66.0) | 0.654 |
| CRP (mg/dL) | 3.2 ± 3.8 | 3.0 ± 3.4 | 0.712 |
| DAS28-CRP | 3.8 ± 1.0 | 3.7 ± 1.3 | 0.414 |
| CDAI | 22.2 ± 13.3 | 18.3 ± 13.3 | 0.155 |
| eGFR (mL/min) | 68.9 ± 21.9 | 76.2 ± 21.9 | 0.061 |
| Hypoalbuminemia (Alb < 3.0), n (%) | 12 (15.4) | 13 (23.6) | 0.295 |
| Diabetes, n (%) | 17 (21.8) | 12 (21.8) | 0.997 |
| Chronic lung disease, n (%) | 20 (25.6) | 10 (18.2) | 0.311 |
| MTX use, n (%) | 33 (42.3) | 16 (29.1) | 0.120 |
| GC use, n (%) | 17 (21.8) | 12 (21.8) | 0.997 |
| Follow up periods (month) | 26.1±16.0 | 29.3 ± 15.6 | 0.240 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Temmoku, J.; Miyata, M.; Suzuki, E.; Sumichika, Y.; Saito, K.; Yoshida, S.; Matsumoto, H.; Fujita, Y.; Matsuoka, N.; Asano, T.; et al. Drug Retention Rates and the Safety of Janus Kinase Inhibitors in Elderly Patients with Rheumatoid Arthritis. J. Clin. Med. 2023, 12, 4585. https://doi.org/10.3390/jcm12144585
Temmoku J, Miyata M, Suzuki E, Sumichika Y, Saito K, Yoshida S, Matsumoto H, Fujita Y, Matsuoka N, Asano T, et al. Drug Retention Rates and the Safety of Janus Kinase Inhibitors in Elderly Patients with Rheumatoid Arthritis. Journal of Clinical Medicine. 2023; 12(14):4585. https://doi.org/10.3390/jcm12144585
Chicago/Turabian StyleTemmoku, Jumpei, Masayuki Miyata, Eiji Suzuki, Yuya Sumichika, Kenji Saito, Shuhei Yoshida, Haruki Matsumoto, Yuya Fujita, Naoki Matsuoka, Tomoyuki Asano, and et al. 2023. "Drug Retention Rates and the Safety of Janus Kinase Inhibitors in Elderly Patients with Rheumatoid Arthritis" Journal of Clinical Medicine 12, no. 14: 4585. https://doi.org/10.3390/jcm12144585
APA StyleTemmoku, J., Miyata, M., Suzuki, E., Sumichika, Y., Saito, K., Yoshida, S., Matsumoto, H., Fujita, Y., Matsuoka, N., Asano, T., Sato, S., & Migita, K. (2023). Drug Retention Rates and the Safety of Janus Kinase Inhibitors in Elderly Patients with Rheumatoid Arthritis. Journal of Clinical Medicine, 12(14), 4585. https://doi.org/10.3390/jcm12144585