

Anti-Inflammatory Drug Therapy in Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis of Prospective Randomized and Placebo-Controlled Trials



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy for Identification of Studies
2.2. Types of Studies
2.3. Data Extraction and Quality Evaluation
2.4. Statistics
3. Results
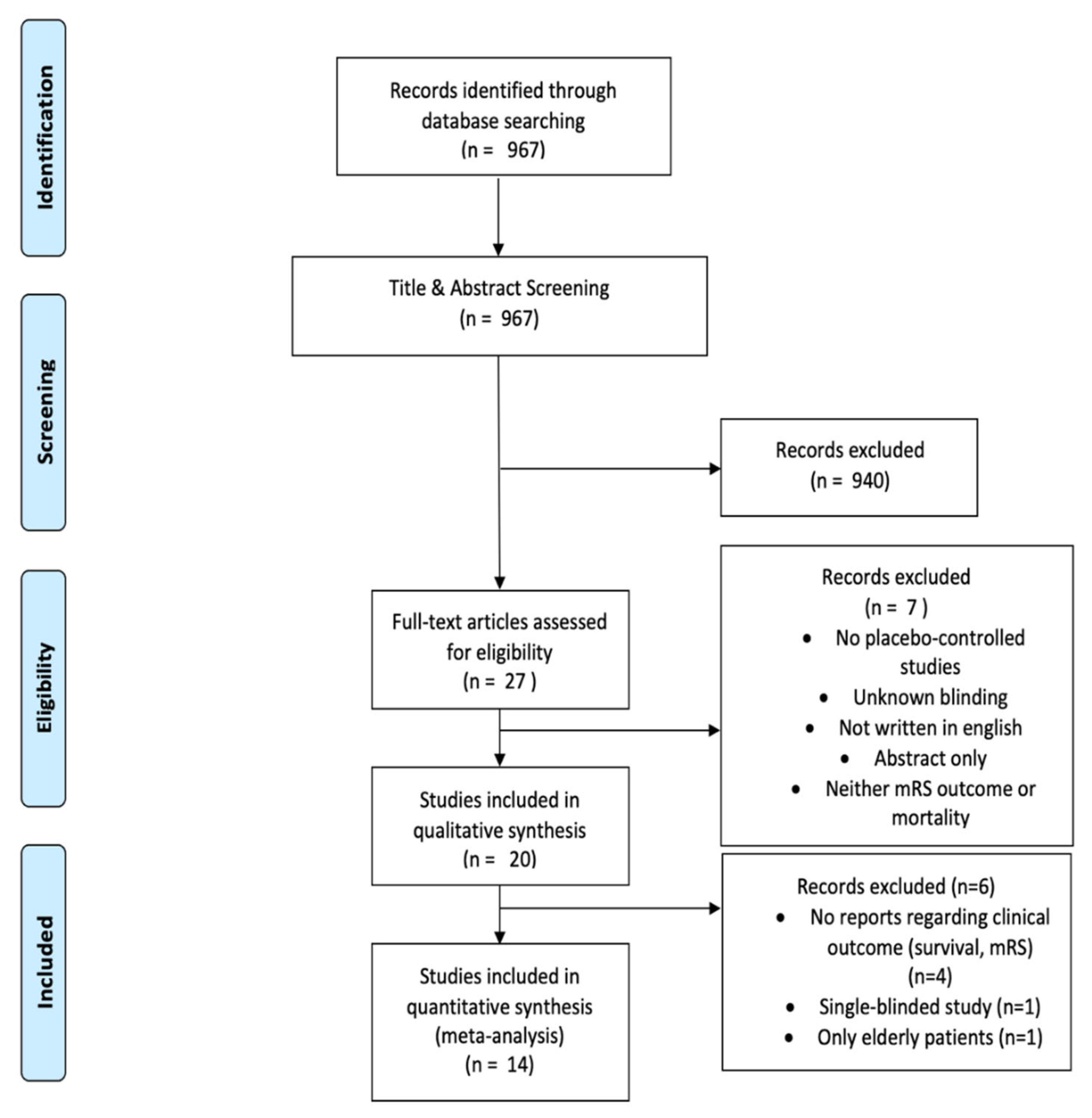
3.1. Literature Search
3.2. Characteristics of Included Studies
3.3. Risk of Bias and Quality Assessment
3.4. Impact of Anti-Inflammatory Therapy in Aneurysmal SAH on Survival
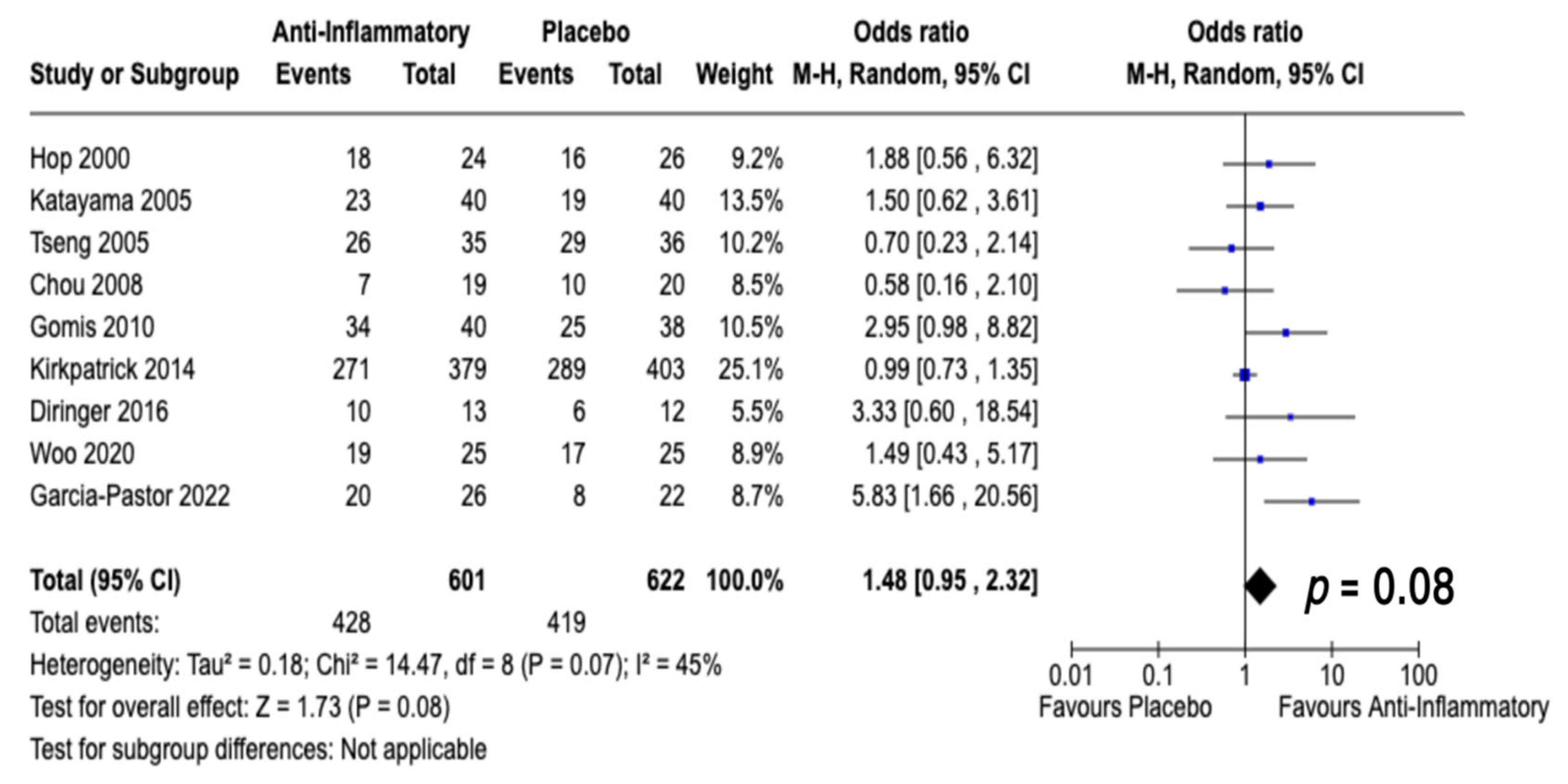
3.5. Impact of Anti-Inflammatory Therapy in Aneurysmal SAH on Neurological Outcome
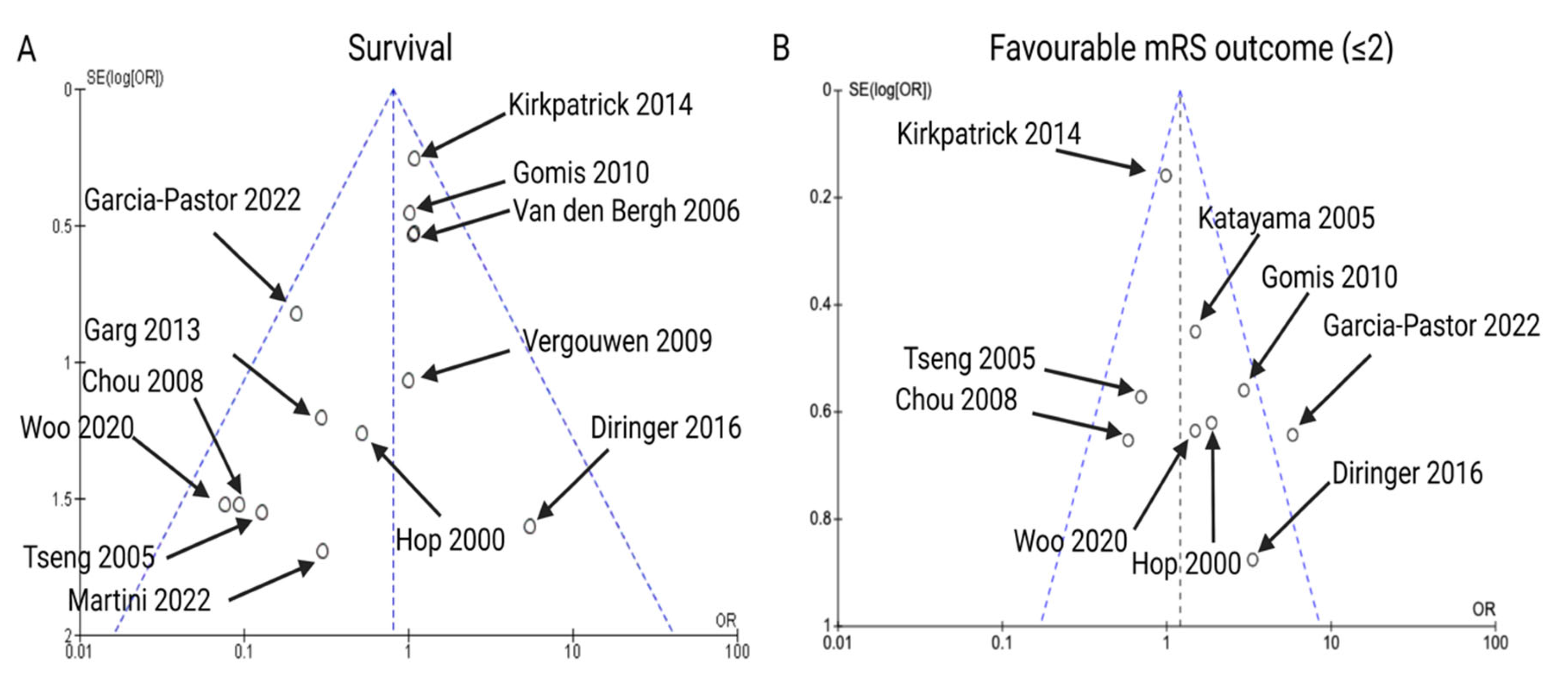
3.6. Publication Bias
4. Discussion
4.1. COX Inhibition
4.2. Thromboxane A2 Synthetase Inhibition
4.3. Epoxide Hydrolase Inhibition
4.4. Statins
4.5. Cerebrolysin
4.6. Dapsone
4.7. Corticosteroids
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neifert, S.N.; Chapman, E.K.; Martini, M.L.; Shuman, W.H.; Schupper, A.J.; Oermann, E.K.; Mocco, J.; Macdonald, R.L. Aneurysmal Subarachnoid Hemorrhage: The Last Decade. Transl. Stroke Res. 2020, 12, 428–446. [Google Scholar] [CrossRef]
- Etminan, N.; Chang, H.S.; Hackenberg, K.; de Rooij, N.K.; Vergouwen, M.D.I.; Rinkel, G.J.E.; Algra, A. Worldwide Incidence of Aneurysmal Subarachnoid Hemorrhage According to Region, Time Period, Blood Pressure, and Smoking Prevalence in the Population: A Systematic Review and Meta-analysis. JAMA Neurol. 2019, 76, 588–597. [Google Scholar] [CrossRef]
- Connolly, E.S., Jr.; Rabinstein, A.A.; Carhuapoma, J.R.; Derdeyn, C.P.; Dion, J.; Higashida, R.T.; Hoh, B.L.; Kirkness, C.J.; Naidech, A.M.; Ogilvy, C.S.; et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke 2012, 43, 1711–1737. [Google Scholar] [CrossRef]
- Hoh, B.L.; Ko, N.U.; Amin-Hanjani, S.; Chou, S.H.-Y.; Cruz-Flores, S.; Dangayach, N.S.; Derdeyn, C.P.; Du, R.; Hänggi, D.; Hetts, S.W.; et al. 2023 Guideline for the Management of Patients with Aneurysmal Subarachnoid Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke 2023. [Google Scholar] [CrossRef]
- Tjahjadi, M.; Heinen, C.; König, R.; Rickels, E.; Wirtz, C.R.; Woischneck, D.; Kapapa, T. Health-Related Quality of Life after Spontaneous Subarachnoid Hemorrhage Measured in a Recent Patient Population. World Neurosurg. 2013, 79, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Taufique, Z.; May, T.; Meyers, E.; Falo, C.; Mayer, S.A.; Agarwal, S.; Park, S.; Connolly, E.S.; Claassen, J.; Schmidt, J.M. Predictors of Poor Quality of Life 1 Year after Subarachnoid Hemorrhage. Neurosurgery 2016, 78, 256–264. [Google Scholar] [CrossRef]
- Al-Khindi, T.; Macdonald, R.L.; Schweizer, T.A. Cognitive and Functional Outcome after Aneurysmal Subarachnoid Hemorrhage. Stroke 2010, 41, e519–e536. [Google Scholar] [CrossRef] [PubMed]
- Eagles, M.E.; Tso, M.K.; Macdonald, R.L. Cognitive impairment, functional outcome, and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. World Neurosurg. 2019, 124, e558–e562. [Google Scholar] [CrossRef]
- Roos, Y.B.; de Haan, R.J.; Beenen, L.F.; Groen, R.J.; Albrecht, K.W.; Vermeulen, M. Complications and outcome in patients with aneurysmal subarachnoid haemorrhage: A prospective hospital based cohort study in the Netherlands. J. Neurol. Neurosurg. Psychiatry 2000, 68, 337–341. [Google Scholar] [CrossRef]
- Platz, J.; Güresir, E.; Vatter, H.; Berkefeld, J.; Seifert, V.; Raabe, A.; Beck, J. Unsecured intracranial aneurysms and induced hypertension safe? Neurocrit. Care 2011, 14, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Caffes, N.; Kurland, D.B.; Gerzanich, V.; Simard, J.M. Glibenclamide for the treatment of ischemic and hemorrhagic stroke. Int. J. Mol. Sci. 2015, 16, 4973–4984. [Google Scholar] [CrossRef]
- Makino, H.; Tada, Y.; Wada, K.; Liang, E.I.; Chang, M.; Mobashery, S.; Kanematsu, Y.; Kurihara, C.; Palova, E.; Kanematsu, M.; et al. Pharmacological stabilization of intracranial aneurysms in mice: A feasibility study. Stroke 2012, 43, 2450–2456. [Google Scholar] [CrossRef]
- Güresir, E.; Gräff, I.; Seidel, M.; Bauer, H.; Coch, C.; Diepenseifen, C.; Dohmen, C.; Engels, S.; Hadjiathanasiou, A.; Heister, U.; et al. Aneurysmal Subarachnoid Hemorrhage during the Shutdown for COVID-19. J. Clin. Med. 2022, 11, 2555. [Google Scholar] [CrossRef]
- Moraes, L.; Grille, S.; Morelli, P.; Mila, R.; Trias, N.; Brugnini, A.; Lluberas, N.; Biestro, A.; Lens, D. Immune cells subpopulations in cerebrospinal fluid and peripheral blood of patients with Aneurysmal Subarachnoid Hemorrhage. Springerplus 2015, 4, 195. [Google Scholar] [CrossRef]
- Kooijman, E.; Nijboer, C.H.; van Velthoven, C.T.; Kavelaars, A.; Kesecioglu, J.; Heijnen, C.J. The rodent endovascular puncture model of subarachnoid hemorrhage: Mechanisms of brain damage and therapeutic strategies. J. Neuroinflamm. 2014, 11, 2. [Google Scholar] [CrossRef]
- Provencio, J.J.; Badjatia, N. Participants in the International Multi-disciplinary Consensus Conference on Multimodality Monitoring. Monitoring inflammation (including fever) in acute brain injury. Neurocrit. Care 2014, 21 (Suppl. 2), S177–S186. [Google Scholar] [CrossRef]
- Xu, H.-L.; Garcia, M.; Testai, F.; Vetri, F.; Barabanova, A.; Pelligrino, D.A.; Paisansathan, C. Pharmacologic blockade of vascular adhesion protein-1 lessens neurologic dysfunction in rats subjected to subarachnoid hemorrhage. Brain Res. 2014, 1586, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0.; Cochrane Collab: London, UK, 2011; Available online: www.cochrane-handbook.org (accessed on 1 September 2022).
- Liberati, M.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Lampmann, T.; Hadjiathanasiou, A.; Asoglu, H.; Wach, J.; Kern, T.; Vatter, H.; Güresir, E. Early Serum Creatinine Levels after Aneurysmal Subarachnoid Hemorrhage Predict Functional Neurological Outcome after 6 Months. J. Clin. Med. 2022, 11, 4753. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G.; Cates, C.J.; Schwarzer, G. Methods for including information from multi-arm trials in pairwise meta-analysis. Res. Synth. Methods 2017, 8, 392–403. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Smith, E.E.; Badjatia, N.; Nogueira, R.G.; Sims, J.R., 2nd; Ogilvy, C.S.; Rordorf, G.A.; Ayata, C. A randomized, double-blind, placebo-controlled pilot study of simvastatin in aneurysmal subarachnoid hemorrhage. Stroke 2008, 39, 2891–2893. [Google Scholar] [CrossRef]
- Diringer, M.N.; Dhar, R.; Scalfani, M.; Zazulia, A.R.; Chicoine, M.; Powers, W.J.; Derdeyn, C.P. Effect of High-Dose Simvastatin on Cerebral Blood Flow and Static Autoregulation in Subarachnoid Hemorrhage. Neurocrit. Care 2015, 25, 56–63. [Google Scholar] [CrossRef]
- García-Pastor, C.; de Llano, J.P.N.-G.; Balcázar-Padrón, J.C.; Tristán-López, L.; Rios, C.; Díaz-Ruíz, A.; Rodríguez-Hernandez, L.A.; Nathal, E. Neuroprotective effect of dapsone in patients with aneurysmal subarachnoid hemorrhage: A prospective, randomized, double-blind, placebo-controlled clinical trial. Neurosurg. Focus 2022, 52, E12. [Google Scholar] [CrossRef]
- Garg, K.; Sinha, S.; Kale, S.S.; Chandra, P.S.; Suri, A.; Singh, M.M.; Kumar, R.; Sharma, M.S.; Pandey, R.M.; Sharma, B.S.; et al. Role of simvastatin in prevention of vasospasm and improving functional outcome after aneurysmal subarachnoid hemorrhage: A prospective, randomized, double-blind, placebo-controlled pilot trial. Br. J. Neurosurg. 2013, 27, 181–186. [Google Scholar] [CrossRef]
- Gomis, P.; Graftieaux, J.P.; Sercombe, R.; Hettler, D.; Scherpereel, B.; Rousseaux, P. Randomized, double-blind, placebo-controlled, pilot trial of high-dose methylprednisolone in aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2010, 112, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Hop, J.W.; Rinkel, G.J.E.; Algra, A.; van der Sprenkel, J.B.; van Gijn, J. Randomized pilot trial of postoperative aspirin in subarachnoid hemorrhage. Neurology 2000, 54, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Katayama, Y.; Haraoka, J.; Hirabayashi, H.; Kawamata, T.; Kawamoto, K.; Kitahara, T.; Kojima, J.; Kuroiwa, T.; Mori, T.; Moro, N.; et al. A randomized controlled trial of hydrocortisone againast hyponatremia in patients with aneurysmal subarachnoid hemorrhage. Stroke 2007, 38, 2373–2375. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, P.J.; Turner, C.L.; Smith, C.; Hutchinson, P.J.; Murray, G.D.; STASH Collaborators. Simvastatin in aneurysmal subarachnoid haemorrhage (STASH): A multicentre randomised phase 3 trial. Lancet Neurol. 2014, 13, 666–675. [Google Scholar] [CrossRef]
- Martini, R.P.; Siler, D.; Cetas, J.; Alkayed, N.J.; Allen, E.; Treggiari, M.M. A Double-Blind, Randomized, Placebo-Controlled Trial of Soluble Epoxide Hydrolase Inhibition in Patients with Aneurysmal Subarachnoid Hemorrhage. Neurocrit. Care 2022, 36, 905–915. [Google Scholar] [CrossRef]
- Suzuki, S.; Sano, K.; Handa, H.; Asano, T.; Tamura, A.; Yonekawa, Y.; Ono, H.; Tachibana, N.; Hanaoka, K. Clinical study of OKY-046, a thromboxane synthetase inhibitor, in prevention of cerebral vasospasms and delayed cerebral ischemic symptomes after subarachnoid haemorrhage due to aneurysmal rupture: A randomized double-blind study. Neurol. Res. 1989, 11, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.Y.; Czosnyka, M.; Richards, H.; Pickard, J.D.; Kirkpatrick, P.J. Faculty Opinions recommendation of Effects of acute treatment with pravastatin on cerebral vasospasm, autoregulation, and delayed ischemic deficits after aneurysmal subarachnoid hemorrhage: A phase II randomized placebo-controlled trial. Stroke 2015, 36, 1627–1632. [Google Scholar] [CrossRef]
- Van den Bergh, W.M.; lgra, A.; Dorhout Mees, S.M.; van Kooten, F.; Dirven, C.M.; van Gijn, J.; Vermeulen, M.; Rinkel, G.J.; MASH Study Group. Randomized controlled trial of acetylsalicylic acid in aneurysmal subarachnoid hemorrhage: The MASH study. Stroke 2006, 37, 2326–2330. [Google Scholar] [CrossRef]
- Vergouwen, M.D.I.; Meijers, J.C.M.; Geskus, R.B.; Coert, B.A.; Horn, J.; Stroes, E.S.G.; Van Der Poll, T.; Vermeulen, M.; Roos, Y.B.W.E.M. Biologic Effects of Simvastatin in Patients with Aneurysmal Subarachnoid Hemorrhage: A Double-Blind, Placebo-Controlled Randomized Trial. J. Cereb. Blood Flow Metab. 2009, 29, 1444–1453. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.Y.M.; Ho, J.W.K.; Ko, N.M.W.; Li, R.P.T.; Jian, L.; Chu, A.C.H.; Kwan, M.C.L.; Chan, Y.; Wong, A.K.S.; Wong, H.-T.; et al. Randomized, placebo-controlled, double-blind, pilot trial to investigate safety and efficacy of Cerebrolysin in patients with aneurysmal subarachnoid hemorrhage. BMC Neurol. 2020, 20, 401. [Google Scholar] [CrossRef]
- Chen, J.; Li, M.; Zhu, X.; Chen, L.; Yang, S.; Zhang, C.; Wu, T.; Feng, X.; Wang, Y.; Chen, Q. Atorvastatin reduces cerebral vasospasm and infarction after aneurysmal subarachnoid hemorrhage in elderly Chinese adults. Aging 2020, 12, 2939–2951. [Google Scholar] [CrossRef]
- Fei, L.; Golwa, F. Topical application of dexamethasone to prevent cerebral vasospasm after aneurysmal subarachnoid haemorrhage: A pilot study. Clin. Drug Investig. 2007, 27, 827–832. [Google Scholar] [CrossRef]
- Galea, J.; Ogungbenro, K.; Hulme, S.; Patel, H.; Scarth, S.; Hoadley, M.; Illingworth, K.; McMahon, C.J.; Tzerakis, N.; King, A.; et al. Reduction of inflammation after administration of interleukin-1 receptor antagonist following aneurysmal subarachnoid hemorrhage: Results of the Subcutaneous Interleukin-1Ra in SAH (SCIL-SAH) study. J. Neurosurg. 2018, 128, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Hasan, D.; Lindsay, K.W.; Wijdicks, E.F.; Murray, G.D.; Brouwers, P.J.; Bakker, W.H.; van Gijn, J.; Vermeulen, M. Effect of fludrocortisone acetate in patients with subarachnoid hemorrhage. Stroke 1989, 20, 1156–1161. [Google Scholar] [CrossRef]
- Hashi, K.; Takakura, K.; Sano, K.; Ohta, T.; Saito, I.; Okada, K. Intravenous hydrocortisone in large doses in the treatment of delayed ischemic neurological deficits following subarachnoid hemorrhage—Results of a multi-center controlled double-blind clinical study. No Shinkei= Brain Nerve 1988, 40, 373–382. [Google Scholar]
- Jaschinski, U.; Scherer, K.; Lichtwarck, M.; Forst, H. Impact of treatment with pravastatin on delayed ischemic disease and mortality after aneurysmal subarachnoid hemorrhage. Crit. Care 2008, 12, P112. [Google Scholar] [CrossRef]
- Lynch, J.R.; Wang, H.; McGirt, M.J.; Floyd, J.; Friedman, A.H.; Coon, A.L.; Blessing, R.; Alexander, M.J.; Graffagnino, C.; Warner, D.S.; et al. Simvastatin reduces vasospasm after aneurysmal subarachnoid hemorrhage: Results of a pilot randomized clinical trial. Stroke 2005, 36, 2024–2026. [Google Scholar] [CrossRef]
- Macedo, S.; Bello, Y.; Silva, A.; Siqueira, C.; Siqueira, S.; Brito, L. Effects of simvastatin in prevention of vasospasm in nontraumatic subarachnoid hemorrhage: Preliminary data. Crit. Care 2009, 13, P103. [Google Scholar] [CrossRef]
- Mori, T.; Katayama, Y.; Kawamata, T.; Hirayama, T.; Khan, M.I.; Dellinger, R.P.; Waguespack, S.G.; Shah, K.; Turgeon, R.D.; Gooderham, P.A.; et al. Improved efficiency of hypervolemic therapy with inhibition of natriuresis by fludrocortisone in patients with aneurysmal subarachnoid hemorrhage. J. Neurosurg. 1999, 91, 947–952. [Google Scholar] [CrossRef]
- Moro, N.; Katayama, Y.; Kojima, J.; Mori, T.; Kawamata, T. Prophylactic management of excessive natriuresis with hydrocortisone for efficient hypervolemic theerapy after subarachnoid hemorrhage. Stroke 2003, 34, 2807–2811. [Google Scholar] [CrossRef]
- Naraoka, M.; Matsuda, N.; Shimamura, N.; Asano, K.; Akasaka, K.; Takemura, A.; Hasegawa, S.; Ohkuma, H. Long-acting statin for aneurysmal subarachnoid hemorrhage: A randomized, double-blind, placebo-controlled trial. J. Cereb. Blood Flow Metab. 2017, 38, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Hopkins, S.J.; Hulme, S.; Galea, J.P.; Hoadley, M.; Vail, A.; Hutchinson, P.J.; Grainger, S.; Rothwell, N.J.; King, A.T.; et al. The effect of intravenous interleukin-1 receptor antagonist on inflammatory mediators in cerebrospinal fluid after subrachnoid haemorrhage: A phase II randomised controlled trial. J. Neuroinflamm. 2014, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.K.; Chan, D.Y.; Siu, D.Y.; Zee, B.C.; Poon, W.S.; Chan, M.T.; Gin, T.; Leung, M.; HDS-SAH Investigators. High-dose simvastatin for aneurysmal subarachnoid hemorrhage: Multicenter randomized controlled double-blinded clinical trial. Stroke 2015, 46, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Pickard, J.D.; Murray, G.D.; Illingworth, R.; Shaw, M.D.; Teasdale, G.M.; Foy, P.M.; Humphrey, P.R.; Lang, D.A.; Nelson, R.; Richards, P. Effect of oral nimodipine on cerebral infarction and outcome after subarachnoid haemorrhage: British aneurysm nimodipine trial. BMJ 1989, 298, 636–642. [Google Scholar] [CrossRef]
- Rouzer, C.A.; Marnett, L.J. Structural and Chemical Biology of the Interaction of Cyclooxygenase with Substrates and Non-Steroidal Anti-Inflammory Drugs. Chem. Rev. 2020, 120, 7592–7641. [Google Scholar] [CrossRef]
- Wu, F.; Liu, Z.; Li, G.; Zhou, L.; Huang, K.; Wu, Z.; Zhan, R.; Shen, J. Inflammation and Oxidative Stress: Potential Targets for Improving Prognosis After Subarachnoid Hemorrhage. Front. Cell. Neurosci. 2021, 15, 739506. [Google Scholar] [CrossRef]
- Dinh, Y.R.T.; Jomaa, A.; Callebert, J.; Reynier-Rebuffel, A.-M.; Tedgui, A.; Savarit, A.; Sercombe, R. Overexpression of Cyclooxygenase-2 in Rabbit Basilar Artery Endothelial Cells after Subarachnoid Hemorrhage. Neurosurgery 2001, 48, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Ayer, R.; Jadhav, V.; Sugawara, T.; Zhang, J.H. The Neuroprotective Effects of Cyclooxygenase-2 Inhibition in a Mouse Model of Aneurysmal Subarachnoid Hemorrhage. Acta Neurochir. Suppl. 2011, 111, 145–149. [Google Scholar] [CrossRef]
- Roumie, C.L.; Mitchel, E.F., Jr.; Kaltenbach, L.; Arbogast, P.G.; Gideon, P.; Griffin, M.R. Nonaspirin NSAIDs, cyclooxygenase 2 inhibitors, and the risk for stroke. Stroke 2008, 39, 2037–2045. [Google Scholar] [CrossRef]
- Parkhutik, V.; Lago, A.; Tembl, J.I.; Rubio, C.; Fuset, M.P.; Vallés, J.; Santos, M.T.; Moscardo, A. Influence of COX-inhibiting Analgesics on the Platelet Function of Patients with Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2012, 21, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Lee, S.H.; Chu, K.; Roh, J.K. Effects of celecoxib on volumes of hematoma and edema in patients with primary intracerebral hemorrhhage. J. Neurol. Sci. 2009, 279, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, B.; Aldington, S.; Weatherall, M.; Shirtcliffe, P.; Beasley, R. Risk of Cardiovascular Events and Celecoxib: A Systematic Review and Meta-Analysis. J. R. Soc. Med. 2006, 99, 132–140. [Google Scholar] [CrossRef]
- Coyle, A.T.; Miggin, S.M.; Kinsella, B.T. Characterization of the 5′ untranslated region of alpha and beta isoforms of the human thromboxane A2 receptor (TP). Differential promoter utilization by the TP isoforms. Eur. J. Biochem. 2002, 269, 4058–4073. [Google Scholar] [CrossRef]
- Davì, G.; Patrono, C. Platelet Activation and Atherothrombosis. N. Engl. J. Med. 2007, 357, 2482–2494. [Google Scholar] [CrossRef]
- Ansar, S.; Larsen, C.; Maddahi, A.; Edvinsson, L. Subarachnoid hemorrhage induces enhanced expression of thromboxane A2 receptors in rat cerebral arteries. Brain Res. 2010, 1316, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Tohgi, H.; Konno, S.; Tamura, K.; Kimura, B.; Kawano, K. Effects of low-to-high doses of aspirin on platelet aggregability and metabolites of thromboxane A2 and prostacyclin. Stroke 1992, 23, 1400–1403. [Google Scholar] [CrossRef] [PubMed]
- Vinge, E.; Brandt, L.; Ljunggren, B.; Andersson, K.E. Thromboxane B2 levels in serum during continous administration of nimodipine to patients with aneurysmal subarachnoid hemorrhage. Stroke 1988, 19, 644–647. [Google Scholar] [CrossRef]
- Collins, T.; Read, M.A.; Neish, A.S.; Whitley, M.Z.; Thanos, D.; Maniatis, T. Transcriptional regulation of endothelial cell adhesion molecules: NF-kappa B and cytokine-inducible enhancers. FASEB J. 1995, 9, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Node, K.; Huo, Y.; Ruan, X.; Yang, B.; Spiecker, M.; Ley, K.; Zeldin, D.C.; Liao, J.K. Anti-inflammatory Properties of Cytochrome P450 Epoxygenase-Derived Eicosanoids. Science 1999, 285, 1276–1279. [Google Scholar] [CrossRef]
- Xiao, L.; Liu, Y.; Wang, N. New paradigms in inflammatory signaling in vascular endothelial cells. Am. J. Physiol. Circ. Physiol. 2014, 306, H317–H325. [Google Scholar] [CrossRef]
- Muldoon, L.L.; Alvarez, J.I.; Begley, D.J.; Boado, R.J.; Del Zoppo, G.J.; Doolittle, N.D.; Engelhardt, B.; Hallenbeck, J.M.; Lonser, R.R.; Ohlfest, J.R.; et al. Immunologic Privilege in the Central Nervous System and the Blood–Brain Barrier. J. Cereb. Blood Flow Metab. 2013, 33, 13–21. [Google Scholar] [CrossRef]
- Siler, D.A.; Berlow, Y.A.; Kukino, A.; Davis, C.M.; Nelson, J.W.; Grafe, M.R.; Ono, H.; Cetas, J.S.; Pike, M.; Alkayed, N.J. Soluble Epoxide Hydrolase in Hydrocephalus, Cerebral Edema, and Vascular Inflammation after Subarachnoid Hemorrhage. Stroke 2015, 46, 1916–1922. [Google Scholar] [CrossRef]
- Greenwood, J.; Etienne-Manneville, S.; Adamson, P.; Couraud, P.-O. Lymphocyte migration into the central nervous system: Implication of ICAM-1 signalling at the blood–brain barrier. Vasc. Pharmacol. 2002, 38, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Laufs, U.; La Fata, V.; Plutzky, J.; Liao, J.K. Upregulation of Endothelial Nitric Oxide Synthase by HMG CoA Reductase Inhibitors. Circulation 1998, 97, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Lynch, J.R.; Parra, A.; Sheng, H.; Pearlstein, R.D.; Laskowitz, D.T.; Pelligrino, D.A.; Warner, D.S. Simvastatin Increases Endothelial Nitric Oxide Synthase and Ameliorates Cerebral Vasospasm Resulting From Subarachnoid Hemorrhage. Stroke 2002, 33, 2950–2956. [Google Scholar] [CrossRef]
- Weitz-Schmidt, G. Statins as anti-inflammatory agents. Trends Pharmacol. Sci. 2002, 23, 482–487. [Google Scholar] [CrossRef]
- McGirt, M.J.; Pradilla, G.; Legnani, F.G.; Thai, Q.-A.; Recinos, P.F.; Tamargo, R.J.; Clatterbuck, R.E. Systemic Administration of Simvastatin after the Onset of Experimental Subarachnoid Hemorrhage Attenuates Cerebral Vasospasm. Neurosurgery 2006, 58, 945–951. [Google Scholar] [CrossRef]
- Vergouwen, M.D.; de Haan, R.J.; Vermeulen, M.; Roos, Y.B. Effect of statin treatment on vasospasm, delayed cerebral ischemia, and functional outcome in patients with aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis update. Stroke 2010, 41, e47–e52. [Google Scholar] [CrossRef]
- Liu, T.; Zhong, S.; Zhai, Q.; Zhang, X.; Jing, H.; Li, K.; Liu, S.; Han, S.; Li, L.; Shi, X.; et al. Optimal Course of Statins for Patients With Aneurysmal Subarachnoid Hemorrhage: Is Longer Treatment Better? A Meta-Analysis of Randomized Controlled Trials. Front. Neurosci. 2021, 15, 757505. [Google Scholar] [CrossRef] [PubMed]
- Maher, M.; Schweizer, T.A.; Macdonald, R.L. Treatment of Spontaneous Subarachnoid Hemorrhage: Guidelines and Gaps. Stroke 2020, 51, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Wang, Y.; Kai, G.; Zhao, S.; Huang, T.; Li, Y.; Xu, Y.; Zhang, L.; Pang, T. Cerebrolysin Ameliorates Focal Cerebral Ischemia Injury Through Neuroinflammatory Inhibition via CREB/PGC-1α Pathway. Front. Pharmacol. 2019, 10, 1245. [Google Scholar] [CrossRef]
- Muresanu, D.F.; Heiss, W.D.; Hoemberg, V.; Bajenaru, O.; Popescu, C.D.; Vester, J.C.; Rahlfs, V.W.; Doppler, E.; Meier, D.; Moessler, H.; et al. Cerebrolysin and recovery after stroke (CARS): A randomized, placebo-controlled, double-blind, multicenter trial. Stroke 2016, 47, 151–159. [Google Scholar] [CrossRef]
- Xue, L.X.; Zhang, T.; Zhao, Y.W.; Geng, Z.; Chen, J.J.; Chen, H. Efficacy and safety comparison of DL-3-n.butylphtalide and Cerebrolysin: Effects on neurological and behavioral outcomes in acute ischemic stroke. Exp. Ther. Med. 2016, 11, 2015–2020. [Google Scholar] [CrossRef]
- Lang, W.; Stadler, C.H.; Poljakovic, Z.; Fleet, D. The Lyse Study Group. A Prospective, Randomized, Placebo-Controlled, Double-Blind Trial about Safety and Efficacy of Combined Treatment with Alteplase (rt-PA) and Cerebrolysin in Acute Ischaemic Hemispheric Stroke. Int. J. Stroke 2012, 8, 95–104. [Google Scholar] [CrossRef]
- Chang, W.H.; Park, C.H.; Kim, D.Y.; Shin, Y.I.; Ko, M.H.; Lee, A.; Jang, S.Y.; Kim, Y.H. Cerebrolysin combined with rehabilitation promotes motro recovery in patients with severe motor impairment after stroke. BMC Neurol. 2016, 16, 31. [Google Scholar] [CrossRef]
- Gharagozli, K.; Harandi, A.; Houshmand, S.; Akbari, N.; Muresanu, D.; Vester, J.; Winter, S.; Moessler, H. Efficacy and safety of Cerebrolysin treatment in early recovery after acute ischemic stroke: A randomized, placebo-controlled, double-blinded, multicenter clinical trial. J. Med. Life 2017, 10, 153–160. [Google Scholar]
- Rezaei, Y.; Amiri-Nikpour, M.R.; Nazarbaghi, S.; Ahmadi-Salmasi, B.; Mokari, T.; Tahmtan, O. Cerebrolysin effects on neurological outcomes and cerebral blood flow in acute ischemic stroke. Neuropsychiatr. Dis. Treat. 2014, 10, 2299–2306. [Google Scholar] [CrossRef]
- Park, Y.K.; Yi, H.-J.; Choi, K.-S.; Lee, Y.-J.; Kim, D.-W.; Kwon, S.M. Cerebrolysin for the Treatment of Aneurysmal Subarachnoid Hemorrhage in Adults: A Retrospective Chart Review. Adv. Ther. 2018, 35, 2224–2235. [Google Scholar] [CrossRef] [PubMed]
- Rıos, C.; Nader-Kawachi, J.; Rodriguez-Payán, A.J.; Nava-Ruiz, C. Neuroprotective effect of dapsone in an occlusive model of focal ischemia in rats. Brain Res. 2004, 999, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Suda, T.; Suzuki, Y.; Matsui, T.; Inoue, T.; Niide, O.; Yoshimaru, T.; Suzuki, H.; Ra, C.; Ochiai, T. Dapsone suppresses human neutrophil superoxide production and elastase release in a calcium-dependent manner. Br. J. Dermatol. 2005, 152, 887–895. [Google Scholar] [CrossRef]
- He, J.; Zhang, X.; He, W.; Xie, Y.; Chen, Y.; Yang, Y.; Chen, R. Neuroprotective effects of zonisamide on cerebral ischemia injury via inhibition of neuronal apoptosis. Braz. J. Med. Biol. Res. 2021, 54, e10498. [Google Scholar] [CrossRef] [PubMed]
- Nader-Kawachi, J.; Góngora-Rivera, F.; Santos-Zambrano, J.; Calzada, P.; Ríos, C. Neuroprotective effect of dapsone in patients with acute ischemic stroke: A pilot study. Neurol. Res. 2007, 29, 331–334. [Google Scholar] [CrossRef]
- Mistry, A.; Mistry, E.A.; Kumar, N.G.; Froehler, M.T.; Fusco, M.R.; Chitale, R.V. Corticosteroids in the Management of Hyponatremia, Hypovolemia, and Vasospasm in Subarachnoid Hemorrhage: A Meta-Analysis. Cerebrovasc. Dis. 2016, 42, 263–271. [Google Scholar] [CrossRef]
- Brown, R.J.; Epling, B.P.; Staff, I.; Fortunato, G.; Grady, J.J.; McCullough, L.D. Polyuria and cerebral vasospasm after aneurysmal subarachnoid hemorrhage. BMC Neurol. 2015, 15, 201. [Google Scholar] [CrossRef] [PubMed]
- Egge, A.; Waterloo, K.; Sjoholm, H.; Solberg, T.; Ingebrigtsen, T.; Romner, B. Prophylactic hyperdynamic postoperative fluid therapy after aneurysmal subarachnoid hemorrhage: A clinical, prospective, randomized, controlled study. Neurosurgery 2001, 49, 593–605. [Google Scholar] [PubMed]
- Lennihan, L.; Mayer, S.A.; Fink, M.E.; Beckford, A.; Paik, M.C.; Zhang, H.; Wu, Y.C.; Klebanoff, L.M.; Raps, E.C.; Solomon, R.A. Effect of hypervolemic therapy on cerebral blood flow after subarachnoid hemorrhage: A randomized controlled trial. Stroke 2000, 31, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, I.; Hironaka, Y.; Nishimura, F.; Takeshima, Y.; Matsuda, R.; Yamada, S.; Motoyama, Y.; Park, Y.-S.; Nakase, H. Early Inhibition of Natriuresis Suppresses Symptomatic Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage. Cerebrovasc. Dis. 2013, 35, 131–137. [Google Scholar] [CrossRef]
- Miller, B.A.; Turan, N.; Chau, M.; Pradilla, G. Inflammation, vasospasm, and brain injury after subarachnoid hemorrhage. Biomed. Res. Int. 2014, 2014, 384342. [Google Scholar] [CrossRef]
- Chaudhry, S.R.; Stoffel-Wagner, B.; Kinfe, T.M.; Güresir, E.; Vatter, H.; Dietrich, D.; Lamprecht, A.; Muhammad, S. Elevated Systemic IL-6 Levels in Patients with Aneurysmal Subarachnoid Hemorrhage Is an Unspecific Marker for Post-SAH Complications. Int. J. Mol. Sci. 2017, 18, 2580. [Google Scholar] [CrossRef]
- Chyatte, D.; Fode, N.C.R.N.; Nichols, D.A.; Sundt, T.M. Preliminary Report: Effects of High Dose Methylprednisolone on Delayed Cerebral Ischemia in Patients at High Risk for Vasospasm after Aneurysmal Subarachnoid Hemorrhage. Neurosurgery 1987, 21, 157–160. [Google Scholar] [CrossRef]
- McGirt, M.J.; Mavropoulos, J.C.; McGirt, L.Y.; Alexander, M.J.; Friedman, A.H.; Laskowitz, D.T.; Lynch, J.R. Leukcytosis as an independent risk factor for cerebral vasospasm following aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2003, 98, 1222–1226. [Google Scholar] [CrossRef]
- Schürkämper, M.; Medele, R.; Zausinger, S.; Schmid-Elsaesser, R.; Steiger, H.-J. Dexamethasone in the treatment of subarachnoid hemorrhage revisited: A comparative analysis of the effect of the total dose on complications and outcome. J. Clin. Neurosci. 2004, 11, 20–24. [Google Scholar] [CrossRef]
- Güresir, E.; Lampmann, T.; Bele, S.; Czabanka, M.; Czorlich, P.; Gempt, J.; Goldbrunner, R.; Hurth, H.; Hermann, E.; Jabbarli, R.; et al. Fight INflammation to Improve outcome after aneurysmal Subarachnoid HEmorRhage (FINISHER) trial: Study protocol for a randomized controlled trial. Int. J. Stroke 2022, 18, 242–247. [Google Scholar] [CrossRef]
- Brotman, D.J.; Girod, J.P.; Posch, A.; Jani, J.T.; Patel, J.V.; Gupta, M.; Lip, G.Y.; Reddy, S.; Kickler, T.S. Effects of short-term glucocorticoids on hemostatic factors in healthy volunteers. Thromb. Res. 2006, 118, 247–252. [Google Scholar] [CrossRef]
- Isidori, A.M.; Minnetti, M.; Sbardella, E.; Graziadio, C.; Grossman, A.B. Mechanisms in endocrinology: The spectrum of haemostatic abnormalities in glucocorticoid excess and defect. Eur. J. Endocrinol. 2015, 173, R101–R113. [Google Scholar] [CrossRef] [PubMed]
- Ornelas, A.; Zacharias-Millward, N.; Menter, D.G.; Davis, J.S.; Lichtenberger, L.; Hawke, D.; Hawk, E.; Vilar, E.; Bhattacharya, P.; Millward, S. Beyond COX-1: The effects of aspirin on platelet biology and potential mechanisms of chemoprevention. Cancer Metastasis Rev. 2017, 36, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Year | Treatments and Sample Size | Doses | Treatment Duration | Recruiting Area |
|---|---|---|---|---|---|
| Chou et al. [25] | 2008 | Simvastatin = 19 versus SNT = 20 | 80 mg oral daily | Until discharge from NICU or until 21 days | United States of America |
| Diringer et al. [26] | 2016 | Simvastatin = 12 versus SNT = 12 | 80 mg oral daily | 21 days | United States of America |
| Garcia-Pastor et al. [27] | 2022 | Dapsone = 26 versus SNT = 22 | 100 mg oral daily | Within 5 days after ictus until day 15 | Mexico |
| Garg et al. [28] | 2013 | Simvastatin = 19 versus SNT = 19 | 80 mg daily for 14 days | 14 days | India |
| Gomis et al. [29] | 2010 | Methylprednisolone = 49 versus SNT = 46 | 16 mg/kg intravenous daily | 3 days | France |
| Hop et al. [30] | 2000 | ASA = 24 versus SNT = 26 | 100 mg suppositories daily | 21 days | Netherlands |
| Katayama et al. [31] | 2007 | Hydrocortisone = 35 versus SNT = 36 | 1200 mg/d (day 0–10), 600 mg/d (day 11–12), 300 mg/d (day 13–14) intravenously | 14 days | Japan |
| Kirkpatrick et al. [32] | 2014 | Simvastatin = 391 versus SNT = 412 | 40 mg oral daily | 3 weeks | UK, Canada, Colombia, Italy, Russia, Singapore, Sweden, Uruguay, USA |
| Martini et al. [33] | 2022 | Epoxide hydrolase inhibitor = 10 versus SNT = 10 | 10 mg oral daily | 10 days | United States of America |
| Suzuki et al. [34] | 1989 | OKY-046 = 172 versus SNT = 86 | 80 mg/day (low-dose group) 400 mg/day (high-dose group) intravenously | 10 to 14 days | Japan |
| Tseng et al. [35] | 2005 | Pravastatin = 40 versus SNT = 40 | 40 mg oral daily | Within 3 days after ictus for 14 days or until discharge | United Kingdom |
| Van den Bergh et al. [36] | 2006 | ASA = 83 versus SNT = 70 | 100 mg suppositories daily | 14 days | Netherlands |
| Vergouwen et al. [37] | 2009 | Simvastatin = 14 versus SNT = 16 | 80 mg oral daily | Within 3 days after SAH until day 14 | Netherlands |
| Woo et al. [38] | 2020 | Cerebrolysin = 25 versus SNT = 25 | 30 mL daily for 14 days | 14 days | Hong Kong |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wach, J.; Vychopen, M.; Güresir, A.; Güresir, E. Anti-Inflammatory Drug Therapy in Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis of Prospective Randomized and Placebo-Controlled Trials. J. Clin. Med. 2023, 12, 4165. https://doi.org/10.3390/jcm12124165
Wach J, Vychopen M, Güresir A, Güresir E. Anti-Inflammatory Drug Therapy in Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis of Prospective Randomized and Placebo-Controlled Trials. Journal of Clinical Medicine. 2023; 12(12):4165. https://doi.org/10.3390/jcm12124165
Chicago/Turabian StyleWach, Johannes, Martin Vychopen, Agi Güresir, and Erdem Güresir. 2023. "Anti-Inflammatory Drug Therapy in Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis of Prospective Randomized and Placebo-Controlled Trials" Journal of Clinical Medicine 12, no. 12: 4165. https://doi.org/10.3390/jcm12124165
APA StyleWach, J., Vychopen, M., Güresir, A., & Güresir, E. (2023). Anti-Inflammatory Drug Therapy in Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis of Prospective Randomized and Placebo-Controlled Trials. Journal of Clinical Medicine, 12(12), 4165. https://doi.org/10.3390/jcm12124165