

Physical Health-Related Quality of Life Improves over Time in Post-COVID-19 Patients: An Exploratory Prospective Study
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
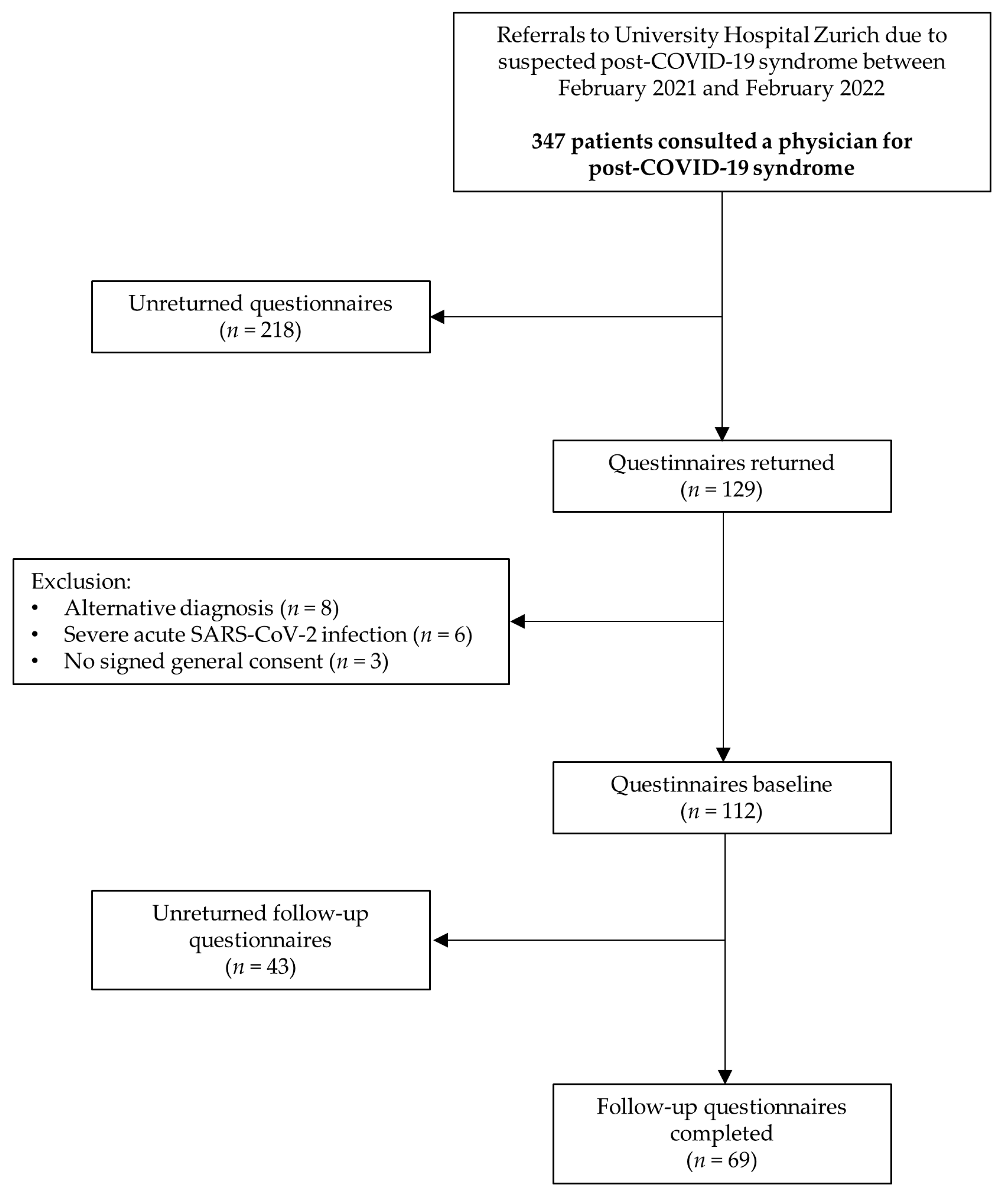
2.1. Study Design and Patient Population
2.2. Questionnaires
2.2.1. St. George’s Respiratory Questionnaire
2.2.2. EuroQol 5 Dimension 5 Level
2.2.3. Short Form-36
2.2.4. Questionnaire about COVID-19 Vaccination
2.3. Statistical Analysis
3. Results
3.1. Study Sample
3.2. Symptom Characterization at Baseline
3.3. Subjective Effect of Vaccination on Post-COVID-19 Symptoms
3.4. SGRQ Questionnaire
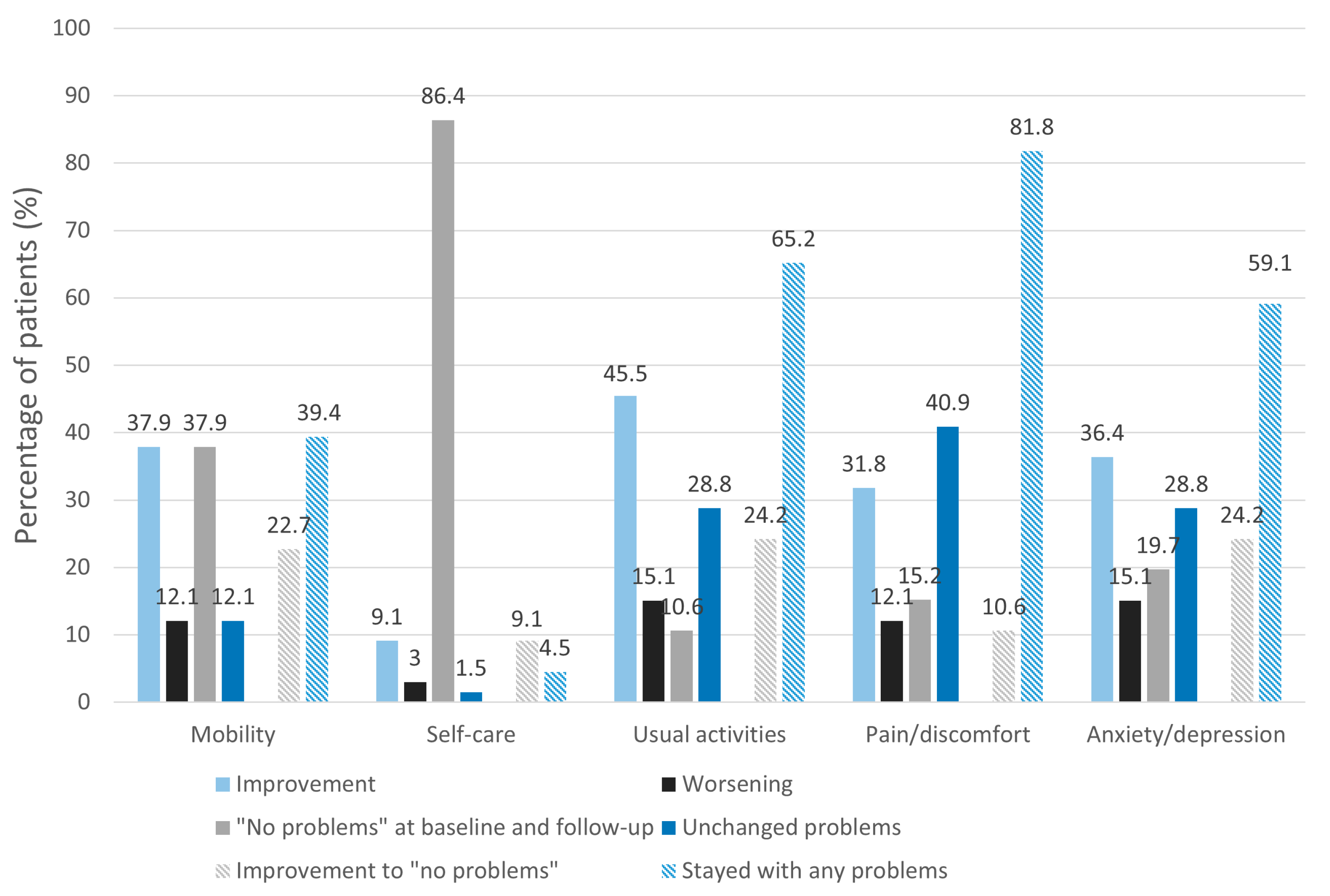
3.5. EQ-5D-5L
3.6. SF-36
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institute for Health and Care Excellence. Clinical Guidelines. In COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute for Health and Care Excellence (NICE): London, UK, 2020. [Google Scholar]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. Eclinicalmedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the Frequency and Variety of Persistent Symptoms among Patients with COVID-19: A Systematic Review. JAMA Netw. Open 2021, 4, e2111417. [Google Scholar] [CrossRef]
- White, P.D.; Thomas, J.M.; Amess, J.; Crawford, D.H.; Grover, S.A.; Kangro, H.O.; Clare, A.W. Incidence, risk and prognosis of acute and chronic fatigue syndromes and psychiatric disorders after glandular fever. Br. J. Psychiatry 1998, 173, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Moldofsky, H.; Patcai, J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; A case-controlled study. BMC Neurol. 2011, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.N.; Hause, A.M.; Walker, C.M.; Orange, J.S.; Hasbun, R.; Murray, K.O. Evaluation of Prolonged Fatigue Post–West Nile Virus Infection and Association of Fatigue with Elevated Antiviral and Proinflammatory Cytokines. Viral Immunol. 2014, 27, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef]
- Hardt, J.; Buchwald, D.; Wilks, D.; Sharpe, M.; Nix, W.; Egle, U. Health-related quality of life in patients with chronic fatigue syndrome: An international study. J. Psychosom. Res. 2001, 51, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Malesevic, S.; Sievi, N.A.; Baumgartner, P.; Roser, K.; Sommer, G.; Schmidt, D.; Vallelian, F.; Jelcic, I.; Clarenbach, C.F.; Kohler, M. Impaired health-related quality of life in long-COVID syndrome after mild to moderate COVID-19. Sci. Rep. 2023, 13, 7717. [Google Scholar] [CrossRef]
- Nittas, V.; Puhan, M. Literature screening repport—Update 6. Long COVID: Evolving Definitions, Burden of Disease and Socio-Economic Consequences; Bundesamt für Gesundheit. 2021. Available online: https://www.bag.admin.ch, (accessed on 2 May 2023).
- Tran, V.-T.; Porcher, R.; Pane, I.; Ravaud, P. Course of post COVID-19 disease symptoms over time in the ComPaRe long COVID prospective e-cohort. Nat. Commun. 2022, 13, 1812. [Google Scholar] [CrossRef]
- Jones, P.W. Quality of life measurement for patients with diseases of the airways. Thorax 1991, 46, 676–682. [Google Scholar] [CrossRef]
- Jones, P.; Quirk, F.; Baveystock, C. The St George’s Respiratory Questionnaire. Respir. Med. 1991, 85, 25–31. [Google Scholar] [CrossRef]
- Jones, P.W. St. George’s Respiratory Questionnaire Manual. Available online: https://meetinstrumentenzorg.nl/wp-content/uploads/instrumenten/SGRQ-handl-Eng.pdf (accessed on 14 April 2022).
- Jones, P.W. St. George’s Respiratory Questionnaire: MCID. COPD J. Chronic Obstr. Pulm. Dis. 2005, 2, 75–79. [Google Scholar] [CrossRef] [PubMed]
- The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef] [PubMed]
- McClure, N.S.; Al Sayah, F.; Ohinmaa, A.; Johnson, J.A. Minimally Important Difference of the EQ-5D-5L Index Score in Adults with Type 2 Diabetes. Value Health 2018, 21, 1090–1097. [Google Scholar] [CrossRef]
- McClure, N.S.; Al Sayah, F.; Xie, F.; Luo, N.; Johnson, J.A. Instrument-Defined Estimates of the Minimally Important Difference for EQ-5D-5L Index Scores. Value Health 2017, 20, 644–650. [Google Scholar] [CrossRef]
- Tsai, A.P.Y.; Hur, S.A.; Wong, A.; Safavi, M.; Assayag, D.; Johannson, K.A.; Morisset, J.; Fell, C.; Fisher, J.H.; Manganas, H.; et al. Minimum important difference of the EQ-5D-5L and EQ-VAS in fibrotic interstitial lung disease. Thorax 2020, 76, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef]
- Laucis, N.C.; Hays, R.D.; Bhattacharyya, T. Scoring the SF-36 in Orthopaedics: A Brief Guide. J. Bone Jt. Surg. 2015, 97, 1628–1634. [Google Scholar] [CrossRef]
- Taft, C.; Karlsson, J.; Sullivan, M. Do SF-36 summary component scores accurately summarize subscale scores? Qual. Life Res. 2001, 10, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Frendl, D.; Ware, J.E. Patient-reported Functional Health and Well-Being Outcomes with Drug Therapy: A Systematic Review of Randomized Trials Using the SF-36 Health Survey. Med. Care 2014, 52, 439–445. [Google Scholar] [CrossRef]
- Bjorner, J.B.; Wallenstein, G.V.; Martin, M.C.; Lin, P.; Blaisdell-Gross, B.; Piech, C.T.; Mody, S.H. Interpreting score differences in the SF-36 Vitality scale: Using clinical conditions and functional outcomes to define the minimally important difference. Curr. Med. Res. Opin. 2007, 23, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Viero, G.; Bettini, G.; Nobili, A.; Tettamanti, M.; Galbussera, A.A.; Muscatello, A.; Mantero, M.; Canetta, C.; Boneschi, F.M.; et al. Patient-Reported Symptoms and Sequelae 12 Months after COVID-19 in Hospitalized Adults: A Multicenter Long-Term Follow-Up Study. Front. Med. 2022, 9, 834354. [Google Scholar] [CrossRef]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M.; et al. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef]
- Petersen, M.S.; Kristiansen, M.F.; Hanusson, K.D.; Danielsen, M.E.; Steig, B.; Gaini, S.; Strøm, M.; Weihe, P. Long COVID in the Faroe Islands: A Longitudinal Study Among Nonhospitalized Patients. Clin. Infect. Dis. 2020, 73, e4058–e4063. [Google Scholar] [CrossRef]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent Symptoms in Adult Patients 1 Year After Coronavirus Disease 2019 (COVID-19): A Prospective Cohort Study. Clin. Infect. Dis. 2022, 74, 1191–1198. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bermingham, C.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Trajectory of long covid symptoms after covid-19 vaccination: Community based cohort study. BMJ 2022, 377, e069676. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.J.; Beiser, M.M. Major Depression and Depressive Symptomatology among the Physically Disabled. Assessing the role of chronic stress. J. Nerv. Ment. Dis. 1990, 178, 343–350. [Google Scholar] [CrossRef]
- Morgan, A.J.; Rapee, R.M.; Bayer, J.K. Increasing response rates to follow-up questionnaires in health intervention research: Randomized controlled trial of a gift card prize incentive. Clin. Trials 2017, 14, 381–386. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n = 69 | |
|---|---|
| Sex | |
| Female | 55 (80.0) |
| Male | 14 (20.0) |
| Age, mean (SD) | 44.2 (11.9) |
| BMI kg/m2, median (IQR) | 24.2 (21.5, 26.7) |
| WHO classification | |
| Mild | 65 (94.2) |
| Moderate | 4 (5.8) |
| Days from first questionnaire to follow-up questionnaire, median (IQR) | 182 (174, 192) |
| Days from symptom onset to follow-up questionnaire, median (IQR) | 326 (300, 391) |
| Smoking history | |
| Current | 6 (8.7) |
| Former | 18 (26.1) |
| Never | 38 (55.2) |
| Ethnicity | |
| Caucasian | 58 (84) |
| Not Caucasian | 2 (3) |
| Missing data | 9 (13) |
| Marital status | |
| Living with a partner | 38 (55.1) |
| Living alone | 10 (14.5) |
| Missing data | 21 (30.4) |
| Reduced employment due to post-COVID-19 | 22 (31.9) |
| Reduced ≥ 50% | 10 (14.5) |
| Reduced < 50% | 12 (17.4) |
| Comorbidities | |
| Asthma | 9 (13.0) |
| Prepandemic mental health issues | 7 (10.1) |
| Other relevant comorbidities a | 14 (20.3) |
| Baseline, Mean (SD) | Follow-Up, Mean (SD) | Δ *, Mean (95% CI) | p-Value | |
|---|---|---|---|---|
| SGRQ symptom score a | 40.4 (21.0) | 26.0 (21.1) | −14.4 (−18.4, −10.3) | p < 0.001 |
| SGRQ activity score b | 51.3 (25.4) | 39.1 (27.6) | −12.2 (−17.4, −7.0) | p < 0.001 |
| SGRQ impact score b | 27.2 (17.7) | 20.8 (18.5) | −6.5 (−10.2, −2.7) | p = 0.001 |
| SGRQ total score c | 37.3 (20.2) | 27.9 (20.2) | −9.4 (−13.3, −5.5) | p < 0.001 |
| EQ index value d | 0.758 (0.203) | 0.818 (0.168) | 0.060 (0.019, 0.102) | p = 0.005 |
| EQ VAS e | 59.1 (20.9) | 66.0 (20.3) | 6.9 (2.7, 11.1) | p = 0.002 |
| Baseline, Mean (SD) | Follow-Up, Mean (SD) | Δ *, Mean (95% CI) | p-Value | |
|---|---|---|---|---|
| Physical functioning a | 63.4 (24.6) | 75.4 (20.3) | 12.1 (7.0, 17.1) | p < 0.001 |
| Role limitations (physical) b | 27.6 (35.7) | 48.1 (42.9) | 20.5 (10.9, 30.2) | p < 0.001 |
| Pain b | 56.7 (28.9) | 67.3 (28.7) | 10.7 (4.2, 17.1) | p = 0.002 |
| General c | 54.1 (18.2) | 54.7 (19.1) | 0.7 (−3.7, 4.9) | p = 0.795 |
| Energy/vitality c | 29.8 (19.4) | 40.8 (21.7) | 11.0 (6.3, 15.7) | p < 0.001 |
| Social functioning d | 57.9 (28.2) | 62.5 (29.7) | 4.6 (−2.4, 11.7) | p = 0.195 |
| Role limitations (emotional) b | 57.7 (44.8) | 69.2 (41.2) | 11.4 (0.98, 21.9) | p = 0.032 |
| Emotional health c | 61.3 (19.1) | 66.9 (18.0) | 5.6 (1.3, 9.8) | p = 0.011 |
| PCS (T-score) d | 38.2 (10.2) | 43.0 (10.9) | 4.9 (2.6, 7.2) | p < 0.001 |
| MCS (T-score) d | 41.8 (11.5) | 44.1 (11.5) | 2.3 (−0.2, 4.8) | p = 0.069 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malesevic, S.; Sievi, N.A.; Schmidt, D.; Vallelian, F.; Jelcic, I.; Kohler, M.; Clarenbach, C.F. Physical Health-Related Quality of Life Improves over Time in Post-COVID-19 Patients: An Exploratory Prospective Study. J. Clin. Med. 2023, 12, 4077. https://doi.org/10.3390/jcm12124077
Malesevic S, Sievi NA, Schmidt D, Vallelian F, Jelcic I, Kohler M, Clarenbach CF. Physical Health-Related Quality of Life Improves over Time in Post-COVID-19 Patients: An Exploratory Prospective Study. Journal of Clinical Medicine. 2023; 12(12):4077. https://doi.org/10.3390/jcm12124077
Chicago/Turabian StyleMalesevic, Stefan, Noriane A. Sievi, Dörthe Schmidt, Florence Vallelian, Ilijas Jelcic, Malcolm Kohler, and Christian F. Clarenbach. 2023. "Physical Health-Related Quality of Life Improves over Time in Post-COVID-19 Patients: An Exploratory Prospective Study" Journal of Clinical Medicine 12, no. 12: 4077. https://doi.org/10.3390/jcm12124077
APA StyleMalesevic, S., Sievi, N. A., Schmidt, D., Vallelian, F., Jelcic, I., Kohler, M., & Clarenbach, C. F. (2023). Physical Health-Related Quality of Life Improves over Time in Post-COVID-19 Patients: An Exploratory Prospective Study. Journal of Clinical Medicine, 12(12), 4077. https://doi.org/10.3390/jcm12124077