

The Association between Dysnatraemia during Hospitalisation and Post-COVID-19 Mental Fatigue
 , , ,
, , , 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
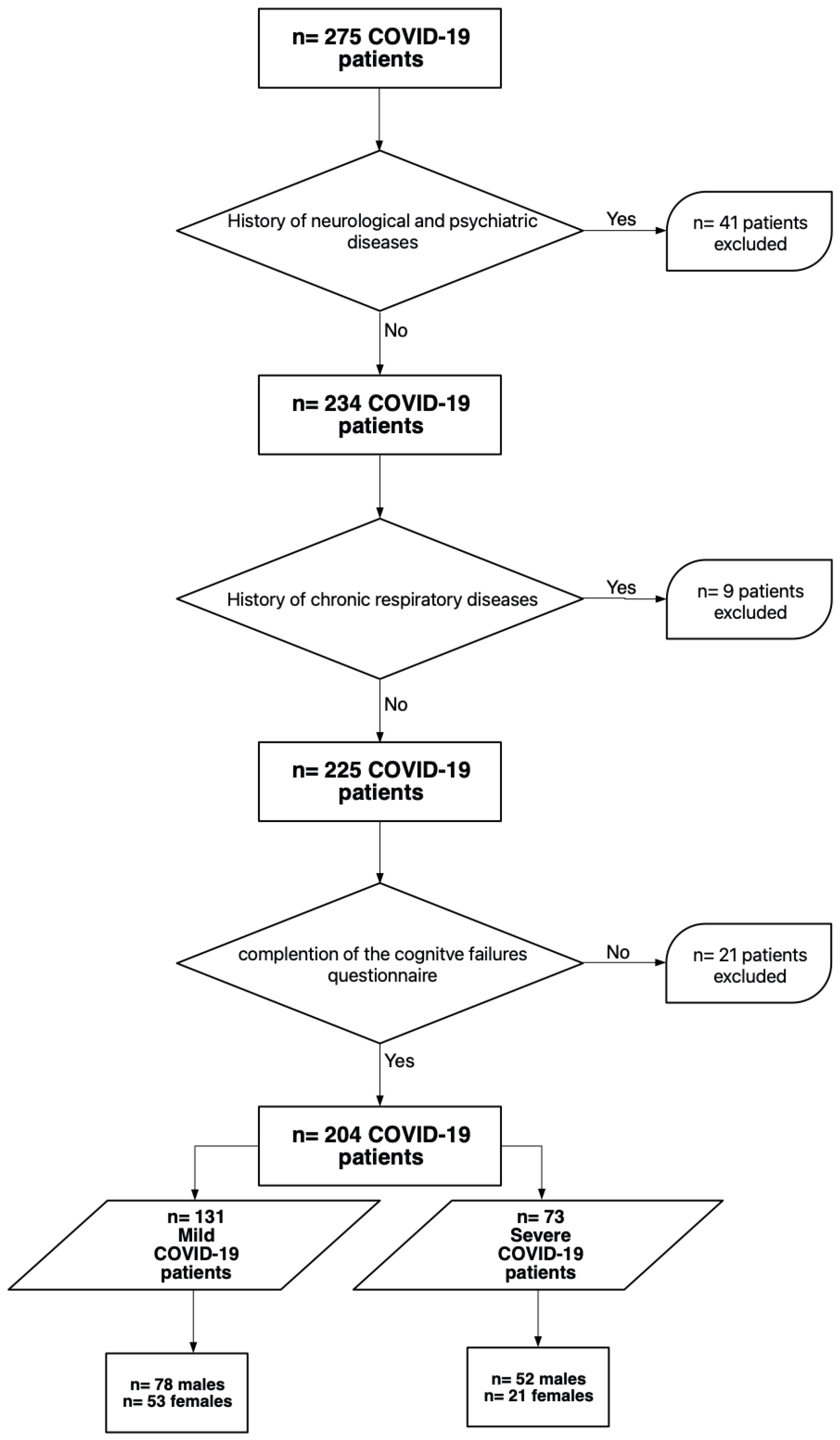
2.1. Patients
2.2. Clinical Questionnaire on Cognitive Failures
2.3. Laboratory Test and Data Sources
2.4. Statistical Analysis Plan
3. Results
3.1. Persistent Cognitive Failures: The Impact of the Disease Course Severity and Sex
3.2. Association between Persistent Mental Fatigue and the Electrolyte Profile during Hospitalisation
4. Discussion
5. Conclusions and Clinical Significance
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. Available online: http://www.nature.com/articles/s41591-021-01283-z (accessed on 15 September 2021). [CrossRef] [PubMed]
- Goërtz, Y.M.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542–02020. [Google Scholar] [CrossRef] [PubMed]
- Manca, R.; De Marco, M.; Ince, P.G.; Venneri, A. Heterogeneity in Regional Damage Detected by Neuroimaging and Neuropathological Studies in Older Adults with COVID-19: A Cognitive-Neuroscience Systematic Review to Inform the Long-Term Impact of the Virus on Neurocognitive Trajectories. Front. Aging Neurosci. 2021, 13, 646908. [Google Scholar] [CrossRef] [PubMed]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef] [PubMed]
- On behalf of the “Cognitive and Behavioral Neurology” Study Group of the Italian Neurological Society; Stracciari, A.; Bottini, G.; Guarino, M.; Magni, E.; Pantoni, L. Cognitive and behavioral manifestations in SARS-CoV-2 infection: Not specific or distinctive features? Neurol. Sci. 2021, 42, 2273–2281. Available online: https://link.springer.com/10.1007/s10072-021-05231-0 (accessed on 15 September 2021). [CrossRef]
- Almeria, M.; Cejudo, J.C.; Sotoca, J.; Deus, J.; Krupinski, J. Cognitive profile following COVID-19 infection: Clinical predictors leading to neuropsychological impairment. Brain Behav. Immun.-Health 2020, 9, 100163. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2666354620301289 (accessed on 14 September 2021). [CrossRef]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. Available online: https://linkinghub.elsevier.com/retrieve/pii/S221503662030287X (accessed on 15 September 2021). [CrossRef]
- Molnar, T.; Varnai, R.; Schranz, D.; Zavori, L.; Peterfi, Z.; Sipos, D.; Tőkés-Füzesi, M.; Illes, Z.; Buki, A.; Csecsei, P. Severe Fatigue and Memory Impairment Are Associated with Lower Serum Level of Anti-SARS-CoV-2 Antibodies in Patients with Post-COVID Symptoms. J. Clin. Med. 2021, 10, 4337. Available online: https://www.mdpi.com/2077-0383/10/19/4337 (accessed on 15 May 2023). [CrossRef]
- The Writing Committee for the COMEBAC Study Group; Morin, L.; Savale, L.; Pham, T.; Colle, R.; Figueiredo, S.; Harrois, A.; Gasnier, M.; Lecoq, A.-L.; Meyrignac, O.; et al. Four-Month Clinical Status of a Cohort of Patients After Hospitalization for COVID-19. JAMA 2021, 325, 1525. Available online: https://jamanetwork.com/journals/jama/fullarticle/2777787 (accessed on 14 April 2022).
- Jacobs, L.G.; Paleoudis, E.G.; Bari, D.L.-D.; Nyirenda, T.; Friedman, T.; Gupta, A.; Rasouli, L.; Zetkulic, M.; Balani, B.; Ogedegbe, C.; et al. Persistence of symptoms and quality of life at 35 days after hospitalisation for COVID-19 infection. PLoS ONE 2020, 15, e0243882. [Google Scholar] [CrossRef]
- Poudel, A.N.; Zhu, S.; Cooper, N.; Roderick, P.; Alwan, N.; Tarrant, C.; Ziauddeen, N.; Yao, G.L. Impact of Covid-19 on health-related quality of life of patients: A structured review. PLoS ONE 2021, 16, e0259164. [Google Scholar] [CrossRef]
- Hampshire, A.; Trender, W.; Chamberlain, S.R.; Jolly, A.E.; Grant, J.E.; Patrick, F.; Mazibuko, N.; Williams, S.C.; Barnby, J.M.; Hellyer, P.; et al. Cognitive deficits in people who have recovered from COVID-19. EClinicalMedicine 2021, 39, 101044. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2589537021003242 (accessed on 14 April 2022). [CrossRef]
- Alemanno, F.; Houdayer, E.; Parma, A.; Spina, A.; Del Forno, A.; Scatolini, A.; Angelone, S.; Brugliera, L.; Tettamanti, A.; Beretta, L.; et al. COVID-19 cognitive deficits after respiratory assistance in the subacute phase: A COVID-rehabilitation unit experience. PLoS ONE 2021, 16, e0246590. [Google Scholar] [CrossRef]
- Romero-Duarte, Á.; Rivera-Izquierdo, M.; de Alba, I.G.-F.; Pérez-Contreras, M.; Fernández-Martínez, N.F.; Ruiz-Montero, R.; Serrano-Ortiz, Á.; González-Serna, R.O.; Salcedo-Leal, I.; Jiménez-Mejías, E.; et al. Sequelae, persistent symptomatology and outcomes after COVID-19 hospitalisation: The ANCOHVID multicentre 6-month follow-up study. BMC Med. 2021, 19, 129. [Google Scholar] [CrossRef]
- Sigfrid, L.; Drake, T.M.; Pauley, E.; Jesudason, E.C.; Olliaro, P.; Lim, W.S.; Gillesen, A.; Berry, C.; Lowe, D.J.; McPeake, J.; et al. Long Covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol. Lancet Reg. Health-Eur. 2021, 8, 100186. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2666776221001630 (accessed on 14 April 2022). [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, e9–e611. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1198743X21006297 (accessed on 14 April 2022). [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. Available online: https://www.bmj.com/lookup/doi/10.1136/bmj.m1985 (accessed on 14 April 2022). [CrossRef]
- Song, H.J.J.M.D.; Chia, A.Z.Q.; Tan, B.K.J.; Teo, C.B.; Lim, V.; Chua, H.R.; Samuel, M.; Kee, A. Electrolyte imbalances as poor prognostic markers in COVID-19: A systemic review and meta-analysis. J. Endocrinol. Investig. 2022, 46, 235–259. Available online: https://link.springer.com/10.1007/s40618-022-01877-5 (accessed on 3 March 2023). [CrossRef]
- Pani, A.; Inglese, E.; Puoti, M.; Cento, V.; Alteri, C.; Romandini, A.; Di Ruscio, F.; Senatore, M.; Moreno, M.; Tarsia, P.; et al. Sex differences in electrolyte imbalances caused by SARS-CoV-2: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14882. [Google Scholar] [CrossRef]
- Zimmer, M.A.; Zink, A.K.; Weißer, C.W.; Vogt, U.; Michelsen, A.; Priebe, H.-J.; Mols, G. Hypernatremia—A Manifestation of COVID-19: A Case Series. AA Pract. 2020, 14, e01295. Available online: https://journals.lww.com/10.1213/XAA.0000000000001295 (accessed on 2 May 2022). [CrossRef]
- Adrogué, H.J.; Madias, N.E. Hypernatremia. N. Engl. J. Med. 2000, 342, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Tsipotis, E.; Price, L.L.; Jaber, B.L.; Madias, N.E. Hospital-Associated Hypernatremia Spectrum and Clinical Outcomes in an Unselected Cohort. Am. J. Med. 2018, 131, 72–82.e1. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0002934317308410 (accessed on 2 May 2022). [CrossRef] [PubMed]
- Nowak, K.L.; Yaffe, K.; Orwoll, E.S.; Ix, J.H.; You, Z.; Barrett-Connor, E.; Hoffman, A.R.; Chonchol, M. Serum Sodium and Cognition in Older Community-Dwelling Men. Clin. J. Am. Soc. Nephrol. 2018, 13, 366–374. Available online: https://cjasn.asnjournals.org/lookup/doi/10.2215/CJN.07400717 (accessed on 6 April 2022). [CrossRef] [PubMed]
- Lee, S.; Min, J.-Y.; Kim, B.; Ha, S.-W.; Han, J.H.; Min, K.-B. Serum sodium in relation to various domains of cognitive function in the elderly US population. BMC Geriatr. 2021, 21, 328. Available online: https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-021-02260-4 (accessed on 6 April 2022). [CrossRef]
- Giuliani, C.; Peri, A. Effects of Hyponatremia on the Brain. J. Clin. Med. 2014, 3, 1163–1177. Available online: https://www.mdpi.com/2077-0383/3/4/1163 (accessed on 6 April 2022). [CrossRef]
- Soiza, R.L.; Cumming, K.; Clarke, J.M.; Wood, K.M.; Myint, P.K. Hyponatremia: Special Considerations in Older Patients. J. Clin. Med. 2014, 3, 944–958. Available online: https://www.mdpi.com/2077-0383/3/3/944 (accessed on 6 April 2022). [CrossRef]
- Broadbent, D.E.; Cooper, P.F.; FitzGerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. Available online: https://onlinelibrary.wiley.com/doi/10.1111/j.2044-8260.1982.tb01421.x (accessed on 6 April 2022). [CrossRef]
- Santangelo, G.; Baldassarre, I.; Barbaro, A.; Cavallo, N.D.; Cropano, M.; Maggi, G.; Nappo, R.; Trojano, L.; Raimo, S. Subjective cognitive failures and their psychological correlates in a large Italian sample during quarantine/self-isolation for COVID-19. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2021, 42, 2625–2635. [Google Scholar] [CrossRef]
- Fang, X.; Ming, C.; Cen, Y.; Lin, H.; Zhan, K.; Yang, S.; Li, L.; Cao, G.; Li, Q.; Ma, X. Post-sequelae one year after hospital discharge among older COVID-19 patients: A multi-center prospective cohort study. J. Infect. 2022, 84, 179–186. Available online: https://linkinghub.elsevier.com/retrieve/pii/S016344532100596X (accessed on 14 April 2022). [CrossRef]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100899. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2589537021001796 (accessed on 14 April 2022). [CrossRef]
- Oliviero, A.; de Castro, F.; Coperchini, F.; Chiovato, L.; Rotondi, M. COVID-19 Pulmonary and Olfactory Dysfunctions: Is the Chemokine CXCL10 the Common Denominator? Neuroscientist 2021, 27, 214–221. Available online: http://journals.sagepub.com/doi/10.1177/1073858420939033 (accessed on 15 September 2021). [CrossRef]
- Ritchie, K.; Chan, D.; Watermeyer, T. The cognitive consequences of the COVID-19 epidemic: Collateral damage? Brain Commun. 2020, 2, fcaa069. Available online: https://academic.oup.com/braincomms/article/doi/10.1093/braincomms/fcaa069/5848404 (accessed on 15 September 2021). [CrossRef]
- Olsson, K.; Öhlin, B.; Melander, O. Epidemiology and characteristics of hyponatremia in the emergency department. Eur. J. Intern. Med. 2013, 24, 110–116. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0953620512002877 (accessed on 15 April 2022). [CrossRef]



{kind=link}
{kind=link}
| Self-Administered Cognitive Failures Questionnaire |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Mild COVID-19 (N = 131) | Severe COVID-19 (N = 73) | Interaction Disease Severity by Sex | |||
|---|---|---|---|---|---|
| Males | Females | Males | Females | p-Value | |
| N | 78 | 53 | 52 | 21 | 0.096 |
| Age, mean (SD) | 58.3 (14.5) | 57.8 (14.3) | 55.0 (11.5) | 62.4 (11.5) | 0.069 |
| Length of hospital stay, mean (SD) | 15.5 (9.9) | 15.01 (7.6) | 22.1 (11.1) | 24.7 (13.6) | 0.373 |
| Follow-up time, mean (SD) | 53.6 (16.6) | 49.6 (13.6) | 46.8 (17.4) | 45.1 (19.6) | 0.664 |
| Sex = Female | Sex = Male | |||||
|---|---|---|---|---|---|---|
| ITEM 18 | β | 95%CI | p-Value | β | 95%CI | p-Value |
| Mild COVID-19 | 0.29 | 0.06; 0.53 | 0.01 | −0.01 | −0.14; 0.11 | 0.82 |
| Follow-up time | 0.004 | −0.003; 0.01 | 0.27 | 0.003 | −0.0007; 0.006 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvato, G.; Inglese, E.; Fazia, T.; Crottini, F.; Crotti, D.; Valentini, F.; Palmas, G.; Bollani, A.; Basilico, S.; Gandola, M.; et al. The Association between Dysnatraemia during Hospitalisation and Post-COVID-19 Mental Fatigue. J. Clin. Med. 2023, 12, 3702. https://doi.org/10.3390/jcm12113702
Salvato G, Inglese E, Fazia T, Crottini F, Crotti D, Valentini F, Palmas G, Bollani A, Basilico S, Gandola M, et al. The Association between Dysnatraemia during Hospitalisation and Post-COVID-19 Mental Fatigue. Journal of Clinical Medicine. 2023; 12(11):3702. https://doi.org/10.3390/jcm12113702
Chicago/Turabian StyleSalvato, Gerardo, Elvira Inglese, Teresa Fazia, Francesco Crottini, Daniele Crotti, Federica Valentini, Giulio Palmas, Alessandra Bollani, Stefania Basilico, Martina Gandola, and et al. 2023. "The Association between Dysnatraemia during Hospitalisation and Post-COVID-19 Mental Fatigue" Journal of Clinical Medicine 12, no. 11: 3702. https://doi.org/10.3390/jcm12113702
APA StyleSalvato, G., Inglese, E., Fazia, T., Crottini, F., Crotti, D., Valentini, F., Palmas, G., Bollani, A., Basilico, S., Gandola, M., Gelosa, G., Gentilini, D., Bernardinelli, L., Stracciari, A., Scaglione, F., Agostoni, E. C., & Bottini, G. (2023). The Association between Dysnatraemia during Hospitalisation and Post-COVID-19 Mental Fatigue. Journal of Clinical Medicine, 12(11), 3702. https://doi.org/10.3390/jcm12113702