
Augmentation Therapies as Treatments for Coexisting Somatic Problems in Schizophrenia—A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Method
2.1. Protocol and Registration
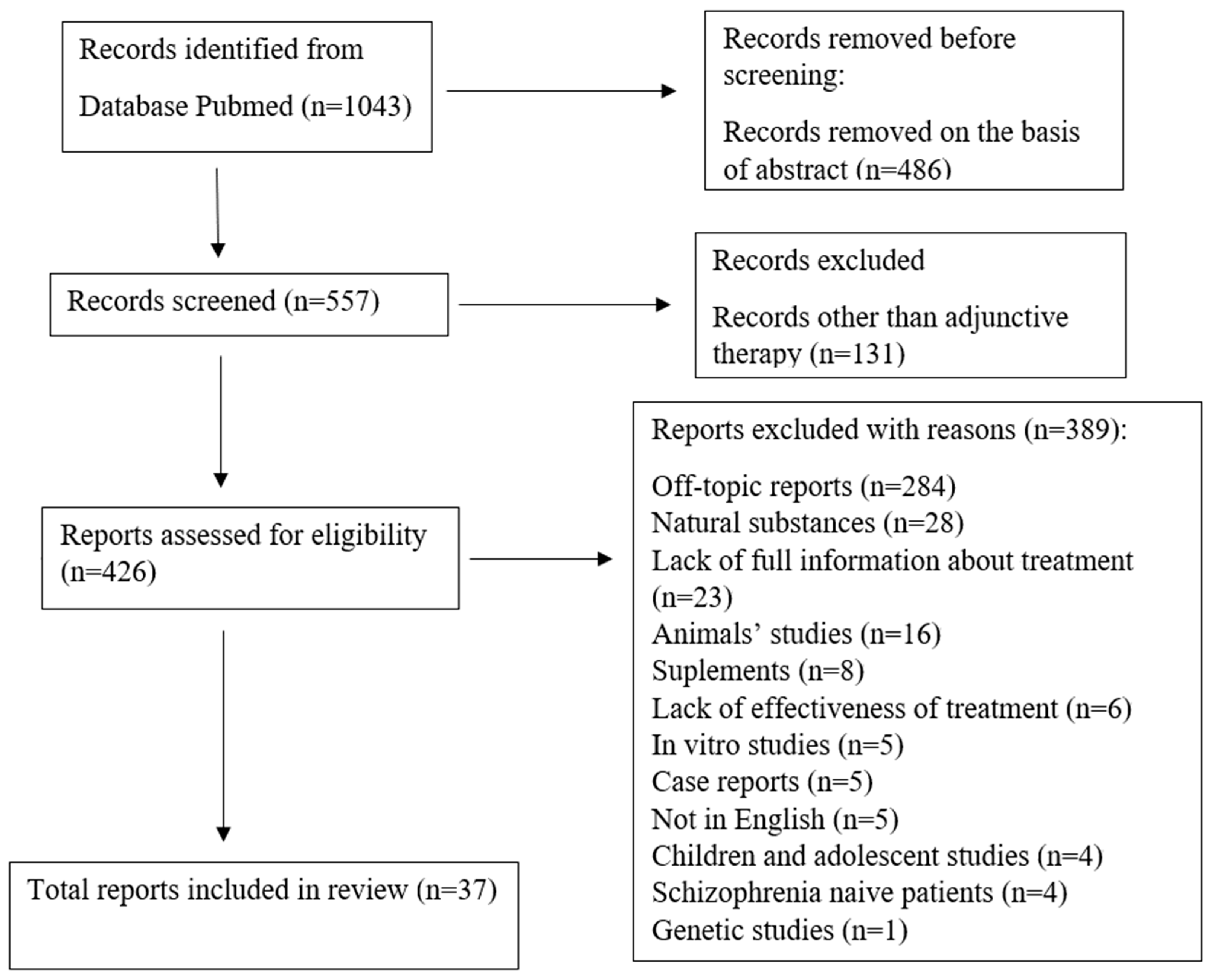
2.2. Search Process
2.3. Data Extraction
2.4. Study Inclusion and Exclusion Criteria
2.5. Risk of Bias Assessment
- 1.
- Control-comparison: Was there a control group or comparator to which adjunctive therapy was compared?
- 2.
- Ordering/assignment control: Was it assured that the interventions or intervention groups being compared were randomized or counterbalanced?
- 3.
- Pre/post-comparison: Was there a pre-measurement to which the post-measurement was compared?
- 4.
- Follow-up: Was there a follow-up measurement after weeks?
- 5.
- Registration: Was the study enrolled in an official study register?
- 6.
- Experimenter-blinding: Were the study conductors blinded with respect to the interventions or intervention groups being compared?
- 7.
- Analyst-blinding: Were the study evaluators blinded with respect to the interventions or intervention groups being compared?
- 8.
- Participant-blinding: Were the participants naive to whether they received an actual intervention or a control intervention?
3. Results
4. Discussion
4.1. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
4.2. Other Anti-Inflammatory Drugs
4.3. Antioxidants: N-acetylcysteine (NAC)
4.4. Peroxisome Proliferator-Activated Receptor Gamma (PPARγ) Agonists
4.5. Estrogens
4.6. N-methyl-D-aspartate Receptor (NMDA) Antagonists
4.7. Serotonergic Drugs
4.8. Antihypertensive Drugs
4.9. Incretin Drugs
5. Clinical Significance—Future Directions
6. Limitations
7. Summary
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Nucifora, F.C.; Woznica, E.; Lee, B.J.; Cascella, N.; Sawa, A. Treatment resistant schizophrenia: Clinical, biological, and therapeutic perspectives. Neurobiol. Dis. 2019, 131, 104257. [Google Scholar] [CrossRef]
- McCutcheon, R.; Marques, T.R.; Howes, O.D. Schizophrenia—An Overview. JAMA Psychiatry 2020, 77, 210. [Google Scholar] [CrossRef]
- Leichsenring, F.; Steinert, C.; Rabung, S.; Ioannidis, J.P. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: An umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry 2022, 21, 133–145. [Google Scholar] [CrossRef]
- Charlson, F.J.; Ferrari, A.J.; Santomauro, D.F.; Diminic, S.; Stockings, E.; Scott, J.G.; McGrath, J.J.; Whiteford, A.H. Global Epidemiology and Burden of Schizophrenia: Findings from the Global Burden of Disease Study 2016. Schizophr. Bull. 2018, 44, 1195–1203. [Google Scholar] [CrossRef]
- Correll, C.U.; Rubio, J.M.; Inczedy-Farkas, G.; Birnbaum, M.L.; Kane, J.M.; Leucht, S. Efficacy of 42 Pharmacologic Cotreatment Strategies Added to Antipsychotic Monotherapy in Schizophrenia: Systematic Overview and Quality Appraisal of the Meta-analytic Evidence. JAMA Psychiatry 2017, 74, 675–684. [Google Scholar] [CrossRef]
- Dieset, I.; Andreassen, O.A.; Haukvik, U.K. Somatic Comorbidity in Schizophrenia: Some Possible Biological Mechanisms Across the Life Span. Schizophr. Bull. 2016, 42, 1316–1319. [Google Scholar] [CrossRef] [Green Version]
- Lindekilde, N.; Scheuer, S.H.; Rutters, F.; Knudsen, L.; Lasgaard, M.; Rubin, K.H.; Henriksen, J.E.; Kivimäki, M.; Andersen, G.S.; Pouwer, F. Prevalence of type 2 diabetes in psychiatric disorders: An umbrella review with meta-analysis of 245 observational studies from 32 systematic reviews. Diabetologia 2021, 65, 440–456. [Google Scholar] [CrossRef]
- Oud, M.J.T.; Jong, B.M.-D. Somatic diseases in patients with schizophrenia in general practice: Their prevalence and health care. BMC Fam. Pr. 2009, 10, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gondek, T.; Królicka, A.; Piotrowski, P.; Kiejna, A. The European studies on mortality in schizophrenia. Psychiatr. Polska 2015, 49, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Laursen, T.M.; Nordentoft, M.; Mortensen, P.B. Excess Early Mortality in Schizophrenia. Annu. Rev. Clin. Psychol. 2014, 10, 425–448. [Google Scholar] [CrossRef] [PubMed]
- Yasar, H.; Yildiz, M. Assessment of Mortality Rate in 10 Years and the Associated Risk Factors in Schizophrenia. Turk. Psikiyatri. Derg. 2020, 32, 151. [Google Scholar] [CrossRef]
- Dias, T.L.; Schuch, V.; Beltrão-Braga, P.C.B.; Martins-De-Souza, D.; Brentani, H.P.; Franco, G.R.; Nakaya, H.I. Drug repositioning for psychiatric and neurological disorders through a network medicine approach. Transl. Psychiatry 2020, 10, 141. [Google Scholar] [CrossRef]
- Wang, Y.; Aldahdooh, J.; Hu, Y.; Yang, H.; Vähä-Koskela, M.; Tang, J.; Tanoli, Z. DrugRepo: A novel approach to repurposing drugs based on chemical and genomic features. Sci. Rep. 2022, 12, 21116. [Google Scholar] [CrossRef]
- Sadeghi, H.M.; Adeli, I.; Mousavi, T.; Daniali, M.; Nikfar, S.; Abdollahi, M. Drug Repurposing for the Management of Depression: Where Do We Stand Currently? Life 2021, 11, 774. [Google Scholar] [CrossRef] [PubMed]
- Fava, M. The promise and challenges of drug repurposing in psychiatry. World Psychiatry 2018, 17, 28–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.-M.; Kim, Y. Drug Repurposing Is a New Opportunity for Developing Drugs against Neuropsychiatric Disorders. Schizophr. Res. Treat. 2016, 2016, 6378137. [Google Scholar] [CrossRef] [Green Version]
- Crosby, N.; Deane, K.H.; Clarke, C.E. Amantadine in Parkinson’s disease. Cochrane Database Systemat. Rev. 2003, 1, CD003468. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef] [PubMed]
- Halladay, C.W.; Trikalinos, T.A.; Schmid, I.T.; Schmid, C.H.; Dahabreh, I.J. Using data sources beyond PubMed has a modest impact on the results of systematic reviews of therapeutic interventions. J. Clin. Epidemiol. 2015, 68, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, A.; Kannen, K.; Selaskowski, B.; Mehren, A.; Thöne, A.-K.; Pramme, L.; Blumenthal, N.; Li, M.; Asché, L.; Jonas, S.; et al. Virtual reality in the diagnostic and therapy for mental disorders: A systematic review. Clin. Psychol. Rev. 2022, 98, 102213. [Google Scholar] [CrossRef]
- Laan, W.; Grobbee, D.E.; Selten, J.-P.; Heijnen, C.J.; Kahn, R.S.; Burger, H. Adjuvant Aspirin Therapy Reduces Symptoms of Schizophrenia Spectrum Disorders: Results from a randomized, double-blind, placebo-controlled trial. J. Clin. Psychiatry 2010, 71, 520–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommer, E.I.; Gangadin, S.S.; de Witte, L.D.; Koops, S.; van Baal, C.; Bahn, S.; Drexhage, H.; Haren, N.E.M.V.; Veling, W.; Bruggeman, R.; et al. Simvastatin Augmentation for Patients with Early-Phase Schizophrenia-Spectrum Disorders: A Double-Blind, Randomized Placebo-Controlled Trial. Schizophr. Bull. 2021, 47, 1108–1115. [Google Scholar] [CrossRef]
- Shen, H.; Li, R.; Yan, R.; Zhou, X.; Feng, X.; Zhao, M.; Xiao, H. Adjunctive therapy with statins in schizophrenia patients: A meta-analysis and implications. Psychiatry Res. 2018, 262, 84–93. [Google Scholar] [CrossRef]
- Vincenzi, B.; Stock, S.; Borba, C.P.; Cleary, S.M.; Oppenheim, C.E.; Petruzzi, L.J.; Fan, X.; Copeland, P.M.; Freudenreich, O.; Cather, C.; et al. A randomized placebo-controlled pilot study of pravastatin as an adjunctive therapy in schizophrenia patients: Effect on inflammation, psychopathology, cognition and lipid metabolism. Schizophr. Res. 2014, 159, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanizadeh, A.; Rezaee, Z.; Dehbozorgi, S.; Berk, M.; Akhondzadeh, S. Lovastatin for the adjunctive treatment of schizophrenia: A preliminary randomized double-blind placebo-controlled trial. Psychiatry Res. 2014, 219, 431–435. [Google Scholar] [CrossRef]
- Tajik-Esmaeeli, S.; Moazen-Zadeh, E.; Abbasi, N.; Shariat, S.V.; Rezaei, F.; Salehi, B.; Akhondzadeh, S. Simvastatin adjunct therapy for negative symptoms of schizophrenia: A randomized double-blind placebo-controlled trial. Int. Clin. Psychopharmacol. 2017, 32, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, I.B.; Husain, N.; Drake, R.; Dunn, G.; Husain, M.O.; Kazmi, A.; Hamirani, M.M.; Rahman, R.; Stirling, J.; Deakin, W. Add-on clinical effects of simvastatin and ondansetron in patients with schizophrenia stabilized on antipsychotic treatment: Pilot study. Ther. Adv. Psychopharmacol. 2013, 4, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Sayyah, M.; Boostani, H.; Ashrafpoori, M.; Pakseresht, S. Effects of Atorvastatin on negative sign in chronic schizophrenia: A double blind clinical trial. Iran J. Pharm. Res. 2015, 14, 1269–1274. [Google Scholar] [CrossRef]
- Deakin, J.; Husain, N.; Parker, J.J. Efficacy of Ondansetron and Simvastatin on Cognition and Negative Symptoms in Established Schizophrenia. In Neuropsychopharmacology; The University of Manchester: Manchester, UK, 2014; Volume 39, pp. S355–S356. [Google Scholar]
- Berk, M.; Copolov, D.; Dean, O.; Lu, K.; Jeavons, S.; Schapkaitz, I.; Anderson-Hunt, M.; Judd, F.; Katz, F.; Katz, P.; et al. N-Acetyl Cysteine as a Glutathione Precursor for Schizophrenia—A Double-Blind, Randomized, Placebo-Controlled Trial. Biol. Psychiatry 2008, 64, 361–368. [Google Scholar] [CrossRef]
- Farokhnia, M.; Azarkolah, A.; Adinehfar, F.; Khodaie-Ardakani, M.-R.; Hosseini, S.-M.; Yekehtaz, H.; Tabrizi, M.; Rezaei, F.; Salehi, B.; Sadeghi, S.-M.; et al. N-Acetylcysteine as an Adjunct to Risperidone for Treatment of Negative Symptoms in Patients with Chronic Schizophrenia: A randomized, double-blind, placebo-controlled study. Clin. Neuropharmacol. 2013, 36, 185–192. [Google Scholar] [CrossRef]
- Sepehrmanesh, Z.; Heidary, M.; Akasheh, N.; Akbari, H.; Heidary, M. Therapeutic effect of adjunctive N-acetyl cysteine (NAC) on symptoms of chronic schizophrenia: A double-blind, randomized clinical trial. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 82, 289–296. [Google Scholar] [CrossRef]
- Iranpour, N.; Zandifar, A.; Farokhnia, M.; Goguol, A.; Yekehtaz, H.; Khodaie-Ardakani, M.-R.; Salehi, B.; Esalatmanesh, S.; Zeionoddini, A.; Mohammadinejad, P.; et al. The effects of pioglitazone adjuvant therapy on negative symptoms of patients with chronic schizophrenia: A double-blind and placebo-controlled trial. Hum. Psychopharmacol. 2016, 31, 103–112. [Google Scholar] [CrossRef]
- Çakici, N.; Van Beveren, N.J.M.; Judge-Hundal, G.; Koola, M.M.; Sommer, I.E.C. An update on the efficacy of anti-inflammatory agents for patients with schizophrenia: A meta-analysis. Psychol. Med. 2019, 49, 2307–2319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, J.; Riedel, A.; de Castella, A.; Fitzgerald, P.; Rolfe, T.; Taffe, J.; Burger, H. Estrogen—A potential treatment for schizophrenia. Schizophr. Res. 2001, 48, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, J.; de Castella, A.; Fitzgerald, P.B.; Gurvich, C.T.; Bailey, M.; Bartholomeusz, C.; Burger, H. Estrogen in Severe Mental Illness: A potential new treatment approach. Arch. Gen. Psychiatry 2008, 65, 955–960. [Google Scholar] [CrossRef]
- Kulkarni, J.; de Castella, A.; Headey, B.; Marston, N.; Sinclair, K.; Lee, S.J.; Gurvich, C.; Fitzgerald, P.B.; Burger, H. Estrogens and men with schizophrenia: Is there a case for adjunctive therapy? Schizophr. Res. 2011, 125, 278–283. [Google Scholar] [CrossRef]
- Akhondzadeh, S.; Nejatisafa, A.A.; Amini, H.; Mohammadi, M.R.; Larijani, B.; Kashani, L.; Raisi, F.; Kamalipour, A. Adjunctive estrogen treatment in women with chronic schizophrenia: A double-blind, randomized, and placebo-controlled trial. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2003, 27, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Louzã, M.R.; Marques, A.P.; Elkis, H.; Bassitt, D.; Diegoli, M.; Gattaz, W.F. Conjugated estrogens as adjuvant therapy in the treatment of acute schizophrenia: A double-blind study. Schizophr. Res. 2004, 66, 97–100. [Google Scholar] [CrossRef]
- Ghafari, E.; Fararouei, M.; Shirazi, H.G.; Farhangfar, A.; Ghaderi, F.; Mohammadi, A. Combination of Estrogen and Antipsychotics in the Treatment of Women with Chronic Schizophrenia: A double-blind, randomized, placebo-controlled clinical trial. Clin. Schizophr. Relat. Psychoses 2013, 6, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Kianimehr, G.; Fatehi, F.; Hashempoor, S.; Khodaei-Ardakani, M.-R.; Rezaei, F.; Nazari, A.; Kashani, L.; Akhondzadeh, S. Raloxifene adjunctive therapy for postmenopausal women suffering from chronic schizophrenia: A randomized double-blind and placebo controlled trial. DARU J. Pharm. Sci. 2014, 22, 55. [Google Scholar] [CrossRef]
- Khodaie-Ardakani, M.-R.; Khosravi, M.; Zarinfard, R.; Nejati, S.; Mohsenian, A.; Tabrizi, M.; Akhondzadeh, S. A Placebo-Controlled Study of Raloxifene Added to Risperidone in Men with Chronic Schizophrenia. Acta MEDICA Iran. 2015, 53, 337–345. [Google Scholar]
- Kulkarni, J.; Gavrilidis, E.; Gwini, S.M.; Worsley, R.; Grigg, J.; Warren, A.; Gurvich, C.; Gilbert, H.; Berk, M.; Davis, S.R. Effect of Adjunctive Raloxifene Therapy on Severity of Refractory Schizophrenia in Women: A Randomized Clinical Trial. JAMA Psychiatry 2016, 73, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Usall, J.; Huerta-Ramos, E.; Labad, J.; Cobo, J.; Núñez, C.; Creus, M.; Parés, G.G.; Cuadras, D.; Franco, J.; Miquel, E.; et al. Raloxifene as an Adjunctive Treatment for Postmenopausal Women with Schizophrenia: A 24-Week Double-Blind, Randomized, Parallel, Placebo-Controlled Trial. Schizophr. Bull. 2015, 42, 309–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiser, M.; Levi, L.; Burshtein, S.; Hagin, M.; Matei, V.; Podea, D.; Micluția, I.; Tiugan, A.; Păcală, B.; Grecu, I.G.; et al. Raloxifene Plus Antipsychotics Versus Placebo Plus Antipsychotics in Severely Ill Decompensated Postmenopausal Women with Schizophrenia or Schizoaffective Disorder: A Randomized Controlled Trial. J. Clin. Psychiatry 2017, 78, e758–e765. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Matsuda, Y.; Iwata, N. Memantine add-on to antipsychotic treatment for residual negative and cognitive symptoms of schizophrenia: A meta-analysis. Psychopharmacology 2017, 234, 2113–2125. [Google Scholar] [CrossRef] [PubMed]
- de Lucena, D.; Fernandes, B.S.; Berk, M.; Dodd, S.; Medeiros, D.W.; Pedrini, M.; Kunz, M.; Gomes, F.A.; Giglio, L.F.; Lobato, M.I.; et al. Improvement of Negative and Positive Symptoms in Treatment-Refractory Schizophrenia: A double-blind, randomized, placebo-controlled trial with memantine as add-on therapy to clozapine. J. Clin. Psychiatry 2009, 70, 1416–1423. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, A.J.; Papadakis, K.; Csernansky, J.; Litman, R.; Volavka, J.; Jia, X.D. MEM-MD-29 Study Group. A randomized, placebo-controlled study of memantine as adjunctive treatment in patients with schizophrenia. Neuropsychopharmacology 2008, 34, 1322–1329. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.G.; Lee, S.W.; Lee, B.J.; Park, S.W.; Kim, G.M.; Kim, Y.H. Adjunctive Memantine Therapy for Cognitive Impairment in Chronic Schizophrenia: A Placebo-Controlled Pilot Study. Psychiatry Investig. 2012, 9, 166–173. [Google Scholar] [CrossRef]
- Rezaei, F.; Mohammad-Karimi, M.; Seddighi, S.; Modabbernia, A.; Ashrafi, M.; Salehi, B.; Hammidi, S.; Motasami, H.; Hajiaghaee, R.; Tabrizi, M.; et al. Memantine Add-On to Risperidone for Treatment of Negative Symptoms in Patients with Stable Schizophrenia: Randomized, double-blind, placebo-controlled study. J. Clin. Psychopharmacol. 2013, 33, 336–342. [Google Scholar] [CrossRef]
- Omranifard, V.; Rajabi, F.; Mohammadian-Sichani, M.; Maracy, M.R. The effect of add-on memantine on global function and quality of life in schizophrenia: A randomized, double-blind, controlled, clinical trial. Adv. Biomed. Res. 2015, 4, 211. [Google Scholar] [CrossRef]
- Fakhri, A.; Pskseresht, S.; Haghdoost, M.R.; Hekmatkhah, N.; Torkashvand, M.; Ghorbanzadeh, B. Memantine Enhances the Effect of Olanzapine in Patients with Schizophrenia: A Randomized, Placebo-Controlled Study. Acta MEDICA Iran. 2016, 54, 696–703. [Google Scholar]
- Veerman, S.R.T.; Schulte, P.F.J.; Smith, J.D.; de Haan, L. Memantine augmentation in clozapine-refractory schizophrenia: A randomized, double-blind, placebo-controlled crossover study. Psychol. Med. 2016, 46, 1909–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazinani, R.; Nejati, S.; Khodaei, M. Effects of memantine added to risperidone on the symptoms of schizophrenia: A randomized double-blind, placebo-controlled clinical trial. Psychiatry Res. 2017, 247, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Cai, D.-B.; Zhang, Q.-E.; He, J.; Zhong, L.-Y.; Sim, K.; Ungvari, G.S.; Ning, Y.-P.; Xiang, Y.-T. Adjunctive ondansetron for schizophrenia: A systematic review and meta-analysis of randomized controlled trials. J. Psychiatr. Res. 2019, 113, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Akhondzadeh, S.; Mohammadi, N.; Noroozian, M.; Karamghadiri, N.; Ghoreishi, A.; Jamshidi, A.-H.; Forghani, S. Added ondansetron for stable schizophrenia: A double blind, placebo controlled trial. Schizophr. Res. 2009, 107, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, J.; Thomas, N.; Hudaib, A.-R.; Gavrilidis, E.; Gurvich, C. Ondansetron-a promising adjunctive treatment for persistent schizophrenia. J. Psychopharmacol. 2018, 32, 1204–1211. [Google Scholar] [CrossRef]
- Samadi, R.; Soluti, S.; Daneshmand, R.; Assari, S.; Manteghi, A.A. Efficacy of Risperidone Augmentation with Ondansetron in the Treatment of Negative and Depressive Symptoms in Schizophrenia: A Randomized Clinical Trial. Iran. J. Med. Sci. 2017, 42, 14–23. [Google Scholar]
- Zhang, Z.-J.; Kang, W.-H.; Li, Q.; Wang, X.-Y.; Yao, S.-M.; Ma, A.-Q. Beneficial effects of ondansetron as an adjunct to haloperidol for chronic, treatment-resistant schizophrenia: A double-blind, randomized, placebo-controlled study. Schizophr. Res. 2006, 88, 102–110. [Google Scholar] [CrossRef]
- Fan, X.; Song, X.; Zhao, M.; Jarskog, L.F.; Natarajan, R.; Shukair, N.; Freudenreich, O.; Henderson, D.C.; Goff, D.C. The effect of adjunctive telmisartan treatment on psychopathology and cognition in patients with schizophrenia. Acta Psychiatr. Scand. 2017, 136, 465–472. [Google Scholar] [CrossRef]
- Miller, B.J.; Buckley, P.; Seabolt, W.; Mellor, A.; Kirkpatrick, B. Meta-Analysis of Cytokine Alterations in Schizophrenia: Clinical Status and Antipsychotic Effects. Biol. Psychiatry 2011, 70, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nye, E.J.; Hockings, G.I.; Grice, J.E.; Torpy, D.J.; Walters, M.M.; Crosbie, G.V.; Wagenaar, M.; Cooper, M.; Jackson, R.V. Aspirin Inhibits Vasopressin-Induced Hypothalamic-Pituitary-Adrenal Activity in Normal Humans1. J. Clin. Endocrinol. Metab. 1997, 82, 812–817. [Google Scholar] [CrossRef] [Green Version]
- Vasović, V.; Banić, B.; JakovljeviĆ, V.; Tomic, Z.; Milic-Djordjevic, V. Effect of aminophylline on aspirin penetration into the central nervous system in rats. Eur. J. Drug Metab. Pharmacokinet. 2008, 33, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Schwieler, L.; Erhardt, S.; Engberg, G. Prostaglandin-mediated control of rat brain kynurenic acid synthesis–opposite actions by COX-1 and COX-2 isoforms. J. Neural Transm. 2004, 112, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.C.; Chan, J.K.N.; Wong, C.S.M.; Hai, J.S.H.; Or, P.C.F.; Chen, E. Mortality, Revascularization, and Cardioprotective Pharmacotherapy After Acute Coronary Syndrome in Patients with Psychotic Disorders: A Population-Based Cohort Study. Schizophr. Bull. 2020, 46, 774–784. [Google Scholar] [CrossRef]
- Postolache, T.T.; Medoff, D.R.; Brown, C.H.; Fang, L.J.; Upadhyaya, S.K.; Lowry, C.A.; Miller, M.; Kreyenbuhl, J.A. Lipophilic vs. hydrophilic statins and psychiatric hospitalizations and emergency room visits in US Veterans with schizophrenia and bipolar disorder. Pteridines 2021, 32, 48–69. [Google Scholar] [CrossRef]
- Rosendo, A.B.; Lima, L.O.; Pizzol, F.D.; Almeida, S. Lipid and C-Reactive Protein Levels, Cardiovascular Disease Risk Factors and Simvastatin Treatment in Brazilian Individuals. Inflammation 2010, 33, 244–250. [Google Scholar] [CrossRef]
- Li, X.-H.; Zhang, Y.-Y.; Wang, M.; Wang, D. Atorvastatin attenuates the production of IL-1β, IL-6, and TNF-α in the hippocampus of an amyloid β1-42-induced rat model of Alzheimer’s disease. Clin. Interv. Aging 2013, 8, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Palacio, J.R.; Markert, U.R.; Martínez, P. Anti-inflammatory properties of N-acetylcysteine on lipopolysaccharide-activated macrophages. Inflamm. Res. 2011, 60, 695–704. [Google Scholar] [CrossRef]
- Chesney, E.; Robson, D.; Patel, R.; Shetty, H.; Richardson, S.; Chang, C.-K.; McGuire, P.; McNeill, A. The impact of cigarette smoking on life expectancy in schizophrenia, schizoaffective disorder and bipolar affective disorder: An electronic case register cohort study. Schizophr. Res. 2021, 238, 29–35. [Google Scholar] [CrossRef]
- van der Weide, J.; Steijns, L.S.; van Weelden, M.J. The effect of smoking and cytochrome P450 CYP1A2 genetic polymorphism on clozapine clearance and dose requirement. Pharmacogenetics 2003, 13, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Froeliger, B.; McConnell, P.; Stankeviciute, N.; McClure, E.; Kalivas, P.; Gray, K. The effects of N -Acetylcysteine on frontostriatal resting-state functional connectivity, withdrawal symptoms and smoking abstinence: A double-blind, placebo-controlled fMRI pilot study. Drug Alcohol Depend. 2015, 156, 234–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, R.C.; Vargas, H.O.; Baracat, M.M.; Urbano, M.R.; Verri , W.A., Jr.; Porcu, M.; Nunes, S.O. N-acetylcysteine as an adjunctive treatment for smoking cessation: A randomized clinical trial. Rev. Bras. De Psiquiatr. 2020, 42, 519–526. [Google Scholar] [CrossRef]
- Nesti, L.; Tricò, D.; Mengozzi, A.; Natali, A. Rethinking pioglitazone as a cardioprotective agent: A new perspective on an overlooked drug. Cardiovasc. Diabetol. 2021, 20, 109. [Google Scholar] [CrossRef] [PubMed]
- Medina-Estrada, I.; Alva-Murillo, N.; López-Meza, J.E.; Ochoa-Zarzosa, A. Immunomodulatory Effects of 17β-Estradiol on Epithelial Cells during Bacterial Infections. J. Immunol. Res. 2018, 2018, 6098961. [Google Scholar] [CrossRef] [Green Version]
- Brand, A.B.; de Boer, J.N.; Dazzan, P.; Sommer, E.I. Towards better care for women with schizophrenia-spectrum disorders. Lancet Psychiatry 2022, 9, 330–336. [Google Scholar] [CrossRef]
- Rizzo, L.F.L.; Mana, D.L.; Serra, A.H.; Danilowicz, K. Hyperprolactinemia associated with psychiatric disorders. Medicina 2020, 80, 670–680. [Google Scholar]
- Bukhari, S.N.A. Consequences of Antipsychotic Medications on Mental Health. Curr. Drug Saf. 2021, 17, 285–293. [Google Scholar] [CrossRef]
- Redman, B.; Kitchen, C.; Johnson, K.W.; Bezwada, P.; Kelly, D.L. Levels of prolactin and testosterone and associated sexual dysfunction and breast abnormalities in men with schizophrenia treated with antipsychotic medications. J. Psychiatr. Res. 2021, 143, 50–53. [Google Scholar] [CrossRef]
- Hashemzadeh, M.; Haseefa, F.; Peyton, L.; Park, S.; Movahed, M.R. The effects of estrogen and hormone replacement therapy on platelet activity: A review. Am. J. Blood Res. 2022, 12, 33–42. [Google Scholar]
- Langer, R.D.; Hodis, H.N.; Lobo, R.A.; Allison, M.A. Hormone replacement therapy–where are we now? Climacteric 2021, 24, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Farkas, S.; Szabó, A.; Hegyi, A.E.; Török, B.; Fazekas, C.L.; Ernszt, D.; Kovács, T.; Zelena, D. Estradiol and Estrogen-like Alternative Therapies in Use: The Importance of the Selective and Non-Classical Actions. Biomedicines 2022, 10, 861. [Google Scholar] [CrossRef] [PubMed]
- Ruan, X.; Mueck, A.O. Impact of smoking on estrogenic efficacy. Climacteric 2014, 18, 38–46. [Google Scholar] [CrossRef]
- Beck, K.; Javitt, D.C.; Howes, O.D. Targeting glutamate to treat schizophrenia: Lessons from recent clinical studies. Psychopharmacology 2016, 233, 2425–2428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, S.; Miyake, N.; Jarskog, L.F.; Fleischhacker, W.W.; Lieberman, J. Pharmacological treatment of schizophrenia: A critical review of the pharmacology and clinical effects of current and future therapeutic agents. Mol. Psychiatry 2012, 17, 1206–1227. [Google Scholar] [CrossRef] [Green Version]
- Kishi, T.; Matsuda, Y.; Nakamura, H.; Iwata, N. Blonanserin for schizophrenia: Systematic review and meta-analysis of double-blind, randomized, controlled trials. J. Psychiatr. Res. 2013, 47, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Briskin, J.K.; Curtis, J.L. Augmentation of clozapine therapy with ondansetron. Am. J. Psychiatry 1997, 154, 1171. [Google Scholar] [CrossRef]
- White, A.; Corn, T.; Feetham, C.; Faulconbridge, C. Ondansetron in treatment of schizophrenia. Lancet 1991, 337, 1173. [Google Scholar] [CrossRef]
- Adler, L.E.; Cawthra, E.M.; Donovan, K.A.; Harris, J.G.; Nagamoto, H.T.; Olincy, A.; Waldo, M.C. Improved P50 Auditory Gating with Ondansetron in Medicated Schizophrenia Patients. Am. J. Psychiatry 2005, 162, 386–388. [Google Scholar] [CrossRef]
- Lintunen, J.; Lähteenvuo, M.; Tiihonen, J.; Tanskanen, A.; Taipale, H. Adenosine modulators and calcium channel blockers as add-on treatment for schizophrenia. Schizophrenia 2021, 7, 1. [Google Scholar] [CrossRef]
- Büki, A.; Kekesi, G.; Horvath, G.; Vécsei, L. A Potential Interface between the Kynurenine Pathway and Autonomic Imbalance in Schizophrenia. Int. J. Mol. Sci. 2021, 22, 10016. [Google Scholar] [CrossRef] [PubMed]
- Zakrocka, I.; Targowska-Duda, K.M.; Wnorowski, A.; Kocki, T.; Jóźwiak, K.; Turski, W.A. Angiotensin II Type 1 Receptor Blockers Inhibit KAT II Activity in the Brain—Its Possible Clinical Applications. Neurotox. Res. 2017, 32, 639–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kane, J.M.; Agid, O.; Baldwin, M.L.; Howes, O.; Lindenmayer, J.-P.; Marder, S.; Olfson, M.; Potkin, S.G.; Correll, C.U. Clinical Guidance on the Identification and Management of Treatment-Resistant Schizophrenia. J. Clin. Psychiatry 2019, 80, 2783. [Google Scholar] [CrossRef] [Green Version]
- Farr, O.M.; Sofopoulos, M.; Tsoukas, M.A.; Dincer, F.; Thakkar, B.; Sahin-Efe, A.; Filippaios, A.; Bowers, J.; Srnka, A.; Gavrieli, A.; et al. GLP-1 receptors exist in the parietal cortex, hypothalamus and medulla of human brains and the GLP-1 analogue liraglutide alters brain activity related to highly desirable food cues in individuals with diabetes: A crossover, randomised, placebo-controlled trial. Diabetologia 2016, 59, 954–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayfield, K.; Siskind, D.; Winckel, K.; Russell, A.W.; Kisely, S.; Smith, G.; Hollingworth, S. Glucagon-like peptide-1 agonists combating clozapine-associated obesity and diabetes. J. Psychopharmacol. 2016, 30, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Babic, I.; Gorak, A.; Engel, M.; Sellers, D.; Else, P.; Osborne, A.L.; Pai, N.; Huang, X.-F.; Nealon, J.; Weston-Green, K. Liraglutide prevents metabolic side-effects and improves recognition and working memory during antipsychotic treatment in rats. J. Psychopharmacol. 2018, 32, 578–590. [Google Scholar] [CrossRef] [Green Version]
- Parthsarathy, V.; Hölscher, C. The type 2 diabetes drug liraglutide reduces chronic inflammation induced by irradiation in the mouse brain. Eur. J. Pharmacol. 2013, 700, 42–50. [Google Scholar] [CrossRef]
- Wiciński, M.; Socha, M.; Malinowski, B.; Wódkiewicz, E.; Walczak, M.; Górski, K.; Słupski, M.; Pawlak-Osińska, K. Liraglutide and its Neuroprotective Properties—Focus on Possible Biochemical Mechanisms in Alzheimer’s Disease and Cerebral Ischemic Events. Int. J. Mol. Sci. 2019, 20, 1050. [Google Scholar] [CrossRef] [Green Version]
- Briyal, S.; Shah, S.; Gulati, A. Neuroprotective and anti-apoptotic effects of liraglutide in the rat brain following focal cerebral ischemia. Neuroscience 2014, 281, 269–281. [Google Scholar] [CrossRef]
- Larsen, J.R.; Vedtofte, L.; Jakobsen, M.S.L.; Jespersen, H.R.; Jakobsen, M.I.; Svensson, C.K.; Koyuncu, K.; Schjerning, O.; Oturai, P.S.; Kjaer, A.; et al. Effect of Liraglutide Treatment on Prediabetes and Overweight or Obesity in Clozapine- or Olanzapine-Treated Patients with Schizophrenia Spectrum Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2017, 74, 719–728. [Google Scholar] [CrossRef]
- Correll, C.U.; Solmi, M.; Croatto, G.; Schneider, L.K.; Rohani-Montez, S.C.; Fairley, L.; Smith, N.; Bitter, I.; Gorwood, P.; Taipale, H.; et al. Mortality in people with schizophrenia: A systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry 2022, 21, 248–271. [Google Scholar] [CrossRef] [PubMed]
- Zorn, J.V.; Schür, R.R.; Boks, M.P.; Kahn, R.S.; Joëls, M.; Vinkers, C.H. Cortisol stress reactivity across psychiatric disorders: A systematic review and meta-analysis. Psychoneuroendocrinology 2017, 77, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Rossom, R.C.; Hooker, S.A.; O’connor, P.J.; Crain, A.L.; Sperl-Hillen, J.M. Cardiovascular Risk for Patients with and Without Schizophrenia, Schizoaffective Disorder, or Bipolar Disorder. J. Am. Heart Assoc. 2022, 11, e021444. [Google Scholar] [CrossRef] [PubMed]
- Tek, C.; Kucukgoncu, S.; Guloksuz, S.; Woods, S.W.; Srihari, V.; Annamalai, A. Antipsychotic-Induced Weight Gain in First-Episode Psychosis Patients: A Meta-Analysis of Differential Effects of Antipsychotic Medications. Focus (Am. Psychiatr. Publ.) 2016, 14, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Bioque, M.; Llerena, A.; Cabrera, B.; Mezquida, G.; Lobo, A.; González-Pinto, A.; Díaz-Caneja, C.M.; Corripio, I.; Aguilar, E.J.; Bulbena, A.; et al. A Pharmacovigilance Study in First Episode of Psychosis: Psychopharmacological Interventions and Safety Profiles in the PEPs Project. Int. J. Neuropsychopharmacol. 2015, 19, pyv121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bret, P.; Bret, M.-C.; Queuille, E. Enquête de pratiques de prescription des antipsychotiques dans 13 centres hospitaliers du réseau PIC [Prescribing patterns of antipsychotics in 13 French psychiatric hospitals]. Encephale 2009, 35, 129–138. [Google Scholar] [CrossRef]
- Jaracz, J.; Tetera-Rudnicka, E.; Kujath, D.; Raczyńska, A.; Stoszek, S.; Czernaś, W.; Wierzbiński, P.; Moniakowski, A.; Jaracz, K.; Rybakowski, J. The prevalence of antipsychotic polypharmacy in schizophrenic patients discharged from psychiatric units in Poland. Pharmacol. Rep. 2014, 66, 613–617. [Google Scholar] [CrossRef]
- Hatta, K.; Hasegawa, H.; Imai, A.; Sudo, Y.; Morikawa, F.; Katayama, S.; Watanabe, H.; Ishizuka, T.; Nakamura, M.; Misawa, F.; et al. Real-world effectiveness of antipsychotic monotherapy and polytherapy in 1543 patients with acute-phase schizophrenia. Asian J. Psychiatry 2019, 40, 82–87. [Google Scholar] [CrossRef]
- Taipale, H.; Tanskanen, A.; Mehtälä, J.; Vattulainen, P.; Correll, C.U.; Tiihonen, J. 20-year follow-up study of physical morbidity and mortality in relationship to antipsychotic treatment in a nationwide cohort of 62,250 patients with schizophrenia (FIN20). World Psychiatry 2020, 19, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Tiihonen, J.; Mittendorfer-Rutz, E.; Majak, M.; Mehtälä, J.; Hoti, F.; Jedenius, E.; Enkusson, D.; Leval, A.; Sermon, J.; Tanskanen, A.; et al. Real-World Effectiveness of Antipsychotic Treatments in a Nationwide Cohort of 29 823 Patients with Schizophrenia. JAMA Psychiatry 2017, 74, 686–693. [Google Scholar] [CrossRef] [Green Version]
- Bartoli, F.; Cavaleri, D.; Bachi, B.; Moretti, F.; Riboldi, I.; Crocamo, C.; Carrà, G. Repurposed drugs as adjunctive treatments for mania and bipolar depression: A meta-review and critical appraisal of meta-analyses of randomized placebo-controlled trials. J. Psychiatr. Res. 2021, 143, 230–238. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | N (Type of the Study) | Intervention/Number of RCT | Results |
|---|---|---|---|
| Non-steroid anti-inflammatory drugs | |||
| Laan [22] | 70 (RCT) | Aspirin added to antipsychotic drugs for 3 months (1RCT) | Reduction of the severity of positive and negative symptoms and total PANSS scale 1.57 point; (95% CI 0.06 ÷ 3.07), p = 0.018. No influence on the efficiency of cognitive functions. |
| Other anti-inflammatory drugs | |||
| Sommer [23] | 61(RCT) | Simvastatin was added to antipsychotic drugs for 24 months in patients with schizophrenia spectrum disease diagnosed less than 3 years (1RCT) | No significant differences in the severity of psychopathological symptoms after 12 months, however, a significant reduction in the severity after 6 and 24 months (p = 0.02 and p = 0.04, respectively); no effect on the cognitive functions, performing daily activities of living, and the severity of depression symptoms. |
| Shen [24] * | 339 (M) | RCTs with the use of different statins (6 RCTs) | Significant reduction of positive symptoms of the PANSS scale in the group receiving statins compared to the placebo: SMD = 0.31 (95% CI: 0.01 ÷ 0.62; p = 0.05, n = 168); reduction of negative symptoms of the PANSS scale: SMD = 0.31 (95% CI: 0.1 ÷ 0.53; p = 0.004, n = 339). In patients receiving simvastatin, the reduction of the total PANSS score: SMD = 0.42 (95% CI: −0.01 ÷ 0.84; p = 0.05, n = 89) and the severity of negative symptoms of the PANSS scale: SMD = 0.40 (95 % CI: 0.14 ÷ 0.67; p = 0.03, n = 220). |
| Vincenzi [25] | 24 | Pravastatin added to antipsychotic drugs for 6 to 12 weeks | Significant reduction in positive symptoms of the PANSS scale at 6 weeks from baseline (p = 0.01), but it failed to remain after 12 weeks from baseline (p = 0.12). |
| Ghanizadeh [26] | 36 | Lovastatin added to risperidone or placebo for 8 weeks | Reduction of the PANSS total score after 8 weeks of treatment in patients receiving risperidone and lovastatin, but without statistical significance. |
| Tajik-Esmaeeli [27] | 33 | Simvastatin added to risperidone or placebo for 8 weeks | In patients receiving simvastatin, a significant reduction in negative symptom scores from baseline to week 8 (p = 0.003) and in total scores (p = 0.001). Results were not significant for positive symptoms or general psychopathology scores. |
| Chaudhry [28] | 108 | Simvastatin added to antipsychotic medication for 12 weeks | Reduction in total symptoms of schizophrenia, especially in positive and general symptoms, rather than negative symptoms. |
| Sayyah [29] | 40 | Atorvastatin added to risperidone or placebo for 6 weeks | No significant changes in schizophrenia symptoms. |
| Deakin [30] | 98 | Simvastatin added to antipsychotic medication for up to 6 months | Combination of simvastatin with risperidone caused a significant reduction of the negative syndrome of schizophrenia while such an effect was not observed when simvastatin was added to other antipsychotic drugs. |
| Antioxidants | |||
| Berk [31] | 40 (RCT) | N-Acetylcysteine added to SGA for 24 weeks (1RCT) | Significant reductions of the score on the PANSS positive subscale [md −5.97 (95% CI: −10.44; −1.51), p = 0.009], PANSS negative subscale [md −1.83 (95% CI: −3.33; −0.32), p = 0.018] and PANSS general subscale [md −2.79 (95% CI: −5.38; −0.20), p = 0.035]. Improvement in akathisia intensity observed (p = 0.022). |
| Farokhnia [32] | 42 (RCT) | N-Acetylcysteine added to risperidone for 8 weeks (1 RCT) | Improvement on the PANSS general subscale (p = 0.006) and on the PANSS general subscale (p < 0.001) in the intervention group. No side effects of NACC addition. |
| Sepehrmanesh [33] | 42 (RCT) | N-Acetylcysteine added to first-generation antipsychotic for 12 weeks (1RCT) | Reduction in the positive (F = 5.47, p = 0.02) and negative (F = 0.20, df = 1) PANSS subscale scores. No significant difference in the frequency of adverse effects. |
| PPARγ agonists | |||
| Iranpour [34] | 40 (RCT) | Pioglitazone added to risperidone treatment for 8 weeks (1RCT) | Improvement in the severity of positive and negative symptoms (p < 0.001). |
| Neuroprotective drugs | |||
| Çakici [35] * | 368 (M) | Estrogens added to antipsychotic drugs for 28 days up to 8 weeks: 4 RCTs in women and 2RCTs in men | Significant reduction of positive and negative symptoms of schizophrenia on the PANSS scale (p < 0.0005) compared to the control group of both sexes; general improvement in functioning as measured by the Comprehensive Psychopathological Rating Scale (p < 0.0005); effect size value = 0.57. |
| Kulkarni [36] | 36 | Estrogens added to antipsychotic treatment for 28 days | Significant improvement on the PANSS positive, negative, and general subscale (p < 0.001) was caused by estradiol (100 mdg-patch) in patients receiving antipsychotic medication versus the placebo group. Additionally, estrogen significantly enhanced treatment of acute, severe psychotic symptoms. |
| Kulkarni [37] | 56 | Estradiol transdermal added to antipsychotic drugs for 28 days | Transdermal estradiol significantly reduced positive (p < 0.005) and general psychopathological symptoms of schizophrenia (p < 0.005) compared with women receiving only antipsychotic treatment. |
| Kulkarni [38] | 53 | Estradiol 2 mg, orally added to antipsychotic drugs for 14 days | Significant improvement on the PANSS positive, negative, total, and general scales (p < 0.0047) in men receiving additionally, orally 2 mg of estradiol in comparison to the placebo group. |
| Akhondzadeh [39] | 32 | Estradiol added to haloperidol for 8 weeks | Estradiol added to haloperidol decreased significantly the score of the PANSS positive, negative, and general psychopathological symptoms of schizophrenia (p < 0.001) versus the placebo group. |
| Louzã [40] | 44 | Conjugated estradiol added to haloperidol for 28 days | Both the conjugated estrogen group and the placebo group showed a similar improvement on the BPRS total score scale (p < 0.001). |
| Ghafari [41] | 32 | Conjugated estradiol added to antipsychotic treatment for 4 weeks | Significant decrease in positive (p = 0.003), negative (p < 0.001), general (p < 0.001), and total (p < 0.001) PANSS scores over 4 weeks in patients receiving a combination of medication versus the control group. |
| Çakici [35] * | 205 (M) | Raloxifene added to antipsychotic drugs for 8 to 24 weeks (5 RTCs) | Improvement in the functioning of patients as measured by the Comprehensive Psychopathological Rating Scale: p < 0.002; Reduction of the severity of positive and negative symptoms on the PANSS scale (p = 0.027) positively correlated with the time of drug use; effect size value = 0.52. |
| Kianimehr [42] | 23 | Raloxifene added to risperidone treatment for 8 weeks | Improvement of positive symptoms on the PANSS scale (p < 0.001) and not a significant change of negative and general psychopathology symptoms in women treated with medication versus the placebo. |
| Khodaie-Ardakani [43] | 23 | Raloxifene added to risperidone treatment for 8 weeks | The raloxifene group showed significantly greater improvement on the negative subscale (p < 0.001), the general psychopathology subscale (p = 0.002), and total PANSS score (p < 0.001) in comparison to the placebo group. |
| Kulkarni [44] | 26 | Raloxifene added to antipsychotic treatment for 12 weeks | Significant reduction in the PANSS general symptom scores for the raloxifene compared with the placebo (β = −3.72; 95%CI, −6.83 to −0.61; p = 0.02) groups. Results were not significant for positive and negative symptoms. |
| Usall [45] | 33 | Raloxifene added to antipsychotic treatment for 24 weeks | Significant reduction of negative (p = 0.027), general symptoms (p = 0.003), and total symptomatology (p = 0.005) measured with the PANSS in women receiving treatment versus the placebo. |
| Weiser [46] | 100 | Raloxifene added to antipsychotic treatment for 16 weeks | No reduction of the severity of positive and negative symptoms and total PANSS scale in severely ill decompensated women treated with a combination of drugs. |
| NMDA antagonists | |||
| Kishi [47] * | 448 (M) | Memantine added to antipsychotic drugs for 6–26 weeks (8 RCTs) | Statistically significant reduction of the severity of negative symptoms on the PANSS scale (p = 0.002), especially in younger adult patients, and improvement in the performance of the MMSE test (p < 0.0001); insignificant reduction of the severity of positive (p = 0.07) and general symptoms on the PANSS scale (p = 0.06) and the severity of depression symptoms (p = 0.326). |
| Lucena [48] | 10 | Memantine added to clozapine for 12 weeks | Significant improvement (p < 0.01) in the total BPRS score, its subscales of positive (effect size [ES] = −1.38) and negative (ES = −3.33) symptoms, the CGI score (ES = 1.56), and the MMSE score was observed with memantine as compared with the placebo. |
| Lieberman [49] | 70 | Memantine added to atypical antipsychotic drugs for 8 weeks | No significant differences in the severity of schizophrenia symptoms after 8 weeks in patients treated with a combination of drugs versus the placebo. Higher incidence of adverse effects than the placebo. |
| Lee [50] | 26 | Memantine added to typical antipsychotic drugs for 12 weeks | Insignificant reduction of the severity of negative symptoms (p < 0.12); no improvement of cognitive functions and depressive symptoms. |
| Rezaei [51] | 40 | Memantine added to risperidone for 8 weeks | A significantly greater improvement on the negative PANSS subscale, the total score (p < 0.001), and the general psychopathology subscale score (p = 0.002) than the placebo group; no significant difference in the reduction of positive symptoms score between the two groups (p = 0.757). |
| Omranifard [52] | 32 | Memantine added to risperidone for 12 weeks | Improvement in the functioning of the intervention group patients was measured using the GAF and QLS scales (p < 0.001) versus the placebo. |
| Fakhri [53] | 30 | Memantine added to olanzapine for 6 weeks | Significantly improved the positive and negative PANSS score in patients treated with a combination of drugs (p < 0.001) versus olanzapine alone; female patients showed significantly better response than males, especially in positive PANSS score. No significant changes in extrapyramidal symptoms. |
| Veerman [54] | 26 | Memantine added to clozapine for 26 weeks | Improvement on the PANSS negative subscale score (effect size = 0.29); improved a composite memory score comprising verbal recognition memory and paired associates learning task scores on the CANTAB (effect size = 0.30) in patients with adjunctive therapy versus the placebo. |
| Mazinani [55] | 23 | Memantine added to risperidone for 12 weeks | Significant improvement of negative symptoms on the PANSS scale (p < 0.001) and cognitive functions; no significant differences between positive and psychopathologic symptoms in the intervention group of patients. |
| Serotonergic drugs | |||
| Zheng [56] * | 184 (M) | Ondansetron added to antipsychotic drugs for 12 weeks (5 RCTs) | Reduction of the severity of negative and general symptoms of schizophrenia (no effect on the severity of positive symptoms): standardized mean difference of the total PANSS score: −0.51. |
| Akhondzadeh [57] | 30 | Ondansetron added to risperidone for 12 weeks | The ondansetron group had significantly greater improvement in the negative symptoms, general psychopathological symptoms, and PANSS total scores (p < 0.001). |
| Chaudhry [28] | 36 | Ondansetron added to antipsychotic treatment for 12 weeks | Reduction of schizophrenia symptoms on PANSS total score versus antipsychotic treatment only, but without statistical significance. |
| Kulkarni [58] | 42 | Ondansetron added to atypical antipsychotic drugs for 12 weeks | Ondansetron caused significant improvement both in the cognitive domain (p < 0.05) as measured by the Positive and Negative Syndrome Scale and on Total Positive and Negative Syndrome Scale (p = 0.06). |
| Samadi [59] | 18 | Ondansetron added to risperidone for 12 weeks | Significantly larger improvement in the PANSS overall scale and subscales for negative symptoms and cognition (p < 0.001) in patients treated with adjunctive therapy, but without influence on depressive symptoms. |
| Zhang [60] | 58 | Ondansetron added to haloperidol for 12 weeks | Significantly greater improvement on PANSS overall scale and subscales for negative symptoms, general psychopathology, and cognition (p < 0.05) in patients treated with adjunctive therapy. |
| Other drugs | |||
| Fan [61] | 43 (RCT) | Telmisartan added to clozapine or olanzapine at a dose for 12 weeks (1RCT) | Significant decrease in the PANSS total score compared to the placebo group (p = 0.038). No differences between groups in the score on the positive PANSS subscale: p = 0.105 (d = 0.39) and on the negative PANSS subscale: p = 0.422 (d = 0.18). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dróżdż, W.; Wiciński, M.; Szota, A.M.; Szambelan, M.; Radajewska, I.; Popławski, I.; Wojciechowski, P. Augmentation Therapies as Treatments for Coexisting Somatic Problems in Schizophrenia—A Systematic Review. J. Clin. Med. 2023, 12, 4012. https://doi.org/10.3390/jcm12124012
Dróżdż W, Wiciński M, Szota AM, Szambelan M, Radajewska I, Popławski I, Wojciechowski P. Augmentation Therapies as Treatments for Coexisting Somatic Problems in Schizophrenia—A Systematic Review. Journal of Clinical Medicine. 2023; 12(12):4012. https://doi.org/10.3390/jcm12124012
Chicago/Turabian StyleDróżdż, Wiktor, Michał Wiciński, Anna Maria Szota, Monika Szambelan, Izabela Radajewska, Igor Popławski, and Paweł Wojciechowski. 2023. "Augmentation Therapies as Treatments for Coexisting Somatic Problems in Schizophrenia—A Systematic Review" Journal of Clinical Medicine 12, no. 12: 4012. https://doi.org/10.3390/jcm12124012
APA StyleDróżdż, W., Wiciński, M., Szota, A. M., Szambelan, M., Radajewska, I., Popławski, I., & Wojciechowski, P. (2023). Augmentation Therapies as Treatments for Coexisting Somatic Problems in Schizophrenia—A Systematic Review. Journal of Clinical Medicine, 12(12), 4012. https://doi.org/10.3390/jcm12124012