A Comprehensive Summary of the Current Understanding of the Relationship between Severe Obesity, Metabolic Syndrome, and Inflammatory Status

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
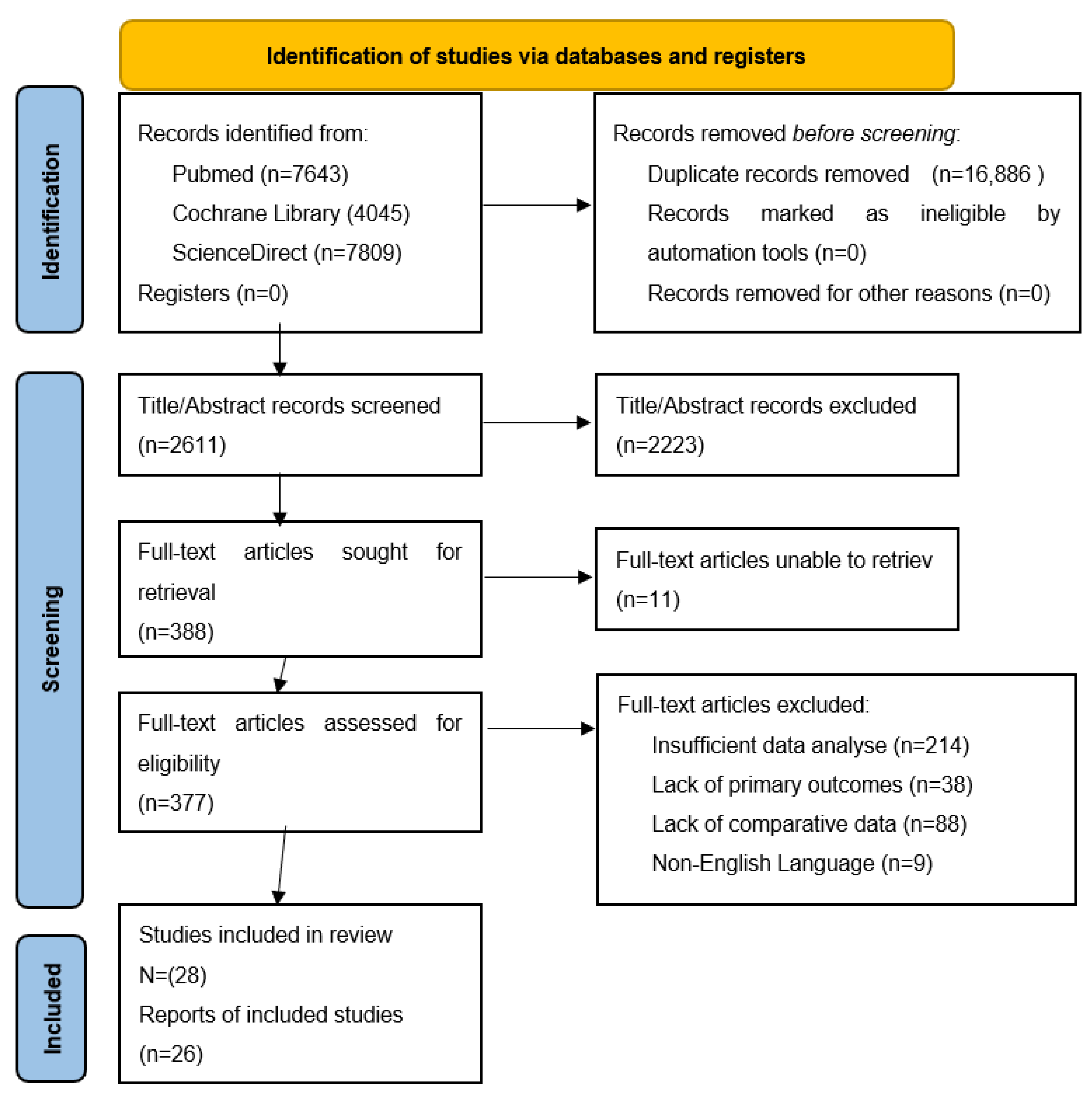
2.1. Search Strategy
2.2. Outcome Measures
3. Metabolic Syndrome Exacerbates Comorbidities
- Grade 1 obesity (commonly referred to as overweight): a BMI between 25 and 29.9 kg/m2;
- Grade 2 obesity (called obesity): a BMI between 30 and 39.9 kg/m2;
4. Inflammation in Obesity: The Link Mechanism and the Complications
5. Correlations between Obesity and Metabolic Syndrome
6. Correlations between Obesity and Inflammatory Induced Comorbidities
6.1. Inflammation in Heart Failure
6.2. Glutamine Metabolism
7. Correlations between Obesity and Pro-Inflammatory Status
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO Regional Office for Europe. Available online: https://www.who.int/europe/publications/i/item/9789289057738 (accessed on 27 June 2022).
- Vasheghani, M.; Hessami, Z.; Rekabi, M.; Abedini, A.; Qanavati, A. Evaluating Possible Mechanisms Linking Obesity to COVID-19: A Narrative Review. Obes. Surg. 2022, 32, 1689–1700. [Google Scholar] [CrossRef] [PubMed]
- Triposkiadis, F.; Xanthopoulos, A.; Starling, R.C.; Iliodromitis, E. Obesity, inflammation, and heart failure: Links and misconceptions. Heart Fail. Rev. 2022, 27, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Liu, J.; Zhang, Z.; Zhang, H.; Wang, N.; Chen, X.; Han, X.; Lu, Q.; Chi, S. Effects of Dietary Intervention on Inflammatory Markers in Metabolic Syndrome: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 846591. [Google Scholar] [CrossRef]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimized digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef]
- Lam, D.W.; LeRoith, D. Metabolic Syndrome. In Comprehensive Free Online Endocrinology Book; NCBI: Bethesda, MD, USA, 2019; Available online: www.endotext.org (accessed on 27 June 2022).
- Nilsson, P.M.; Tuomilehto, J.; Ryden, L. The metabolic syndrome—What is it and how should it be managed? Eur. J. Prev. Cardiol. 2019, 26, 33–46. [Google Scholar] [CrossRef]
- Barati, E.; Ghazizadeh, H.; Sadabadi, F.; Kazemi, E.; Ferns, G.A.; Avan, A.; Ghayour-Mobarhan, M. Association of the IL6 Gene Polymorphism with Component Features of Metabolic Syndrome in Obese Subjects. Biochem. Genet. 2019, 57, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, O.; Uwaifo, G.I.; Oral, E.A. Obesity. Medscape, 9 June 2021. [Google Scholar]
- Gârgavu, S.R.; Clenciu, D.; Roșu, M.M.; Țenea Cojan, T.Ș.; Costache, A.; Vladu, I.M.; Moța, M. Visceral adiposity index (vai)—A potential marker of cardiometabolic risk. Arch. Balk. Med. Union 2018, 53, 246–251. [Google Scholar] [CrossRef]
- Jameson, J.L. Harrison’s Endocrinology, 3rd ed.; McGraw Hill: New York, NY, USA, 2013. [Google Scholar]
- Eley, V.A.; Thuzar, M.; Navarro, S.; Dodd, B.R.; Zundert, A.A.V. Obesity, metabolic syndrome, and inflammation: An update for anaesthetists caring for patients with obesity. Anaesth. Crit. Care Pain Med. 2021, 40, 100947. [Google Scholar] [CrossRef]
- Kaisanlahti, A.; Glumoff, T. Browning of white fat: Agents and implications for beige adipose tissue to type 2 diabetes. J. Physiol. Biochem. 2019, 75, 1–10. [Google Scholar] [CrossRef]
- Lidell, M.E.; Betz, M.J.; Enerbäck, S. Brown adipose tissue and its therapeutic potential. J. Intern. Med. 2014, 276, 364–377. [Google Scholar] [CrossRef]
- Cheng, L.; Wang, J.; Dai, H.; Duan, Y.; An, Y.; Shi, L.; Lv, Y.; Li, H.; Wang, C.; Ma, Q.; et al. Brown and beige adipose tissue: A novel therapeutic strategy for obesity and type 2 diabetes mellitus, National Library of Medicine. Adipocyte 2021, 10, 48–65. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, E.J.; LeRoith, D.; Karnieli, E. The Metabolic Syndrome—From Insulin Resistance to Obesity and Diabetes. Med. Clin. N. Am. 2011, 95, 855–873. [Google Scholar] [CrossRef]
- Dieny, F.F.; Tsani, A.F.A.; Suryawati, S. Visceral Adiposity Index and Lipid Accumulation Product Related to Insulin Resistance and Metabolic Syndrome in Obese College Students. Open Access Maced. J. Med. Sci. 2022, 10, 667–673. [Google Scholar] [CrossRef]
- Ibrahim, Q.; Ahsan, M. Measurement of Visceral Fat, Abdominal Circumference and Waist-hip Ratio to Predict Health Risk in Males and Females. Pak. J. Biol. Sci. 2019, 22, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, E.; López-Sobaler, A.M.; Ortega, R.M.; Delgado-Losada, M.L.; López-Parra, A.M.; Aparicio, A. Association between Neutrophil-to-Lymphocyte Ratio with Abdominal Obesity and Healthy Eating Index in a Representative Older Spanish Population. Nutrients 2020, 12, 855. [Google Scholar] [CrossRef]
- Russo, L.; Muir, L.; Geletka, L.; Delproposto, J.; Baker, N.; Flesher, C.; O’Rourke, R.; Lumeng, C.N. Cholesterol 25-hydroxylase (CH25H) as a promoter of adipose tissue inflammation in obesity and diabetes. Mol. Metab. 2020, 39, 100983. [Google Scholar] [CrossRef]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Myśliwiec, H.; Choromańska, K.; Dadan, J.; Żendzian-Piotrowska, M.; Zalewska, A.; Maciejczyk, M. Bariatric Surgery Normalizes Protein Glycoxidation and Nitrosative Stress in Morbidly Obese Patients. Antioxidants 2020, 9, 1087. [Google Scholar] [CrossRef]
- Cӑtoi, A.F.; Pârvu, A.E.; Mironiuc, A.; Chiorescu, Ş.; Crӑciun, A.; Pop, I.D.; Cӑtoi, C. Chemerin, Inflammatory, and Nitrooxidative Stress Marker Changes Six Months after Sleeve Gastrectomy. Oxidative Med. Cell. Longev. 2018, 2018, 1583212. [Google Scholar] [CrossRef]
- Min, T.; Prior, S.L.; Dunseath, G.; Churm, R.; Barry, J.D.; Stephens, J.W. Temporal Effects of Bariatric Surgery on Adipokines, Inflammation and Oxidative Stress in Subjects with Impaired Glucose Homeostasis at 4 Years of Follow-up. Obes. Surg. 2020, 30, 1712–1718. [Google Scholar] [CrossRef]
- Aratani, Y. Myeloperoxidase: Its role for host defense, inflammation, and neutrophil function. Arch. Biochem. Biophys. 2018, 640, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Adiels, M.; Olofsson, S.-O.; Taskinen, M.-R.; Bore, J. Overproduction of Very Low–Density Lipoproteins Is the Hallmark of the Dyslipidemia in the Metabolic Syndrome. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1225–1236. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shields, G.S.; Guo, C.; Liu, Y. Executive function performance in obesity and overweight individuals: A meta-analysis and review. Neurosci. Biobehav. Rev. 2018, 84, 225–244. [Google Scholar] [CrossRef]
- Russo, L.; Lumeng, C.N. Properties and functions of adipose tissue macrophages in obesity. Immunology 2018, 155, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Gold, E.S.; Diercks, A.H.; Podolsky, I.; Podyminogin, R.L.; Askovich, P.S.; Treuting, P.M.; Aderem, A. 25-Hydroxycholesterol acts as an amplifier of inflammatory signaling. Proc. Natl. Acad. Sci. USA 2014, 111, 10666–10671. [Google Scholar] [CrossRef]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Dadan, J.; Myśliwiec, H.; Choromańska, K.; Zalewska, A.; Maciejczyk, M. A Longitudinal Study of the Antioxidant Barrier and Oxidative Stress in Morbidly Obese Patients after Bariatric Surgery. Does the Metabolic Syndrome Affect the Redox Homeostasis of Obese People? J. Clin. Med. 2020, 9, 976. [Google Scholar] [CrossRef]
- Cho, K.W.; Zamarron, B.F.; Muir, L.A.; Singer, K.; Porsche, C.E.; DelProposto, J.B.; Geletka, L.; Meyer, K.A.; O’Rourke, R.W.; Lumeng, C.N. Adipose Tissue Dendritic Cells Are Independent Contributors to Obesity-Induced Inflammation and Insulin Resistance. J. Immunol. 2016, 197, 3650–3661. [Google Scholar] [CrossRef]
- Cӑtoi, A.F.; Pârvu, A.E.; Andreicuț, A.D.; Mironiuc, A.; Crӑciun, A.; Cӑtoi, C.; Pop, I.D. Metabolically Healthy versus Unhealthy Morbidly Obese: Chronic Inflammation, Nitro-Oxidative Stress, and Insulin Resistance. Nutrients 2018, 10, 1199. [Google Scholar] [CrossRef]
- Freitas, W.R.; Oliveira, L.V.F.; Perez, E.A.; Ilias, E.J.; Lottenberg, C.P.; Silva, A.S.; Urbano, J.J.; Oliveira, M.C.; Vieira, R.P.; Ribeiro-Alves, M.; et al. Systemic Inflammation in Severe Obese Patients Undergoing Surgery for Obesity and Weight-Related Diseases. Obes. Surg. 2018, 28, 1931–1942. [Google Scholar] [CrossRef]
- Stephens, J.W.; Min, T.; Dunseath, G.; Churm, R.; Barry, J.D.; Prior, S.L. Temporal effects of laparoscopic sleeve gastrectomy on adipokines, inflammation, and oxidative stress in patients with impaired glucose homeostasis. Surg. Obes. Relat. Dis. 2019, 15, 2011–2017. [Google Scholar] [CrossRef]
- Saleh, Z.T.; Lennie, T.A.; Darawad, M.; Alduraidi, H.; Elshatarat, R.A.; Almansour, I.M.; Moser, D.K. The health outcomes of inflammation and obesity in patients with heart failure. Heart Lung 2020, 49, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Farkhondeh, T.; Llorens, S.; Pourbagher-Shahri, A.M.; Ashrafizadeh, M.; Talebi, M.; Shakibaei, M.; Samarghandian, S. An Overview of the Role of Adipokines in Cardiometabolic Diseases. Molecules 2020, 25, 5218. [Google Scholar] [CrossRef] [PubMed]
- Petrus, P.; Lecoutre, S.; Dollet, L.; Wiel, C.; Sulen, A.; Gao, H.; Tavira, B.; Laurencikiene, J.; Rooyackers, O.; Checa, A.; et al. Glutamine Links Obesity to Inflammation in Human White Adipose Tissue. Cell Metab. 2020, 31, 375–390.e11. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, K.; Devarajan, N.; Ganesan, M.; Ragunathan, M. Obesity, Inflammation and Acute Myocardial Infarction—Expression of leptin, IL-6 and high sensitivity-CRP in Chennai based population. Thromb. J. 2012, 10, 13. [Google Scholar] [CrossRef]
- Popko, K.; Gorska, E.; Stelmaszczyk-Emmel, A.; Plywaczewski, R.; Stoklosa, A.; Gorecka, D.; Pyrzak, B.; Demkow, U. Proinflammatory cytokines IL-6 and TNF-α and the development of inflammation in obese subjects. Eur. J. Med. Res. 2010, 15, 120. [Google Scholar] [CrossRef]
- Beresescu, G.; Sala, D.T.; Ion, R.M.; Tegla, E.; Balmos, A.; Cosarca, A.; Ormenisan, A. Relationship Between Obesity and Periodontal Disease after Minimally Invasive Sleeve Gastrostomy. Rev. Chim. 2019, 70, 3258–3266. [Google Scholar] [CrossRef]
- Phillips, C.L.; Grayson, B.E. The immune remodel: Weight loss-mediated inflammatory changes to obesity. Exp. Biol. Med. 2020, 245, 109–121. [Google Scholar] [CrossRef]
- Youssef, E.M.; Elfiky, A.M.; Abu-Shahba, N. and Elhefnawi, M.M. Expression profiling and analysis of some miRNAs in subcutaneous white adipose tissue during development of obesity. Genes Nutr. 2020, 15, 8. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Duration (y) | Study Type | Gender | Number of Patients | Study Groups (Average Age) | Objectives | Analyzed Markers | Indicator of MetSyn |
|---|---|---|---|---|---|---|---|---|
| Ibrahim et al. [19] | 2017–2018 (2) | Cross-sectional analytical study | Men—240 Women—240 | 159 | Men (19.17 ± 2.54) Women (18.96 ± 1.18) | Association between selected variables and health risk | BMI, WC, HC, VCA, AC, WHR, VAT | |
| Rodriguez-Rodriguez et al. [20] | 2011 (1) | Observational and cross-sectional study | Men—771 Women—976 | 1747 | Men (65.49 ± 10.45) Women (66.79 ± 10.76) | Association between selected variables and inflammatory state | BMI, WC, HC, WHtR, WHR, | Neutrophils-Lymphocytes(NLR), Inflammation status, Body Fat |
| Russo et al. [21] | 2018 (1) | Cross-sectional study | Men—50 Women—50 | 100 | 50% DM (40.4 ± 11.8) 50% non-DM (46.6 ± 11.0) | Role of CH25H in metabolic inflammation | BMI, WC, HC | HbA1C and HOMA-IR, Cholesterol 25-Hydroxylase (CH25H); 25-Hydroxycholesterol (25-HC), |
| Choromansk et al. [22] | 2012–2018 (7) | Cross-sectional study | Women—65 | 65 | 34—OB (39) 31—OB + MetS (49) | Insulin resistance and lipid profile markers | BMI, WC, HC, WHR, | LIPID PROFILE(HDL, TG, LDL, CHOLESTEROL), CRP, ALT, AST, WBC, RBC, HGB, PLT, GLUCOSE, INSULIN, HOMA-IR, Risk of T2DM and HTA |
| Catoi el al. [23] | 2014–2016 (3) 2009–2015 (7) | Prospective study | Male—8 Women—16 | 24 72 | (Control- 36.38 ± 6.3; MO- 42.15 ± 6.86) (MHMO-40.4 ± 9.0; MUHMO- 43.3 ± 10.03) | Insulin resistance and lipid profile markers | BMI, TC, HDL-C, TG, EBMIL, | HOMA-IR, hs-CRP, Chemerin, TNF-alpha, |
| Min et al. [24] | 4 years follow-up | Prospective study | Male—6 Women—13 | 19 | 4 groups: Pre-operatively, 1 and 6 months, and 4 years Mean age (50.4 ± 6.2) | Biochemical changes in obesity-related inflammatory status at 1 and 6 months, as well as 4 years after BS | BMI, EWL, SBP, DBP, TC, | Adiponectin, leptin, CRP, Il-6, Il-10, HbA1C, lipid profile(LDL, HDL, TG), Fasting C-peptide, Insulin, HOMA-IR |
| Ibrahim et al. [19] | Men | Women | Both | |||||
|---|---|---|---|---|---|---|---|---|
| Age | 19.17 ± 2.54 | 18.96 ± 1.18 | 19.07 ± 1.99 | |||||
| Height | 167.57 ± 8.38 | 157.22 ± 5.27 | 162.40 ± 8.71 | |||||
| Weight | 76.888 ± 27.89 | 56.52 ± 12.26 | 66.70 ± 23.81 | |||||
| BMI | 76.888 ± 27.89 | 22.86 ± 4.81 | 24.98 ± 7.32 | |||||
| VCA | 103.738 ± 72.26 | 55.95 ± 32.63 | 79.84 ± 60.89 | |||||
| AC | 93.89 ± 22.17 | 76.29 ± 8.97 | 85.09 ± 19.05 | |||||
| WHR | 93.89 ± 22.17 | 76.29 ± 8.97 | 0.87 ± 0.98 | |||||
| Rodriguez-Rodriguez et al. [20] | Men (n = 771) | Women (n = 976) | p value | |||||
| BMI (kg/m2) | 28.55 ± 4.07 | 28.20 ± 4.98 | p < 0.05 | |||||
| WC (cm) | 100.67 ± 10.42 | 94.79 ± 12.75 | p < 0.001 | |||||
| WHtR | 0.60 ± 0.06 | 0.61 ± 0.09 | p < 0.01 | |||||
| WHR | 0.97 ± 0.07 | 0.91 ± 0.08 | p < 0.001 | |||||
| Body Fat (%) | 30.63 ± 6.16 | 36.96 ± 7.61 | p < 0.001 | |||||
| Neutrophils (1000/mm3) | 4.00 ± 1.33 | 3.75 ± 1.27 | p < 0.001 | |||||
| Lymphocytes (1000/mm3) | 2.03 ± 0.70 | 2.08 ± 0.64 | p < 0.01 | |||||
| NLR | 2.15 ± 0.96 | 1.93 ± 0.82 | p <0.001 | |||||
| Russo et al. [21] | Non-DM (n = 10) | DM (n = 10) | p value | |||||
| BMI (kg/m2) | 48.31 ± 7.6 | 48.44 ± 6.3 | 0.946 | |||||
| HbA1C (%) | 5.61 ± 0.32 | 6.92 ± 1.21 | 0.0006 | |||||
| Glucose (mg/dL) | 88.2 ± 9.2 | 134.4 ± 49.2 | 0.0038 | |||||
| Choromanska et al. [22] | Control | OB 0 | OB 1 | OB 3 | OB 6 | OB 12 | p values | |
| Weight (kg) | 62 (60.32–63) | 124 | 113 | 100.5 | 90 | 81.5 | <0.0001 | |
| (121.5–131.1) | (106.4–115.8) | (96.6–104.9) | (86.4–93.2) | (78–84.8) | ||||
| BMI (kg/m2) | 23 (23–23) | 46 (45–48) | 41 (40–43) | 37 (36–40) | 34 (32–35) | 30 (29–32) | <0.0001 | |
| WHR | 0.72 (0.71–0.72) | 0.97 | 0.98 | 0.97 | 0.96 | 0.92 | <0.0001 | |
| (0.96–0.99) | (0.96–0.99) | (0.94–0.99) | (0.93–0.97) | (0.91–0.94) | ||||
| SBP (mmHg) | 120 (110–120) | 130 (125–140) | 130 (125–140) | 130 (125–135) | 128 (120–135) | 125 (120–130) | <0.0001 | |
| DBP (mmHg) | 80 (70–80) | 85 (80–90) | 85 (80–90) | 80 (80–90) | 80 (80–85) | 80 (80–85) | <0.0001 | |
| TC (mmol/L) | 175 (170–178) | 198 (186–209) | 185 (175–192) | 177 (173–184) | 184 (174–191) | 175 (167–180) | <0.0001 | |
| LDL (mmol/L) | 118 (116–120) | 137 (128–148) | 115 (110–120) | 112 (104–119) | 109 (99–118) | 103 (99–113) | <0.0001 | |
| HDL (mmol/L) | 60 (59–62) | 46 (42–54) | 45 (39–49) | 47 (43–49) | 50 (48–54) | 55 (51–57) | <0.0001 | |
| TG (mmol/L) | 134 (130–135) | 135 (125–151) | 126 (107–139) | 115 (103–135) | 116 (99–124) | 98 (85–126) | <0.0001 | |
| Glucose (mg/dL) | 76 (73–78) | 101 (95–106) | 98 (91–99) | 93 (90–97) | 93 (87–96) | 87 (85–92) | <0.0001 | |
| Insulin (mUI/dL) | 7.6 (7.4–7.8) | 19 (17–22) | 13 (9.8–15) | 9 (7.3–11) | 8.6 (7.5–9.2) | 7.8 (6.9–8.5) | <0.0001 | |
| HOMA-IR | 1.4 (1.3–1.5) | 4.4 (4–5.4) | 3 (2.4–3.5) | 2 (1.7–2.4) | 1.9 (1.7–2.2) | 1.7 (1.5–1.9) | <0.0001 | |
| Catoi et al. [23] | Control group | Morbidly obese group | p-value | |||||
| Glucose (mg/dL) | 90.75 ± 7.19 | 104.15 ± 21.06 | 0.093 | |||||
| Insulin (mg/dL) | 6.84 ± 3.64 | 19.28 ± 19.09 | 0.215 | |||||
| HOMA-IR | 1.43 (0.78–2.08) | 3.31(2.66–5.05) | 0.008 | |||||
| Triglycerides (mg/dL) | 80.50 (69.50–89) | 122 (116–173) | 0.004 | |||||
| TC (mg/dL) | 150 ± 22.82 | 187.35 ± 43.08 | 0.032 | |||||
| HDL-chol (mg/dL) | 40.18 ± 8.71 | 49.66 ± 15.81 | 0.135 | |||||
| LDL-chol (mg/dL) | 93.80 ± 19.34 | 112 ± 39.83 | 0.242 | |||||
| Min et al. [24] | Baseline | 1 month | 6 months | 4 years | p value | |||
| Weight (kg) | 150 ± 37 | 132 ± 32 | 117 ± 29 | 116 ± 27 | <0.001 | |||
| BMI (kg/m2) | 54 ± 14 | 48 ± 12 | 43 ± 11 | 43 ± 11 | <0.001 | |||
| SBP (mmHg) | 137 ± 25 | 123 ± 15 | 131 ± 14 | 129 ± 20 | 0.021 | |||
| DBP (mmHg) | 81 ± 14 | 71 ± 10 | 76 ± 8 | 73 ± 13 | 0.001 | |||
| TC (mmol/L) | 4.3 ± 0.8 | 3.8 ± 1.1 | 4.2 ± 1.3 | 4.6 ± 1.3 | 0.178 | |||
| LDL (mmol/L) | 2.3 ± 0.6 | 2.1 ± 0.9 | 2.5 ± 1.2 | 2.4 ± 1.0 | 0.416 | |||
| HDL (mmol/L) | 1.2 ± 0.3 | 1.1 ± 0.3 | 1.2 ± 0.3 | 1.5 ± 0.6 | 0.002 | |||
| TG (mmol/L) | 1.7 ± 0.9 | 1.5 ± 0.5 | 1.4 ± 0.5 | 1.3 ± 0.5 | 0.151 | |||
| Glucose (mg/dL) | 7.3 (5.9–9.2) | 5.7 (4.8–6.8) | 5.4 (4.5–6.9) | 6.4 (5.5–9.0) | 0.378 | |||
| Insulin (mU/L) | 27.7 (19.6–38.6) | 12.6 (7.6–25.6) | 10.3 (6.0–20.7) | 16.9 (6.0–34.4) | 0.135 | |||
| HbA1c (mg/dL) | 58 ± 18 | 47 ± 12 | 45 ± 15 | 46 ± 15 | 0.049 | |||
| HOMA-IR assessment score | 0.4 ± 0.2 | 0.2 ± 0.3 | 0.1 ± 0.4 | 0.2 ± 0.4 | 0.098 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ion, R.-M.; Sibianu, M.; Hutanu, A.; Beresescu, F.G.; Sala, D.T.; Flavius, M.; Rosca, A.; Constantin, C.; Scurtu, A.; Moriczi, R.; et al. A Comprehensive Summary of the Current Understanding of the Relationship between Severe Obesity, Metabolic Syndrome, and Inflammatory Status. J. Clin. Med. 2023, 12, 3818. https://doi.org/10.3390/jcm12113818
Ion R-M, Sibianu M, Hutanu A, Beresescu FG, Sala DT, Flavius M, Rosca A, Constantin C, Scurtu A, Moriczi R, et al. A Comprehensive Summary of the Current Understanding of the Relationship between Severe Obesity, Metabolic Syndrome, and Inflammatory Status. Journal of Clinical Medicine. 2023; 12(11):3818. https://doi.org/10.3390/jcm12113818
Chicago/Turabian StyleIon, Razvan-Marius, Melania Sibianu, Adina Hutanu, Felicia Gabriela Beresescu, Daniela Tatiana Sala, Mocian Flavius, Ancuta Rosca, Calin Constantin, Alexandra Scurtu, Renata Moriczi, and et al. 2023. "A Comprehensive Summary of the Current Understanding of the Relationship between Severe Obesity, Metabolic Syndrome, and Inflammatory Status" Journal of Clinical Medicine 12, no. 11: 3818. https://doi.org/10.3390/jcm12113818
APA StyleIon, R.-M., Sibianu, M., Hutanu, A., Beresescu, F. G., Sala, D. T., Flavius, M., Rosca, A., Constantin, C., Scurtu, A., Moriczi, R., Muresan, M. G., Gabriel, P., Niculescu, R., & Neagoe, R. M. (2023). A Comprehensive Summary of the Current Understanding of the Relationship between Severe Obesity, Metabolic Syndrome, and Inflammatory Status. Journal of Clinical Medicine, 12(11), 3818. https://doi.org/10.3390/jcm12113818