
Co-Design of an Intervention to Increase the Participation in Leisure Activities Including Adolescents with Cerebral Palsy with GMFCS Levels IV and V: A Study Protocol
 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
Selection Criteria
Inclusion Criteria
Exclusion Criteria
2.3. Recruitment
2.4. Setting
2.5. Assessment Tools
- Listener is a less active role but certainly not less important in the project;
- Co-thinker can also involve asking questions and giving feedback, as well as giving an opinion when asked;
- Advisor gives feedback from project leaders to patients on whether or not advice has been followed at any time;
- Partner is valuable not only at the start of a project but also at the intermediate and final phases. The partner has the same function as the main researcher;
- Decision-maker requires project leaders to have a ‘hands off’ attitude.

2.5.1. Qualitative Tools
Research Phases
- What are the needs of adolescents with CP within the community?
- What barriers do you find in enhancing your participation in leisure activities?
- What are your perspectives on how to improve your participation?
- Do families and health professionals have the same perspectives on participation in the community as adolescents with CP?
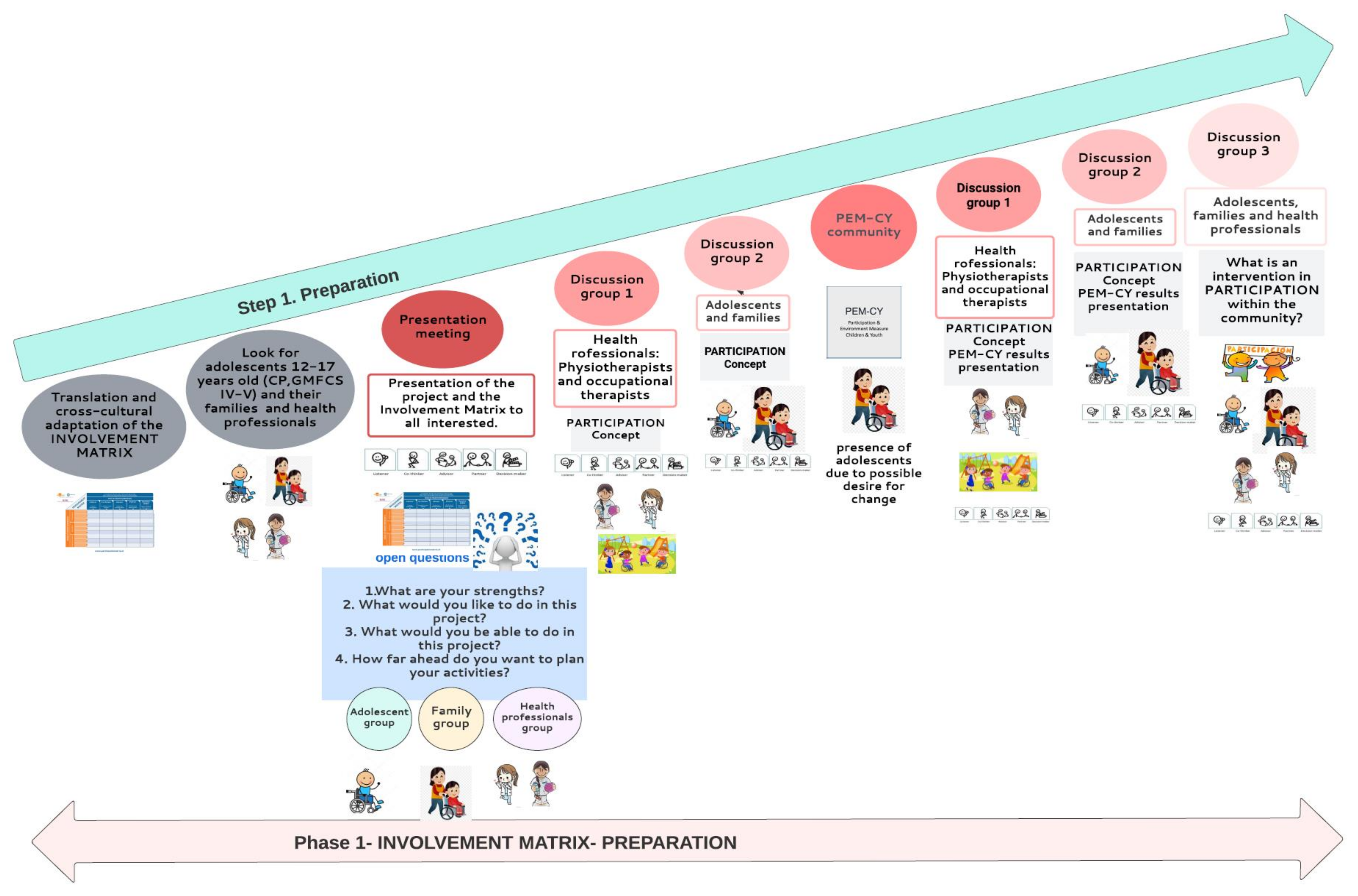
2.5.2. Phase (1) Preparation Phase-Step 1
(1.1) Involvement Matrix Translation
(1.2) Participants’ Recruitment
(1.3). Discussion/Development/Group Meetings (Shown in Figure 4)

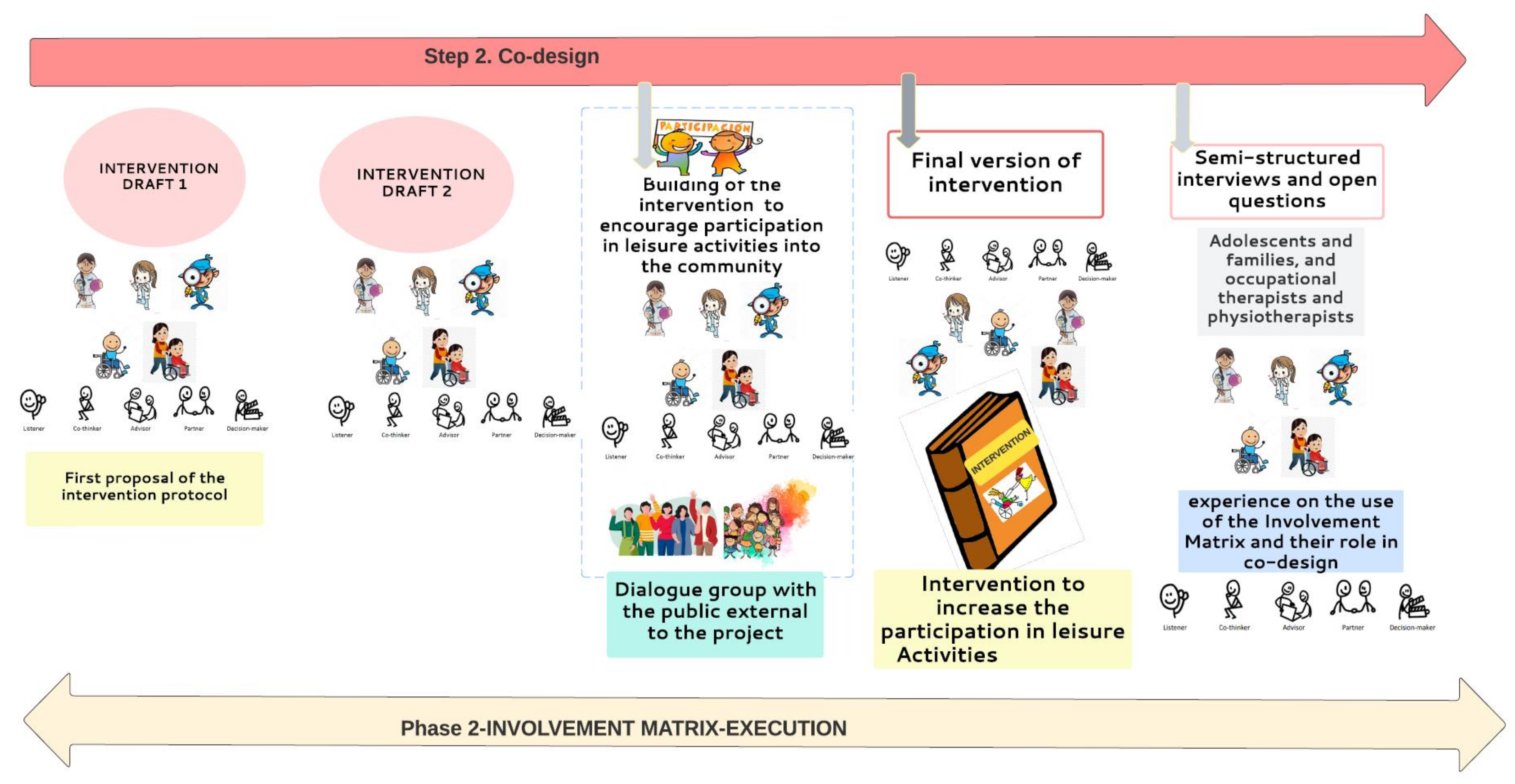
2.5.3. Phase (2) Execution Phase-Step 2 (Shown in Figure 5)

(2.1) Intervention Checking
(2.2) Co-Design Evaluation
3. Analysis Procedure
3.1. Data Analysis of Co-Design Experiences and Role
3.2. Participation of the Public in the Selection and Dissemination of Results and Analysis of the Feasibility of the Co-Design of the Study and Strategies of Dissemination
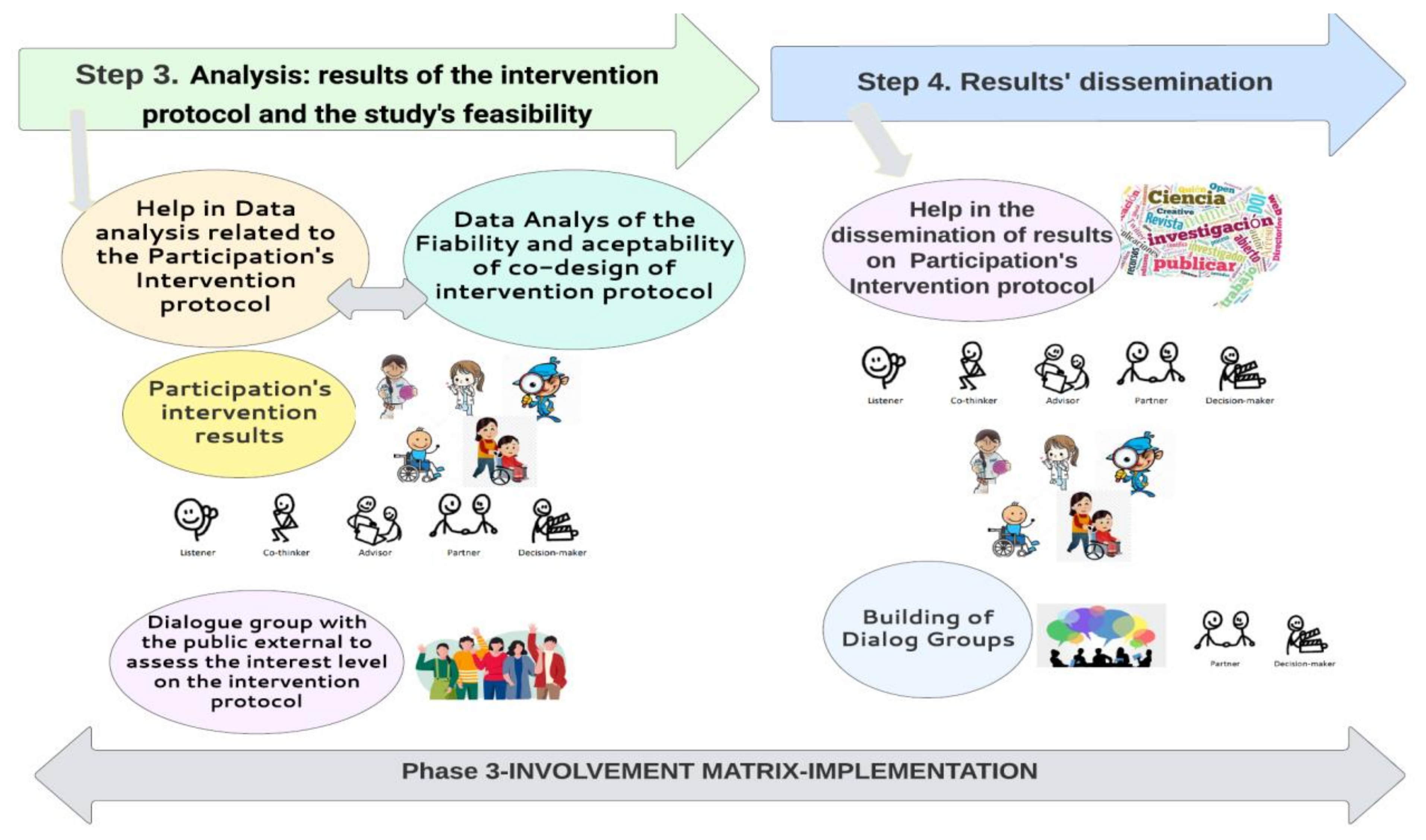
Phase (3) Implementation Phase-Step 3 and Step 4
Feasibility and Acceptability Analysis
Dissemination Strategies (Shown in Figure 6)

Coordination Brazil–Spain to Analyze the Data and Interpretation of Results from the Research Project
4. Time Line
5. Discussion and Perspectives
- What is the current participation of young people of adolescents with CP within the community like?
- Detection of barriers present in the community;
- Facilitators that increase participation: Improvements in access, adaptations and resources for participation according to the needs of young people with CP;
- Places within the community where the participation of young people with CP is encouraged (schools, leisure places, home, etc.);
- Role that the family and health professionals should have in the implementation of leisure activities within the community to encourage the participation of young people;
- Usefulness of the involvement of the PPI in the co-design of the intervention program to encourage the participation of young people with CP (GMFCS IV-V) within the community;
- Feasibility of co-designing the intervention protocol to encourage the participation of young people with CP (GMFCS IV-V) within the community;
- What should an intervention protocol to improve participation for adolescents GMFCS IV–V be like?
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sadowska, M.; Sarecka-Hujar, B.; Kopyta, I. Cerebral Palsy: Current Opinions on Definition, Epidemiology, Risk Factors, Classification and Treatment Options. Neuropsychiatr. Dis. Treat. 2020, 16, 1505–1518. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar] [PubMed]
- Weber, P.; Bolli, P.; Heimgartner, N.; Merlo, P.; Zehnder, T.; Kätterer, C. Behavioral and emotional problems in children and adults with cerebral palsy. Eur. J. Paediatr. Neurol. 2016, 20, 270–274. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Lawm, M.; King, S.; Rosenbaum, P.; Kertoy, M.K.; Young, N.L. A Conceptual Model of the Factors Affecting the Recreation and Leisure Participation of Children with Disabilities. Phys. Occup. Ther. Pediatr. 2003, 23, 63–90. [Google Scholar] [CrossRef]
- World Health Organization (WHO). International Classification of Functioning, Disability and Health; World Health Organization (WHO): Genova, Switzerland, 2001; ISBN 9241545429. [Google Scholar]
- Imms, C.; Granlund, M.; Wilson, P.H.; Steenbergen, B.; Rosenbaum, P.L.; Gordon, A.M. Participation, both a means and an end: A conceptual analysis of processes and outcomes in childhood disability. Dev. Med. Child Neurol. 2017, 59, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Shields, N.; Synnot, A. Perceived barriers and facilitators to participation in physical activity for children with disability: A qualitative study. BMC Pediatr. 2016, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Sienko, S. Understanding the factors that impact the participation in physical activity and recreation in young adults with cerebral palsy (CP). Disabil. Health J. 2019, 12, 467–472. [Google Scholar] [CrossRef]
- Engel-Yeger, B.; Jarus, T.; Anaby, D.; Law, M. Differences in Patterns of Participation Between Youths With Cerebral Palsy and Typically Developing Peers. Am. J. Occup. Ther. 2009, 63, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Rožkalne, Z.; Mukāns, M.; Vētra, A. Transition-Age Young Adults with Cerebral Palsy: Level of Participation and the Influencing Factors. Medicina 2019, 55, 737. [Google Scholar] [CrossRef] [PubMed]
- Boyd, H.; McKernon, S.; Mullin, B.; Old, A. Improving healthcare through the use of co-design. N. Z. Med. J. 2012, 125, 76–87. [Google Scholar]
- Harrison, J.D.; Auerbach, A.D.; Anderson, W.; Fagan, M.; Carnie, M.; Hanson, C.; Banta, J.; Symczak, G.; Robinson, E.; Schnipper, J.; et al. Patient stakeholder engagement in research: A narrative review to describe foundational principles and best practice activities. Health Expect. 2019, 22, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.; Boddy, K.; Briscoe, S.; Morris, C. Involving disabled children and young people as partners in research: A systematic review. Child. Care. Health Dev. 2015, 41, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Van Schelven, F.; Van Der Meulen, E.; Kroeze, N.; Ketelaar, M.; Boeije, H. Patient and public involvement of young people with a chronic condition: Lessons learned and practical tips from a large participatory program. Res. Involv. Engagem. 2020, 6, 59. [Google Scholar] [CrossRef]
- Involvement Matrix. Available online: https://www.kcrutrecht.nl/involvement-matrix/ (accessed on 10 November 2022).
- Hoddinott, P.; Pollock, A.; O’cathain, A.; Boyer, I.; Taylor, J.; Macdonald, C.; Oliver, S.; Donovan, J.L. How to incorporate patient and public perspectives into the design and conduct of research [version 1; peer review: 3 approved, 2 approved with reservations]. F1000Research 2018, 7, 752. [Google Scholar] [CrossRef] [PubMed]
- Smits, D.W.; Van Meeteren, K.; Klem, M.; Alsem, M.; Ketelaar, M. Designing a tool to support patient and public involvement in research projects: The Involvement Matrix. Res. Involv. Engagem. 2020, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.; Shilling, V.; Mchugh, C.; Wyatt, K. Why it is crucial to involve families in all stages of childhood disability research. Dev. Med. Child Neurol. 2011, 53, 769–771. [Google Scholar] [CrossRef] [PubMed]
- Kirwan, J.R.; de Wit, M.; Frank, L.; Haywood, K.L.; Salek, S.; Brace-McDonnell, S.; Lyddiatt, A.; Barbic, S.P.; Alonso, J.; Guillemin, F.; et al. Emerging Guidelines for Patient Engagement in Research. Value Health 2017, 20, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Hinton, L.; Finlay, T.; Macfarlane, A.; Fahy, N.; Clyde, B.; Chant, A. Frameworks for supporting patient and public involvement in research: Systematic review and co-design pilot. Health Expect. 2019, 22, 785–801. [Google Scholar] [CrossRef]
- Smith, E.; Bélisle-Pipon, J.-C.; Resnik, D. Patients as research partners; how to value their perceptions, contribution and labor? Citiz. Sci. Theory Pract. 2019, 4, 15. [Google Scholar] [CrossRef] [PubMed]
- McDermott, L.; Yardley, L.; Little, P.; Ashworth, M.; Gulliford, M. Developing a computer delivered, theory based intervention for guideline implementation in general practice. BMC Fam. Pract. 2010, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- Wintels, S.C.; Smits, D.W.; van Wesel, F.; Verheijden, J.; Ketelaar, M.; van der Leest, A.; de Groot, C.; Snel, D.; van de Water, J.; Sluiter, L.; et al. How do adolescents with cerebral palsy participate? Learning from their personal experiences. Health Expect. 2018, 21, 1024. [Google Scholar] [CrossRef] [PubMed]
- Cusack, C.; Cohen, B.; Mignone, J.; Chartier, M.J.; Lutfiyya, Z. Participatory action as a research method with public health nurses. J. Adv. Nurs. 2018, 74, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.C.; Bradette-Laplante, M.; Bérubé, D.; Brière, É.; Moisan, N.; Niquay, D.; Dogba, M.J.; Légaré, F.; McComber, A.; McGavock, J.; et al. Engaging indigenous patient partners in patient-oriented research: Lessons from a one-year initiative. Res. Involv. Engagem. 2020, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.; Lambert, C.; Coulthard, L.; Pennington, L.; Kolehmainen, N. Social participation to support good mental health in neurodisability. Child. Care. Health Dev. 2021, 47, 675–684. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.; Khetani, M.; Cousins, M.; Teplicky, R. Development of the participation and environment measure for children and youth: Conceptual basis. Disabil. Rehabil. 2012, 34, 238–246. [Google Scholar] [CrossRef]
- Coster, W.; Bedell, G.; Law, M.; Khetani, M.A.; Teplicky, R.; Liljenquist, K.; Gleason, K.; Kao, Y.C. Psychometric evaluation of the Participation and Environment Measure for Children and Youth. Dev. Med. Child Neurol. 2011, 53, 1030–1037. [Google Scholar] [CrossRef]
- Waisman-Nitzan, M.; Ivzori, Y.; Anaby, D. Implementing Pathways and Resources for Engagement and Participation (PREP) for Children with Disabilities in Inclusive Schools: A Knowledge Translation Strategy. Phys. Occup. Ther. Pediatr. 2022, 42, 526–541. [Google Scholar] [CrossRef]
- Anaby, D.R.; Law, M.; Feldman, D.; Majnemer, A.; Avery, L. The effectiveness of the Pathways and Resources for Engagement and Participation (PREP) intervention: Improving participation of adolescents with physical disabilities. Dev. Med. Child Neurol. 2018, 60, 513–519. [Google Scholar] [CrossRef]
- Law, M.; Anaby, D.; Teplicky, R.; Turner, L. Pathways and Resources for Engagement and Participation, a Practice Model for Occupational Therapists; CanChild: Hamilton, ON, Canada, 2016. [Google Scholar]
- IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0; IBM Corp: Armonk, NY, USA.
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Zamawe, F.C. The Implication of Using NVivo Software in Qualitative Data Analysis: Evidence-Based Reflections. Malawi Med. J. 2015, 27, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.D.; Anderson, W.G.; Fagan, M.; Robinson, E.; Schnipper, J.; Symczak, G.; Hanson, C.; Carnie, M.B.; Banta, J.; Chen, S.; et al. Patient and Family Advisory Councils (PFACs): Identifying Challenges and Solutions to Support Engagement in Research. Patient 2018, 11, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.; Forsythe, L.; Ellis, L.; Schrandt, S.; Sheridan, S.; Gerson, J.; Konopka, K.; Daugherty, S. Conceptual and practical foundations of patient engagement in research at the patient-centered outcomes research institute. Qual. Life Res. 2015, 24, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Marlett, N.; Shklarov, S.; Marshall, D.; Santana, M.J.; Wasylak, T. Building new roles and relationships in research: A model of patient engagement research. Qual. Life Res. 2015, 24, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Hersh, D.; Israel, M.; Shiggins, C. The ethics of patient and public involvement across the research process: Towards partnership with people with aphasia. Aphasiology 2021, 1–27. [Google Scholar] [CrossRef]
- Dada, S.; May, A.; Bastable, K.; Samuels, A.; Tönsing, K.; Wilder, J.; Casey, M.; Ntuli, C.; Reddy, V. The involvement matrix as a framework for involving youth with severe communication disabilities in developing health education materials. Health Expect. 2022, 25, 1004–1015. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Spain | Brazil |
|---|---|---|
| Places of recruitment | Fundació Aspace Catalunya em Barcelona (Aspace Foundation-Catalonia) | Associations, support networks and social networks |
| Type of meetings | Remote | Remote |
| Number of Adolescents with CP | 9 | 9 |
| Number of families of adolescents with CP | 9 | 9 |
| Health professionals: PTs | 3 | 3 |
| Health professionals: OTs | 3 | 3 |
| Country | Spain | Brazil | Description | Duration of Each Group (min) |
|---|---|---|---|---|
| Presentation meeting | 1 | 1 | Presentation of the project and the IM to all stakeholders | 60 |
| Discussion groups-Participation | 2 | 2 | Presentation of the concept of participation based on the ICF and its meaning in practice | 60–90 |
| PEMCY questionnaire | 9 | 9 | Application of the PEM-CY community session | 60–90 |
| Discussion groups-Participation + PEMCY results | 2 | 2 | Discussion of the concept of participation now based on the results of the application of PEM-CY | 60–90 |
| Discussion Group-What is a community participation intervention? | 1 | 1 | Discussion about what is an intervention aimed to improve the participation of young people with disabilities in the community | 60–90 |
| Discussion Group-intervention draft | 2 | 2 | Co-design of an intervention draft aimed at the participation of young people with CP GMFCS IV-V in leisure activities | 60–90 |
| Meetings with the external public | 1 | 1 | Presentation of protocol results so far and capture criticism and suggestions from an external group made up of adolescents with CP GMFCS IV and V | 60 |
| Discussion Group-final version | 3 | 3 | Co-design of final version with all ingredients that should be present in the intervention for CP to increase the community participation | 60–90 |
| Semi-structured interviews and open-ended questions | 24 | 24 | A guide with questions will be used | 60–90 |
| Oct–Dec 2022 | Jan–Mar 2023 | Apr–Jun 2023 | Jul–Sep 2023 | Oct–Dec 2023 | Jan–Mar 2024 | ||
|---|---|---|---|---|---|---|---|
| Phase 1. Step 1 | X | X | |||||
| Phase 2. Step 2 | X | X | |||||
| Phase 3 | Step 3 | X | |||||
| Step 4 | X | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomo-Carrión, R.; De Araújo Ferreira Jesus, C.C.; Santana, C.A.S.; Lindquist, R.; Alencar, R.; Romay-Barrero, H.; Contell-Gonzalo, E.; Monteiro, K.S.; Pinero-Pinto, E.; Longo, E. Co-Design of an Intervention to Increase the Participation in Leisure Activities Including Adolescents with Cerebral Palsy with GMFCS Levels IV and V: A Study Protocol. J. Clin. Med. 2023, 12, 182. https://doi.org/10.3390/jcm12010182
Palomo-Carrión R, De Araújo Ferreira Jesus CC, Santana CAS, Lindquist R, Alencar R, Romay-Barrero H, Contell-Gonzalo E, Monteiro KS, Pinero-Pinto E, Longo E. Co-Design of an Intervention to Increase the Participation in Leisure Activities Including Adolescents with Cerebral Palsy with GMFCS Levels IV and V: A Study Protocol. Journal of Clinical Medicine. 2023; 12(1):182. https://doi.org/10.3390/jcm12010182
Chicago/Turabian StylePalomo-Carrión, Rocío, Caline Cristine De Araújo Ferreira Jesus, Camila Araújo Santos Santana, Raquel Lindquist, Roselene Alencar, Helena Romay-Barrero, Elena Contell-Gonzalo, Karolinne Souza Monteiro, Elena Pinero-Pinto, and Egmar Longo. 2023. "Co-Design of an Intervention to Increase the Participation in Leisure Activities Including Adolescents with Cerebral Palsy with GMFCS Levels IV and V: A Study Protocol" Journal of Clinical Medicine 12, no. 1: 182. https://doi.org/10.3390/jcm12010182
APA StylePalomo-Carrión, R., De Araújo Ferreira Jesus, C. C., Santana, C. A. S., Lindquist, R., Alencar, R., Romay-Barrero, H., Contell-Gonzalo, E., Monteiro, K. S., Pinero-Pinto, E., & Longo, E. (2023). Co-Design of an Intervention to Increase the Participation in Leisure Activities Including Adolescents with Cerebral Palsy with GMFCS Levels IV and V: A Study Protocol. Journal of Clinical Medicine, 12(1), 182. https://doi.org/10.3390/jcm12010182