

Aero-Medical Evacuation during SARS-CoV-2 Pandemic: Extraordinary Measure or Emerging Treatment Option?


 ,
on behalf of the COVID-19 INMI group
,
on behalf of the COVID-19 INMI group
Abstract
:1. Introduction
2. Materials and Methods
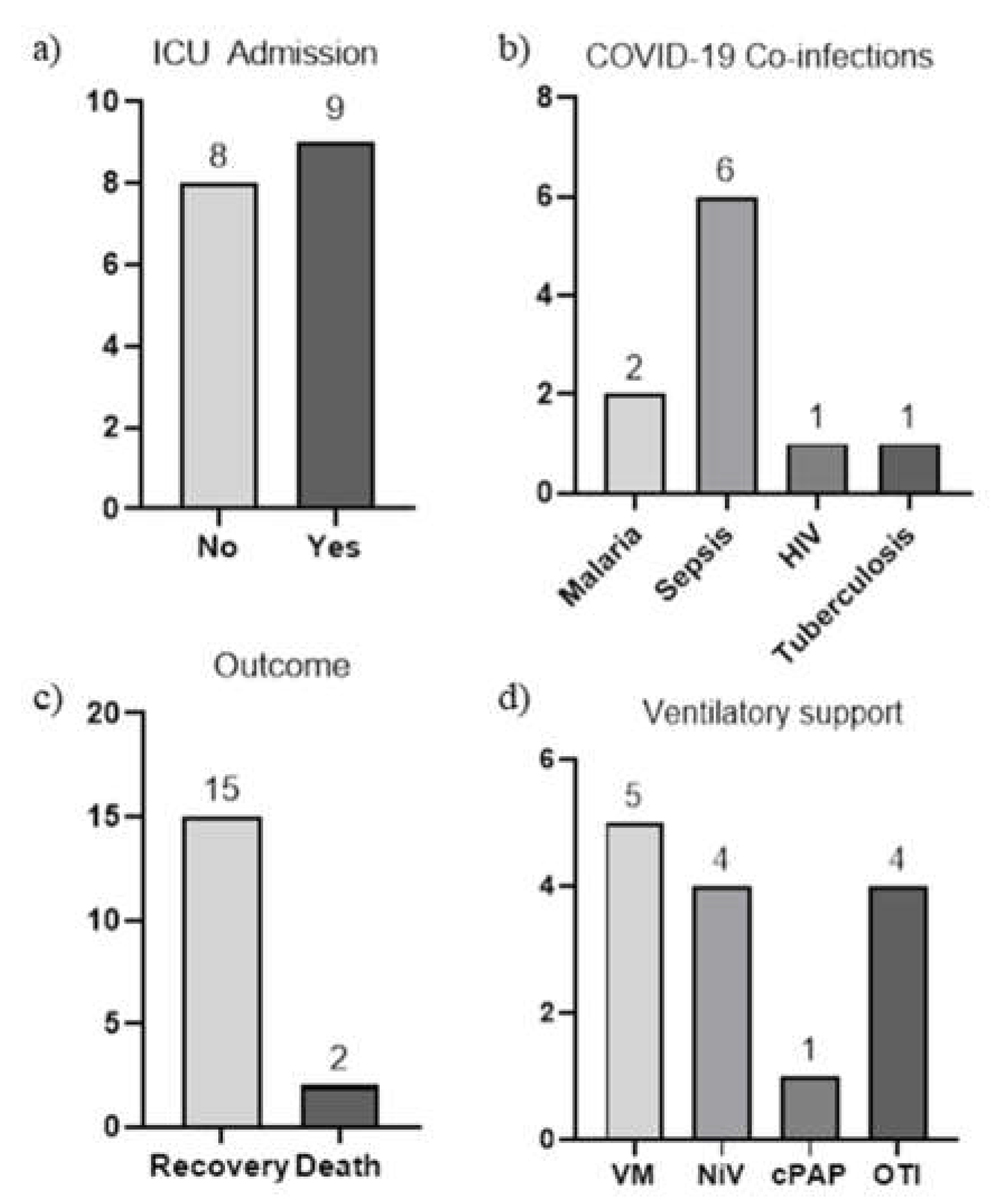
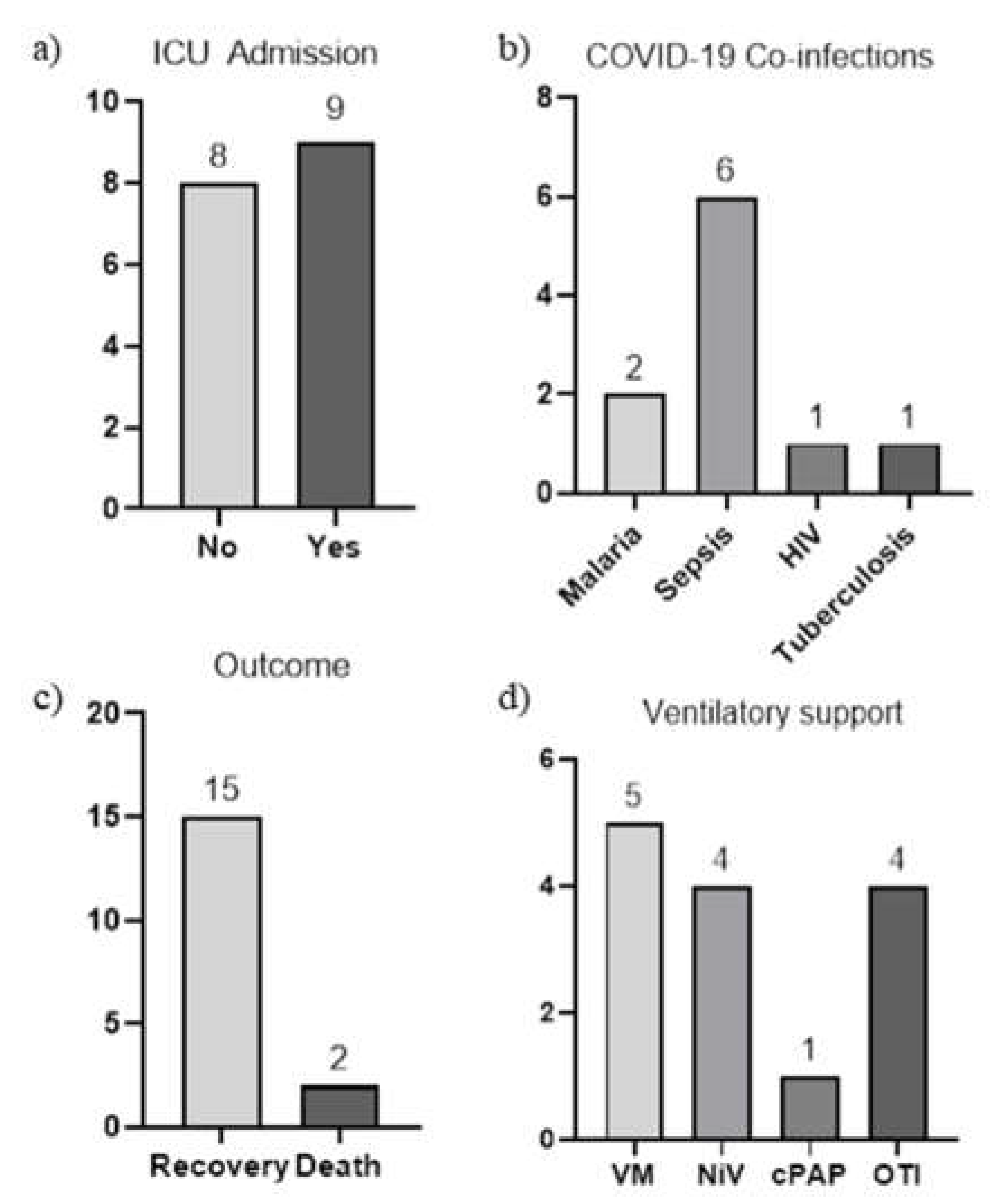
3. Results
- A 57 year-old male patient treated, very early in the first phase of the COVID pandemic, with three infusions of 250 mL hyperimmune convalescent plasma with >1: 320 neutralizing antibody titer against SARS-CoV-2.
- A 64 year-old female patient treated with three infusions of 250 ml hyperimmune convalescent plasma with >1:320 neutralizing antibody titer against SARS-CoV-2 and with oral acyclovir (800 mg thrice per day) for Herpes Virus—2 reactivation.
- A 50 year-old male, treated with iv tocilizumab (8 mg followed by a second infusion, 12 h apart).
- A 57-year-old patient, treated with highly active antiretroviral therapy with an oral fixed combination of emtricitabine, rilpivirine and tenofovir alafenamide.
- A 67 year-old patient, treated for severe ARDS and for polymicrobial sepsis sustained by pseudomonas, aspergillus, pneumocystis pneumonia (PCP) and cytomegalovirus (CMV), candida tropicalis and a vancomycin-resistant enterococcus (VRE). He was treated with i.v. linezolid (600 mg every 12 h), merrem (2 g every 8 h), colistin (9,000,000 I.U./daily), daptomycin (500 mg/daily), ganciclovir, anidulafungin (an initial dose 200 mg followed by 100 mg/daily), voriconazole (an initial dose of 400 mg every 12 h for the first 24 h followed by 200 mg every 12 h), Tigecycline (an initial dose of 100 mg, followed by 50 mg every 12 h), Ampicillin (2 g every 6 h) and trimethoprim (100 mg every 12 h) but unfortunately died.
- Two young males (23 and 30 years old, respectively) traveling in West Africa with no malaria prophylaxis, initially admitted to a local hospital for uncomplicated Plasmodium falciparum malaria and COVID-19 coinfection. They were treated with oral artemisinin-based combination therapy (ACT) with 20/120 mg artemether/lumefantrine, four tablets twice-daily for three days; while in Italy they received oral dexamethasone (6 mg per day) and oxygen therapy for COVID-19 pneumonia only. Two weeks after discharge, the older patient was re-admitted for uncomplicated P. falciparum malaria relapse. He was re-treated with a three-day course of ACT including 320/40 mg piperaquine/artenimol four tablets per day for three days with full recovery at the follow-up visit.
- A 59 year-old patient, admitted for malaria and COVID-19 coinfection. He was locally treated with unspecified ACT antimalarial oral therapy for 3 days, methylprednisolone (1 mg/Kg for 5 days), enoxaparin (6000 IU every 12 hours for 22 days), ceftriaxone (2 g daily for 5 days) and oxygen therapy. For the worsening of the respiratory function 12 hours after his admission, he began therapy with C-PAP for 2 weeks. During the length of stay, there was a progressive improvement until discharge with full recovery.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teichman, P.G.; Donchin, Y.; Kot, R.J. International aeromedical evacuation. N. Engl. J. Med. 2007, 356, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, S.G.; Herstein, J.J.; Le, A.B.; Beam, E.L.; Cieslak, T.J.; Lawler, J.V.; Santarpia, J.L.; Stentz, T.L.; Kopocis-Herstein, K.R.; Achutan, C.; et al. Need for Aeromedical Evacuation High-Level Containment Transport Guidelines. Emerg. Infect. Dis. 2019, 25, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Araiza, A.; Duran, M.; Surani, S.; Varon, J. Aeromedical Transport of Critically Ill Patients: A Literature Review. Cureus 2021, 13, e14889. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, K.; Bornales, R.B. Historic Firsts: Aeromedical Evacuation and the Transportation Isolation System. Air Med. J. 2021, 40, 76–78. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gender | Country | Hospitalization (Days) | Age (Years) | VM, cPAP, NiV, OTI † | Coinfections | Clinical Outcome |
|---|---|---|---|---|---|---|
| F | Albania | 92 | 64 | OTI | sepsis | Recovery |
| M | Albania | 39 | 50 | OTI | sepsis | Recovery |
| F | Albania | 21 | 78 | VM | Recovery | |
| F | Albania | 38 | 78 | OTI | sepsis | Recovery |
| M | Nigeria | 38 | 67 | OTI | sepsis | Death |
| M | Nigeria | 7 | 63 | VM | HIV § | Recovery |
| F | DRC * | 14 | 67 | NiV | TB ‡ | Recovery |
| M | Kenya | 30 | 51 | c-PAP | sepsis | Recovery |
| M | Libya | 9 | 59 | NiV | Recovery | |
| M | Angola | 22 | 59 | c-PAP | malaria | Recovery |
| M | Kazakhstan | 25 | 57 | NiV | sepsis | Recovery |
| M | Nigeria | 3 | 65 | OTI | Recovery | |
| F | Zimbabwe | 16 | 64 | OTI | Death | |
| M | Egypt | 11 | 55 | VM | Recovery | |
| M | Romania | 24 | 47 | OTI | Recovery | |
| M | Libya | 10 | 23 | VM | malaria | Recovery |
| M | Libya | 12 | 30 | VM | malaria | Recovery |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benvenuto, D.; Ascoli Bartoli, T.; Curtolo, A.; Palazzolo, C.; Vita, S.; Mariano, A.; Scorzolini, L.; Ippolito, G.; Marchioni, L.; Cerini, F.; et al. Aero-Medical Evacuation during SARS-CoV-2 Pandemic: Extraordinary Measure or Emerging Treatment Option? J. Clin. Med. 2023, 12, 133. https://doi.org/10.3390/jcm12010133
Benvenuto D, Ascoli Bartoli T, Curtolo A, Palazzolo C, Vita S, Mariano A, Scorzolini L, Ippolito G, Marchioni L, Cerini F, et al. Aero-Medical Evacuation during SARS-CoV-2 Pandemic: Extraordinary Measure or Emerging Treatment Option? Journal of Clinical Medicine. 2023; 12(1):133. https://doi.org/10.3390/jcm12010133
Chicago/Turabian StyleBenvenuto, Domenico, Tommaso Ascoli Bartoli, Ambrogio Curtolo, Claudia Palazzolo, Serena Vita, Andrea Mariano, Laura Scorzolini, Giuseppe Ippolito, Luisa Marchioni, Federico Cerini, and et al. 2023. "Aero-Medical Evacuation during SARS-CoV-2 Pandemic: Extraordinary Measure or Emerging Treatment Option?" Journal of Clinical Medicine 12, no. 1: 133. https://doi.org/10.3390/jcm12010133
APA StyleBenvenuto, D., Ascoli Bartoli, T., Curtolo, A., Palazzolo, C., Vita, S., Mariano, A., Scorzolini, L., Ippolito, G., Marchioni, L., Cerini, F., D’Offizi, G., Vaia, F., & Nicastri, E., on behalf of the COVID-19 INMI group. (2023). Aero-Medical Evacuation during SARS-CoV-2 Pandemic: Extraordinary Measure or Emerging Treatment Option? Journal of Clinical Medicine, 12(1), 133. https://doi.org/10.3390/jcm12010133