
Acute Pulmonary Artery Thrombosis despite Anticoagulation in Patients with COVID-19 Pneumonia: A Single-Center Retrospective Cohort Study

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
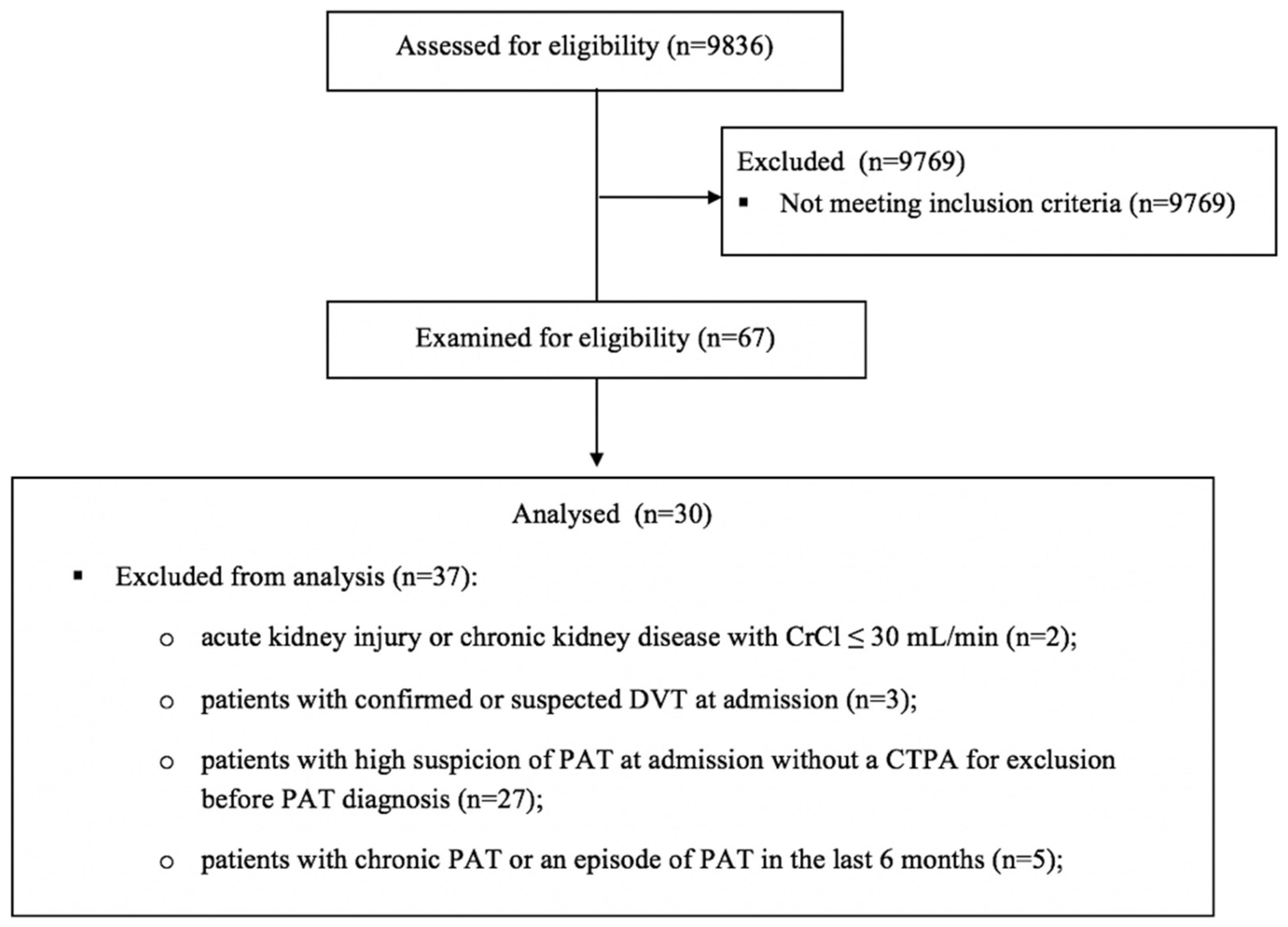
2.1. Study Design and Population
2.2. Definitions
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Clinical Characteristics, Anticoagulation and Imaging Data of Patients with PAT
3.2. Comparative Clinical and Laboratory Data at Hospital Admission and at PAT Diagnosis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Becker, R.C. COVID-19 update: COVID-19-associated coagulopathy. J. Thromb. Thrombolysis 2020, 50, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.-P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and MetaAnalysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, D.; Sperhake, J.P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Loo, J.; Spittle, D.A.; Newnham, M. COVID-19, immunothrombosis and venous thromboembolism: Biological mechanisms. Thorax 2021, 76, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Thachil, J.; Srivastava, A. SARS-2 Coronavirus-Associated Hemostatic Lung Abnormality in COVID-19: Is It Pulmonary Thrombosis or Pulmonary Embolism? Semin. Thromb. Hemost. 2020, 46, 777–780. [Google Scholar] [CrossRef]
- Kutsogiannis, D.J.; Alharthy, A.; Balhamar, A.; Faqihi, F.; Papanikolaou, J.; Alqahtani, S.A.; Memish, Z.A.; Brindley, P.G.; Brochard, L.; Karakitsos, D. Mortality and Pulmonary Embolism in Acute Respiratory Distress Syndrome From COVID-19 vs. Non-COVID-19. Front. Med. 2022, 9, 800241. [Google Scholar] [CrossRef]
- Angelo, P.; Roberto, P. Venous Thromboembolism and Heparin Use in COVID-19 Patients: Juggling between Pragmatic Choices, Suggestions of Medical Societies and the Lack of Guidelines. J. Thromb. Thrombolysis 2020, 50, 68–71. [Google Scholar] [CrossRef]
- Chandra, A.; Chakraborty, U.; Ghosh, S.; Dasgupta, S. Anticoagulation in COVID-19: Current concepts and controversies. Postgrad. Med. J. 2021, 98, 395–402. [Google Scholar] [CrossRef]
- Mueller-Peltzer, K.; Krauss, T.; Benndorf, M.; Lang, C.N.; Bamberg, F.; Bode, C.; Duerschmied, D.; Staudacher, D.L.; Zotzmann, V. Pulmonary artery thrombi are co-located with opacifications in SARS-CoV2 induced ARDS. Respir. Med. 2020, 172, 106135. [Google Scholar] [CrossRef]
- Kampouri, E.; Filippidis, P.; Viala, B.; Méan, M.; Pantet, O.; Desgranges, F.; Tschopp, J.; Regina, J.; Karachalias, E.; Bianchi, C.; et al. Predicting Venous Thromboembolic Events in Patiens with Coronavirus Disease 2019 Requiring Hospitalisation: An Observational Retrospective Study by the COVIDIC Initiative in a Swiss University Hospital. BioMed Res. Int. 2020, 2020, 9126148. [Google Scholar] [CrossRef]
- Mehta, O.P.; Bhandari, P.; Raut, A.; Kacimi, S.E.O.; Huy, N.T. Coronavirus Disease (COVID-19): Comprehensive Review of Clinical Presentation. Front. Public Health 2021, 8, 582932. [Google Scholar] [CrossRef] [PubMed]
- Nutescu, E.A.; Spinler, S.A.; Wittkowsky, A.; Dager, W.E. Low-molecular-weight heparins in renal impairment and obesity: Available evidence and clinical practice recommendations across medical and surgical settings. Ann. Pharmacother. 2009, 43, 1064–1083. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612–1620. [Google Scholar] [CrossRef] [PubMed]
- Rindi, L.V.; Al Moghazi, S.; Donno, D.R.; Cataldo, M.A.; Petrosillo, N. Predictive scores for the diagnosis of Pulmonary Embolism in COVID-19: A systematic review. Int. J. Infect. Dis. 2022, 115, 93–100. [Google Scholar] [CrossRef]
- Di Tano, G.; Dede, M.; Pellicelli, I.; Martinelli, E.; Moschini, L.; Calvaruso, E.; Danzi, G.B. Pulmonary embolism in patients with COVID-19 pneumonia on adequate oral anticoagulation. J. Thromb. Thrombolysis 2021, 53, 576–580. [Google Scholar] [CrossRef]
- Terrigno, V.R.; Ricketti, D.A.; Patel, P.; Roy, S. Recurrent chronic thromboembolic disease despite optimal anticoagulation in setting of recent COVID-19 infection. BMJ Case Rep. 2021, 14, e238733. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef]
- Salam, S.; Mallat, J.; Elkambergy, H. Acute high-risk pulmonary embolism requiring thrombolytic therapy in a COVID-19 pneumonia patient despite intermediate dosing deep vein thromboprophylaxis. Respir. Med. Case Rep. 2020, 31, 1101263. [Google Scholar] [CrossRef]
- McFadyen, J.D.; Stevens, H.; Peter, K. The Emerging Threat of (Micro)Thrombosis in COVID-19 and Its Therapeutic Implications. Circ. Res. 2020, 127, 571–587. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. Crics Triggersep Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- van Dam, L.; Kroft, L.; van der Wal, L.; Cannegieter, S.; Eikenboom, J.; de Jonge, E.; Huisman, M.; Klok, F. Clinical and computed tomography characteristics of COVID-19 associated acute pulmonary embolism: A different phenotype of thrombotic disease? Thromb. Res. 2020, 193, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Bompard, F.; Monnier, H.; Saab, I.; Tordjman, M.; Abdoul, H.; Fournier, L.; Sanchez, O.; Lorut, C.; Chassagnon, G.; Revel, M.-P. Pulmonary embolism in patients with COVID-19 pneumonia. Eur. Respir. J. 2020, 56, 2001365. [Google Scholar] [CrossRef] [PubMed]
- De Cobelli, F.; Palumbo, D.; Ciceri, F.; Landoni, G.; Ruggeri, A.; Rovere-Querini, P.; D’Angelo, A.; Steidler, S.; Galli, L.; Poli, A.; et al. Pulmonary Vascular Thrombosis in COVID-19 Pneumonia. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3631–3641. [Google Scholar] [CrossRef] [PubMed]
- Liao, S.C.; Shao, S.C.; Chen, Y.T.; Chen, Y.C.; Hung, M.J. Incidence and mortality of pulmonary embolism in COVID-19: A systematic review and meta-analysis. Crit. Care 2020, 24, 464. [Google Scholar] [CrossRef]


{kind=link}
| Variables | All Patients (N = 30) |
|---|---|
| Male, N (%) | 25 (83.3) |
| Age (years), median (25–75th percentile) | 62 (54–74) |
| Comorbidities, N (%) | 22 (73.3) |
| Obesity | 8 (26.6) |
| Type 2 diabetes mellitus | 9 (30) |
| Cardiovascular comorbidities, | |
| Hypertension | 15 (50) |
| Congestive heart failure | 2 (6.6) |
| Coronary artery disease | 2 (6.6) |
| Cardiac arrhythmias | 5 (16.6) |
| Hypertrophic cardiomyopathy | 1 (3.3) |
| Valvular heart disease | 2 (6.6) |
| Peripheral venous disease | 1 (3.3) |
| Dyslipidemia | 7 (23.3) |
| Prior stroke | 1 (3.3) |
| Dementia | 1 (3.3) |
| Chronic eye disorders (glaucoma) | 2 (6.6) |
| Gastrointestinal and liver diseases | 7 (23.3) |
| Active malignancy | 1 (3.3) |
| Non-malignant solid tumors | 3 (10) |
| Clinical presentation, N (%) | |
| Dyspnea | 18 (60) |
| Hemoptysis | 2 (6.6) |
| Chest tightness | 3 (10) |
| Clinical signs of DVT at PAT diagnosis | 0 (0) |
| Signs of right-sided heart failure | 2 (6.6) |
| Massive PAT (hemodynamic instability) | 1 (3.3) |
| Duration of LMWH anticoagulation until PAT (days), median (25–75th percentile) | 8 (4.7–12) |
| LMWH anticoagulation type, N (%) | |
| Prophylactic doses | 7 (23.3) |
| Intermediate doses | 14 (46.6) |
| Therapeutic doses | 9 (30) |
| The time from symptoms onset at PAT diagnosis, (days), median (25–75th percentile) | 16 (11.7–20) |
| Modified two-level Wells score for pulmonary embolism, N (%) | |
| ≤4 points (pulmonary embolism unlikely) | 29 (96.6) |
| >4 points (pulmonary embolism likely) | 1 (3.3) |
| Original Wells score for pulmonary embolism, N (%) | |
| <2 points (low probability) | 24 (80) |
| 2–6 points (intermediate probability) | 6 (20) |
| >6 points (high probability) | 0 |
| PADUA Prediction Score at PAT diagnosis, N (%) | |
| 1–3 points (low risk of VTE disease) | 4 (13.3) |
| ≥4 points (high risk of VTE disease) | 26 (86.6) |
| PAT localisation by CTPA, N (%) | 9 (30) |
| Right lung | 11 (36.6) |
| Left lung | 10 (33.3) |
| Bilateral | 23 (76.6) |
| Lung base | |
| One lobe | 15 (50) |
| Two lobes | 10 (33.3) |
| 3–4 lobes | 5 (16.6) |
| Main artery | 3 (10) |
| Lobar arteries | 9 (30) |
| Segmental arteries | 20 (66.6) |
| Subsegmental arteries | 7 (23.3) |
| Chest CT analysis of COVID-19 lung involvement at PAT diagnosis, N (%) | |
| ≤25% | 1 (3.3) |
| 25–50% | 7 (23.3) |
| 50–75% | 15 (50) |
| ≥75% | 7 (23.3) |
| Duration of hospitalisation (days), median (25–75th percentile) | 24 (20–28) |
| Outcome, N (%) | |
| Deceased | 9 (30) |
| Discharged with no sequalae | 11 (36.6) |
| Discharged with persistent respiratory failure | 10 (33.3) |
| Cases | Duration of Therapeutic LMWH between CTPAs (Days) | D-Dimer (ng/mL) (When First CTPA Was Performed) | CTPA Changes (at PAT Diagnosis) | D-Dimer (ng/mL) (at PAT Diagnosis) |
|---|---|---|---|---|
| Case 1, 72-year-old man | 6 | 11,000 | Main right artery, extended to lobar, segmental and subsegmental arteries | >20,000 |
| Case 2, 69-year-old woman | 4 | 1930 | Minor PAT, lower inferior lobe, right lung | 9530 |
| Case 3, 76-year-old man | 8 | 14,330 | Bilateral PAT—left inferior lobar artery and segmental arteries in middle lobe | 2730 |
| Case 4, 81-year-old man | 8 | 5337 | Minor PAT, lower inferior lobe, segmental arteries, left lung | 8712 |
| Variables | At Hospital Admission (N = 30) | At PAT Diagnosis (N = 30) | p Value |
|---|---|---|---|
| Oxygen flow rate, N (%) | |||
| ≤15 (L/min) | 12 (40) | 5 (16.6) | 0.006 |
| HFOT | 13 (43.3) | 13 (43.3) | - |
| Mechanical ventilation | 5 (16.6) | 12 (40) | 0.006 |
| Leukocyte count (cells/mm3), mean ± SD | 8430 ± 3520 | 12,105 ± 4795 | 0.001 |
| Lymphocyte count (cells/mm3), mean ± SD | 800 ± 456 | 959 ± 545 | 0.17 |
| Neutrophils/lymphocytes ratio, median (25–75th percentile) | 8.8 (6.3–14.2) | 11.8 (5.2–22.8) | 0.26 |
| CRP (mg/L), mean ± SD (nv: <3) | 124.8 ± 70.7 | 40.4 ± 41.4 | <0.001 |
| Ferritin (ng/mL), mean ± SD (nv: <290) | 1689 ± 1178 | 1493 ± 691 | 0.46 |
| D-dimer (ng/mL), mean ± SD (nv: <230) | 1819 ± 3247 | 7449 ± 6979 | <0.001 |
| Fibrinogen (mg/dL), mean ± SD (nv: <400) | 613 ± 202 | 398 ± 215 | <0.001 |
| PT (s), mean ± SD | 13.9 ± 1.8 | 16.2 ± 10.7 | 0.26 |
| PC (%), mean ± SD | 84.5 ± 16.7 | 80 ± 23 | 0.4 |
| aPTT (s), mean ± SD | 30.2 ± 6.4 | 37.8 ± 23.3 | 0.23 |
| CK (U/L), mean ± SD (nv: <135) | 233 ± 254 | 137 ± 222 | 0.11 |
| CK-MB (U/L), mean ± SD (nv: <16) | 18 ± 14 | 20 ± 14 | 0.48 |
| NT-proBNP (pg/mL), mean ± SD (nv: <450) | 678 ± 752 | 2282 ± 7754 | 0.36 |
| LDH (U/L), mean ± SD (nv: <246) | 546 ± 234 | 663 ± 366 | 0.09 |
| AST (U/L), mean ± SD (nv: <36) | 66 ± 46 | 61 ± 40 | 0.61 |
| ALT (U/L), mean ± SD (nv: <35) | 57 ± 53 | 76 ± 62 | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niculae, C.-M.; Anghel, A.-M.-J.; Militaru, E.-D.; Tîrlescu, L.-G.; Lazar, M.; Hristea, A. Acute Pulmonary Artery Thrombosis despite Anticoagulation in Patients with COVID-19 Pneumonia: A Single-Center Retrospective Cohort Study. J. Clin. Med. 2022, 11, 2633. https://doi.org/10.3390/jcm11092633
Niculae C-M, Anghel A-M-J, Militaru E-D, Tîrlescu L-G, Lazar M, Hristea A. Acute Pulmonary Artery Thrombosis despite Anticoagulation in Patients with COVID-19 Pneumonia: A Single-Center Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(9):2633. https://doi.org/10.3390/jcm11092633
Chicago/Turabian StyleNiculae, Cristian-Mihail, Ana-Maria-Jennifer Anghel, Eliza-Daniela Militaru, Laura-Georgiana Tîrlescu, Mihai Lazar, and Adriana Hristea. 2022. "Acute Pulmonary Artery Thrombosis despite Anticoagulation in Patients with COVID-19 Pneumonia: A Single-Center Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 9: 2633. https://doi.org/10.3390/jcm11092633
APA StyleNiculae, C.-M., Anghel, A.-M.-J., Militaru, E.-D., Tîrlescu, L.-G., Lazar, M., & Hristea, A. (2022). Acute Pulmonary Artery Thrombosis despite Anticoagulation in Patients with COVID-19 Pneumonia: A Single-Center Retrospective Cohort Study. Journal of Clinical Medicine, 11(9), 2633. https://doi.org/10.3390/jcm11092633