
A Comparison of Barrier Factors between Hospitals with and without Cardiac Rehabilitation Programs in Korea: A Nation-Wide Survey Research

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Target Subjects and Conducting of the Survey
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. The General Characteristic between the Hospitals with and without CRP
3.2. The Response Rate to the Survey
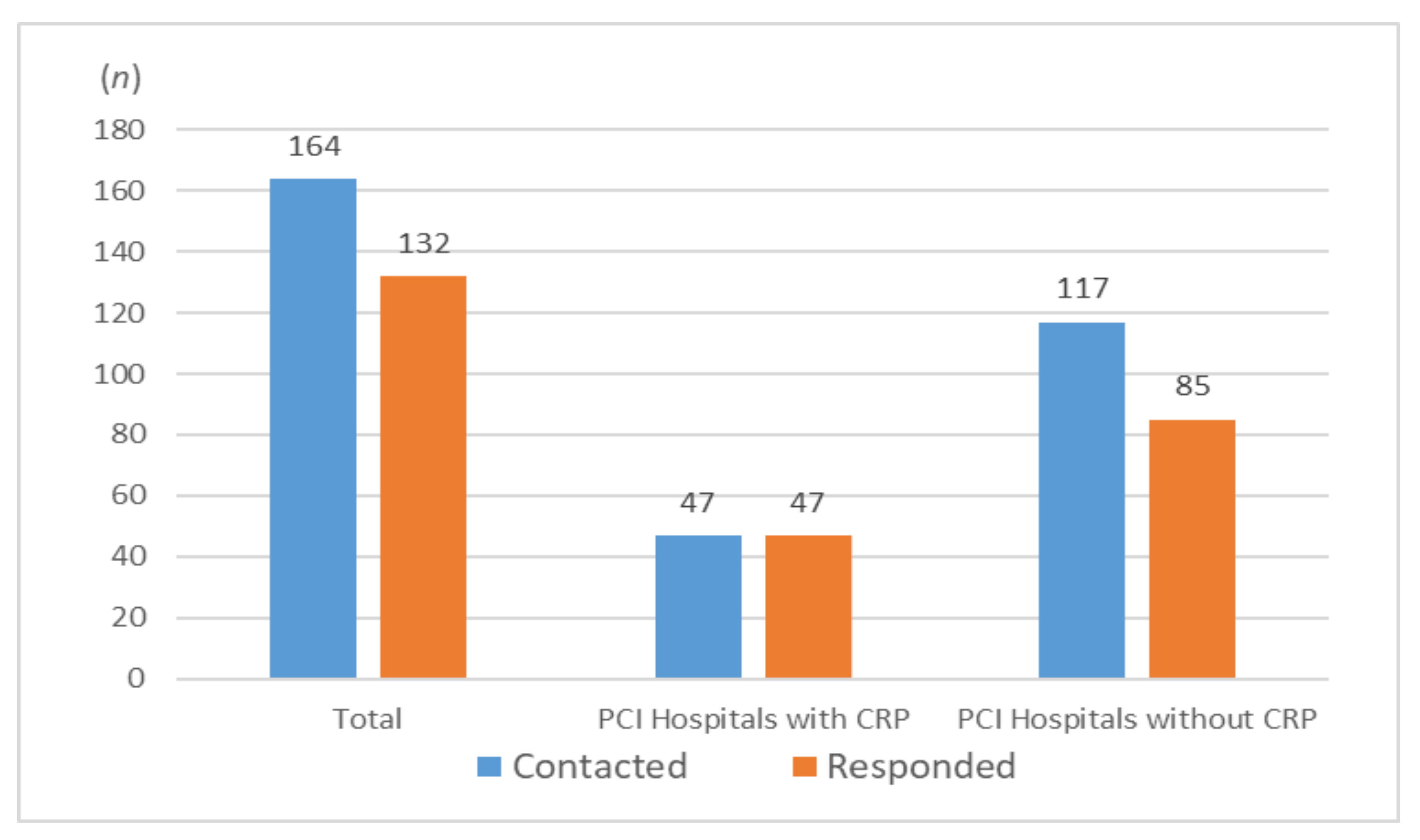
- Of the 164 hospitals, 132 responded (response rate: 80.5%). All 47 hospitals with CRP responded (100%), whereas of the 117 hospitals without CRP, 85 responded (72.6%) (Figure 1).
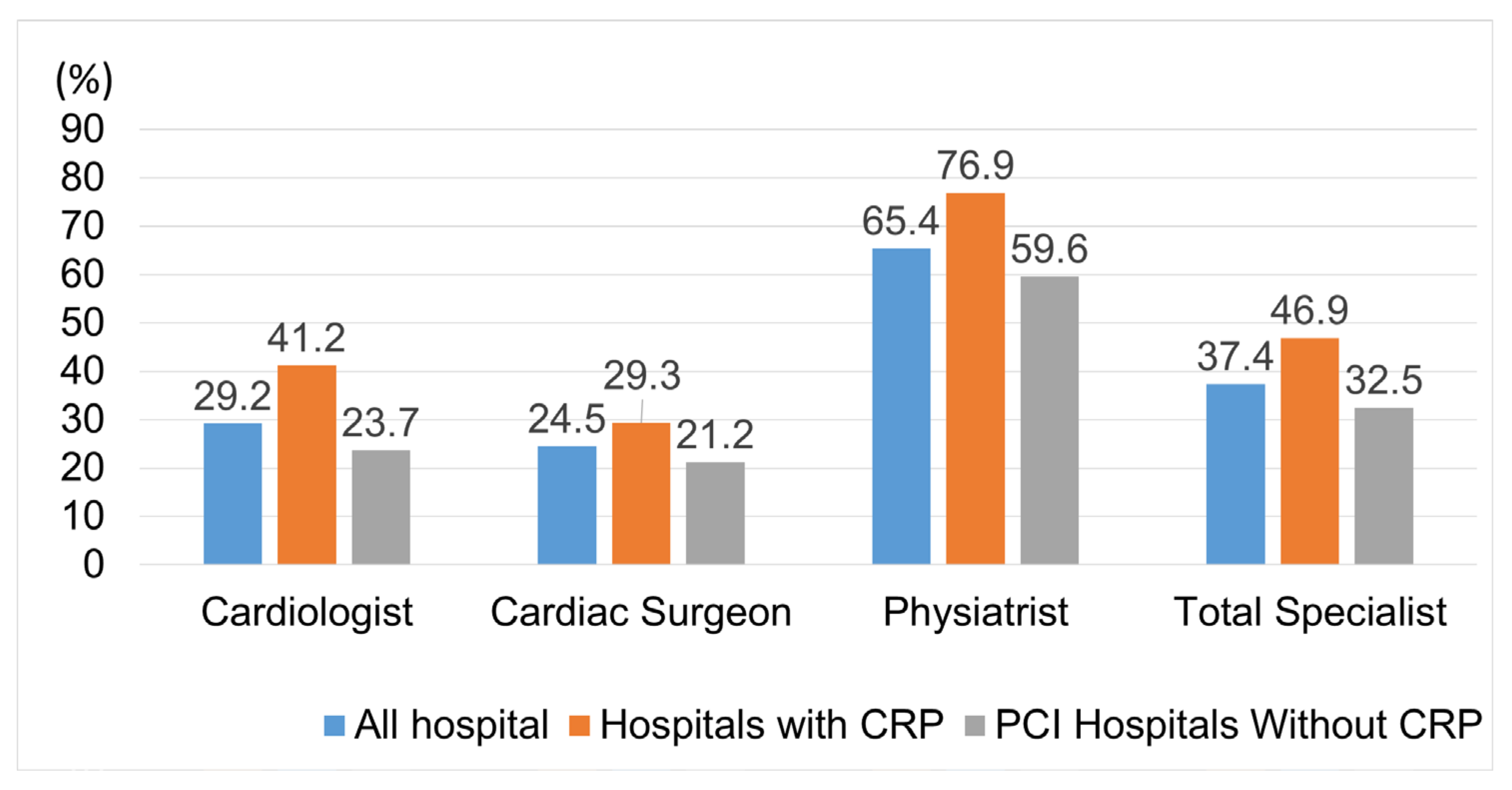
- Of the 607 specialists, 227 responded (response rate: 36.9%). The response rates according to specialty were as follows: cardiologists (28.9%), cardiac surgeons (24.5%), and physiatrists (64.1%) (Figure 2).
3.3. Barriers Based on the Results of the Survey
- All items except for patient referral were the differences between hospitals with or without CRP. Moreover, the transportation (mode and distance) items, unlike other items, were a barrier that was considered more serious in hospitals with CRP. Whereas specialists in hospitals without CRP considered all the items as barriers, especially the items related to equipment, space, workforce, and budget, which were more serious barriers. (Table 3).
- Differences between rehabilitation medicine specialists and other specialists in hospitals with CRP were seen in the following items: Lack of Equipment for CRP, Lack of Budget for CRP, Patient Transportation: Mode and Distance (Table 4).
- Differences between rehabilitation medicine specialists and other specialists in hospitals without CRP were seen in the following items: Lack of Equipment for CRP and Lack of Space for CRP (Table 5).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [Green Version]
- Korean Statistical Infarmation Service. Causes of Death Statistics [Internet] Daejeon: National Statistical Offic. 2020. Available online: https://kosis.kr/eng/statisticsList (accessed on 1 January 2020).
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2020, 23, 1715–1733. [Google Scholar] [CrossRef] [PubMed]
- Turk-Adawi, K.; Supervia, M.; Lopez-Jimenez, F.; Pesah, E.; Ding, R.; Britto, R.R.; Bjarnason-Wehrens, B.; Derman, W.; Abreu, A.; Babu, A.S.; et al. Cardiac Rehabilitation Availability and Density around the Globe. EClinicalMedicine 2019, 13, 31–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turk-Adawi, K.I.; Grace, S.L. Narrative review comparing the benefits of and participation in cardiac rehabilitation in high-, middle- and low-income countries. Heart Lung Circ. 2015, 24, 510–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chindhy, S.; Taub, P.R.; Lavie, C.J.; Shen, J. Current challenges in cardiac rehabilitation: Strategies to overcome social factors and attendance barriers. Expert Rev. Cardiovasc. Ther. 2020, 18, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Sung, J.; Lee, J.H.; Kim, W.S.; Lee, G.J.; Jee, S.; Jung, I.Y.; Rah, U.W.; Kim, B.O.; Choi, K.H.; et al. Clinical Practice Guideline for Cardiac Rehabilitation in Korea. Ann. Rehabil. Med. 2019, 43, 355–443. [Google Scholar] [CrossRef] [PubMed]
- Ades, P.A.; Keteyian, S.J.; Wright, J.S.; Hamm, L.F.; Lui, K.; Newlin, K.; Shepard, D.S.; Thomas, R.J. Increasing Cardiac Rehabilitation Participation From 20% to 70%: A Road Map From the Million Hearts Cardiac Rehabilitation Collaborative. Mayo Clin. Proc. 2017, 92, 234–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Ro, J.S.; Kim, Y.; Leigh, J.H.; Kim, W.S. Underutilization of Hospital-based Cardiac Rehabilitation after Acute Myocardial Infarction in Korea. J. Korean Med. Sci. 2020, 35, e262. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Choi, I.; Cho, S.; Han, J.Y.; Kim, A.R.; Kim, W.S.; Jee, S.; Lee, J.H.; Joo, M.C.; Bang, H.J.; et al. Cardiac rehabilitation and 5-year mortality after acute myocardial infarction. Report from 11 tertiary hospitals in Korea (ETHIK Study). Eur. J. Phys. Rehabil. Med. 2020, 56, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Sung, J.; Han, J.Y.; Jee, S.; Lee, J.W.; Lee, J.H.; Kim, W.S.; Bang, H.J.; Baek, S.; Joa, K.L.; et al. Current Status of Cardiac Rehabilitation in the Regional Cardiocerebrovascular Centers in Korea. J. Clin. Med. 2021, 10, 5079. [Google Scholar] [CrossRef] [PubMed]
- Park, M.S.; Lee, S.; Ahn, T.; Kim, D.; Jung, M.H.; Choi, J.H.; Han, S.; Ryu, K.H.; Kim, E.J. Current status of cardiac rehabilitation among representative hospitals treating acute myocardial infarction in South Korea. PLoS ONE 2021, 16, e0261072. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Question: If Cardiac Rehabilitation Programs (CRP) Are Not Actively Used in Your Respective Hospitals, What Do You Think Would Be the Barriers and Factors for Cardiac Rehabilitation? (Select One for Each Item) | |||||
|---|---|---|---|---|---|
| Not at All 1 Point | Not Really 2 Points | Neutral 3 Points | Some-What 4 Points | Very Much 5 Points | |
| (1) Lack of Patient Referrals /Lack of Awareness among Specialists | |||||
| (2) Lack of Equipment for CRP | |||||
| (3) Lack of Space for CRP | |||||
| (4) Lack of Workforce for CRP | |||||
| (5) Lack of Budget for CRP | |||||
| (6) Insufficient Insurance/ High Costs | |||||
| (7) Patient Transportation: Mode and Distance | |||||
| (8) Additional Opinions | |||||
| Hospitals with CRP (N = 47) | Hospitals without CRP (N = 85) | |
|---|---|---|
| Performing of Procedure or Surgery (N) | ||
| Percutaneous Coronary Interventions (PCI) | 47 | 85 |
| Coronary Artery Bypass Grafting (CABG) | 42 | 46 |
| Pecutaneous Valve Implantation | 42 | 31 |
| Valvuloplasty | 43 | 42 |
| Endovascular Repair | 45 | 49 |
| Permanent Pacemaker | 46 | 67 |
| Left Ventricular Assis Device (LVAD) | 20 | 11 |
| Annual Number of PCI (N) | ||
| <100 | 0 | 11 |
| 100~300 | 6 | 24 |
| 300~500 | 8 | 5 |
| 500~700 | 6 | 10 |
| 700~900 | 8 | 1 |
| 900~1100 | 6 | 5 |
| >1100 | 7 | 1 |
| unanswered | 6 | 28 |
| Duration of the CRP (N) | ||
| 0~1 year | 3 | 85 |
| 1~3 year | 10 | 0 |
| 3~6 year | 15 | 0 |
| 6~9 year | 5 | 0 |
| 9~12 year | 9 | 0 |
| >12 year | 4 | 0 |
| unanswered | 1 | 0 |
| No. of Responded Specialist (N) | 97 | 130 |
| Interventional Cardiologist | 40 | 50 |
| Cardiac Surgeon | 17 | 18 |
| Physiatrist | 40 | 62 |
| Respondent in Hospitals with CRP (N = 97) | Respondent in Hospitals without CRP (N = 130) | p * | |
|---|---|---|---|
| Lack of Patient Referrals/Awareness among Physicians | 3.11 ± 1.19 | 3.22 ± 1.09 | 0.502 |
| Lack of Equipment for CRP | 2.14 ± 1.02 | 4.32 ± 0.78 | 0.000 * |
| Lack of Space for CRP | 2.33 ± 1.13 | 4.29 ± 0.81 | 0.000 * |
| Lack of Workforce for CRP | 2.93 ± 1.16 | 4.40 ± 0.69 | 0.000 * |
| Lack of Budget for CRP | 2.87 ± 1.17 | 4.31 ± 0.72 | 0.000 * |
| Insufficient Insurance/High Costs | 3.42 ± 0.90 | 3.80 ± 0.97 | 0.003 * |
| Patient Transportation: Mode and Distance | 3.77 ± 1.01 | 3.18 ± 0.98 | 0.000 * |
| Hospitals with CRP | Physiatrists (N = 40) | Others Specialists (N = 57) | p * |
|---|---|---|---|
| Lack of Patient Referrals/Awareness among Physicians | 3.21 ± 1.22 | 2.97 ± 1.15 | 0.471 |
| Lack of Equipment for CRP | 1.63 ± 0.91 | 2.47 ± 0.92 | 0.003 * |
| Lack of Space for CRP | 1.96 ± 1.17 | 2.50 ± 1.02 | 0.086 |
| Lack of Workforce for CRP | 2.75 ± 1.18 | 3.23 ± 1.06 | 0.128 |
| Lack of Budget for CRP | 2.54 ± 1.20 | 3.17 ± 1.03 | 0.039 * |
| Insufficient Insurance/High Cost | 3.46 ± 0.85 | 3.37 ± 0.91 | 0.666 |
| Patient Transportation Mode and Distance | 4.25 ± 0.82 | 3.50 ± 1.02 | 0.004 * |
| Hospitals without CRP | Physiatrists (N = 62) | Others Specialists (N = 68) | p * |
|---|---|---|---|
| Lack of Patient Referrals/Awareness among Physicians | 3.26 ± 1.11 | 3.18 ± 1.05 | 0.670 |
| Lack of Equipment for CRP | 4.48 ± 0.59 | 4.18 ± 0.89 | 0.024 * |
| Lack of Space for CRP | 4.48 ± 0.68 | 4.12 ± 0.85 | 0.010 * |
| Lack of Workforce for CRP | 4.48 ± 0.67 | 4.32 ± 0.66 | 0.186 |
| Lack of Budget for CRP | 4.37 ± 0.77 | 4.25 ± 0.66 | 0.344 |
| Insufficient Insurance/High Costs | 3.73 ± 1.02 | 3.87 ± 0.91 | 0.406 |
| Patient Transportation: Mode and Distance | 3.10 ± 1.02 | 3.26 ± 0.91 | 0.330 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.; Sung, J.; Han, J.-Y.; Jee, S.; Lee, J.W.; Lee, J.H.; Kim, W.-S.; Bang, H.J.; Baek, S.; Joa, K.-L.; et al. A Comparison of Barrier Factors between Hospitals with and without Cardiac Rehabilitation Programs in Korea: A Nation-Wide Survey Research. J. Clin. Med. 2022, 11, 2560. https://doi.org/10.3390/jcm11092560
Kim C, Sung J, Han J-Y, Jee S, Lee JW, Lee JH, Kim W-S, Bang HJ, Baek S, Joa K-L, et al. A Comparison of Barrier Factors between Hospitals with and without Cardiac Rehabilitation Programs in Korea: A Nation-Wide Survey Research. Journal of Clinical Medicine. 2022; 11(9):2560. https://doi.org/10.3390/jcm11092560
Chicago/Turabian StyleKim, Chul, Jidong Sung, Jae-Young Han, Sungju Jee, Jang Woo Lee, Jong Hwa Lee, Won-Seok Kim, Heui Je Bang, Sora Baek, Kyung-Lim Joa, and et al. 2022. "A Comparison of Barrier Factors between Hospitals with and without Cardiac Rehabilitation Programs in Korea: A Nation-Wide Survey Research" Journal of Clinical Medicine 11, no. 9: 2560. https://doi.org/10.3390/jcm11092560
APA StyleKim, C., Sung, J., Han, J.-Y., Jee, S., Lee, J. W., Lee, J. H., Kim, W.-S., Bang, H. J., Baek, S., Joa, K.-L., Kim, A. R., Lee, S. Y., Kim, J., Kim, C. R., & Kwon, O. P. (2022). A Comparison of Barrier Factors between Hospitals with and without Cardiac Rehabilitation Programs in Korea: A Nation-Wide Survey Research. Journal of Clinical Medicine, 11(9), 2560. https://doi.org/10.3390/jcm11092560