
PRISM (Pictorial Representation of Illness and Self-Measure) as Visual Tool to Support Oral Health Education Prior to Endoprosthetic Joint Replacement—A Novel Approach in Dentistry

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Oral Examination
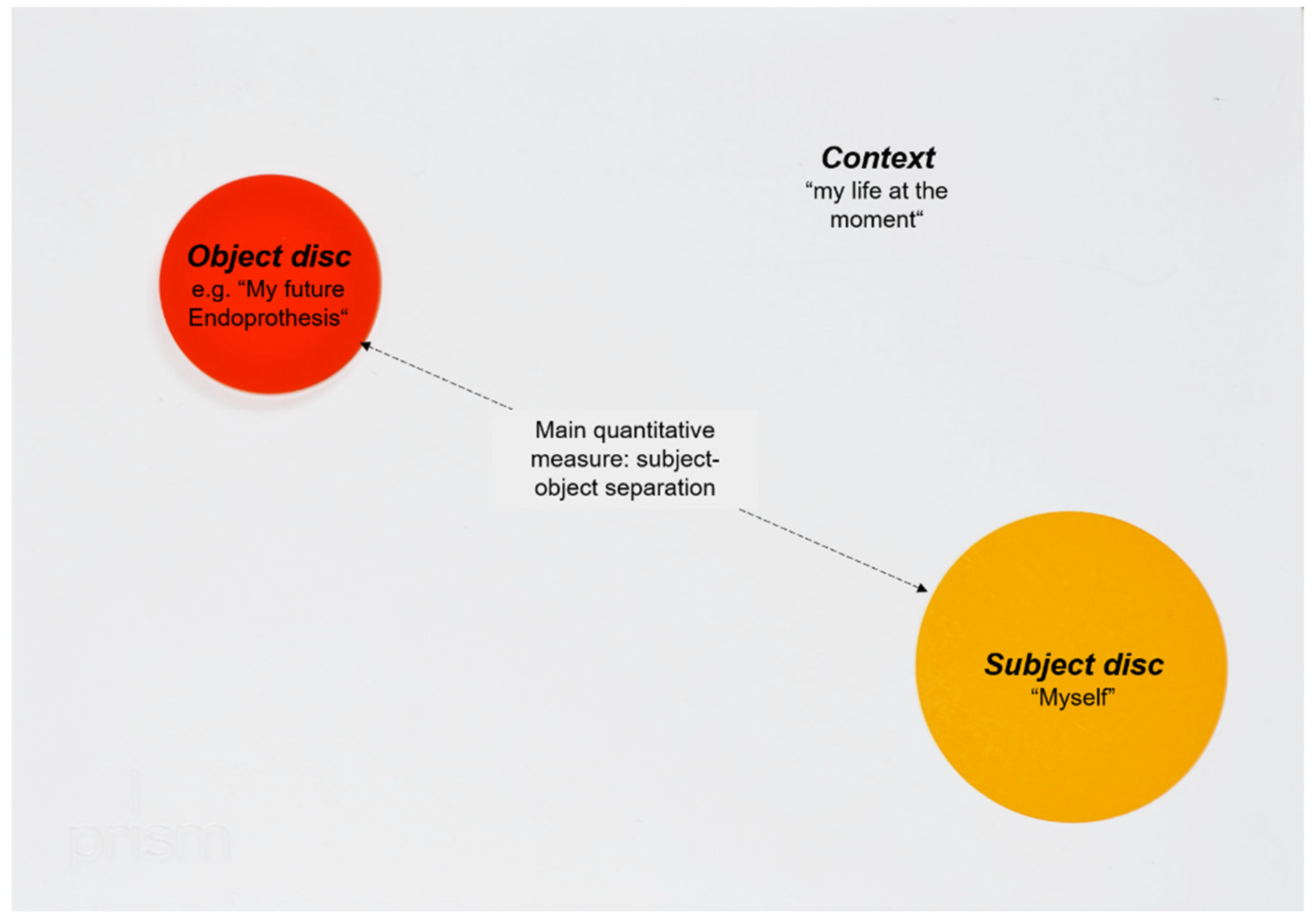
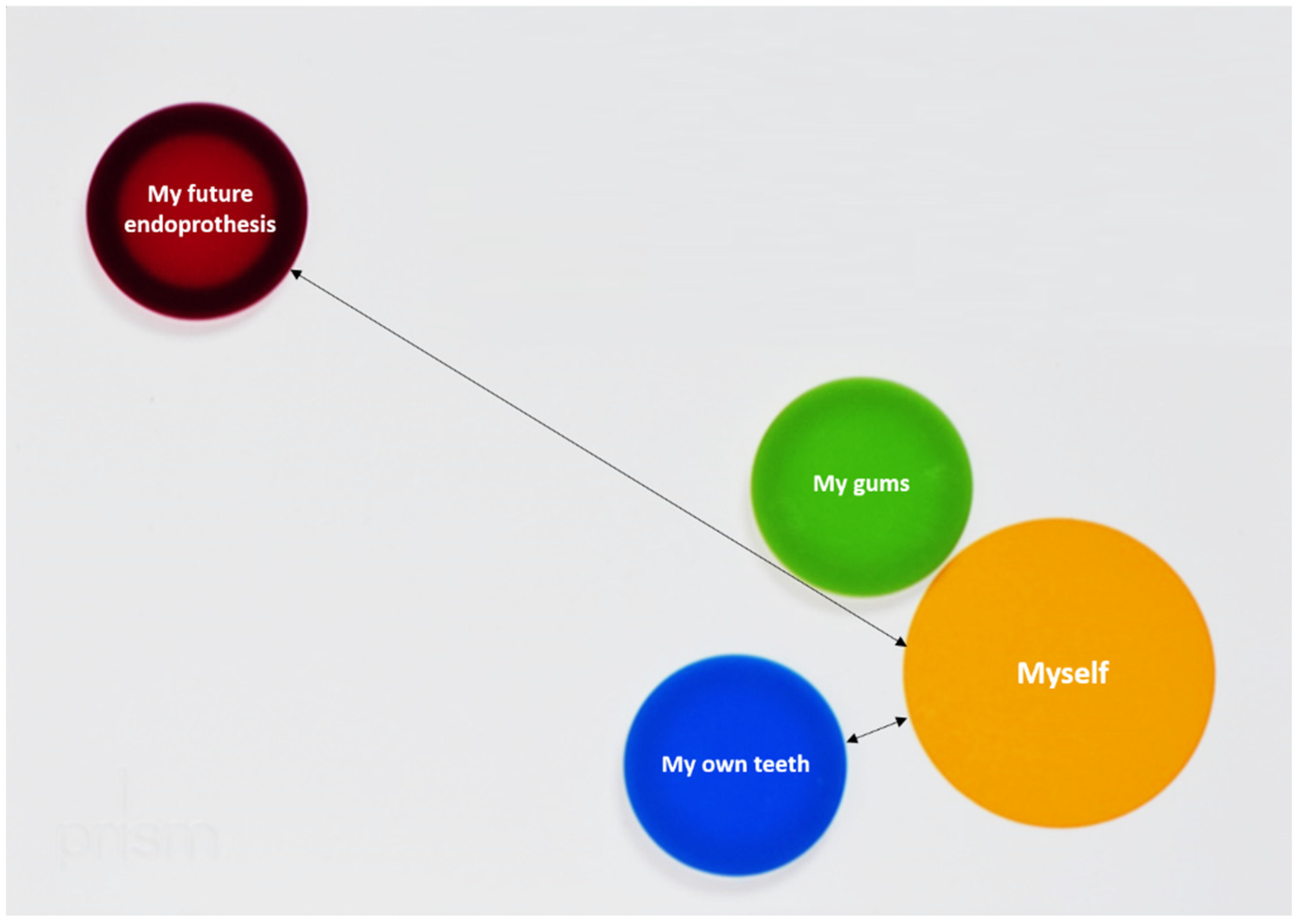
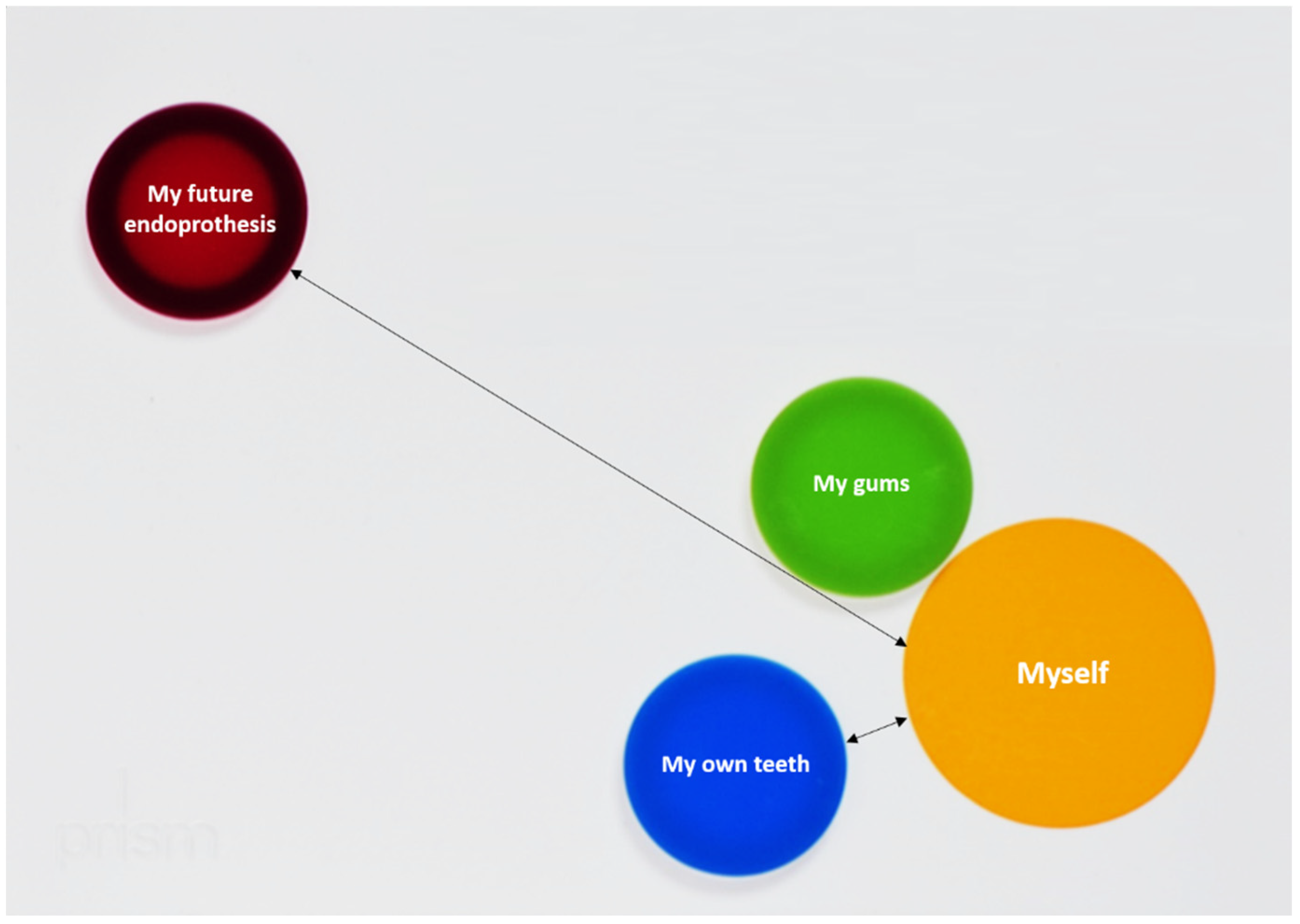
2.3. PRISM and Verbal Briefing
2.4. Questionnaires
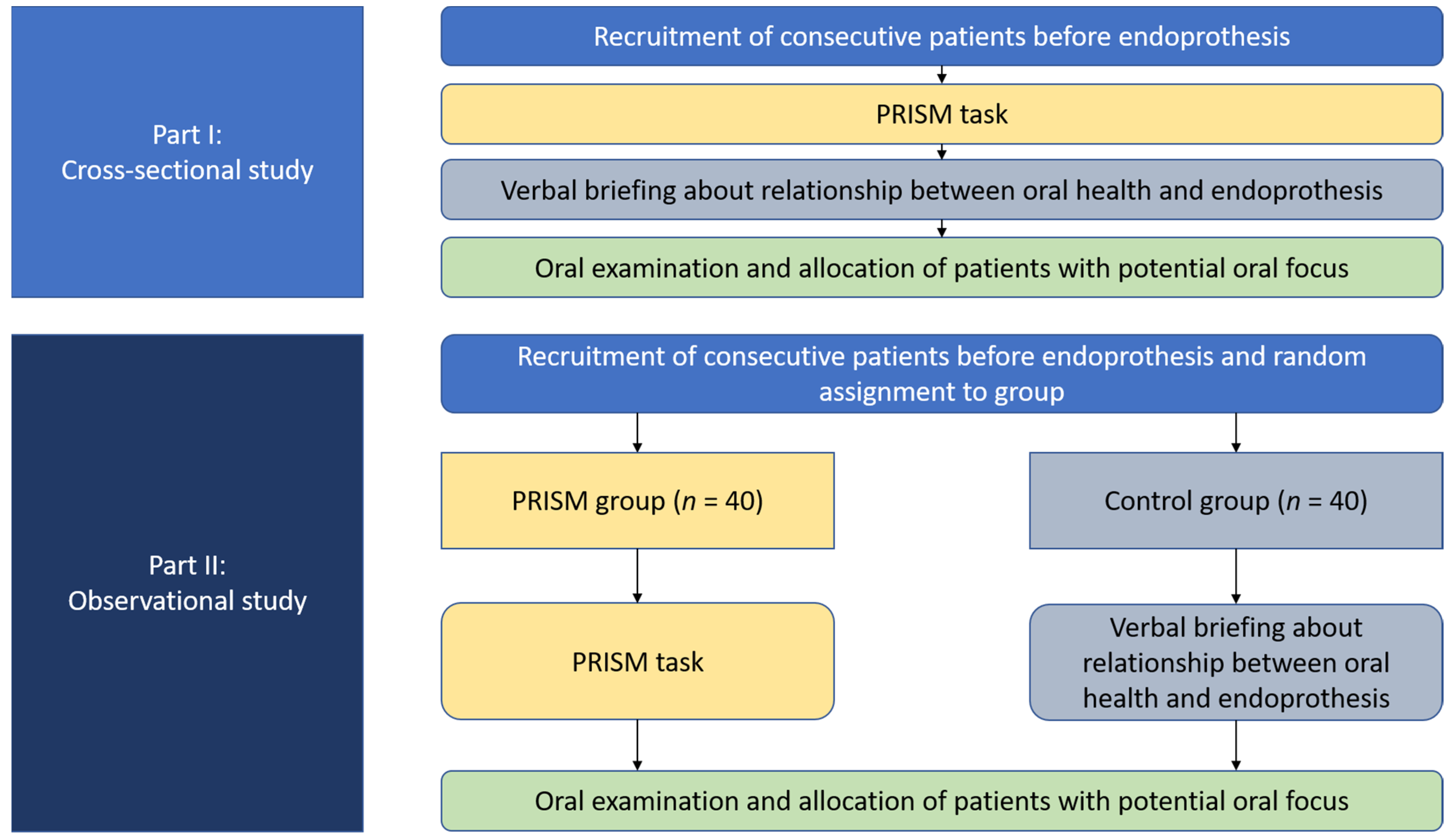
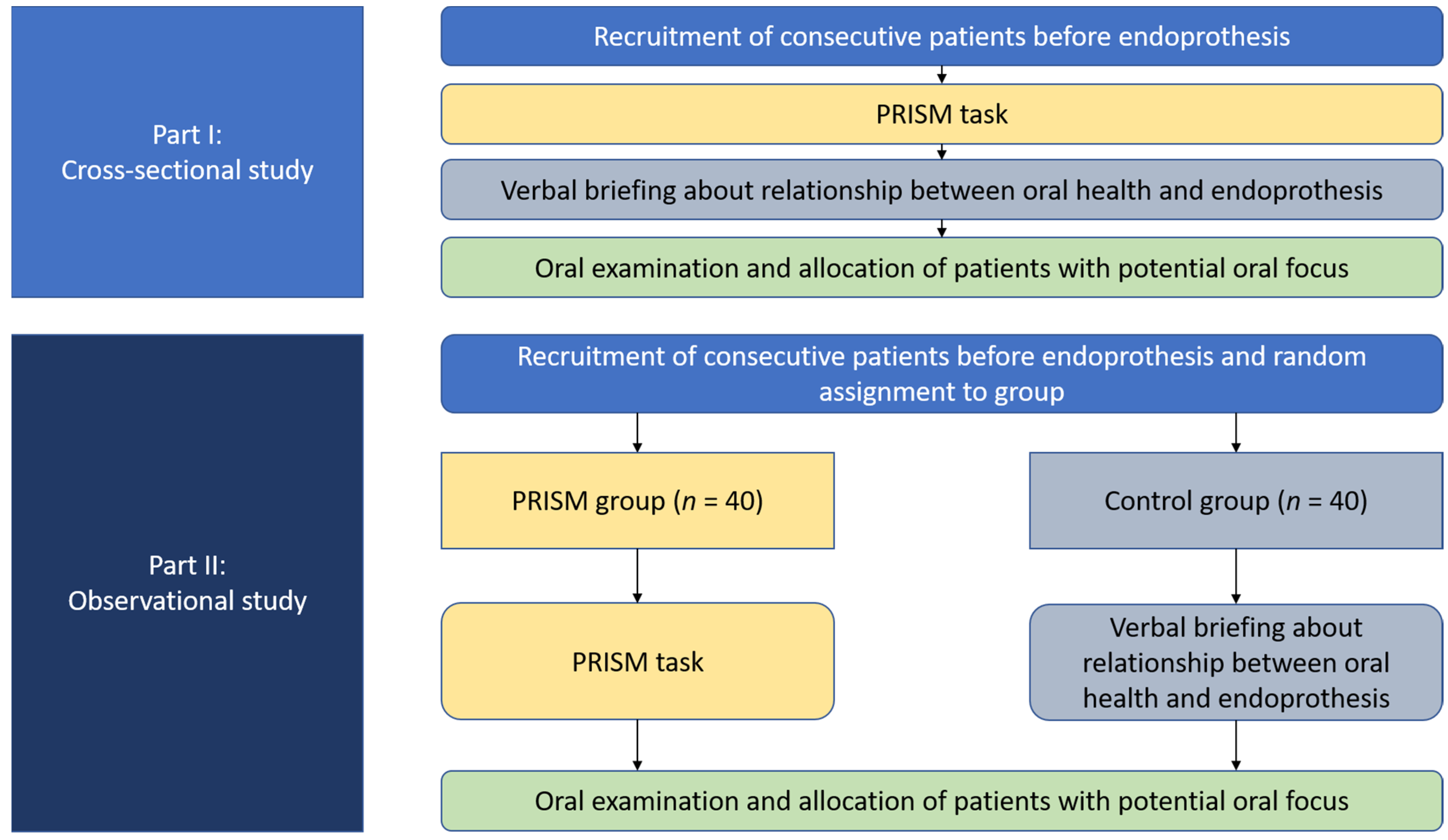
2.5. Study Flow
2.6. Statistical Analysis
3. Results
3.1. Part I—Cross-Sectional Study (n = 122)
3.1.1. Patients
3.1.2. PRISM Findings
3.2. Part II—Interventional Study (n = 80)
3.2.1. Patients
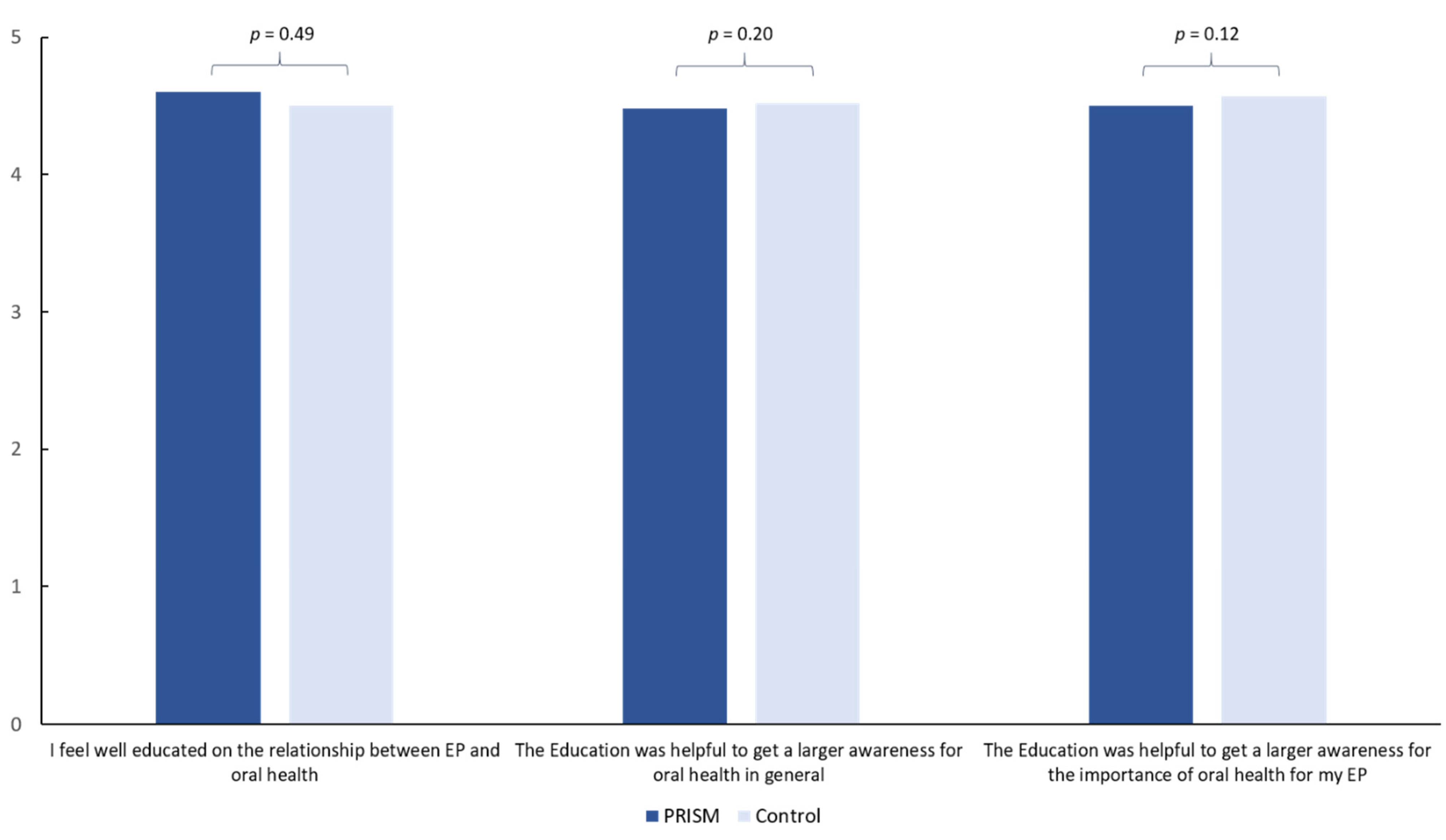
3.2.2. Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akl, S.; Ranatunga, M.; Long, S.; Jennings, E.; Nimmo, A. A systematic review investigating patient knowledge and awareness on the association between oral health and their systemic condition. BMC Public Health 2021, 21, 2077. [Google Scholar] [CrossRef] [PubMed]
- Kane, S.F. The effects of oral health on systemic health. Gen. Dent. 2017, 65, 30–34. [Google Scholar] [PubMed]
- Poudel, P.; Griffiths, R.; Wong, V.W.; Arora, A.; Flack, J.R.; Khoo, C.L.; George, A. Oral health knowledge, attitudes and care practices of people with diabetes: A systematic review. BMC Public Health 2018, 18, 577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqi, A.; Zafar, S.; Sharma, A.; Quaranta, A. Diabetic patients’ knowledge of the bidirectional link: Are dental health care professionals effectively conveying the message? Aust. Dent. J. 2019, 64, 312–326. [Google Scholar] [CrossRef]
- Gambhir, R.S.; Nirola, A.; Gupta, T.; Sekhon, T.S.; Anand, S. Oral health knowledge and awareness among pregnant women in India: A systematic review. J. Indian Soc. Periodontol. 2015, 19, 612–617. [Google Scholar] [CrossRef]
- Albano, M.G.; d’Ivernois, J.F.; de Andrade, V.; Levy, G. Patient education in dental medicine: A review of the literature. Eur. J. Dent. Educ. 2019, 23, 110–118. [Google Scholar] [CrossRef]
- Sensky, T.; Büchi, S. PRISM, a Novel Visual Metaphor Measuring Personally Salient Appraisals, Attitudes and Decision-Making: Qualitative Evidence Synthesis. PLoS ONE 2016, 11, e0156284. [Google Scholar] [CrossRef] [Green Version]
- Büchi, S.; Sensky, T. PRISM: Pictorial Representation of Illness and Self Measure. A brief nonverbal measure of illness impact and therapeutic aid in psychosomatic medicine. Psychosomatics 1999, 40, 314–320. [Google Scholar] [CrossRef]
- Büchi, S.; Buddeberg, C.; Klaghofer, R.; Russi, E.W.; Brändli, O.; Schlösser, C.; Stoll, T.; Villiger, P.M.; Sensky, T. Preliminary validation of PRISM (Pictorial Representation of Illness and Self Measure)—A brief method to assess suffering. Psychother Psychosom. 2002, 71, 333–341. [Google Scholar] [CrossRef]
- Reinhardt, S.; Bischof, G.; Grothues, J.; John, U.; Rumpf, H.J. Performance of the pictorial representation of illness and self measure in individuals with alcohol dependence, alcohol abuse or at-risk drinking. Psychother Psychosom. 2006, 75, 249–256. [Google Scholar] [CrossRef]
- Zimmermann, R.; Hattendorf, J.; Blum, J.; Nüesch, R.; Hatz, C. Risk perception of travelers to tropical and subtropical countries visiting a swiss travel health center. J. Travel Med. 2013, 20, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.; Weksler, N.; Gidron, Y.; Heldman, E.; Gurski, E.; Smith, O.R.; Gurman, G.M. Do waking salivary cortisol levels correlate with anesthesiologist’s job involvement? J. Clin. Monit. Comput. 2012, 26, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Niedermann, K.; de Bie, R.A.; Kubli, R.; Ciurea, A.; Steurer-Stey, C.; Villiger, P.M.; Büchi, S. Effectiveness of individual resource-oriented joint protection education in people with rheumatoid arthritis. A randomized controlled trial. Patient Educ. Couns. 2011, 82, 42–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira, A.I.; Mendes, L.; Pereira, J.A. Is there scientific evidence to support antibiotic prophylaxis in patients with periodontal disease as a means to decrease the risk of prosthetic joint infections? A systematic review. Int. Orthop. 2020, 44, 231–236. [Google Scholar] [CrossRef]
- Olson, L.B.; Turner, D.J.; Cox, G.M.; Hostler, C.J. Streptococcus salivarius Prosthetic Joint Infection following Dental Cleaning despite Antibiotic Prophylaxis. Case Rep. Infect. Dis. 2019, 2019, 8109280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skaar, D.D.; O’Connor, H.; Hodges, J.S.; Michalowicz, B.S. Dental procedures and subsequent prosthetic joint infections: Findings from the Medicare Current Beneficiary Survey. J. Am. Dent. Assoc. 2011, 142, 1343–1351. [Google Scholar] [CrossRef]
- Vuorinen, M.; Mäkinen, T.; Rantasalo, M.; Leskinen, J.; Välimaa, H.; Huotari, K. Incidence and risk factors for dental pathology in patients planned for elective total hip or knee arthroplasty. Scand. J. Surg. 2019, 108, 338–342. [Google Scholar] [CrossRef] [Green Version]
- Kapadia, B.H.; Berg, R.A.; Daley, J.A.; Fritz, J.; Bhave, A.; Mont, M.A. Periprosthetic joint infection. Lancet. 2016, 387, 386–394. [Google Scholar] [CrossRef]
- Diamanti-Kipioti, A.; Papapanou, T.N.; Moraitaki-Zamitsai, A.; Lindhe, J.; Mitsis, F. Comparative estimation of periodontal conditions by means of different index systems. J. Clin. Periodontol. 1993, 20, 656. [Google Scholar] [CrossRef]
- Meyle, J.; Jepsen, S. The Periodontal Screening-Index (PSI). Parodontologie 2000, 11, 17–21. (In German) [Google Scholar]
- Streffer, M.L.; Büchi, S.; Mörgeli, H.; Galli, U.; Ettlin, D. PRISM (pictorial representation of illness and self measure): A novel visual instrument to assess pain and suffering in orofacial pain patients. J. Orofac. Pain 2009, 23, 140–146. [Google Scholar] [PubMed]
- Jordan, R.A.; Micheelis, W. The Fifth German Oral Health Study (DMS V); Institut der Deutschen Zahnärzte (Hrsg.), (IDZ Materialienreihe Band 35); Deutscher Zahnärzte Verlag DÄV: Köln, Germany, 2016. (In German) [Google Scholar]
- Schmalz, G.; Garbade, J.; Kollmar, O.; Ziebolz, D. Does oral health-related quality of life of patients after solid organ transplantation indicate a response shift? Results of a systematic review. BMC Oral Health 2020, 20, 356. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.B.; Botelho, J.; Machado, V.; Zehra, S.A.; Mendes, J.J.; Ciurtin, C.; Orlandi, M.; D’Aiuto, F. Is there a bidirectional association between rheumatoid arthritis and periodontitis? A systematic review and meta-analysis. Semin. Arthritis Rheum. 2020, 50, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Témoin, S.; Chakaki, A.; Askari, A.; El-Halaby, A.; Fitzgerald, S.; Marcus, R.E.; Han, Y.W.; Bissada, N.F. Identification of oral bacterial DNA in synovial fluid of patients with arthritis with native and failed prosthetic joints. J. Clin. Rheumatol. 2012, 18, 117–121. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez Duque, J.C.; Galindo Rubín, P.; González Humara, B.; Quesada Sanz, A.A.; Busta Val-lina, M.B.; Fernández-Sampedro, M. Fusobacterium nucleatum prosthetic hip infection: Case report and review of the literature of unusual anaerobic prosthetic joint infection. Anaerobe 2018, 54, 75–82. [Google Scholar] [CrossRef]
- Rakow, A.; Perka, C.; Trampuz, A.; Renz, N. Origin and characteristics of haematogenous periprosthetic joint infection. Clin. Microbiol. Infect. 2019, 25, 845–850. [Google Scholar] [CrossRef]
- Lima-Verde, A.C.; Pozza, D.H.; Rodrigues, L.L.; Velly, A.M.; Guimarães, A.S. Cross-cultural adaptation and validation for Portuguese (Brazilian) of the pictorial representation of illness and self measure instrument in orofacial pain patients. J. Orofac. Pain. 2013, 27, 271–275. [Google Scholar] [CrossRef] [Green Version]
- Fabrikant, S.I.; Montello, D.R. The effect of instructions on distance and similarity judgements in information spatializations. Int. J. Geogr. Inf. Sci. 2008, 22, 463–478. [Google Scholar] [CrossRef]
- Wilson, D.; Carston, R. Metaphor, Relevance and the Emergent Property Issue. Mind Lang. 2006, 21, 404–433. [Google Scholar] [CrossRef]
- Tendahl, M.; Gibbs, R.W.J. Complementary perspectives on metaphor: Cognitive linguistics and relevance theory. J. Pragmat. 2008, 40, 1823–1864. [Google Scholar] [CrossRef] [Green Version]
- Mollborn, S.; Lawrence, E.M.; Hummer, R.A. A gender framework for understanding health lifestyles. Soc. Sci. Med. 2020, 265, 113182. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, L.G. Dental patient education: Self-care to healthy human development. Patient Educ. Couns. 1990, 15, 65–71. [Google Scholar] [CrossRef]
- Lam, O.L.; Zhang, W.; Samaranayake, L.P.; Li, L.S.; McGrath, C. A systematic review of the effectiveness of oral health promotion activities among patients with cardiovascular disease. Int. J. Cardiol. 2011, 151, 261–267. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients before Implantation of EP (n = 122) | |
|---|---|
| Gender (female in % (n)) | 46.7% (57) |
| Age in years (mv ± sd) | 66.38 ± 11,42 |
| Number of remaining teeth (mv ± sd) | 18.66 ± 8.42 |
| Dental treatment need (% (n)) | 24.6% (30) |
| Periodontal treatment need (% (n)) | 86.1% (105) |
| Presence of potential dental focus (% (n)) | 43.4% (53) |
| Patients before Implantation of EP (n = 122) | ||
|---|---|---|
| Importance of healthy teeth (in mm, mv ± sd (median, range)) | 11.0 ± 33.9 (0, 0–170) | |
| Importance of healthy gums (in mm, mv ± sd (median, range)) | 11.8 ± 34.4 (0, 0–169) | |
| Importance of consulting dentist (in mm, mv ± sd (median, range)) | 13.4 ± 42.0 (0, 0–209) | |
| Cluster relationship of EP and teeth (% (n)) | Same importance of EP and teeth | 76.2% (93) |
| Teeth more important than EP | 11.5% (14) | |
| EP more important than teeth | 12.3% (15) | |
| Importance of Healthy Teeth | Importance of Healthy Gums | Importance of Consulting the Dentist | Relationship EP and Teeth | |
|---|---|---|---|---|
| Age | 0.76 a | 0.68 a | 0.64 a | 0.16 b |
| Gender | 0.68 c | 0.57 c | 0.09 c | 0.02 b |
| Number of teeth | 0.04 a | 0.41 a | 0.29 a | 0.26 b |
| Dental treatment need | 0.46 c | 0.19 c | 0.56 c | 0.56 b |
| Periodontal treatment need | 0.64 c | 0.45 c | 0.12 c | 0.76 b |
| Potential dental focus | 0.62 a | 0.74 a | 0.61 a | 0.86 b |
| PRISM (n = 40) | Control (n = 40) | p-Value | |
|---|---|---|---|
| Gender (female in % (n)) | 55.0% (22) | 47.5% (19) | 0.67 |
| Age in years (mv ± sd) | 69.78 ± 11.02 | 70.02 ± 11.04 | 0.87 |
| Number of remaining teeth (mv ± sd) | 21.10 ± 8.09 | 19.10 ± 8.63 | 0.29 |
| Dental treatment need (% (n)) | 42.5% (17) | 45.0% (18) | 0.99 |
| Periodontal treatment need (% (n)) | 80.0% (32) | 75.0% (30) | 0.79 |
| Presence of a potential dental focus (% (n)) | 30.0% (12) | 30.0% (12) | 0.99 |
| Question | PRISM (n = 40) | Control (n = 40) | ||||
|---|---|---|---|---|---|---|
| Before | After | p-Value | Before | After | p-Value | |
| I perceive EP as a foreign body | 1.35 ± 1.83 | 0.58 ± 1.26 | 0.01 | 1.35 ± 1.76 | 1.10 ± 1.69 | 0.36 |
| Oral health has high relevance in my life | 4.28 ± 1.41 | 4.55 ± 1.15 | 0.12 | 4.50 ± 1.15 | 4.70 ± 0.65 | 0.34 |
| My oral health status is a problem | 1.20 ± 1.62 | 0.88 ± 1.40 | 0.23 | 1.42 ± 1.95 | 1.35 ± 1.94 | 0.76 |
| My teeth are a disruptive factor | 0.59 ± 1.41 | 0.34 ± 0.94 | 0.23 | 0.79 ± 1.82 | 0.72 ± 1.62 | 0.81 |
| I see a relationship between EP and teeth | 1.60 ± 1.86 | 4.20 ± 1.24 | <0.01 | 1.33 ± 1.83 | 4.43 ± 1.24 | <0.01 |
| I see a relationship between EP and gums | 1.50 ± 1.88 | 4.05 ± 1.41 | <0.01 | 1.05 ± 1.75 | 4.43 ± 1.15 | <0.01 |
| I see a relationship between EP and dental consultations | 2.18 ± 2.22 | 4.18 ± 1.57 | <0.01 | 1.85 ± 2.09 | 4.23 ± 1.37 | <0.01 |
| Since I need an EP, I performed oral hygiene less intensively | 0.65 ± 1.41 | 0.65 ± 1.37 | 0.99 | 0.40 ± 1.19 | 0.73 ± 1.54 | 0.19 |
| Since I need an EP, I visited the dentist less often for prevention | 0.68 ± 1.56 | 0.77 ± 1.51 | 0.72 | 1.05 ± 1.96 | 1.20 ± 1.95 | 0.82 |
| Since I need an EP, I have less energy to perform oral hygiene | 0.37 ± 1.13 | 0.70 ± 1.44 | 0.12 | 0.63 ± 1.35 | 1.05 ± 1.80 | 0.13 |
| Since I need an EP, oral health has a lower importance in my life | 0.60 ± 1.39 | 0.85 ± 1.67 | 0.29 | 0.63 ± 1.53 | 0.93 ± 1.83 | 0.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmalz, G.; Schmidt, L.; Haak, R.; Büchi, S.; Goralski, S.; Roth, A.; Ziebolz, D. PRISM (Pictorial Representation of Illness and Self-Measure) as Visual Tool to Support Oral Health Education Prior to Endoprosthetic Joint Replacement—A Novel Approach in Dentistry. J. Clin. Med. 2022, 11, 2508. https://doi.org/10.3390/jcm11092508
Schmalz G, Schmidt L, Haak R, Büchi S, Goralski S, Roth A, Ziebolz D. PRISM (Pictorial Representation of Illness and Self-Measure) as Visual Tool to Support Oral Health Education Prior to Endoprosthetic Joint Replacement—A Novel Approach in Dentistry. Journal of Clinical Medicine. 2022; 11(9):2508. https://doi.org/10.3390/jcm11092508
Chicago/Turabian StyleSchmalz, Gerhard, Laura Schmidt, Rainer Haak, Stefan Büchi, Szymon Goralski, Andreas Roth, and Dirk Ziebolz. 2022. "PRISM (Pictorial Representation of Illness and Self-Measure) as Visual Tool to Support Oral Health Education Prior to Endoprosthetic Joint Replacement—A Novel Approach in Dentistry" Journal of Clinical Medicine 11, no. 9: 2508. https://doi.org/10.3390/jcm11092508
APA StyleSchmalz, G., Schmidt, L., Haak, R., Büchi, S., Goralski, S., Roth, A., & Ziebolz, D. (2022). PRISM (Pictorial Representation of Illness and Self-Measure) as Visual Tool to Support Oral Health Education Prior to Endoprosthetic Joint Replacement—A Novel Approach in Dentistry. Journal of Clinical Medicine, 11(9), 2508. https://doi.org/10.3390/jcm11092508