
Fatty Acid-Binding Protein 7 (FABP-7), Glutamic Acid and Neurofilament Light Chain (NFL) as Potential Markers of Neurodegenerative Disorders in Psoriatic Patients—A Pilot Study

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Serum Collection
2.2. Statistical Analysis
3. Results
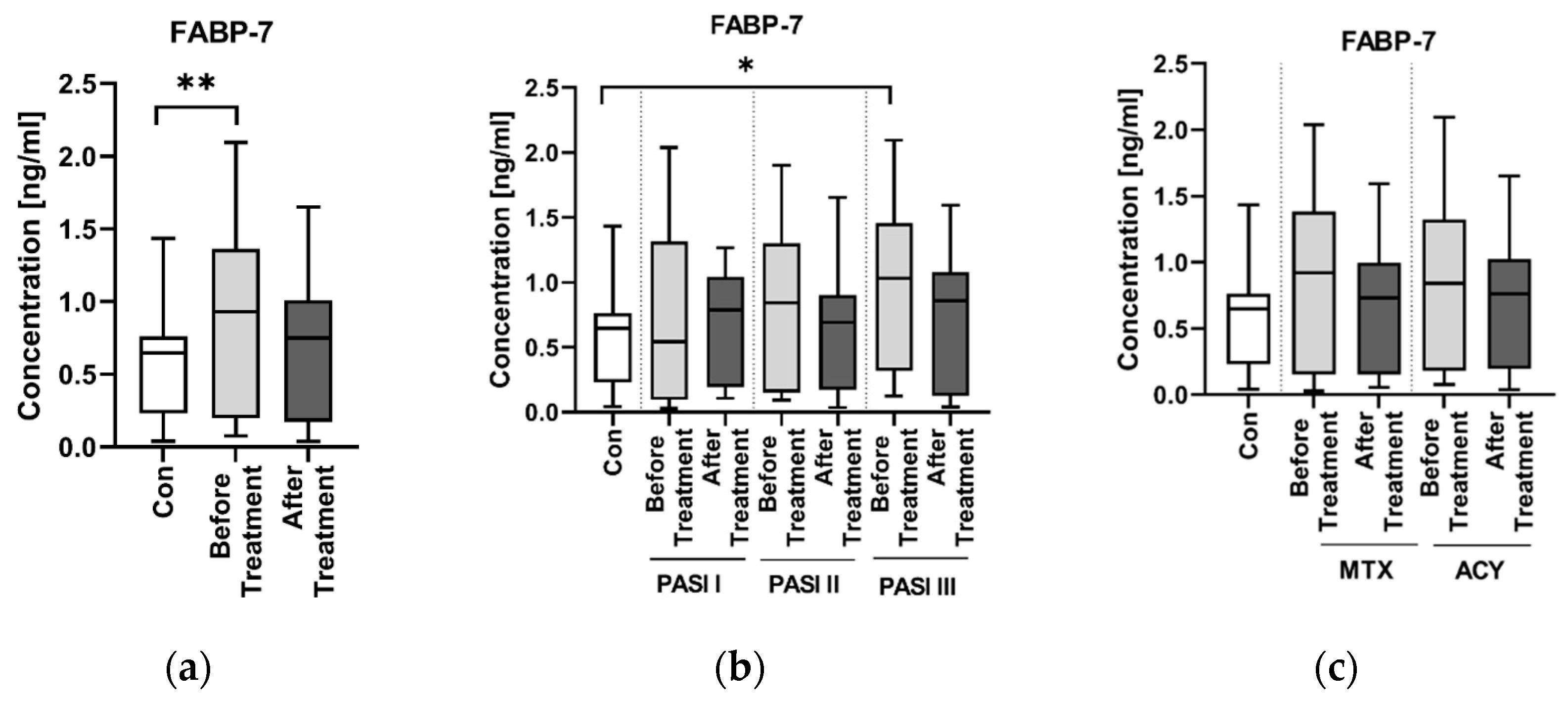
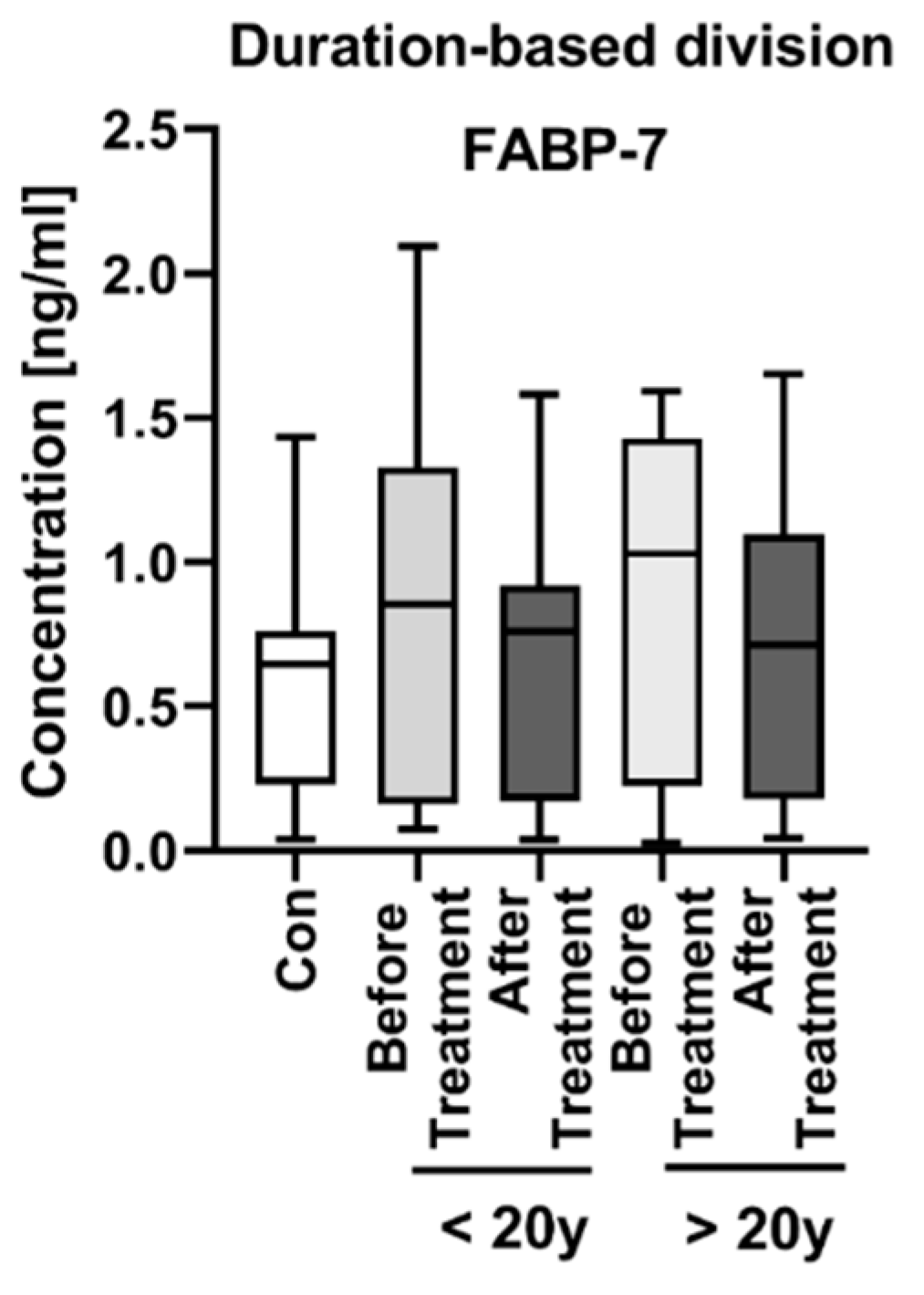
3.1. FABP-7
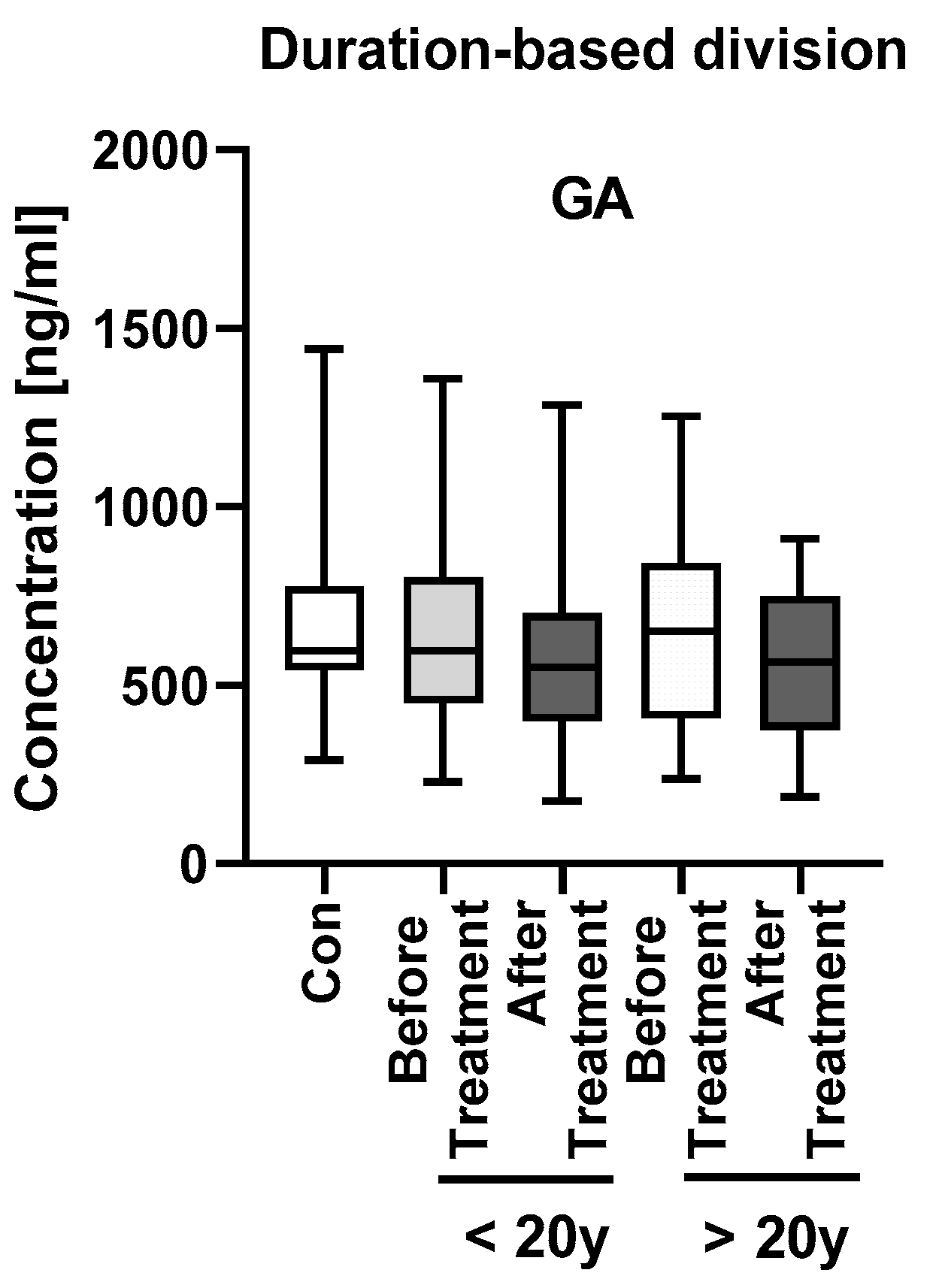
3.2. GA
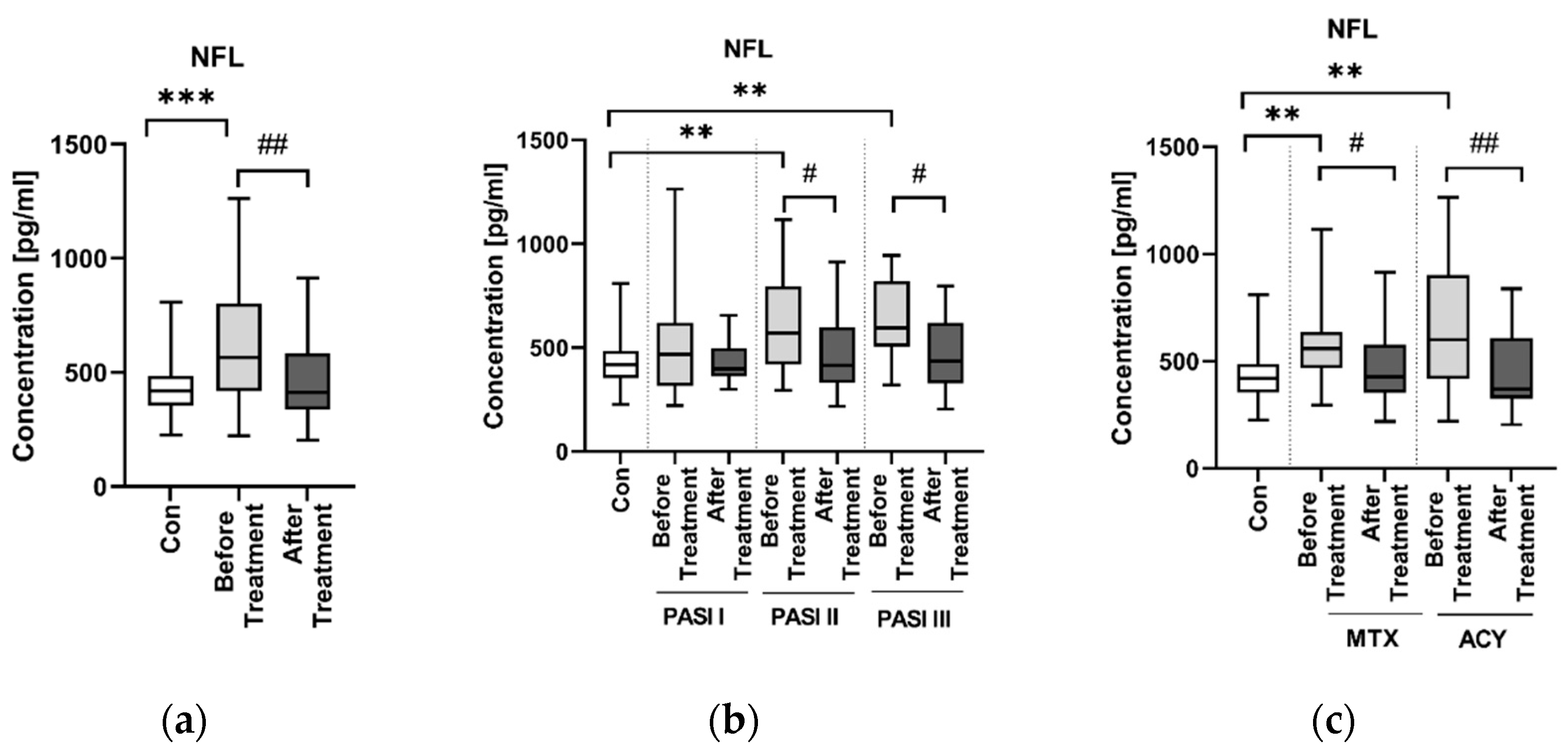
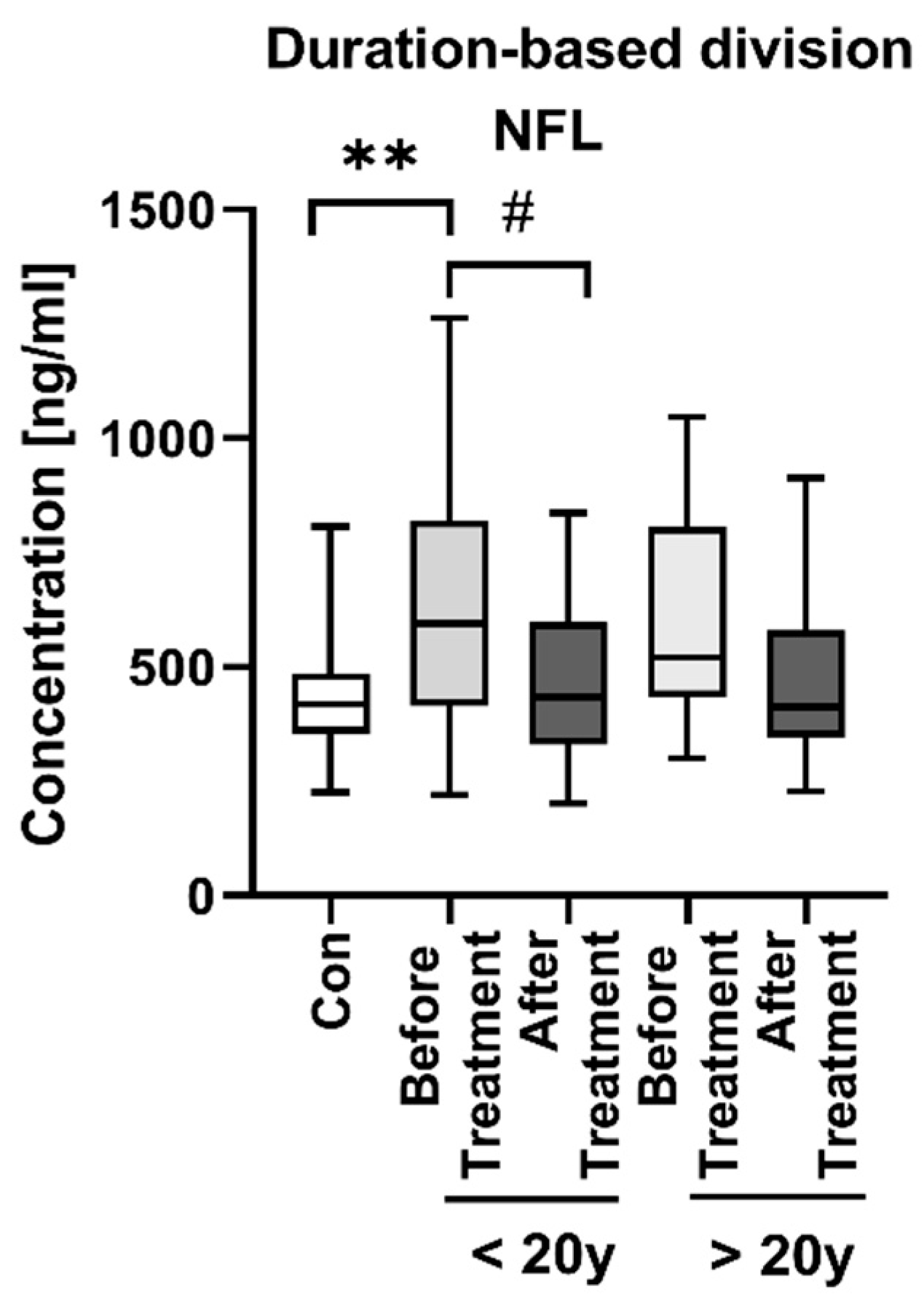
3.3. NFL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Psoriasis Statistics. The National Psoriais Foundation. Available online: https://www.psoriasis.org/psoriasis-statistics/ (accessed on 1 January 2022).
- Tokuyama, M.; Mabuchi, T. New Treatment Addressing the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2020, 21, 7488. [Google Scholar] [CrossRef] [PubMed]
- Elmets, C.A.; Leonardi, C.L.; Davis, D.M.; Gelfand, J.M.; Lichten, J.; Mehta, N.N.; Armstrong, A.W.; Connor, C.; Cordoro, K.M.; Elewski, B.E.; et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. J. Am. Acad. Dermatol. 2019, 80, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Nowowiejska, J.; Baran, A.; Flisiak, I. Psoriasis and cardiometabolic disorders. Dermatol. Rev. 2020, 107, 508–520. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.; Biswas, A. Molecular diagnostics of neurodegenerative disorders. Front. Mol. Biosci. 2015, 2, 54. [Google Scholar] [CrossRef]
- Binvignat, O.; Olloquequi, J. Excitotoxicity as a Target against Neurodegenerative Processes. Curr. Pharm. Des. 2020, 26, 1251–1262. [Google Scholar] [CrossRef]
- Chiurchiù, V.; Maccarrone, M. Chronic Inflammatory Disorders and Their Redox Control: From Molecular Mechanisms to Therapeutic Opportunities. Antioxid. Redox Signal 2011, 15, 2605–2641. [Google Scholar] [CrossRef]
- Choromańska, B.; Myśliwiec, P.; Dadan, J.; Hady Razak, H.; Chabowski, A. Znaczenie kliczne białek wiążących kwasy tłuszczowe. Postepy Hig. Med. Dosw. 2011, 65, 759–763. [Google Scholar] [CrossRef]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry 2019, 90, 870–881. [Google Scholar] [CrossRef]
- Mironova, Y.S.; Zhukova, I.A.; Zhukova, N.G.; Alifirova, V.M.; Izhboldina, O.P.; Latypova, A.V. Bolezn’ Parkinsona i Glutamatnaia Éksaĭtotoksichnost’ [Parkinson’s Disease And Glutamate Excitotoxicity]. Zhurnal Nevrol. I Psikhiatrii Im. SS Korsakova 2018, 118, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Hao, J.; Zeng, J.; Sauter, E.R. SnapShot: FABP Functions. Cell 2020, 182, 1066.e1. [Google Scholar] [CrossRef] [PubMed]
- Baran, A.; Świderska, M.; Bacharewicz-Szczerbicka, J.; Myśliwiec, H.; Flisiak, I. Serum Fatty Acid-Binding Protein 4 is Increased in Patients with Psoriasis. Lipids 2017, 52, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Baran, A.; Kiluk, P.; Maciaszek, M.; Świderska, M.; Flisiak, I. Liver fatty acid-binding protein might be a predictive marker of clinical response to systemic treatment in psoriasis. Arch. Dermatol. Res. 2019, 311, 389–397. [Google Scholar] [CrossRef]
- Hara, T.; Umaru, B.A.; Sharifi, K.; Yoshikawa, T.; Owada, Y.; Kagawa, Y. Fatty Acid Binding Protein 7 is Involved in the Proliferation of Reactive Astrocytes, but not in Cell Migration and Polarity. Acta Histochem. ET Cytochem. 2020, 53, 73–81. [Google Scholar] [CrossRef]
- Maximin, E.; Langelier, B.; Aïoun, J.; Al-Gubory, K.H.; Bordat, C.; Lavialle, M.; Heberden, C. Fatty acid binding protein 7 and n-3 poly unsaturated fatty acid supply in early rat brain development. Dev. Neurobiol. 2016, 76, 287–297. [Google Scholar] [CrossRef]
- Teunissen, C.E.; Veerhuis, R.; De Vente, J.; Verhey, F.R.J.; Vreeling, F.; Van Boxtel, M.P.J.; Glatz, J.F.C.; Pelsers, M.A.L. Brain-specific fatty acid-binding protein is elevated in serum of patients with dementia-related diseases. Eur. J. Neurol. 2011, 18, 865–871. [Google Scholar] [CrossRef]
- Steinacker, P.; Mollenhauer, B.; Bibl, M.; Cepek, L.; Esselmann, H.; Brechlin, P.; Lewczuk, P.; Poser, S.; Kretzschmar, H.A.; Wiltfang, J.; et al. Heart fatty acid binding protein as a potential diagnostic marker for neurodegenerative diseases. Neurosci. Lett. 2004, 370, 36–39. [Google Scholar] [CrossRef]
- Schultz, J.; Uddin, Z.; Singh, G.; Howlader, M.M.R. Glutamate sensing in biofluids: Recent advances and research challenges of electrochemical sensors. Analyst 2020, 145, 321–347. [Google Scholar] [CrossRef]
- Iovino, L.; Tremblay, M.E.; Civiero, L. Glutamate-induced excitotoxicity in Parkinson’s disease: The role of glial cells. J. Pharmacol. Sci. 2020, 144, 151–164. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, D.; Zhang, B.; Zhu, J.; Zhou, Z.; Cui, L. Regulation of microglia by glutamate and its signal pathway in neurodegenerative diseases. Drug Discov. Today 2020, 25, 1074–1085. [Google Scholar] [CrossRef] [PubMed]
- Witoelar, A.; Jansen, I.E.; Wang, Y.; Desikan, R.S.; Gibbs, J.R.; Blauwendraat, C.; Thompson, W.K.; Hernandez, D.G.; Djurovic, S.; Schork, A.J.; et al. Genome-wide Pleiotropy Between Parkinson Disease and Autoimmune Diseases. JAMA Neurol. 2017, 74, 780–792. [Google Scholar] [CrossRef] [PubMed]
- Okan, G.; Baki, A.M.; Yorulmaz, E.; Doğru-Abbasoğlu, S.; Vural, P. A preliminary study about neurofilament light chain and tau protein levels in psoriasis: Correlation with disease severity. J. Clin. Lab. Anal. 2021, 35, e23564. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Park, H.E.; Lee, S.H.; Han, K.; Lee, J.H. Increased risk of Alzheimer’s disease in patients with psoriasis: A nation-wide population-based cohort study. Sci. Rep. 2020, 10, 6454. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Xu, R.; Kaelber, D.; Gurney, M.E. Tumor Necrosis Factor (TNF) blocking agents are associated with lower risk for Alzheimer’s disease in patients with rheumatoid arthritis and psoriasis. PLoS ONE 2020, 15, e0229819. [Google Scholar] [CrossRef]
- Li, C.Y.; Yang, T.M.; Ou, R.W.; Wei, Q.Q.; Shang, H.F. Genome-wide genetic links between amyotrophic lateral sclerosis and autoimmune diseases. BMC Med. 2021, 19, 27. [Google Scholar] [CrossRef]
- Bartkiewicz, P.; Gornowicz-Porowska, J.; Pietkiewicz, P.P.; Świrkowicz, A.; Bowszyc-Dmochowska, M.; Dmochowski, M. Neurodegenerative disorders, bullous pemphigoid and psoriasis: A comparative study in ethnic Poles indicates that Parkinson’s disease is more relevant to bullous pemphigoid. Adv. Dermatol. Allergol. 2017, 34, 42–46. [Google Scholar] [CrossRef]
- Reich, A.; Adamski, Z.; Chodorowska, G.; Kaszuba, A.; Krasowska, D.; Lesiak, A.; Maj, J.; Narbutt, J.; Osmola-Mańkowska, A.J.; Owczarczyk-Saczonek, A.; et al. Psoriasis. Diagnostic and therapeutic recommendations of the Polish Dermatological Society. Part 2. Dermatol. Rev. 2020, 107, 110–137. [Google Scholar] [CrossRef]
- Liu, S.; Li, C.; Shi, Z.; Wang, X.; Zhou, Y.; Liu, S.; Liu, J.; Yu, T.; Ji, Y. Caregiver burden and prevalence of depression, anxiety and sleep disturbances in Alzheimer’s disease caregivers in China. J. Clin. Nurs. 2017, 26, 1291–1300. [Google Scholar] [CrossRef]
- Sheu, J.-J.; Wang, K.-H.; Lin, H.-C.; Huang, C.-C. Psoriasis is associated with an increased risk of parkinsonism: A population-based 5-year follow-up study. J. Am. Acad. Dermatol. 2013, 68, 992–999. [Google Scholar] [CrossRef]
- Senbokuya, N.; Yoshioka, H.; Yagi, T.; Owada, Y.; Kinouchi, H. Effects of FABP7 on functional recovery after spinal cord injury in adult mice. J. Neurosurg. Spine 2019, 31, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Rui, Q.; Ni, H.; Lin, X.; Zhu, X.; Li, D.; Liu, H.; Chen, G. Astrocyte-derived fatty acid-binding protein 7 protects blood-brain barrier integrity through a caveolin-1/MMP signaling pathway following traumatic brain injury. Exp. Neurol. 2019, 322, 113044. [Google Scholar] [CrossRef] [PubMed]
- Ajith, T.A. A Recent Update on the Effects of Omega-3 Fatty Acids in Alzheimer’s Disease. Curr. Clin. Pharmacol. 2018, 13, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Grimm, M.; Haupenthal, V.J.; Mett, J.; Stahlmann, C.P.; Blümel, T.; Mylonas, N.T.; Endres, K.; Grimm, H.S.; Hartmann, T. Oxidized Docosahexaenoic Acid Species and Lipid Peroxidation Products Increase Amyloidogenic Amyloid Precursor Protein Processing. Neurodegener. Dis. 2016, 16, 44–54. [Google Scholar] [CrossRef]
- Leke, R.; Oliveira, D.; Schmidt, A.; Ávila, T.; Jorge, R.; Fischer, A.; Wofchuk, S.; Souza, D.; Portela, L. Methotrexate induces seizure and decreases glutamate uptake in brain slices: Prevention by ionotropic glutamate receptors antagonists and adenosine. Life Sci. 2006, 80, 1–8. [Google Scholar] [CrossRef]
- Weller, M.; Marini, A.M.; Finiels-Marlier, F.; Martin, B.; Paul, S.M. MK-801 and memantine protect cultured neurons from glutamate toxicity induced by glutamate carboxypeptidase-mediated cleavage of methotrexate. Eur. J. Pharmacol. Environ. Toxicol. Pharmacol. 1993, 248, 303–312. [Google Scholar] [CrossRef]
- Mattsson, N.; Andreasson, U.; Zetterberg, H.; Blennow, K.; Alzheimer’s Disease Neuroimaging Initiative. Association of Plasma Neurofilament Light With Neurodegeneration in Patients with Alzheimer Disease. JAMA Neurol. 2017, 74, 557–566. [Google Scholar] [CrossRef]
- Rabbito, A.; Dulewicz, M.; Kulczyńska-Przybik, A.; Mroczko, B. Biochemical Markers in Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 1989. [Google Scholar] [CrossRef]
- Barro, C.; Chitnis, T.; Weiner, H.L. Blood neurofilament light: A critical review of its application to neurologic disease. Ann. Clin. Transl. Neurol. 2020, 7, 2508–2523. [Google Scholar] [CrossRef]
- Karpouzis, A.; Caridha, R.; Tripsianis, G.; Michailidis, C.; Martinis, G.; Veletza, S.V. Apolipoprotein E gene polymorphism in psoriasis. Arch. Dermatol. Res. 2009, 301, 405–410. [Google Scholar] [CrossRef]
- Zhang, H.; Wu, L.-M.; Wu, J. Cross-Talk between Apolipoprotein E and Cytokines. Mediat. Inflamm. 2011, 2011, 949072. [Google Scholar] [CrossRef] [PubMed]
- Manouchehrinia, A.; Piehl, F.; Hillert, J.; Kuhle, J.; Alfredsson, L.; Olsson, T.; Kockum, I. Confounding effect of blood volume and body mass index on blood neurofilament light chain levels. Ann. Clin. Transl. Neurol. 2020, 7, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Carlson, B.A.; Paulson, R.F.; Prabhu, K.S. The intricate role of selenium and selenoproteins in erythropoiesis. Free Radic. Biol. Med. 2018, 127, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Kuhle, J.; Kropshofer, H.; Haering, D.A.; Kundu, U.; Meinert, R.; Barro, C.; Dahlke, F.; Tomic, D.; Leppert, D.; Kappos, L. Blood neurofilament light chain as a biomarker of MS disease activity and treatment response. Neurology 2019, 92, e1007–e1015. [Google Scholar] [CrossRef]
- Rosito, M.; Testi, C.; Parisi, G.; Cortese, B.; Baiocco, P.; Di Angelantonio, S. Exploring the Use of Dimethyl Fumarate as Microglia Modulator for Neurodegenerative Diseases Treatment. Antioxidants 2020, 9, 700. [Google Scholar] [CrossRef]
- Lauer, A.A.; Janitschke, D.; Guilherme, M.D.S.; Nguyen, V.T.T.; Bachmann, C.M.; Qiao, S.; Schrul, B.; Boehm, U.; Grimm, H.S.; Hartmann, T.; et al. Shotgun lipidomics of liver and brain tissue of Alzheimer’s disease model mice treated with acitretin. Sci. Rep. 2021, 11, 15301. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Controls (n = 30) | Patients (n = 60) |
|---|---|---|
| Sex (M/F) | 10/20 | 39/21 |
| Age [years] | 52.5 (25–64) | 57 (19–80) NS |
| Height [cm] | 166 (156–186) | 175 (154–190) NS |
| Weight [kg] | 67.5 (50–133) | 83 (54–136) NS |
| BMI | 24.6 (20–41) | 27.1 (17–44.4) NS |
| Protein | PASIR
(p Value) | BMIR
(p Value) |
|---|---|---|
| GA | 0.188 (0.158) | −0.069 (0.604) |
| FABP-7 | −0.476 (1604 × 10−4) | 0.149 (0.265) |
| NFL | −0.091 (0.499) | −0.051 (0.593) |
| AST R (p) | ALT R (p) | GLU R (p) | CRP R (p) | Chol R (p) | TG R (p) | RBC R (p) | WBC R (p) | PLT R (p) | |
|---|---|---|---|---|---|---|---|---|---|
| GA | −0.05 0.711 | −0.14 0.318 | 0.03 0.830 | −0.27 0.049 * | 0.24 0.086 | 0.09 0.498 | 0 0.989 | −0.14 0.302 | −0.14 0.363 |
| FABP-7 | 0.03 0.837 | 0.08 0.579 | 0.05 0.701 | −0.02 0.873 | −0.01 0.949 | −0.01 0.964 | −0.24 0.086 | 0.05 0.737 | 0.08 0.981 |
| NFL | −0.21 0.109 | −0.02 0.891 | −0.02 0.904 | −0.03 0.832 | 0.1 0.469 | 0.19 0.163 | −0.12 0.374 | −0.13 0.327 | −0.12 0.782 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowowiejska, J.; Baran, A.; Hermanowicz, J.M.; Sieklucka, B.; Krahel, J.A.; Kiluk, P.; Pawlak, D.; Flisiak, I. Fatty Acid-Binding Protein 7 (FABP-7), Glutamic Acid and Neurofilament Light Chain (NFL) as Potential Markers of Neurodegenerative Disorders in Psoriatic Patients—A Pilot Study. J. Clin. Med. 2022, 11, 2430. https://doi.org/10.3390/jcm11092430
Nowowiejska J, Baran A, Hermanowicz JM, Sieklucka B, Krahel JA, Kiluk P, Pawlak D, Flisiak I. Fatty Acid-Binding Protein 7 (FABP-7), Glutamic Acid and Neurofilament Light Chain (NFL) as Potential Markers of Neurodegenerative Disorders in Psoriatic Patients—A Pilot Study. Journal of Clinical Medicine. 2022; 11(9):2430. https://doi.org/10.3390/jcm11092430
Chicago/Turabian StyleNowowiejska, Julia, Anna Baran, Justyna Magdalena Hermanowicz, Beata Sieklucka, Julita Anna Krahel, Paulina Kiluk, Dariusz Pawlak, and Iwona Flisiak. 2022. "Fatty Acid-Binding Protein 7 (FABP-7), Glutamic Acid and Neurofilament Light Chain (NFL) as Potential Markers of Neurodegenerative Disorders in Psoriatic Patients—A Pilot Study" Journal of Clinical Medicine 11, no. 9: 2430. https://doi.org/10.3390/jcm11092430
APA StyleNowowiejska, J., Baran, A., Hermanowicz, J. M., Sieklucka, B., Krahel, J. A., Kiluk, P., Pawlak, D., & Flisiak, I. (2022). Fatty Acid-Binding Protein 7 (FABP-7), Glutamic Acid and Neurofilament Light Chain (NFL) as Potential Markers of Neurodegenerative Disorders in Psoriatic Patients—A Pilot Study. Journal of Clinical Medicine, 11(9), 2430. https://doi.org/10.3390/jcm11092430