
Association between Frequency of Central Respiratory Events and Clinical Outcomes in Heart Failure Patients with Sleep Apnea



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Respiratory Event Estimation
2.3. Outcome Measure
2.4. Statistical Analysis
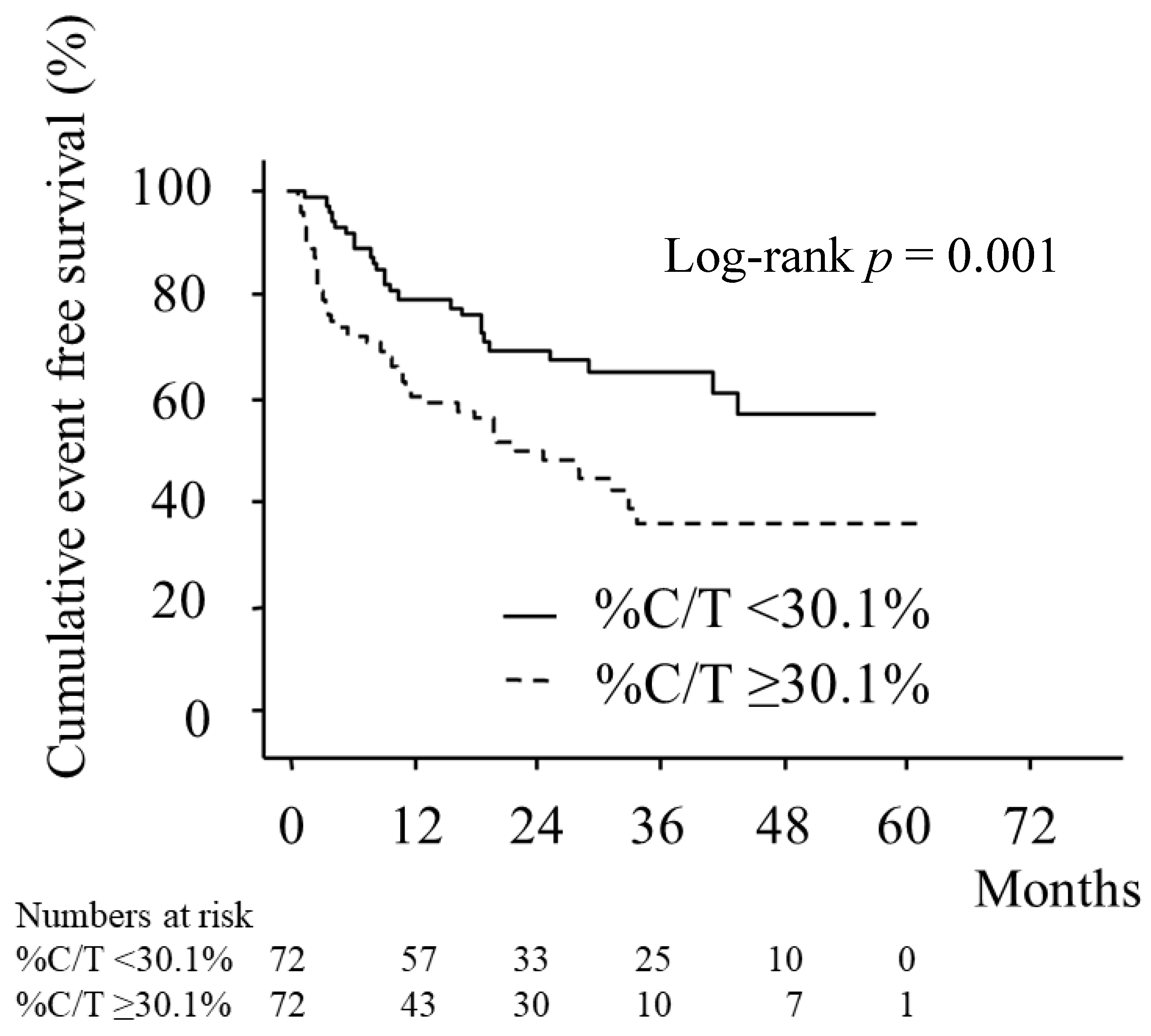
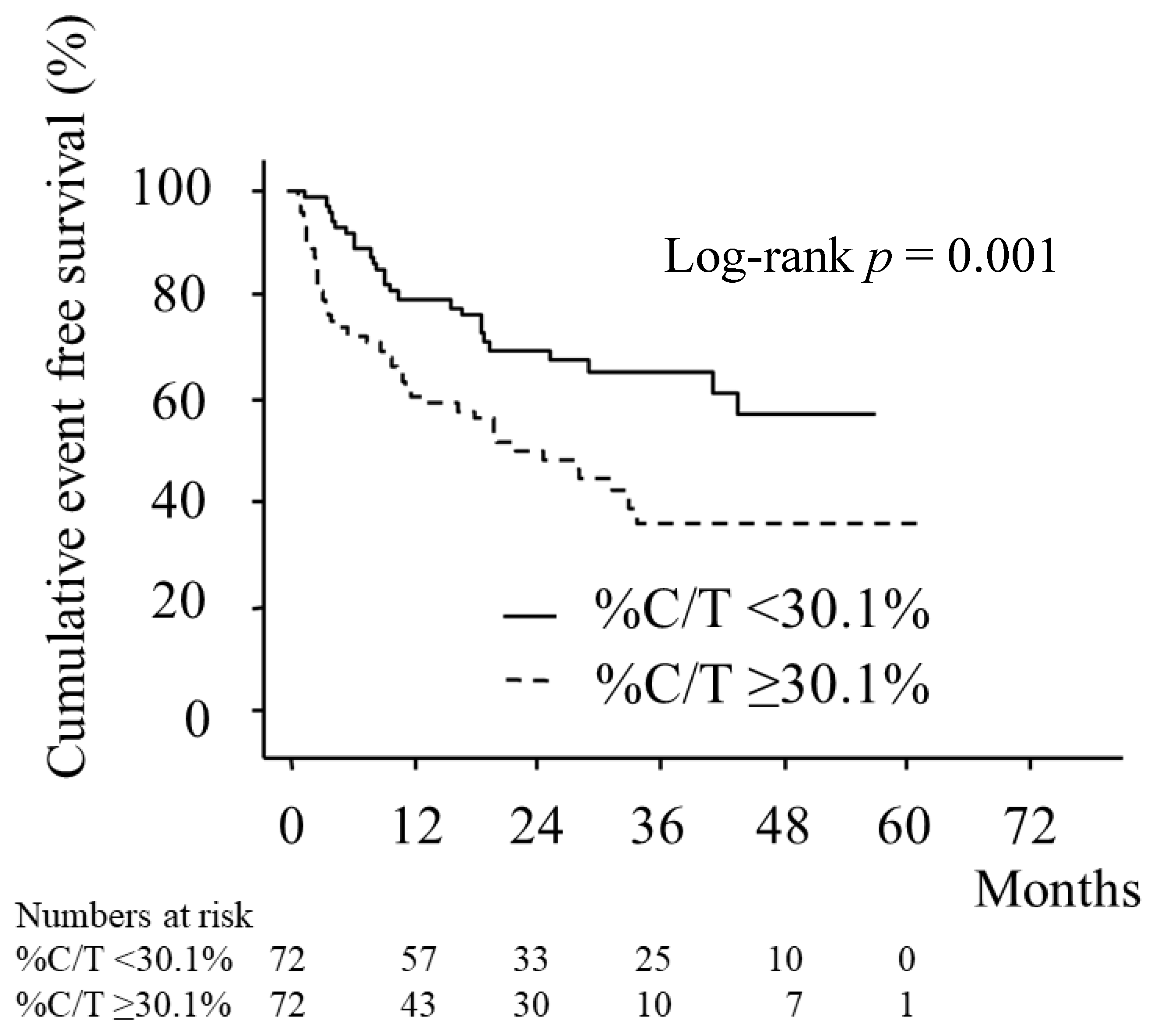
3. Results
4. Discussion
4.1. Clinical Implications and Future Perspectives
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savarese, G.; Lund, L.H. Global public health burden of heart failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics—2018 update: A report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Kasai, T.; Floras, J.S.; Bradley, T.D. Sleep apnea and cardiovascular disease: A bidirectional relationship. Circulation 2012, 126, 1495–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yumino, D.; Wang, H.; Floras, J.S.; Newton, G.E.; Mak, S.; Ruttanaumpawan, P.; Parker, J.D.; Bradley, T.D. Prevalence and physiological predictors of sleep apnea in patients with heart failure and systolic dysfunction. J. Card. Fail. 2009, 15, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Kasai, T. Sleep apnea and heart failure. J. Cardiol. 2012, 60, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sin, D.D.; Fitzgerald, F.; Parker, J.D.; Newton, G.; Floras, J.S.; Bradley, T.D. Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am. J. Respir. Crit. Care Med. 1999, 160, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Quan, S.F.; Abreu, A.R.; Bibbs, M.L.; DelRosso, L.; Harding, S.M.; Marcus, C.; Vaughn, B.V. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.6; American Academy of Sleep Medicine: Darien, IL, USA, 2020; Available online: http://www.aasmnet.org/scoringmanual/ (accessed on 1 March 2022).
- Oates, C.P.; Ananthram, M.; Gottlieb, S.S. Management of Sleep Disordered Breathing in Patients with Heart Failure. Curr. Heart Fail. Rep. 2018, 15, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Drager, L.F.; McEvoy, R.D.; Barbe, F.; Lorenzi-Filho, G.; Redline, S.; INCOSACT Initiative (International Collaboration of Sleep Apnea Cardiovascular Trialists). Sleep Apnea and Cardiovascular Disease: Lessons from Recent Trials and Need for Team Science. Circulation 2017, 136, 1840–1850. [Google Scholar] [CrossRef]
- Javaheri, S.; Shukla, R.; Zeigler, H.; Wexler, L. Central sleep apnea, right ventricular dysfunction, and low diastolic blood pressure are predictors of mortality in systolic heart failure. J. Am. Coll. Cardiol. 2007, 49, 2028–2034. [Google Scholar] [CrossRef] [Green Version]
- Bradley, T.D.; Floras, J.S. Sleep apnea and heart failure: Part I: Obstructive sleep apnea. Circulation 2003, 107, 1671–1678. [Google Scholar] [CrossRef]
- Arabi, Y.; Morgan, B.J.; Goodman, B.; Puleo, D.S.; Xie, A.; Skatrud, J.B. Daytime blood pressure elevation after nocturnal hypoxia. J. Appl. Physiol. 1999, 87, 689–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naughton, M.T.; Benard, D.C.; Liu, P.P.; Rutherford, R.; Rankin, F.; Bradley, T.D. Effects of nasal CPAP on sympathetic activity in patients with heart failure and central sleep apnea. Am. J. Respir. Crit. Care Med. 1995, 152, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Perger, E.; Inami, T.; Lyons, O.D.; Alshaer, H.; Smith, S.; Floras, J.S.; Logan, A.G.; Arzt, M.; Duran Cantolla, J.; Delgado, D.; et al. Distinct Patterns of Hyperpnea During Cheyne-Stokes Respiration: Implication for Cardiac Function in Patients with Heart Failure. J. Clin. Sleep Med. 2017, 13, 1235–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naughton, M.T.; Liu, P.P.; Bernard, D.C.; Goldstein, R.S.; Bradley, T.D. Treatment of congestive heart failure and Cheyne-Stokes respiration during sleep by continuous positive airway pressure. Am. J. Respir. Crit. Care Med. 1995, 151, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Naughton, M.T.; Benard, D.C.; Rutherford, R.; Bradley, T.D. Effect of continuous positive airway pressure on central sleep apnea and nocturnal PCO2 in heart failure. Am. J. Respir. Crit. Care Med. 1994, 150, 1598–1604. [Google Scholar] [CrossRef] [PubMed]
- Tkacova, R.; Liu, P.P.; Naughton, M.T.; Bradley, T.D. Effect of continuous positive airway pressure on mitral regurgitant fraction and atrial natriuretic peptide in patients with heart failure. J. Am. Coll. Cardiol. 1997, 30, 739–745. [Google Scholar] [CrossRef]
- Arzt, M.; Floras, J.S.; Logan, A.G.; Kimoff, R.J.; Series, F.; Morrison, D.; Ferguson, K.; Belenkie, I.; Pfeifer, M.; Fleetham, J.; et al. CANPAP Investigators. Suppression of central sleep apnea by continuous positive airway pressure and transplant-free survival in heart failure: A post hoc analysis of the Canadian Continuous Positive Airway Pressure for Patients with Central Sleep Apnea and Heart Failure Trial (CANPAP). Circulation 2007, 115, 3173–3180. [Google Scholar] [PubMed]
- Teschler, H.; Döhring, J.; Wang, Y.M.; Berthon-Jones, M. Adaptive pressure support servo-ventilation: A novel treatment for Cheyne-Stokes respiration in heart failure. Am. J. Respir. Crit. Care Med. 2001, 164, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Kasai, T.; Usui, Y.; Yoshioka, T.; Yanagisawa, N.; Takata, Y.; Narui, K.; Yamaguchi, T.; Yamashita, A.; Momomura, S.I. JASV Investigators. Effect of flow-triggered adaptive servo-ventilation compared with continuous positive airway pressure in patients with chronic heart failure with coexisting obstructive sleep apnea and Cheyne-Stokes respiration. Circ. Heart Fail. 2010, 3, 140–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowie, M.R.; Woehrle, H.; Wegscheider, K.; Angermann, C.; d’Ortho, M.P.; Erdmann, E.; Levy, P.; Simonds, A.K.; Somers, V.K.; Zannad, F.; et al. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure. N. Engl. J. Med. 2015, 373, 1095–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Characteristic | % C/T ≥ 30.1% (n = 72) | % C/T < 30.1% (n = 72) | p |
|---|---|---|---|
| Age, years | 64.3 ± 12.9 | 60.4 ± 12.8 | 0.076 |
| Male sex, n (%) | 65 (90.3) | 66 (91.7) | 0.771 |
| BMI, kg/m2 | 25.7 ± 6.3 | 26.8 ± 5.2 | 0.266 |
| Systolic BP, mmHg | 130.9 ± 9.8 | 130.9 ± 12.6 | 0.965 |
| Diastolic BP, mmHg | 77.3 ± 10.9 | 79.1 ± 9.8 | 0.309 |
| HR, /min | 75.5 ± 8.6 | 76.5 ± 11.1 | 0.519 |
| LVEF, % | 36.3 ± 9.6 | 38.9 ± 9.4 | 0.101 |
| BNP, pg/mL | 440.1 ± 56.2 | 256.6 ± 24.1 | 0.003 |
| PNE, pg/mL | 555.1 ± 25.0 | 515.6 ± 17.2 | 0.196 |
| NYHA class | 0.030 | ||
| II, n (%) | 30 (41.7) | 45 (62.5) | |
| III, n (%) | 38 (52.8) | 26 (36.1) | |
| IV, n (%) | 4 (5.5) | 1 (1.4) | |
| Ischemic, n (%) | 23 (31.9) | 17 (23.6) | 0.264 |
| Atrial fibrillation, n (%) | 38 (52.8) | 24 (33.3) | 0.019 |
| ICD, n (%) | 4 (5.6) | 1 (1.4) | 0.172 |
| ESS | 8.7 ± 3.9 | 9.1 ± 3.9 | 0.493 |
| CPAP therapy, n (%) | 57 (78.2) | 54 (75.0) | 0.552 |
| Medication | % C/T ≥ 30.1% (n = 72) | % C/T < 30.1% (n = 72) | p |
|---|---|---|---|
| Beta-blockers, n (%) | 47 (65.3) | 38 (52.8) | 0.127 |
| ACE inhibitors/ARBs, n (%) | 62 (86.1) | 61 (84.7) | 0.813 |
| Diuretics, n (%) | 58 (80.6) | 57 (79.2) | 0.835 |
| Digoxin, n (%) | 26 (36.1) | 23 (31.9) | 0.598 |
| % C/T ≥ 30.1% (n = 72) | % C/T < 30.1% (n = 72) | p | |
|---|---|---|---|
| TST, min | 317.7 ± 76.3 | 322.5 ± 84.0 | 0.730 |
| Total AHI, /h | 46.3 ± 17.8 | 40.4 ± 17.9 | 0.049 |
| Obstructive AHI, /h | 14.5 ± 13.8 | 36.2 ± 16.4 | <0.001 |
| Central AHI, /h | 31.8 ± 14.6 | 4.2 ± 4.9 | <0.001 |
| % C/T, % | 71.3 ± 22.9 | 10.9 ± 13.5 | <0.001 |
| % TST SpO2 < 90%, % | 30.6 ± 31.2 | 25.1 ± 30.5 | 0.290 |
| Lowest SpO2, % | 78.4 ± 9.1 | 75.4 ± 15.2 | 0.157 |
| Arousal index, /h | 40.5 ± 21.5 | 39.1 ± 19.5 | 0.692 |
| Sleep stage, % of TST | |||
| Slow wave sleep, % | 5.6 ± 7.9 | 8.1 ± 8.7 | 0.081 |
| REM sleep, % | 10.2 ± 7.2 | 9.8 ± 6.5 | 0.734 |
| Factors | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (1-year increase) | 1.01 | 0.99–1.03 | 0.397 | 1.01 | 0.99–1.03 | 0.518 |
| Male sex | 1.44 | 0.62–3.34 | 0.396 | 1.68 | 0.70–4.00 | 0.245 |
| Systolic BP (1-mmHg increase) | 0.98 | 0.94–0.99 | 0.013 | 0.97 | 0.94–0.99 | 0.026 |
| LVEF (1% increase) | 0.97 | 0.95–0.99 | 0.035 | 0.97 | 0.94–0.99 | 0.012 |
| BNP (10-pg/mL increase) | 1.06 | 1.02–1.09 | 0.003 | 1.05 | 1.01–1.09 | 0.007 |
| Atrial fibrillation | 1.87 | 1.15–3.05 | 0.012 | 1.75 | 1.08–2.82 | 0.023 |
| Beta blocker use | 0.67 | 0.39–0.95 | 0.045 | 0.63 | 0.37–1.10 | 0.105 |
| CPAP therapy | 0.50 | 0.29–0.86 | 0.012 | 0.51 | 0.30–0.87 | 0.014 |
| % C/T ≥ 30.1% | 2.16 | 1.27–3.68 | 0.005 | - | ||
| % C/T (1% increase) | - | 1.02 | 1.01–1.03 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naito, R.; Kasai, T.; Narui, K.; Momomura, S.-I. Association between Frequency of Central Respiratory Events and Clinical Outcomes in Heart Failure Patients with Sleep Apnea. J. Clin. Med. 2022, 11, 2403. https://doi.org/10.3390/jcm11092403
Naito R, Kasai T, Narui K, Momomura S-I. Association between Frequency of Central Respiratory Events and Clinical Outcomes in Heart Failure Patients with Sleep Apnea. Journal of Clinical Medicine. 2022; 11(9):2403. https://doi.org/10.3390/jcm11092403
Chicago/Turabian StyleNaito, Ryo, Takatoshi Kasai, Koji Narui, and Shin-Ichi Momomura. 2022. "Association between Frequency of Central Respiratory Events and Clinical Outcomes in Heart Failure Patients with Sleep Apnea" Journal of Clinical Medicine 11, no. 9: 2403. https://doi.org/10.3390/jcm11092403
APA StyleNaito, R., Kasai, T., Narui, K., & Momomura, S.-I. (2022). Association between Frequency of Central Respiratory Events and Clinical Outcomes in Heart Failure Patients with Sleep Apnea. Journal of Clinical Medicine, 11(9), 2403. https://doi.org/10.3390/jcm11092403