Abstract
This systematic review’s objective was to conduct a complete analysis of the literature on the root canal morphology using advanced micro-computed tomography. The electronic web databases PubMed, Scopus, and Cochrane were examined for research papers concerning the chosen keywords, evaluating the root canal morphology using Micro-CT, published up to 2021. The articles were searched using MeSH keywords and searched digitally on four specialty journal websites. DARE2 extended (Database of Attributes of Reviews of Effects) was used to assess bias risk. The information was gathered from 18 published studies that strictly met the criteria for inclusion. In the included studies, a total of 6696 samples were studied. The studies were conducted on either maxillary (n-2222) or mandibular teeth (n-3760), permanent anteriors (n-625), and Third molars (n-89). To scan samples, a Scanco Medical machine in was used in 10 studies, Bruker Micro-CT in 34, and seven other machines were utilized in the rest. Bruker Micro-CT software from Kontich, Belgium, VG-Studio Max 2.2 software from Volume Graphics, Heidelberg, Germany, was the most commonly used software. The minimum Voxel size (resolution) adopted in the included studies was 11.6 µm. However, 60 µm was the maximum. Most studies classified the root canal morphology using Vertucci’s classification system (n-16) and the four-digit system (n-6).
Keywords:
dental anatomy; dental pulp; dental diagnostic imaging; endodontics; morphology; Micro-CT; root; root canal 1. Introduction
Endodontic therapy aims to thoroughly clean and obturate the whole system of the root canal. However, to prevent endodontic failure and execute successful root canal therapy, specific determinants play an essential role [1,2]. Precise shaping, cleaning, and filling of all spaces previously filled by the radicular pulp tissues or pulp capping/pulpotomy to maintain healthy dental pulp is required. The morphologic uniqueness of each root necessitates a comprehensive knowledge of variations in the root canal system, which should be reflected during the diagnostic and treatment process [3]. Research upon the root canal morphology in lasting teeth has revealed that the root canal’s amount and classification can differ by ethnicity, gender, and in different populations, within the same population, and uniquely in each person [4,5]. Furthermore, it is possible that a variety of morphologic root canal system configurations exist; as a result, each tooth should be evaluated separately using a proper classification system [6].
The investigation of external and internal anatomy of different teeth using many in vitro and in vivo techniques were performed in the beginning of 20th century [7]. Various in vitro techniques were used to identify root and canal morphology which includes root sectioning, staining, tooth clearing, microscopic investigation, radiographic investigations using conventional radiographs, and three-dimensional techniques such as CBCT and microcomputed tomography (MCT) [8]. The in vivo techniques include conventional radiographic examinations, retrospective evaluation of patients’ data, clinical evaluation during root canal treatment, digital radiography, and advanced radiographic techniques such as CBCT [8]. An investigation showed a technique by using longitudinal sectioning to produce a sagittal view of pulp space from pulp chamber to the root apex [9]. Opaque wax was used to fill the exposed canals, but this method showed lateral canals very rarely [10]. Rosenstiel (1957) introduced a technique using a Radio opaque material to reproduce the root canals. A study demonstrated a simple in vitro technique to evaluate both endodontically treated and untreated root canal systems. The following steps were used in the technique to make teeth transparent. Firstly, teeth were decalcified using nitric acid, then dehydrated using alcohol, and finally cleared with methyl salicylate [11].
Digital radiography, magnetic resonance imaging (MRI), densitometry, ultrasound, and computed tomography (CT) are just a few of the noninvasive dental imaging technologies that have been developed in recent years. However, most of these approaches are restricted since they only provide a 2-dimensional (2-D) examination of the root canal system (RCS) and cannot be easily compared subjectively or quantitatively with other samples [12]. Furthermore, these methods do not allow for synchronized 3-dimensional (3-D) examination of teeth surface and interior anatomy [13]. In endodontic research, microcomputed tomography (Micro-CT) has acquired much interest since it displays high-resolution (10 µm) tooth morphological structures and has proven to be an essential information source for dentists, as shown in Figure 1 [14]. Microcomputed tomography is a nondestructive and reproducible ex vivo research method and is considered as the research method that offers the foremost possibility for an accurate examination of the morphology of the root canal system.
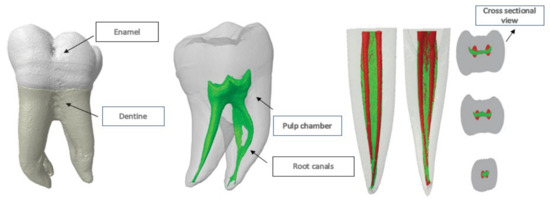
Figure 1.
Micro-CT in endodontics.
The ex vivo investigation is used in Micro-CT imaging, which is widely accepted because of its accuracy, repeatability, and noninvasiveness, all of which are superior to other commonly used research methods [15]. Maxillary central incisors have one root and one main canal. Rarely, at a 6% rate, one canal of central maxillary teeth splits into two parts at the apical foramina which can be classified as Vertucci type V [16]. Apical root canal morphology should be considered because of its main effect on the success of root canal treatment. In the study of Adorno et al. [17], accessory canals in the apical 3 mm in the Japanese population were found among 46% of the specimens. Over the years, different studies have been conducted to understand the root canal morphology of premolars using different research methods [18] and different populations [19,20,21]. The frequency of a single canal is 54–88.5%. However, multiple canals were reported in 11.5–46% of cases [21,22]. In the study of Pan et al. [23], the prevalence of maxillary first premolar teeth with one main root canal was 67.8%, with two roots at 31.9%, and with two canals at 88.2%. In the Malaysian population, according to Vertucci’s classification, the second premolar was detected as single-root type I with the rate of 58.2% [16]. In posterior teeth, mandibular first molars are recognized to exhibit various complex and distinct morphological variations of the root canal system [24,25]. This tooth usually has two roots, but sometimes it has three, with two or three canals in the mesial root and one, two, or three canals in the distal root [26,27]. When only one distal root canal is present, it is often buccolingually oval, and untreated surface areas were shown to be as high as 59–79% when rotary instruments were used for the shaping procedure [28].
Similarly, a study on the Burmese population showed that the prevalence of two canals in mesiobuccal roots of the upper first molar teeth decrease gradually towards the upper third molars. About 85.2% of the 270 roots of the maxillary teeth had one root canal at the apex, 14% had two apical canals, and 0.8% had three apical canals [25,29]. Moreover, the morphology of root canals was explored, white spot lesions on enamel were identified, and enamel demineralization with therapy were assessed using Micro-CT [30,31]. The latest evidence demonstrated the ability to scan isthmuses successfully, while another claimed to detect inorganic material within a tooth root [32,33]. The nondestructive Micro-CT imaging method allows for multiple exposures and data collection. As a result, this imaging method is beneficial for evaluating experimental endodontics [34]. The goal of this systematic review was to carry out a thorough examination of the literature on root canal physiology using sophisticated microcomputed tomography.
2. Methods
2.1. Study Protocol and Registration
The Reporting Items preferred for Meta-Analysis and systematic Review (PRISMA) procedures (http://www.prisma-statement.org, accessed on 10 April 2022) were respected in this work. The current systematic review is registered in PROSPERO with the number CRD42021278968.
2.2. Research Question
Studies about assessment of root canal morphologies through microcomputed tomography were selected based on the “PICOS” (PRISMA-P 2016) technique:
- P (population): Extracted teeth models
- I (intervention): Assessment by Micro-CT
- C (comparison): None
- O (result): Root and root canal morphologies
- S (study design): In vitro studies
2.3. Search Strategies
The electronic online databases search was conducted for research papers based on selected keywords, assessing root canal morphology using Micro-CT, published until March 2022. The number of studies obtained from each dataset is displayed in Table 1. The articles were searched using MeSH keywords and searched digitally on four specialty journal websites. The MeSH keywords were searched in PubMed and Scopus initially, as per our initial search criteria. Further, to add more scientific evidence related to the topic, the search was carried out in Cochrane. Furthermore, to include the latest articles up to the last search date published in the specialty journals as it may take some time for the articles to be included in the indexes after they are published, the search on websites of four endodontic specialty Journals were performed, including the Journal of Endodontics, the International Endodontic Journal, the Australian Endodontic Journal, and the Iranian Endodontic Journal.

Table 1.
Information of sources and search strategies using MeSH keywords.
2.4. Data Sources
Two separate researchers (M.I.K and N.A.) performed an electronic literature search on 20 March 2022, using MeSH terms and keywords, as well as the Boolean operators “OR” and “AND” to compile relevant material using appropriate filters. The keywords used were “Tooth Root/anatomy and histology”, “Tooth Root/diagnosis”, “Tooth Root/diagnostic imaging”, “Tooth root”, “dental pulp cavity”, “Micro-CT”, and “X-ray Microtomography/methods”. The required literature was then gathered using proper filters by combining these key terms with the Boolean operators “OR” and “AND” as shown in Table 1. Furthermore, a hand search was also conducted by two different reviewers using keywords such as “Root canal morphology,” “Root canal configuration,” “Root canal system,” “Microcomputed tomography,” “Micro-computed tomography,” and “Micro-CT” from databases such as PubMed, Scopus, ScienceDirect, and Cochrane.
2.5. Eligibility Criteria
A literature search was performed to uncover studies that used Micro-CT to assess root canal morphology. Two reviewers used the PICOS approach to examine the entire texts of the remaining papers and set inclusion and exclusion criteria. The year of publication was not restricted in any way. On 20 March 2021, the final database search was accomplished. A third reviewer’s decision was used to settle disagreements. Figure 2 illustrates the inclusion and exclusion criteria.
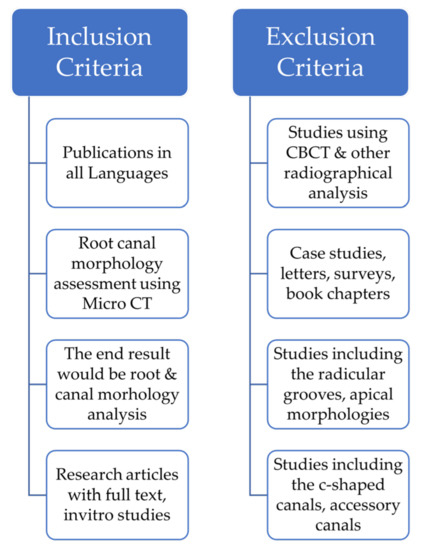
Figure 2.
Inclusion and Exclusion Criteria.
2.6. Study Selection
The studies that examined the assessment of root canal morphology using the Micro-CT technique, which are published in various medical journals, were found through a random check of research papers from online sources. Two researchers evaluated relevant studies against previously defined inclusion and exclusion criteria to substantiate the search technique, as shown in Figure 2.
2.7. Data Extraction
Two reviewers (M.I.K and S.A.) assessed the titles and abstracts of the publications for the inclusion/exclusion criteria mentioned above, and “relevant” articles were chosen for a full-text reading. This procedure was carried out independently, with the help of a third researcher (NA), in the event of any questions or conflicts. A manual hand search was also carried out using different keywords, and studies were included based on selected criteria.
2.8. Quality Assessment and Risk of Bias of Research Articles
The papers were selected for inclusion and exclusion based on their titles, abstracts, and inclusion and exclusion criteria. Following the screening process, full-text articles were reviewed one by one, and the material’s quality was evaluated. The articles were rated for allotment biases, preference biases, involvement integrity, allocation concealment, withdrawals and dropouts, confusion, data collection methods, and statistical analysis using internal and external validity guidelines. A total of 60 papers were screened for quality, with nine being rejected due to a lack of information about the processes, teeth, research nature, and outcomes.
The Joanna Briggs Institute (JBI) critical assessment checklist was used to appraise the quality of the included studies [35]. This checklist assessed nine items: (i) appropriate sampling frame, (ii) proper sampling technique, (iii) adequate sample size, (iv) study subject and setting description, (v) sufficient data analysis, (vi) use of valid methods for the identified conditions, (vii) valid measurement for all the participants, (viii) use of appropriate statistical analysis, and (ix) adequate response rate. Answers such as yes, no, unclear, or not applicable are assigned to each item. The ‘yes’ response received a 1 score, whereas the ‘no’ and ‘unclear’ responses received ratings of 0. Finally, the average score for each item was computed. The quality of studies with scores below and above the mean was then classified as good or poor quality, respectively. The study was included or excluded based on the methodological quality assessment. (Supplementary Table S1).
Two researchers (M.I.K. and N.A.) oversaw scoring, and they used the JBI criteria to base their scores. After comparing the results of their individual questions, they resolved any discrepancies to arrive at an ‘agreed score’. All of the 51 included studies individually had a total score of ≥70%. Hence, both the researchers (M.I.K and N.A.) showed agreement for most of the included studies and were given >70% scores, thus limiting the bias.
3. Results
3.1. Study Selection Results
PubMed yielded a total of 236 research papers using MeSH keywords, 483 from Cochrane using MeSH keywords, 131 from Scopus using MeSH keywords, and 2179 from ScienceDirect. Following the removal of duplicate articles (98), a total of 2931 studies were recognized for further consideration. After reading the titles of the articles, another 2519 were eliminated. In addition, 352 additional articles were eliminated after reading the abstracts. By reading the full texts of the residual 60 articles, they were evaluated for further selection; nine more articles were eliminated. The data were extracted from the 51 studies that strictly met the eligibility criteria. Figure 3 depicts the selection criteria as it follows the PRISMA guidelines. These 51 articles were examined for the current study based on the quality of the research studies.
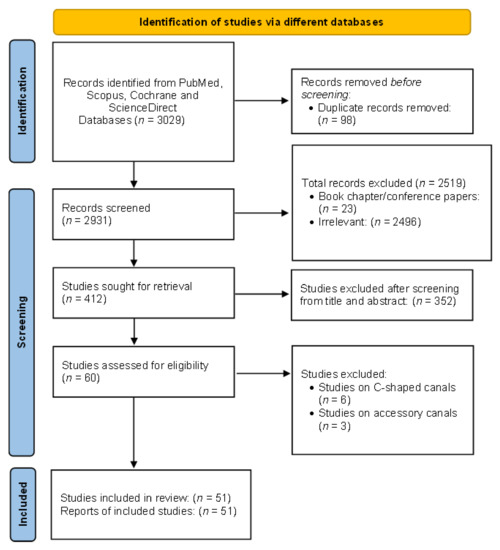
Figure 3.
PRISMA flowchart showing the selection process of articles retrieved from different web sources.
3.2. Study Features
The studies’ basic features included in the systematic review are summarized in Table 2. The studies were performed in various countries, lasted varying amounts of time, and were published in various journals. Each included study was published in a good, reputed journal indexed in Web of Science/PubMed/Scopus. The technical characteristics, such as sample size, type of teeth, instrument used, resolution, software, classification system, methods, outcomes, and conclusion, were omitted from the systematic review. Most of the reports comprised were issued in the Journal of Endodontics (n-13). In contrast, six were published in the International Endodontic Journal, four in the Clinical Oral Investigations, two in the Scientific reports, two in the Journal of Conservative Dentistry, two in Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, two in the Archives of Oral Biology, two in the Journal of Applied Oral Sciences, two in Clinical Oral Investigations, two in Clinical Anatomy, one in the Australian Endodontic Journal, one in the International Journal of Oral Sciences, one in the Swiss Dental Journal, one in the European Endodontic Journal, one in Acta Odontologica Latinoamericana, one in the Journal of Dental Sciences, one in the Nigerian Journal of Clinical Practice, one in the International Medical Journal of Experimental and Clinical Research, one in the British Journal of Oral and Maxillofacial Surgery, one in The Saudi Dental Journal, one in Imaging Science in Dentistry, one in Medical Principles and Practice, one in The Bulletin of Tokyo Dental College, and one in Annals of Anatomy. All the included studies were published between 2008–2022. The research included was carried out in a variety of nations, including Brazil (n-16), China (n-7), Egypt (n-5), Germany (n-5), Poland (n-3), the United States (n-2), Korea (n-2), Turkey (n-2), New Zealand (n-1), Chile (n-1), France (n-1), Myanmar (n-1), Saudi Arabia (n-1), Italy (n-1), Japan (n-1), and the United Arab Emirates (n-1)
Table 2.
Studies included in the systematic review.
In the studies included, a total of 6696 samples were studied. The studies were conducted on either maxillary (n-2222) or mandibular teeth (n-3760), permanent anteriors (n-625), and third molars (n-89). Of the total maxillary and mandibular teeth, 970 were maxillary first molars, 262 were maxillary second molars, 659 were both maxillary first and second molars, 331 were maxillary premolars, 789 were mandibular first molars, 158 were mandibular second molars, 529 were mandibular first premolars, 1254 were mandibular incisors, 281 were mandibular canines, and the remaining 1463 were mixed. The authors used different reagents to store the samples (70% Alcohol, 0.5% sodium azide solution, or 10% formalin). To scan samples, a Scanco Medical machine was used in 10 studies, a Bruker Micro-CT machine in 34 studies, Micro-CT Inveon, Siemens Medical Solutions, Knoxville in two studies, VGStudio Max 2.2 in one study, Nikon Metrology Inc, Brighton in one study, Nanotom S, General Electric in one study, Kodak, Rochester, New York, USA in one study, and HMX 225-ACTIS 4, Tesco, Inc in one study.
Bruker Micro-CT software from Kontich, Belgium (n-27), software VG-Studio Max 2.2 from Volume Graphics, Germany Heidelberg (n-10), NRecon software (n-5), CTAn v.1.12 software Mimics 17.01, Materialize, Leuven, Belgium (n-4), MICs 10.01 software Materialise, Leuven, Belgium (n-1), Image processing language (n-1), On-Demand 3D software from Cybermed, Seoul, Republic of Korea (n-2), Cobra software Siemens Medical Solutions, Knoxville (n-1), and MeVisLab v3.2 software (MeVis Medical Solutions AG, Bremen, Germany) (n-1) was used in the studies to interpret the data about root canal morphologies. The minimum Voxel size (resolution) adopted in included studies was 11.6 µm. However, 60 µm was the maximum resolution adopted in included studies. Most studies classified the root canal morphology using Vertucci’s classification system (n-16) and the four-digit system (n-6). Furthermore, Weine’s classification system (n-3), Pucci & Reig (1944), a new classification system by Ahmed et al., Pomeranz ‘s classification and the American Association of Endodontics system for classification were also used. The technical characteristics of the studies are shown in Table 3.
Table 3.
Characteristics of the included studies.
4. Discussion
Micro-CT analysis has proven useful in a wide variety of applications in dental research. It can provide high-resolution images, as well as qualitative and quantitative analysis of teeth [83,84]. To achieve long-term treatment success, endodontic anatomical knowledge is required. As a result, a detailed description of the apical region is required [85]. Until now, there was a scarcity of detailed information on the anatomy of the RCS; therefore, 3-D, high-resolution techniques dominated. Compact commercial systems are now available and are quickly becoming vital in many academic and corporate research laboratories. It is possible to study a wide range of specimens using Micro-CT to examine mineralized tissue, teeth, bone, and materials such as ceramics, polymers, and biomaterial scaffolds [86,87,88,89]. Micro-CT provides a repeatable, nondestructive, and noninvasive technique for nonclinical ex vivo evaluation with this goal in mind, enabling measured values of the structures investigated and providing critical info regarding minimal structures such as the end part of the apical portion of teeth [49,50,90,91].
Even though data is challenging to come by, it appears that a large group of researchers agree that Micro-CT gives more objective information than traditional 2-D optical techniques [92], the clearing procedure, or scanning microscopy [44]. As a result, in the present study, a substantial number of sufficiently recognized teeth were evaluated using Micro-CT, allowing for a thorough statistical analysis of the sample. Compared with other investigating techniques, the advantages of Micro-CT produce extraordinary resolution 3-D and 2-D figures, with possibilities of rescanning the sample and volumetric analysis of external and internal structures. The Micro-CT system using a microfocal spot X-ray source and a high-resolution detector is projected in several directions to obtain a three-dimensional reconstructed image of the sample. Since the imaging process is nondestructive, the unique properties of the same sample can be tested multiple times, and the sample can still be used after scanning for further biological and mechanical testing [89]. Some of the recent applications of Micro-CT in dental research includes enamel thickness and tooth measurement [93], analysis of root canal morphology and evaluation of root canal preparation [94], craniofacial skeletal development and structure [95], biomechanics, tissue engineering, determination of mineral concentrations of teeth [96], and the measurement of implant stability and osseointegration [97]. The main disadvantage of Micro-CT is that it cannot be utilized in medical practices due to elevated radiation heights, the operating cost, time taken to process data, cost-effectiveness, and safety [98,99].
The current study provides an overview of the Micro-CT studies for root canal morphology. The data included in this systematic review are secondary information collected from various past research studies. Secondary data are prone to flaws or biases present in the original data, which might eventually appear in the study’s findings. For example, it may appear in the analysis technique, or the smallest number of teeth examined in the research. However, the goal was to give the dentistry and endodontic communities a Micro-CT-based analysis of the massive data on the root canal morphology.
Endodontic therapy, both nonsurgical and surgical, needs a thorough understanding of tooth anatomy and morphology [100,101]. Because it is used to instrument and fill root canals to a considerable extent, the morphological interpretation of the apical region should be accurate. Understanding the apical region and the configuration of the root canals is an essential and challenging condition that the clinician must have to make judgments about during endodontic therapy [102].
Despite the fact that the permanent anterior maxillary and mandibular teeth are typically single-rooted, studies suggest that an auxiliary root might be present [103]. Earlier studies in other ethnicities, comprising Turkish, American, Brazilian, and Indian communities, found that all maxillary incisor teeth were single-rooted [104,105,106]. This suggests that the number of roots in maxillary incisors does not differ structurally throughout all populations. Nevertheless, it is important to note that the presence of a double-rooted maxillary anterior has only been confirmed in a few case studies [103]. However, studies revealed a double-rooted mandibular anterior [4]. Numerous root canal morphology differences in mandibular incisors were documented [37,43,47]. The current review showed that the most common type of root canal morphology classified using the four-digit system was 1-1-1, Type I using Vertucci’s classification system, and Type 1-1 using Weine’s classification. According to previous research, Vertucci type I in mandibular incisors can range between 55% and 87% [107]. In two earlier investigations of Turkish populations, type I in the mandibular incisors was lower [108,109]. The most common type of root canal configuration identified in this study was type I (75 percent), similar to Vertucci’s results [16]. Both mandibular incisors had 88% of type 1 configuration, according to Madeira and Hetem [110]. Furthermore, De Almeida, MM et al. revealed that the most common was type III from the Vertucci classification (16%) [47].
The mandibular first molar is not only the most treated endodontically, but it also presents several anatomic difficulties. The diversity includes isthmuses, several canals, apical ramifications, and lateral canals [3]. Additionally, the distal surface of the mesial root has a thin patch of dentin referred to as a danger zone because there is a higher chance of perforation of dentin in this region during mechanical instrumentation. Hence, orthograde and retrograde endodontic treatment in this tooth may be difficult because of its unusual form [40,102]. The anatomy of the mandibular second molar has been widely investigated, notably using the cleaning procedure [102]. According to previous research, the frequency of C-shaped canals is between 31 and 45% (mostly of Asian people) [52,111,112,113]. Various classifications of the tridimensional distributions of RCS and the transverse sections have also been published subsequently [114,115].
The canal shape of posterior maxillary teeth varies significantly between races and geographical locations. As per Mohara et al., Brazilians have a 64.2 percent frequency of MB2 in the foremost permanent molar and a 33.5 percent incidence in the subsequent permanent maxillary molar, respectively [116]. In South Africa, type IV root canals are widespread in maxillary primary molar and type I root canals are the most familiar in a maxillary second molar, according to the Vertucci classification of the root canal [117]. According to Li et al., the most common maxillary first premolar anatomy in the Chinese population is one root with two canals (58.0 percent), and the most common canal morphology is type IV (42.7 percent) [118]. Guo et al., on the other hand, examined the maxillary first molars’ morphology amongst the North American population and discovered that Asians had a higher occurrence of type I (35.0 percent) and type IV (45.0 percent) configurations than whites (type IV: 36.3 percent, type I: 23.4 percent) [119]. As a result, root canal shape varies depending on where you live. Relevant studies in native communities can help dentists better analyze and understand root canal therapy while also adding to the body of information about root and canal morphology in humans.
The current work uses Micro-CT imaging of many samples to provide a detailed assessment of root canal morphology of the mandibular and maxillary teeth. This knowledge will help practitioners comprehend and anticipate the challenges of 3-D endodontic therapy, particularly during root canal shaping and cleaning. This study revealed that the maxillary first molar and mandibular first premolars had a higher incidence of morphological endodontic variables than the other maxillary and mandibular molars and incisors, indicating that they are more complicated.
5. Study Limitations
We searched data from a small number of significant websites for our systematic review. Articles that have appeared in other publications not indexed in the indices searched may have been ignored. We have also only included items published in English; as a result, publications in other languages may have been overlooked. A limited number of studies have been performed using Micro-CT.
6. Conclusions
This review used Micro-CT studies to provide detailed information atop the anatomy of the root and canal morphology in permanent dentition of various populations. Further, it revealed wide disparities concerning root and canal morphology in permanent dentition, which could perhaps derive from the geographical area studied. In Micro-CT findings, the mandibular incisors followed by maxillary molars were the most studied teeth. The use of multiple categorization systems and Micro-CT allowed for a more precise description of the root canal system and its ramifications, with some inconsistencies noted for molars. This Micro-CT study adds to the existing categorization methods by providing a detailed description of the diversity among root canals and their ramifications and clinically relevant data on the presence and location of lateral canals in all human tooth groups.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm11092287/s1, Table S1: Quality of included studies by JBI critical appraisal checklist for included studies.
Author Contributions
Conceptualization, M.I.K. and T.Y.N.; methodology, M.I.K., S.A., N.A., S.N.B. and T.Y.N.; software, S.N.B. and S.W.P.; validation, A.M. and C.M.M.; formal analysis, A.M. and C.M.M.; investigation, M.I.K., S.A. and N.A.; resources, S.N.B. and S.W.P.; data curation, M.I.K., S.A. and N.A.; writing—original draft preparation, M.I.K., S.A. and A.M.; writing—review and editing, T.Y.N., P.M. and G.A.S.; visualization, N.A.; supervision, T.Y.N. and G.A.S.; project administration, M.I.K.; funding acquisition, P.M. All authors have read and agreed to the published version of the manuscript.
Funding
This systematic review received no outside funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data used in the current study will be made available at a reasonable request.
Conflicts of Interest
The authors declared no conflict of interest.
References
- Versiani, M.A.; Pécora, J.D.; de Sousa-Neto, M.D. Root and Root Canal Morphology of Four-rooted Maxillary Second Molars: A Micro–Computed Tomography Study. J. Endod. 2012, 38, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Bianchi, S.; Fantozzi, G.; Leuter, C.; Continenza, M.A.; Macchiarelli, G. Morphometric study on single-root premolars in a European population sample: An update on lengths and diameters. Eur. J. Anat. 2019, 23, 17–25. [Google Scholar]
- Wolf, T.G.; Kim, P.; Campus, G.; Stiebritz, M.; Siegrist, M.; Briseño-Marroquín, B. 3-Dimensional Analysis and Systematic Review of Root Canal Morphology and Physiological Foramen Geometry of 109 Mandibular First Premolars by Micro–computed Tomography in a Mixed Swiss-German Population. J. Endod. 2020, 46, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Karobari, M.I.; Noorani, T.Y.; Halim, M.S.; Ahmed, H.M.A. Root and canal morphology of the anterior permanent dentition in Malaysian population using two classification systems: A CBCT clinical study. Aust. Endod. J. 2020, 47, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Karobari, M.I.; Noorani, T.Y.; Halim, M.S.; Dummer, P.M.H.; Ahmed, H.M.A. Should inter-canal communications be included in the classification of root canal systems? Int. Endod. J. 2019, 52, 917–919. [Google Scholar] [CrossRef] [PubMed]
- Karobari, M.I.; Parveen, A.; Mirza, M.B.; Makandar, S.D.; Nik Abdul Ghani, N.R.; Noorani, T.Y.; Marya, A. Root and Root Canal Morphology Classification Systems. Int. J. Dent. 2021, 2021, 6682189. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Arshad, S.; Basheer, S.N.; Karobari, M.I.; Marya, A.; Marya, C.M.; Taneja, P.; Messina, P.; Yean, C.Y.; Scardina, G.A. Smoking a Dangerous Addiction: A Systematic Review on an Underrated Risk Factor for Oral Diseases. Int. J. Environ. Res. Public Health 2021, 18, 11003. [Google Scholar] [CrossRef]
- Ahmad, I.A. Root and root canal morphology of Saudi Arabian permanent dentition. Saudi Endod. J. 2015, 5, 99–106. [Google Scholar] [CrossRef]
- Sommer, L.H. 0-F. Bennett, PG Campbell and DR Weyenberg. J. Am. Chem. Soc. 1957, 79, 3295. [Google Scholar] [CrossRef]
- Gupta, B.; Tiwari, B.; Raj, V.; Kashyap, B.; Chandra, S.; Dwivedi, N. Transparent tooth model: A study of root canal morphology using different reagents. Eur. J. Gen. Dent. 2014, 3, 66–70. [Google Scholar] [CrossRef]
- Robertson, D.; Leeb, I.J.; Mckee, M.; Brewer, E. A clearing technique for the study of root canal systems. J. Endod. 1980, 6, 421–424. [Google Scholar] [CrossRef]
- Tomaszewska, I.M.; Leszczyński, B.; Wróbel, A.; Gładysz, T.; Duncan, H.F. A micro-computed tomographic (Micro-CT) analysis of the root canal morphology of maxillary third molar teeth. Ann. Anat.-Anat. Anz. 2018, 215, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Grande, N.M.; Plotino, G.; Gambarini, G.; Testarelli, L.; D’Ambrosio, F.; Pecci, R.; Bedini, R. Present and future in the use of Micro-CT scanner 3D analysis for the study of dental and root canal morphology. Annali dell’Istituto Superiore di Sanita 2012, 48, 26–34. [Google Scholar] [PubMed]
- Acar, B.; Kamburoğlu, K.; Tatar, İ.; Arıkan, V.; Çelik, H.H.; Yüksel, S.; Özen, T. Comparison of micro-computerized tomography and cone-beam computerized tomography in the detection of accessory canals in primary molars. Imaging Sci. Dent. 2015, 45, 205. [Google Scholar] [CrossRef] [PubMed]
- Solomonov, M.; Paqué, F.; Fan, B.; Eilat, Y.; Berman, L.H. The Challenge of C-shaped Canal Systems: A Comparative Study of the Self-Adjusting File and ProTaper. J. Endod. 2012, 38, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Vertucci, F.J. Root canal anatomy of the human permanent teeth. Oral Surg. Oral Med. Oral Pathol. 1984, 58, 589–599. [Google Scholar] [CrossRef]
- Adorno, C.; Yoshioka, T.; Suda, H. Incidence of accessory canals in Japanese anterior maxillary teeth following root canal filling ex vivo. Int. Endod. J. 2010, 43, 370–376. [Google Scholar] [CrossRef]
- Zillich, R.; Dowson, J. Root canal morphology of mandibular first and second premolars. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 738–744. [Google Scholar] [CrossRef]
- Khedmat, S.; Assadian, H.; Saravani, A.A. Root canal morphology of the mandibular first premolars in an Iranian population using cross-sections and radiography. J. Endod. 2010, 36, 214–217. [Google Scholar] [CrossRef]
- Awawdeh, L.; Abdullah, H.; Al-Qudah, A. Root form and canal morphology of Jordanian maxillary first premolars. J. Endod. 2008, 34, 956–961. [Google Scholar] [CrossRef]
- Celikten, B.; Orhan, K.; Aksoy, U.; Tufenkci, P.; Kalender, A.; Basmaci, F.; Dabaj, P. Cone-beam CT evaluation of root canal morphology of maxillary and mandibular premolars in a Turkish Cypriot population. BDJ Open 2016, 2, 15006. [Google Scholar] [CrossRef] [PubMed]
- Alkaabi, W.; AlShwaimi, E.; Farooq, I.; Goodis, H.E.; Chogle, S.M. A micro-computed tomography study of the root canal morphology of mandibular first premolars in an Emirati population. Med. Princ. Pract. 2017, 26, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.Y.Y.; Parolia, A.; Chuah, S.R.; Bhatia, S.; Mutalik, S.; Pau, A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health 2019, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Villas-Bôas, M.H.; Bernardineli, N.; Cavenago, B.C.; Marciano, M.; del Carpio-Perochena, A.; de Moraes, I.G.; Duarte, M.H.; Bramante, C.M.; Ordinola-Zapata, R. Micro–Computed Tomography Study of the Internal Anatomy of Mesial Root Canals of Mandibular Molars. J. Endod. 2011, 37, 1682–1686. [Google Scholar] [CrossRef] [PubMed]
- Gulabivala, K.; Aung, T.; Alavi, A.; Ng, Y.L. Root and canal morphology of Burmese mandibular molars. Int. Endod. J. 2001, 34, 359–370. [Google Scholar] [CrossRef]
- Gulabivala, K.; Opasanon, A.; Ng, Y.L.; Alavi, A. Root and canal morphology of Thai mandibular molars. Int. Endod. J. 2002, 35, 56–62. [Google Scholar] [CrossRef]
- Gu, Y.; Lu, Q.; Wang, H.; Ding, Y.; Wang, P.; Ni, L. Root Canal Morphology of Permanent Three-rooted Mandibular First Molars—Part I: Pulp Floor and Root Canal System. J. Endod. 2010, 36, 990–994. [Google Scholar] [CrossRef]
- Paqué, F.; Balmer, M.; Attin, T.; Peters, O.A. Preparation of Oval-shaped Root Canals in Mandibular Molars Using Nickel-Titanium Rotary Instruments: A Micro-computed Tomography Study. J. Endod. 2010, 36, 703–707. [Google Scholar] [CrossRef]
- Guven, E.P. Root Canal Morphology and Anatomy. In Human Teeth-Key Skills and Clinical Illustrations; IntechOpen: London, UK, 2019. [Google Scholar]
- Hamba, H.; Nikaido, T.; Inoue, G.; Sadr, A.; Tagami, J. Effects of CPP-ACP with sodium fluoride on inhibition of bovine enamel demineralization: A quantitative assessment using micro-computed tomography. J. Dent. 2011, 39, 405–413. [Google Scholar] [CrossRef]
- Huang, T.T.; Jones, A.S.; He, L.H.; Darendeliler, M.A.; Swain, M.V. Characterisation of enamel white spot lesions using X-ray micro-tomography. J. Dent. 2007, 35, 737–743. [Google Scholar] [CrossRef]
- Fan, B.; Pan, Y.; Gao, Y.; Fang, F.; Wu, Q.; Gutmann, J.L. Three-dimensional Morphologic Analysis of Isthmuses in the Mesial Roots of Mandibular Molars. J. Endod. 2010, 36, 1866–1869. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.P.; Lumley, P.J.; Claridge, E.; Cooper, P.R.; Grover, L.M.; Williams, R.L.; Walmsley, A.D. An analytical Micro CT methodology for quantifying inorganic dentine debris following internal tooth preparation. J. Dent. 2012, 40, 999–1005. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rossi-Fedele, G.; Ahmed, H.M.A. Assessment of root canal filling removal effectiveness using micro–computed tomography: A systematic review. J. Endod. 2017, 43, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute (JBI). Checklist for Prevalence Studies; Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Briseño-Marroquín, B.; Paqué, F.; Maier, K.; Willershausen, B.; Wolf, T.G. Root canal morphology and configuration of 179 maxillary first molars by means of micro–computed tomography: An ex vivo study. J. Endod. 2015, 41, 2008–2013. [Google Scholar] [CrossRef]
- Wolf, T.G.; Stiebritz, M.; Boemke, N.; Elsayed, I.; Paqué, F.; Wierichs, R.J.; Briseño-Marroquín, B. 3-dimensional Analysis and Literature Review of the Root Canal Morphology and Physiological Foramen Geometry of 125 Mandibular Incisors by Means of Micro–Computed Tomography in a German Population. J. Endod. 2020, 46, 184–191. [Google Scholar] [CrossRef]
- Mazzi-Chaves, J.F.; Silva-Sousa, Y.T.C.; Leoni, G.B.; Silva-Sousa, A.C.; Estrela, L.; Estrela, C.; Jacobs, R.; Sousa-Neto, M.D.d. Micro-computed tomographic assessment of the variability and morphological features of root canal system and their ramifications. J. Appl. Oral Sci. 2020, 28, e20190393. [Google Scholar] [CrossRef]
- Domark, J.D.; Hatton, J.F.; Benison, R.P.; Hildebolt, C.F. An ex vivo comparison of digital radiography and cone-beam and micro computed tomography in the detection of the number of canals in the mesiobuccal roots of maxillary molars. J. Endod. 2013, 39, 901–905. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Bramante, C.; Versiani, M.; Moldauer, B.; Topham, G.; Gutmann, J.; Nuñez, A.; Duarte, M.H.; Abella, F. Comparative accuracy of the Clearing Technique, CBCT and Micro-CT methods in studying the mesial root canal configuration of mandibular first molars. Int. Endod. J. 2017, 50, 90–96. [Google Scholar] [CrossRef]
- Kim, Y.; Chang, S.-W.; Lee, J.-K.; Chen, I.-P.; Kaufman, B.; Jiang, J.; Cha, B.Y.; Zhu, Q.; Safavi, K.E.; Kum, K.-Y. A micro-computed tomography study of canal configuration of multiple-canalled mesiobuccal root of maxillary first molar. Clin. Oral Investig. 2013, 17, 1541–1546. [Google Scholar] [CrossRef]
- Marceliano-Alves, M.F.; Lima, C.O.; Bastos, L.G.d.P.M.N.; Bruno, A.M.V.; Vidaurre, F.; Coutinho, T.M.; Fidel, S.R.; Lopes, R.T. Mandibular mesial root canal morphology using micro-computed tomography in a Brazilian population. Aust. Endod. J. 2019, 45, 51–56. [Google Scholar] [CrossRef]
- Leoni, G.B.; Versiani, M.A.; Pécora, J.D.; de Sousa-Neto, M.D. Micro–computed tomographic analysis of the root canal morphology of mandibular incisors. J. Endod. 2014, 40, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Filpo-Perez, C.; Bramante, C.M.; Villas-Boas, M.H.; Duarte, M.A.H.; Versiani, M.A.; Ordinola-Zapata, R. Micro–computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. J. Endod. 2015, 41, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Marceliano-Alves, M.; Alves, F.R.F.; de Melo Mendes, D.; Provenzano, J.C. Micro–computed tomography analysis of the root canal morphology of palatal roots of maxillary first molars. J. Endod. 2016, 42, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Love, R. A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int. Endod. J. 2011, 44, 210–217. [Google Scholar] [CrossRef]
- De Almeida, M.M.; Bernardineli, N.; Ordinola-Zapata, R.; Villas-Bôas, M.H.; Amoroso-Silva, P.A.; Brandao, C.G.; Guimaraes, B.M.; De Moraes, I.G.; Húngaro-Duarte, M.A. Micro–computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J. Endod. 2013, 39, 1529–1533. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Martins, J.; Bramante, C.; Villas-Boas, M.; Duarte, M.; Versiani, M. Morphological evaluation of maxillary second molars with fused roots: A Micro-CT study. Int. Endod. J. 2017, 50, 1192–1200. [Google Scholar] [CrossRef]
- Wolf, T.G.; Paqué, F.; Zeller, M.; Willershausen, B.; Briseño-Marroquín, B. Root canal morphology and configuration of 118 mandibular first molars by means of micro–computed tomography: An ex vivo study. J. Endod. 2016, 42, 610–614. [Google Scholar] [CrossRef]
- Wolf, T.G.; Paqué, F.; Woop, A.-C.; Willershausen, B.; Briseño-Marroquín, B. Root canal morphology and configuration of 123 maxillary second molars by means of Micro-CT. Int. J. Oral Sci. 2017, 9, 33–37. [Google Scholar] [CrossRef]
- Wolf, T.G.; Kozaczek, C.; Campus, G.; Paqué, F.; Wierichs, R.J. Root Canal Morphology of 116 Maxillary Second Premolars by Micro–Computed Tomography in a Mixed Swiss-German Population with Systematic Review. J. Endod. 2020, 46, 1639–1647. [Google Scholar] [CrossRef]
- Zhang, W.; Tang, Y.; Liu, C.; Shen, Y.; Feng, X.; Gu, Y. Root and root canal variations of the human maxillary and mandibular third molars in a Chinese population: A micro–computed tomographic study. Arch. Oral Biol. 2018, 95, 134–140. [Google Scholar] [CrossRef]
- Marceliano-Alves, M.F.; de Lima, C.O.; Augusto, C.M.; Almeida Barbosa, A.F.; Vieira Bruno, A.M.; Rosa, A.M.; Lopes, R.T. The internal root canal morphology of single-rooted mandibular canines revealed by micro-computed tomography. J. Conserv. Dent. JCD 2018, 21, 588–591. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Cristancho, A.; González-Osuna, L.; Poblete, D.; Cafferata, E.A.; Carvajal, P.; Lozano, C.P.; Vernal, R. Micro-tomographic characterization of the root and canal system morphology of mandibular first premolars in a Chilean population. Sci. Rep. 2021, 11, 93. [Google Scholar] [CrossRef]
- Espir, C.G.; Nascimento, C.A.; Guerreiro-Tanomaru, J.M.; Bonetti-Filho, I.; Tanomaru-Filho, M. Radiographic and micro-computed tomography classification of root canal morphology and dentin thickness of mandibular incisors. J. Conserv. Dent. JCD 2018, 21, 57–62. [Google Scholar] [CrossRef]
- Wolf, T.G.; Paqué, F.; Betz, P.; Willershausen, B.; Briseño-Marroquín, B. Micro-CT assessment of internal morphology and root canal configuration of non C-shaped mandibular second molars. Swiss Dent. J. 2017, 127, 513–519. [Google Scholar]
- Divine, K.A.; McClanahan, S.B.; Fok, A. Anatomic Analysis of Palatal Roots of Maxillary Molars Using Micro–computed Tomography. J. Endod. 2019, 45, 724–728. [Google Scholar] [CrossRef] [PubMed]
- Camargo Dos Santos, B.; Pedano, M.S.; Giraldi, C.K.; De Oliveira, J.C.M.; Lima, I.C.B.; Lambrechts, P. Mesiobuccal Root Canal Morphology of Maxillary First Molars in a Brazilian Sub-Population—A Micro-CT Study. Eur. Endod. J. 2020, 5, 105–111. [Google Scholar] [CrossRef]
- Tomaszewska, I.M.; Skinningsrud, B.; Jarzębska, A.; Pękala, J.R.; Tarasiuk, J.; Iwanaga, J. Internal and external morphology of mandibular molars: An original Micro-CT study and meta-analysis with review of implications for endodontic therapy. Clin. Anat. 2018, 31, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.O.; Magalhães, L.T.; Marceliano-Alves, M.F.; de Oliveira, P.Y.; Lacerda, M.F. Internal Lower Incisor Morphology revealed by Computerized Microtomography. Acta Odontol. Latinoam. AOL 2020, 33, 33–37. [Google Scholar] [CrossRef]
- Fu, Y.; Gao, Y.; Gao, Y.; Tan, X.; Zhang, L.; Huang, D. Three-dimensional analysis of coronal root canal morphology of 136 permanent mandibular first molars by micro-computed tomography. J. Dent. Sci. 2022, 17, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Grande, N.M.; Plotino, G.; Pecci, R.; Bedini, R.; Pameijer, C.H.; Somma, F. Micro–computerized tomographic analysis of radicular and canal morphology of premolars with long oval canals. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, e70–e76. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Bramante, C.M.; Villas-Boas, M.H.; Cavenago, B.C.; Duarte, M.H.; Versiani, M.A. Morphologic micro-computed tomography analysis of mandibular premolars with three root canals. J. Endod. 2013, 39, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Gu, Y. Assessment of the presence of a second mesiobuccal canal in maxillary first molars according to the location of the main mesiobuccal canal-a micro-computed tomographic study. Clin. Oral Investig. 2021, 25, 3937–3944. [Google Scholar] [CrossRef] [PubMed]
- Dou, L.; Li, D.; Xu, T.; Tang, Y.; Yang, D. Root anatomy and canal morphology of mandibular first premolars in a Chinese population. Sci. Rep. 2017, 7, 750. [Google Scholar] [CrossRef]
- Alashiry, M.K.; Zeitoun, R.; Elashiry, M.M. Prevalence of middle mesial and middle distal canals in mandibular molars in an Egyptian subpopulation using micro-computed tomography. Niger. J. Clin. Pr. 2020, 23, 534–538. [Google Scholar] [CrossRef]
- Qiao, X.; Xu, T.; Chen, L.; Yang, D. Analysis of Root Canal Curvature and Root Canal Morphology of Maxillary Posterior Teeth in Guizhou, China. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e928758. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, B.; Lacoste, J.P.; Gaborit, N.; Brossard, G.; Cruard, A.; Baslé, M.F.; Chappard, D. Microcomputed tomography used in the analysis of the morphology of root canals in extracted wisdom teeth. Br. J. Oral Maxillofac. Surg. 2006, 44, 240–244. [Google Scholar] [CrossRef]
- Chen, M.; Wang, H.; Tsauo, C.; Huang, D.; Zhou, X.; He, J.; Gao, Y. Micro-computed tomography analysis of root canal morphology and thickness of crown and root of mandibular incisors in Chinese population. Clin. Oral Investig. 2022, 26, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Kyaw Moe, M.M.; Jo, H.J.; Ha, J.H.; Kim, S.K. Root Canal Configuration of Burmese (Myanmar) Maxillary First Molar: A Micro-Computed Tomography Study. Int. J. Dent. 2021, 2021, 3433343. [Google Scholar] [CrossRef]
- Elnour, M.; Khabeer, A.; AlShwaimi, E. Evaluation of root canal morphology of maxillary second premolars in a Saudi Arabian sub-population: An in vitro microcomputed tomography study. Saudi Dent. J. 2016, 28, 162–168. [Google Scholar] [CrossRef]
- Versiani, M.A.; Pécora, J.D.; Sousa-Neto, M.D. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int. Endod. J. 2013, 46, 800–807. [Google Scholar] [CrossRef]
- Wolf, T.G.; Anderegg, A.L.; Haberthür, D.; Khoma, O.Z.; Schumann, S.; Boemke, N.; Wierichs, R.J.; Hlushchuk, R. Internal morphology of 101 mandibular canines of a Swiss-German population by means of Micro-CT: An ex vivo study. Sci. Rep. 2021, 11, 21281. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Li, X.; Liu, N.; Ye, L.; An, J.; Nie, X.; Liu, L.; Deng, M. A micro-computed tomography study of the root canal morphology of the mandibular first premolar in a population from southwestern China. Clin. Oral Investig. 2013, 17, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.T.; de Oliveira-Santos, C.; Bernardineli, N.; Duarte, M.A.H.; Bramante, C.M.; Minotti-Bonfante, P.G.; Ordinola-Zapata, R. Prevalence and morphometric analysis of three-rooted mandibular first molars in a Brazilian subpopulation. J. Appl. Oral Sci. 2016, 24, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.G.; Kozaczek, C.; Siegrist, M.; Betthäuser, M.; Paqué, F.; Briseño-Marroquín, B. An Ex Vivo Study of Root Canal System Configuration and Morphology of 115 Maxillary First Premolars. J. Endod. 2020, 46, 794–800. [Google Scholar] [CrossRef]
- Şallı, G.A.; Egil, E. Evaluation of mesial root canal configuration of mandibular first molars using micro-computed tomography. Imaging Sci. Dent. 2021, 51, 383–388. [Google Scholar] [CrossRef]
- Somma, F.; Leoni, D.; Plotino, G.; Grande, N.M.; Plasschaert, A. Root canal morphology of the mesiobuccal root of maxillary first molars: A micro-computed tomographic analysis. Int. Endod. J. 2009, 42, 165–174. [Google Scholar] [CrossRef]
- Tomaszewska, I.M.; Jarzębska, A.; Skinningsrud, B.; Pękala, P.A.; Wroński, S.; Iwanaga, J. An original Micro-CT study and meta-analysis of the internal and external anatomy of maxillary molars-implications for endodontic treatment. Clin. Anat. 2018, 31, 838–853. [Google Scholar] [CrossRef]
- Yamada, M.; Ide, Y.; Matsunaga, S.; Kato, H.; Nakagawa, K. Three-dimensional analysis of mesiobuccal root canal of Japanese maxillary first molar using Micro-CT. Bull. Tokyo Dent. Coll. 2011, 52, 77–84. [Google Scholar] [CrossRef]
- Park, J.W.; Lee, J.K.; Ha, B.H.; Choi, J.H.; Perinpanayagam, H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using micro-computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 437–442. [Google Scholar] [CrossRef]
- Keleş, A.; Keskin, C.; Alqawasmi, R.; Versiani, M.A. Micro-computed tomographic analysis of the mesial root of mandibular first molars with bifid apex. Arch. Oral Biol. 2020, 117, 104792. [Google Scholar] [CrossRef]
- Versiani, M.A.; Keleș, A. Applications of Micro-CT technology in endodontics. In Micro-Computed Tomography (Micro-CT) in Medicine and Engineering; Springer: Berlin/Heidelberg, Germany, 2020; pp. 183–211. [Google Scholar]
- Peters, O.A.; Laib, A.; Rüegsegger, P.; Barbakow, F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J. Dent. Res. 2000, 79, 1405–1409. [Google Scholar] [CrossRef] [PubMed]
- Ayranci, L.B.; Yeter, K.Y.; Arslan, H.; Kseoğlu, M. Morphology of apical foramen in permanent molars and premolars in a Turkish population. Acta Odontol. Scand 2013, 71, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Guldberg, R.E.; Lin, A.S.; Coleman, R.; Robertson, G.; Duvall, C. Microcomputed tomography imaging of skeletal development and growth. Birth Defects Res. Part C Embryo Today Rev. 2004, 72, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Chen, Z.; Liu, J.; Wu, M.; Yang, J.; Zhu, Y.; Lu, W.W.; Ruan, C. 3D-printed pre-tapped-hole scaffolds facilitate one-step surgery of predictable alveolar bone augmentation and simultaneous dental implantation. Compos. Part B Eng. 2022, 229, 109461. [Google Scholar] [CrossRef]
- Fang, H.; Zhu, D.; Yang, Q.; Chen, Y.; Zhang, C.; Gao, J.; Gao, Y. Emerging zero-dimensional to four-dimensional biomaterials for bone regeneration. J. Nanobiotech. 2022, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Swain, M.V.; Xue, J. State of the art of Micro-CT applications in dental research. Int. J. Oral Sci. 2009, 1, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Grande, N.M.; Pecci, R.; Bedini, R.; Pameijer, C.H.; Somma, F. Three-dimensional imaging using microcomputed tomography for studying tooth macromorphology. J. Am. Dent. Assoc. 2006, 137, 1555–1561. [Google Scholar] [CrossRef]
- Rhodes, J.; Ford, T.P.; Lynch, J.; Liepins, P.; Curtis, R. Micro-computed tomography: A new tool for experimental endodontology. Int. Endod. J. 1999, 32, 165–170. [Google Scholar] [CrossRef]
- Marroquín, B.B.; El-Sayed, M.A.; Willershausen-Zönnchen, B. Morphology of the physiological foramen: I. Maxillary and mandibular molars. J. Endod. 2004, 30, 321–328. [Google Scholar] [CrossRef]
- Smith, T.M.; Harvati, K.; Olejniczak, A.J.; Reid, D.J.; Hublin, J.J.; Panagopoulou, E. Brief communication: Dental development and enamel thickness in the Lakonis Neanderthal molar. Am. J. Phys. Anthropol. 2009, 138, 112–118. [Google Scholar] [CrossRef]
- Cheung, L.H.; Cheung, G.S. Evaluation of a rotary instrumentation method for C-shaped canals with micro-computed tomography. J. Endod. 2008, 34, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Luan, Q.; Desta, T.; Chehab, L.; Sanders, V.; Plattner, J.; Graves, D. Inhibition of experimental periodontitis by a topical boron-based antimicrobial. J. Dent. Res. 2008, 87, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Rahemtulla, F.; Zhang, P.; Beck, P.; Thomas, H.F. Different enamel and dentin mineralization observed in VDR deficient mouse model. Arch. Oral Biol. 2009, 54, 299–305. [Google Scholar] [CrossRef]
- Freilich, M.; Shafer, D.; Wei, M.; Kompalli, R.; Adams, D.; Kuhn, L. Implant system for guiding a new layer of bone. Computed microtomography and histomorphometric analysis in the rabbit mandible. Clin. Oral Implant. Res. 2009, 20, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.; Yong, R.; Surman, T.; Rajion, Z.; Ranjitkar, S. Application of three-dimensional computed tomography in craniofacial clinical practice and research. Aust. Dent. J. 2014, 59, 174–185. [Google Scholar] [CrossRef]
- Loch, C.; Schwass, D.R.; Kieser, J.A.; Fordyce, R.E. Use of micro-computed tomography for dental studies in modern and fossil odontocetes: Potential applications and limitations. NAMMCO Sci. Publ. 2018, 10, 1–24. [Google Scholar] [CrossRef][Green Version]
- Peters, O.A.; Boessler, C.; Paqué, F. Root canal preparation with a novel nickel-titanium instrument evaluated with micro-computed tomography: Canal surface preparation over time. J. Endod. 2010, 36, 1068–1072. [Google Scholar] [CrossRef]
- Xu, T.; Tay, F.R.; Gutmann, J.L.; Fan, B.; Fan, W.; Huang, Z.; Sun, Q. Micro–computed tomography assessment of apical accessory canal morphologies. J. Endod. 2016, 42, 798–802. [Google Scholar] [CrossRef]
- Baratto Filho, F.; Zaitter, S.; Haragushiku, G.A.; de Campos, E.A.; Abuabara, A.; Correr, G.M. Analysis of the Internal Anatomy of Maxillary First Molars by Using Different Methods. J. Endod. 2009, 35, 337–342. [Google Scholar] [CrossRef]
- Ahmed, H.; Hashem, A. Accessory roots and root canals in human anterior teeth: A review and clinical considerations. Int. Endod. J. 2016, 49, 724–736. [Google Scholar] [CrossRef]
- Altunsoy, M.; Ok, E.; Nur, B.G.; Aglarci, O.S.; Gungor, E.; Colak, M. A cone-beam computed tomography study of the root canal morphology of anterior teeth in a Turkish population. Eur. J. Dent. 2014, 8, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Amardeep, N.S.; Raghu, S.; Natanasabapathy, V. Root canal morphology of permanent maxillary and mandibular canines in Indian population using cone beam computed tomography. Anat. Res. Int. 2014, 2014, 731859. [Google Scholar]
- Nogueira Leal da Silva, E.J.; Queiroz de Castro, R.W.; Nejaim, Y.; Vespasiano Silva, A.I.; Haiter-Neto, F.; Silberman, A.; Cohenca, N. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: An in-vivo study. Quintessence Int. 2016, 47, 19–24. [Google Scholar]
- Miyashita, M.; Kasahara, E.; Yasuda, E.; Yamamoto, A.; Sekizawa, T. Root canal system of the mandibular incisor. J. Endod. 1997, 23, 479–484. [Google Scholar] [CrossRef]
- Kartal, N.; Yanıkoğlu, F.Ç. Root canal morphology of mandibular incisors. J. Endod. 1992, 18, 562–564. [Google Scholar] [CrossRef]
- Sert, S.; Bayirli, G.S. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J. Endod. 2004, 30, 391–398. [Google Scholar] [CrossRef]
- Madeira, M.C.; Hetem, S. Incidence of bifurcations in mandibular incisors. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 589–591. [Google Scholar] [CrossRef]
- Seo, M.; Park, D. C-shaped root canals of mandibular second molars in a Korean population: Clinical observation and in vitro analysis. Int. Endod. J. 2004, 37, 139–144. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, J.; Yang, H.-B.; Han, X.; Yu, Y. Incidence of C-shaped root canal systems in mandibular second molars in the native Chinese population by analysis of clinical methods. Int. J. Oral Sci. 2012, 4, 161–165. [Google Scholar] [CrossRef]
- Zheng, Q.; Zhang, L.; Zhou, X.; Wang, Q.; Wang, Y.; Tang, L.; Song, F.; Huang, D. C-shaped root canal system in mandibular second molars in a Chinese population evaluated by cone-beam computed tomography. Int. Endod. J. 2011, 44, 857–862. [Google Scholar] [CrossRef]
- Fan, B.; Cheung, G.S.; Fan, M.; Gutmann, J.L.; Bian, Z. C-shaped canal system in mandibular second molars: Part I—anatomical features. J. Endod. 2004, 30, 899–903. [Google Scholar] [CrossRef]
- Min, Y.; Fan, B.; Cheung, G.S.; Gutmann, J.L.; Fan, M. C-shaped canal system in mandibular second molars Part III: The morphology of the pulp chamber floor. J. Endod. 2006, 32, 1155–1159. [Google Scholar] [CrossRef] [PubMed]
- Mohara, N.T.; Coelho, M.S.; de Queiroz, N.V.; Borreau, M.L.S.; Nishioka, M.M.; de Jesus Soares, A.; Frozoni, M. Root anatomy and canal configuration of maxillary molars in a Brazilian subpopulation: A 125-μm cone-beam computed tomographic study. Eur. J. Dent. 2019, 13, 082–087. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, G.D.; Gamieldien, M.Y.; Tredoux, S.; Vally, Z.I. Root and canal configurations of maxillary premolars in a South African subpopulation using cone beam computed tomography and two classification systems. J. Oral Sci. 2020, 62, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-h.; Bao, S.-j.; Yang, X.-w.; Tian, X.-m.; Wei, B.; Zheng, Y.-l. Symmetry of root anatomy and root canal morphology in maxillary premolars analyzed using cone-beam computed tomography. Arch. Oral Biol. 2018, 94, 84–92. [Google Scholar] [CrossRef]
- Guo, J.; Vahidnia, A.; Sedghizadeh, P.; Enciso, R. Evaluation of root and canal morphology of maxillary permanent first molars in a North American population by cone-beam computed tomography. J. Endod. 2014, 40, 635–639. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).