
Effectiveness of Tocilizumab in Patients with Severe or Critical Lung Involvement in COVID-19: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
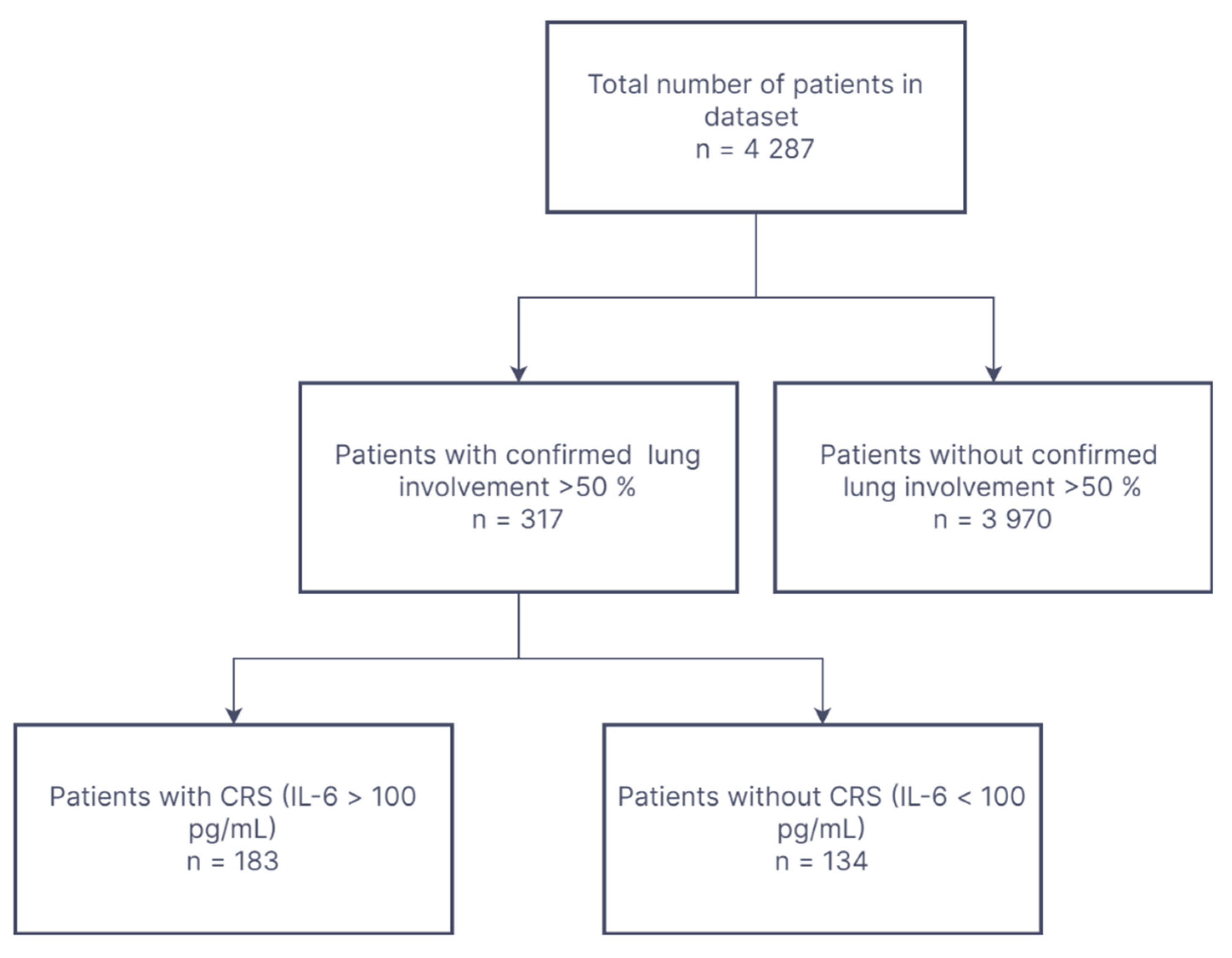
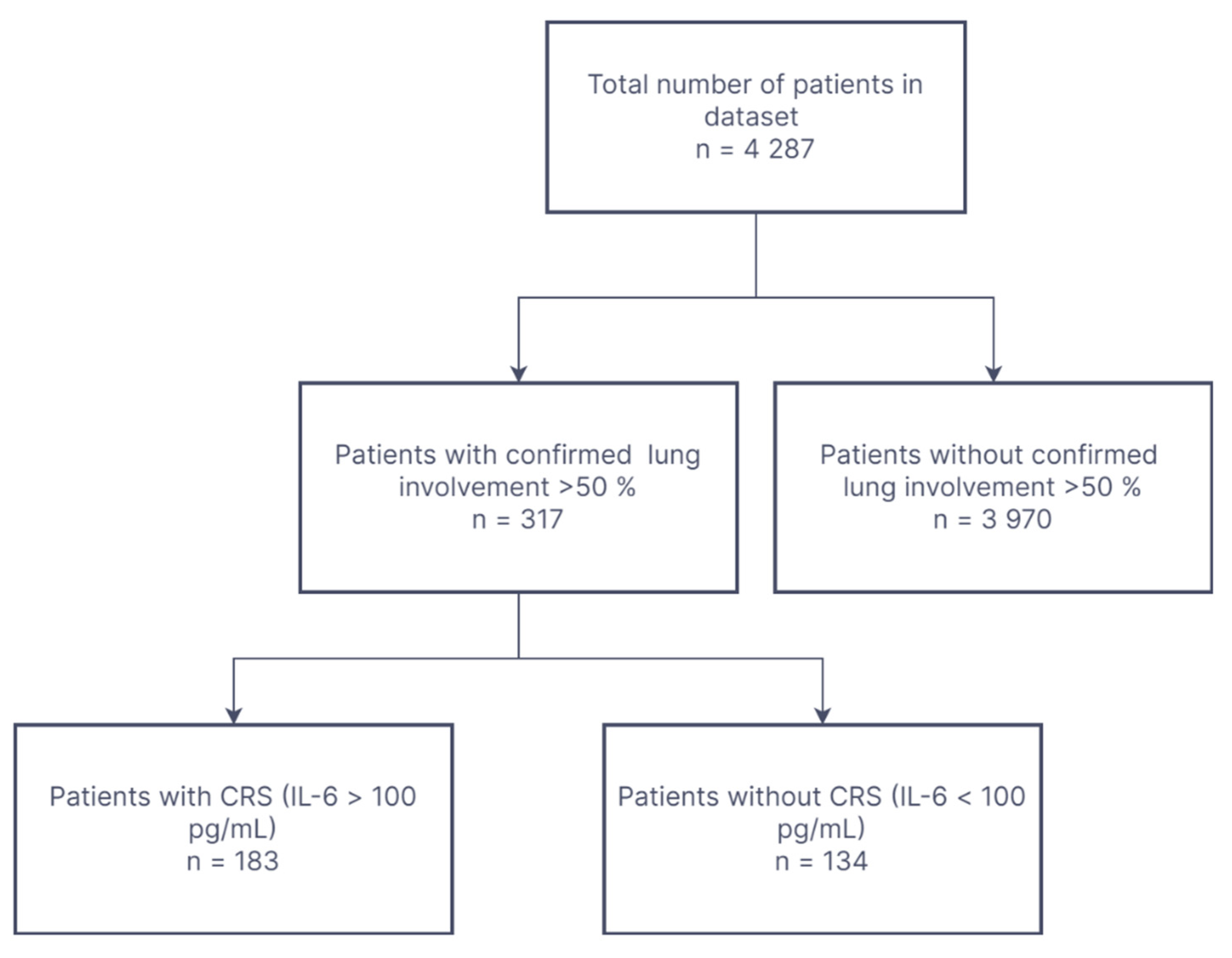
2.1. Study Groups
- -
- Antibiotic therapy (intravenous ceftriaxon was the drug of choice but could vary depending on the patient’s condition);
- -
- Oxygen therapy (low- or high-flow oxygen therapy or mechanical ventilation were used, while no extracorporeal ventilation was used among patients included in this analysis);
- -
- Intravenous rehydration based on individual needs;
- -
- Dexamethasone administered intravenously at a dose of at least 6 mg per day;
- -
- Low-molecular-weight heparin administered in prophylactic or therapeutic doses depending on patient condition.
- -
- CT-confirmed COVID-19-associated severe (lung involvement 50–75%) or critical (lung involvement > 75%) pneumonia;
- -
- Biochemical indicators of cytokine release storm IL-6 level > 100 pg/mL (the level of interleukin-6 was established on the basis of the recommendations [21]);
- -
- Age > 18 years.
2.2. Ethical Issues
2.3. Sampling and Data Collection Methodology
2.4. Statistics
3. Results
3.1. Clinical Characteristics of Patients with COVID-19
3.2. Clinical and Laboratory Data on TCZ Treated vs. Control Group
3.3. Factors Associated with ICU Admission in the Analyzed Group
3.4. Overall Mortality Risk
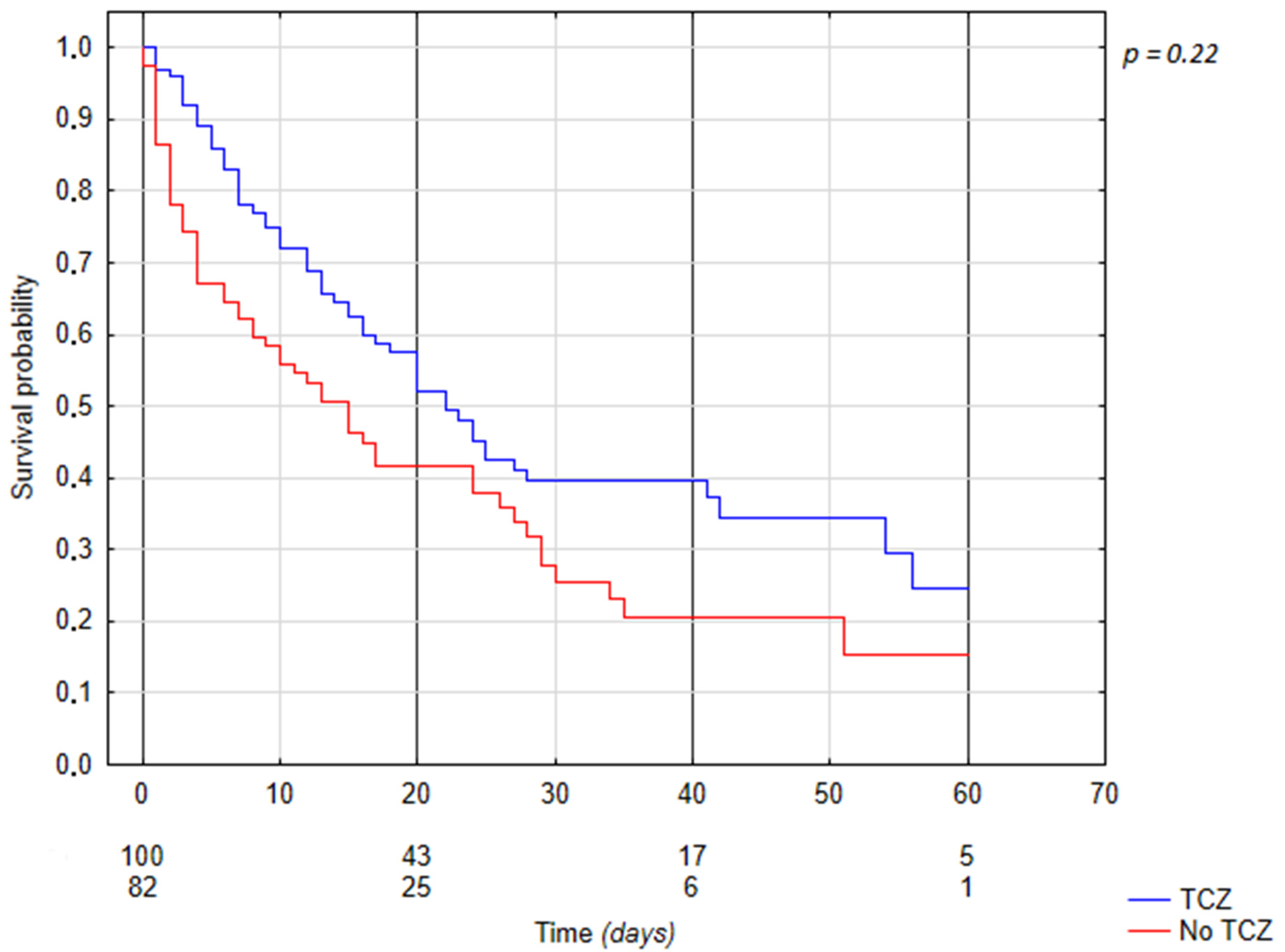
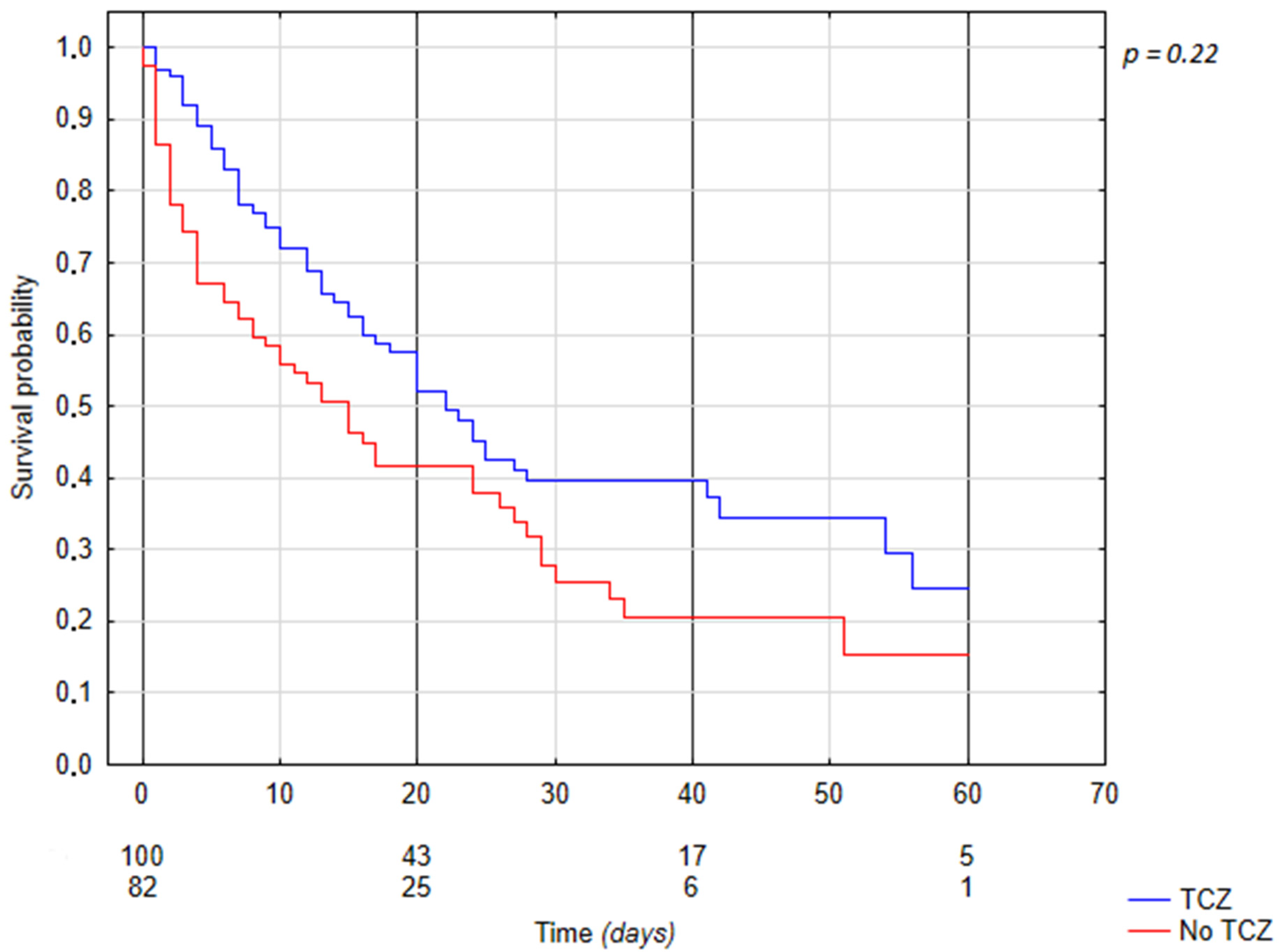
3.5. Tocilizumab Associated Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 12 March 2022).
- Son, K.B.; Lee, T.J.; Hwang, S.S. Disease severity classification and COVID-19 outcomes, Republic of Korea. Bull. World Health Organ. 2021, 99, 62. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- COVID-19: Epidemiology, Clinical Features, and Prognosis of the Critically Ill Adult—Up To Date. Available online: https://www.uptodate.com/contents/COVID-19-epidemiology-clinical-features-and-prognosis-of-the-critically-ill-adult (accessed on 26 March 2022).
- Li, X.; To, K.K.W. Biomarkers for severe COVID-19. eBioMedicine 2021, 68, 103405. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Ma, Y.; Ruan, L.; Li, D.; Lu, C.; Huang, L. Comparing different machine learning techniques for predicting COVID-19 severity. Infect. Dis. Poverty 2022, 11, 19. [Google Scholar] [CrossRef]
- Wiśniewska, H.; Skonieczna-Żydecka, K.; Parczewski, M.; Niścigorska-Olsen, J.; Karpińska, E.; Hornung, M.; Jurczyk, K.; Witak-Jędra, M.; Laurans, Ł.; Maciejewska, K.; et al. Hepatotropic Properties of SARS-CoV-2-Preliminary Results of Cross-Sectional Observational Study from the First Wave COVID-19 Pandemic. J. Clin. Med. 2021, 10, 672. [Google Scholar] [CrossRef]
- Sanli, D.E.T.; Yildirim, D.; Sanli, A.N.; Erozan, N.; Husmen, G.; Altundag, A.; Tuzuner, F.; Dikensoy, O.; Kirisoglu, C.E. Predictive value of CT imaging findings in COVID-19 pneumonia at the time of first-screen regarding the need for hospitalization or intensive care unit. Diagn. Interv. Radiol. 2021, 27, 599. [Google Scholar] [CrossRef]
- Yang, R.; Li, X.; Liu, H.; Zhen, Y.; Zhang, X.; Xiong, Q.; Luo, Y.; Gao, C.; Zeng, W. Chest ct severity score: An imaging tool for assessing severe COVID-19. Radiol. Cardiothorac. Imaging 2020, 2, e200047. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated with Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and High-Resolution CT Features of the COVID-19 Infection: Comparison of the Initial and Follow-up Changes. Investig. Radiol. 2020, 55, 332–339. [Google Scholar] [CrossRef]
- Jalaber, C.; Lapotre, T.; Morcet-Delattre, T.; Ribet, F.; Jouneau, S.; Lederlin, M. Chest CT in COVID-19 pneumonia: A review of current knowledge. Diagn. Interv. Imaging 2020, 101, 431–437. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of April 26, 2021. Pol. Arch. Intern. Med. 2021, 131, 48–496. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Flisiak, R.; Jaroszewicz, J.; Rogalska, M.; Łapiński, T.; Berkan-Kawińska, A.; Bolewska, B.; Tudrujek-Zdunek, M.; Kozielewicz, D.; Rorat, M.; Leszczyński, P.; et al. Tocilizumab Improves the Prognosis of COVID-19 in Patients with High IL-6. J. Clin. Med. 2021, 10, 1583. [Google Scholar] [CrossRef] [PubMed]
- Cabaro, S.; D’Esposito, V.; Di Matola, T.; Sale, S.; Cennamo, M.; Terracciano, D.; Parisi, V.; Oriente, F.; Portella, G.; Beguinot, F.; et al. Cytokine signature and COVID-19 prediction models in the two waves of pandemics. Sci. Rep. 2021, 11, 20793. [Google Scholar] [CrossRef] [PubMed]
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Salama, C.; Han, J.; Yau, L.; Reiss, W.G.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in Patients Hospitalized with COVID-19 Pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs Standard Care on Clinical Worsening in Patients Hospitalized with COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with COVID-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of March 31, 2020. Pol. Arch. Intern. Med. 2020, 130, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Radulescu, A.; Istrate, A.; Muntean, M. Treatment with Tocilizumab in Adult Patients with Moderate to Critical COVID-19 Pneumonia: A Single-Center Retrospective Study. Int. J. Infect. Dis. 2022, 117, 1–7. [Google Scholar] [CrossRef]
- Word Health Organization. Therapeutics and COVID-19: Living Guideline; Word Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Mahendra, M.; Nuchin, A.; Kumar, R.; Shreedhar, S.; Mahesh, P.A. Predictors of mortality in patients with severe COVID-19 pneumonia—A retrospective study. Adv. Respir. Med. 2021, 89, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Remap-Cap Investigators. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Shankar-Hari, M.; Vale, C.L.; Godolphin, P.J.; Fisher, D.; Higgins, J.P.T.; Spiga, F.; Savović, J.; Tierney, J.; Baron, G.; et al. Association Between Administration of IL-6 Antagonists and Mortality Among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Baseline Characteristics of All Patients Included in the Study | ||||
|---|---|---|---|---|
| n | Median | Lower Quartile | Upper Quartile | |
| Age, years | 182 | 68.50 | 61.00 | 76.00 |
| Percentage of Lung Involvement, % | 182 | 59.61 | 54.52 | 67.38 |
| WBC, ×103/μL | 181 | 9.05 | 6.37 | 11.88 |
| NEU, ×103/μL | 181 | 7.10 | 5.20 | 9.90 |
| LYM, ×103/μL | 181 | 0.80 | 0.50 | 1.10 |
| RBC, ×106/μL | 181 | 4.57 | 4.15 | 4.91 |
| HGB g/dL | 181 | 13.60 | 12.30 | 14.70 |
| HCT, % | 181 | 39.50 | 36.10 | 42.70 |
| Platelets, ×103/μL | 181 | 231.00 | 183.00 | 284.00 |
| Procalcitonin, ng/mL | 179 | 0.35 | 0.17 | 0.65 |
| CRP, mg/L | 182 | 183.97 | 133.75 | 258.28 |
| IL-6, pg/mL | 182 | 177.50 | 129.00 | 287.00 |
| LDH, U/L | 176 | 630.00 | 521.50 | 783.50 |
| D-dimer, μg/L | 178 | 1195.50 | 631.00 | 4387.00 |
| Creatinine, mg/dL | 182 | 1.13 | 0.87 | 1.48 |
| AST, U/L | 176 | 59.00 | 47.00 | 82.00 |
| ALT, U/L | 176 | 39.00 | 26.50 | 60.50 |
| Troponin T, ng/L | 174 | 26.80 | 15.70 | 49.00 |
| GGTP, U/L | 167 | 63.00 | 36.00 | 127.00 |
| Bilirubin total, mg/dL | 167 | 0.59 | 0.42 | 0.77 |
| Characteristics of Groups Admitted to ICU vs. Not Admitted to ICU | Cox Proportional Hazards Model for ICU Admission | ||||||
|---|---|---|---|---|---|---|---|
| ICU n = 59 | Non-ICU n = 123 | p | p Value | Hazard Ratio (HR) | Lower 95%CI HR Value | Upper 95%CI HR Value | |
| Percentage of Lung Involvement, median (IQR) | 59.06 (54.39–63.76) | 63.51 (54.61–71.39) | 0.049 | 0.161 | 1024 | 0.991 | 1058 |
| RBC, ×106/μL, median (IQR) | 4475 (4.04–4.86) | 4.7 (4.33–5) | 0.022 | 0.441 | 1211 | 0.744 | 1974 |
| CRP, mg/L, median (IQR) | 175.2 (125.4–249.81) | 205.71 (156.79–277.91) | 0.021 | 0.004 | 1005 | 1002 | 1009 |
| D-dimers, μg/L, median (IQR) | 1488 (660–6501) | 868 (594–1923) | 0.009 | 0.158 | 1000 | 1000 | 1000 |
| Troponin T, ng/L, median (IQR) | 30.65 (18.7–54.25) | 21.2 (12.8–39.1) | 0.034 | 0.321 | 1002 | 0.998 | 1006 |
| Age Group 18–65 (reference) vs. 65+ | 34 (58%) | 33 (27%) | 0.001 | 0.517 | 1236 | 0.651 | 2345 |
| Hypertension n (%) Yes (reference) | 38 (60%) | 25(40%) | Chi-square Pearson p = 0.001 | 0.468 | 0.780 | 0.398 | 1526 |
| Diabetes, n (%) Yes (reference) | 26 (68%) | 12 (32%) | Chi-square Pearson p = 0.001 | 0.021 | 2117 | 1119 | 4002 |
| Remdesivir, n (%) Yes (reference) | 28 (47%) | 29 (24%) | Chi-square Pearson p = 0.001 | 0.645 | 1148 | 0.637 | 2070 |
| Tocilizumab, n (%) Yes (reference) | 29 (49%) | 71 (58%) | Chi-square Pearson p = 0.277 | 0.064 | 0.575 | 0.320 | 1032 |
| Characteristics of Surviving Group Compared to the Patients Who Died | Cox Proportional Hazards Model for Mortality | ||||||
|---|---|---|---|---|---|---|---|
| Survived n = 67 | Died n = 115 | p Value | p Value | Hazard Ratio (HR) | Lower 95%CI HR Value | Upper 95%CI HR Value | |
| Percentage of Lung Involvement, median (IQR) | 56.73 (53.71–63.76) | 61.11 (54.78–68.34) | 0.051 | 0.199 | 1017 | 0.992 | 1044 |
| LYM, ×103/μL, median (IQR) | 0.9 (0.6–1.3) | 0.7 (0.5–1.1) | 0.024 | 0.438 | 0.854 | 0.574 | 1273 |
| RBC, ×106/μL, median (IQR) | 4.78 (4.25–5.12) | 4.46 (4.05–4.82) | 0.004 | 0.797 | 0.891 | 0.368 | 2157 |
| HGB g/dL, median (IQR) | 14 (12.8–14.8) | 13.4 (12–14.4) | 0.016 | 0.867 | 0.957 | 0.570 | 1607 |
| HCT, %, median (IQR) | 41.2 (37.5–43.3) | 39.2 (35.4–41.8) | 0.026 | 0.826 | 1024 | 0.834 | 1256 |
| ALT, U/L, median (IQR) | 44 (36–69) | 33.5 (23–55) | 0.001 | 0.638 | 0.999 | 0.992 | 1006 |
| Troponin T, ng/L, median (IQR) | 19.1 (11.8–27.1) | 34.55 (21.5–60.4) | 0.000 | 0.013 | 1002 | 1001 | 1004 |
| GGTP, U/L, median (IQR) | 76.5 (45.5–158.5) | 47 (31–95) | 0.001 | 0.092 | 0.998 | 0.995 | 1001 |
| Age Group 18–65 (reference) vs. 65+ | 35 (52%) | 32 (28%) | Chi-square Pearson p = 0.001 | 0.003 | 0.466 | 0.286 | 0.761 |
| Gender, n (%) Male(reference) | 52 (78%) | 72 (63%) | Chi-square Pearson p = 0.036 | 0.966 | 1012 | 0.611 | 1676 |
| Procalcitonin, n (%) <2.0 ng/mL (reference) | 65 (98%) | 100 (88%) | Chi-square Pearson p = 0.016 | 0.683 | 0.840 | 0.364 | 1940 |
| Creatinine Level, n (%) <2.0 mg/dL (reference) | 66 (99%) | 97 (84%) | Chi-square Pearson p = 0.002 | 0.048 | 0.499 | 0.251 | 0.993 |
| Diabetes, n (%) Yes | 11 (16%) | 27 (23%) | Chi-square Pearson p = 0.258 | 0.346 | 0.789 | 0.482 | 1292 |
| Tocilizumab, n (%) Yes (reference) | 42 (63%) | 58 (50%) | Chi-square Pearson p = 0.109 | 0.032 | 0.615 | 0.394 | 0.956 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chober, D.; Aksak-Wąs, B.; Bobrek-Lesiakowska, K.; Budny-Finster, A.; Hołda, E.; Mieżyńska-Kurtycz, J.; Jamro, G.; Parczewski, M. Effectiveness of Tocilizumab in Patients with Severe or Critical Lung Involvement in COVID-19: A Retrospective Study. J. Clin. Med. 2022, 11, 2286. https://doi.org/10.3390/jcm11092286
Chober D, Aksak-Wąs B, Bobrek-Lesiakowska K, Budny-Finster A, Hołda E, Mieżyńska-Kurtycz J, Jamro G, Parczewski M. Effectiveness of Tocilizumab in Patients with Severe or Critical Lung Involvement in COVID-19: A Retrospective Study. Journal of Clinical Medicine. 2022; 11(9):2286. https://doi.org/10.3390/jcm11092286
Chicago/Turabian StyleChober, Daniel, Bogusz Aksak-Wąs, Katarzyna Bobrek-Lesiakowska, Anna Budny-Finster, Ewa Hołda, Joanna Mieżyńska-Kurtycz, Grzegorz Jamro, and Miłosz Parczewski. 2022. "Effectiveness of Tocilizumab in Patients with Severe or Critical Lung Involvement in COVID-19: A Retrospective Study" Journal of Clinical Medicine 11, no. 9: 2286. https://doi.org/10.3390/jcm11092286
APA StyleChober, D., Aksak-Wąs, B., Bobrek-Lesiakowska, K., Budny-Finster, A., Hołda, E., Mieżyńska-Kurtycz, J., Jamro, G., & Parczewski, M. (2022). Effectiveness of Tocilizumab in Patients with Severe or Critical Lung Involvement in COVID-19: A Retrospective Study. Journal of Clinical Medicine, 11(9), 2286. https://doi.org/10.3390/jcm11092286