
Parafibromin Is Highly Expressed in Hepatocellular Carcinoma and Its Expression Correlates with Poor Prognosis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Clinicopathologic Features and Tissue Microarray Construction
2.2. Immunohistochemical Staining
2.3. Statistical Analysis
3. Results
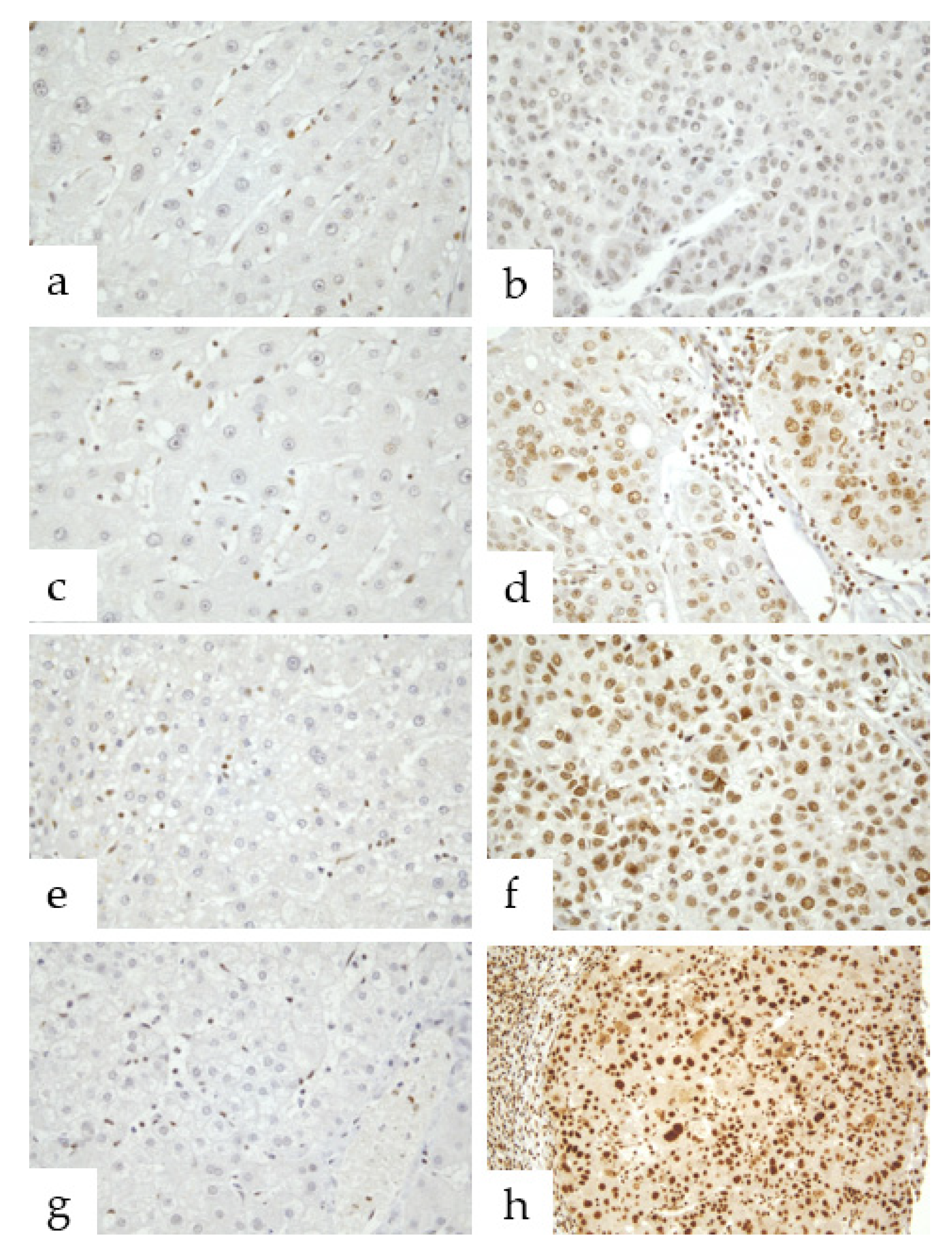
3.1. Parafibromin Expression Patterns
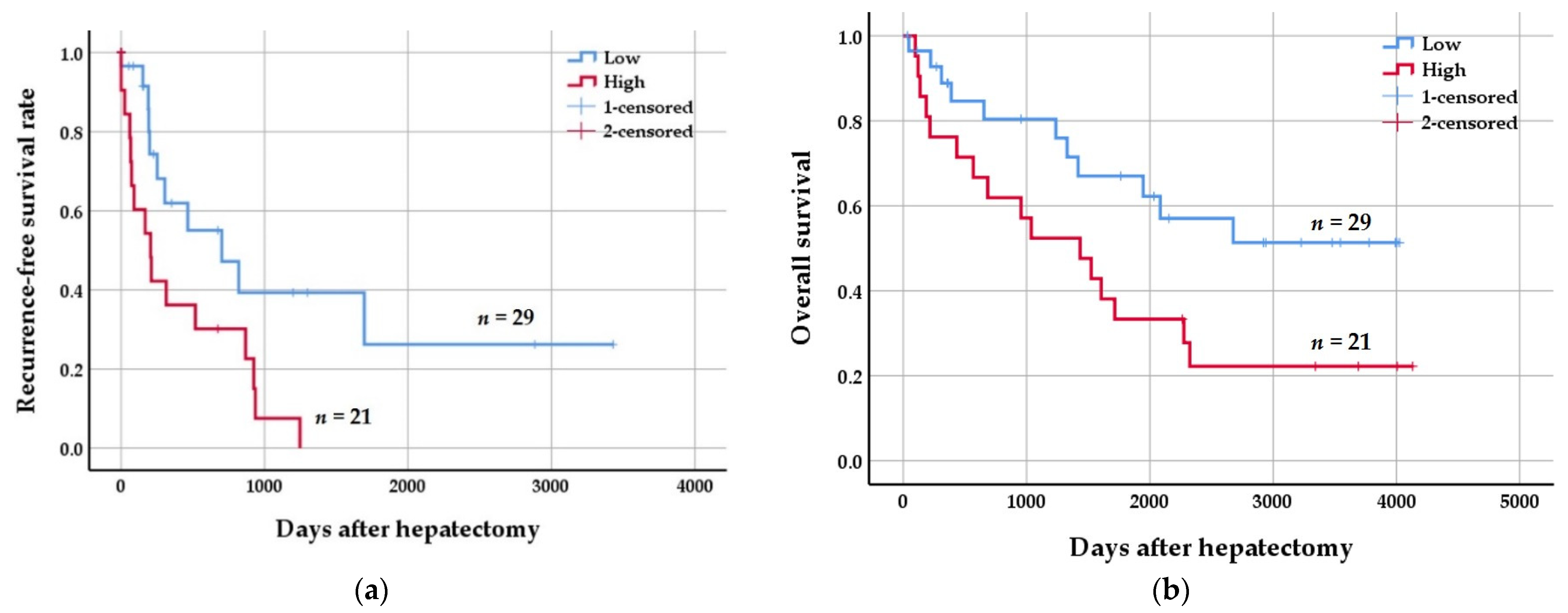
3.2. Clinicopathologic Significance of Parafibromin Expression
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Y.; Wang, X.; Yang, Y. Hepatic Hippo signaling inhibits development of hepatocellular carcinoma. Clin. Mol. Hepatol. 2020, 26, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Passi, M.; Zahler, S. Mechano-Signaling Aspects of Hepatocellular Carcinoma. J. Cancer 2021, 12, 6411–6421. [Google Scholar] [CrossRef] [PubMed]
- Borgia, M.; Dal Bo, M.; Toffoli, G. Role of Virus-Related Chronic Inflammation and Mechanisms of Cancer Immune-Suppression in Pathogenesis and Progression of Hepatocellular Carcinoma. Cancers 2021, 13, 4387. [Google Scholar] [CrossRef] [PubMed]
- Borzio, M.; Paladino, F.; Francica, G. Liver carcinogenesis: Diagnostic and clinical aspects of preneoplastic nodules. Hepatoma Res. 2019, 5, 15. [Google Scholar] [CrossRef] [Green Version]
- Vasuri, F.; Golfieri, R.; Fiorentino, M.; Capizzi, E.; Renzulli, M.; Pinna, A.D.; Grigioni, W.F.; D’Errico-Grigioni, A. OATP 1B1/1B3 expression in hepatocellular carcinomas treated with orthotopic liver transplantation. Virchows Arch. 2011, 459, 141–146. [Google Scholar] [CrossRef]
- Golfieri, R.; Garzillo, G.; Ascanio, S.; Renzulli, M. Focal Lesions in the Cirrhotic Liver: Their Pivotal Role in Gadoxetic Acid-Enhanced MRI and Recognition by the Western Guidelines. Dig. Dis. 2014, 32, 696–704. [Google Scholar] [CrossRef]
- Block, T.M.; Mehta, A.S.; Fimmel, C.J.; Jordan, R. Molecular viral oncology of hepatocellular carcinoma. Oncogene 2003, 22, 5093–5107. [Google Scholar] [CrossRef] [Green Version]
- Canavese, M.; Wijesundara, D.; Maddern, G.J.; Grubor-Bauk, B.; Hauben, E. Hepatitis C virus drives the pathogenesis of hepatocellular carcinoma: From immune evasion to carcinogenesis. Clin. Transl. Immunol. 2016, 5, e101. [Google Scholar] [CrossRef]
- Levrero, M. Viral hepatitis and liver cancer: The case of hepatitis C. Oncogene 2006, 25, 3834–3847. [Google Scholar] [CrossRef] [Green Version]
- Thorgeirsson, S.S.; Grisham, J.W. Molecular pathogenesis of human hepatocellular carcinoma. Nat. Genet. 2002, 31, 339–346. [Google Scholar] [CrossRef]
- Wang, W.; Pan, Q.; Fuhler, G.M.; Smits, R.; Peppelenbosch, M.P. Action and function of Wnt/beta-catenin signaling in the progression from chronic hepatitis C to hepatocellular carcinoma. J. Gastroenterol. 2017, 52, 419–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, A.; Tsutsumi, R.; Kikuchi, I.; Obuse, C.; Saito, Y.; Seidi, A.; Karisch, R.; Fernandez, M.; Cho, T.; Ohnishi, N.; et al. SHP2 tyrosine phosphatase converts parafibromin/Cdc73 from a tumor suppressor to an oncogenic driver. Mol. Cell 2011, 43, 45–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karaarslan, S.; Yurum, F.N.; Kumbaraci, B.S.; Pala, E.E.; Sivrikoz, O.N.; Akyildiz, M.; Bugdayci, M.H. The Role of Parafibromin, Galectin-3, HBME-1, and Ki-67 in the Differential Diagnosis of Parathyroid Tumors. Oman Med. J. 2015, 30, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Carpten, J.D.; Robbins, C.M.; Villablanca, A.; Forsberg, L.; Presciuttini, S.; Bailey-Wilson, J.; Simonds, W.F.; Gillanders, E.M.; Kennedy, A.M.; Chen, J.D.; et al. HRPT2, encoding parafibromin, is mutated in hyperparathyroidism-jaw tumor syndrome. Nat. Genet. 2002, 32, 676–680. [Google Scholar] [CrossRef]
- Rozenblatt-Rosen, O.; Hughes, C.M.; Nannepaga, S.J.; Shanmugam, K.S.; Copeland, T.D.; Guszczynski, T.; Resau, J.H.; Meyerson, M. The parafibromin tumor suppressor protein is part of a human Paf1 complex. Mol. Cell Biol. 2005, 25, 612–620. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Zhang, J.H.; Panicker, L.M.; Simonds, W.F. The parafibromin tumor suppressor protein inhibits cell proliferation by repression of the c-myc proto-oncogene. Proc. Natl. Acad. Sci. USA 2008, 105, 17420–17425. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Takano, Y.; Zheng, H.C. The pathobiological features of gastrointestinal cancers (Review). Oncol. Lett. 2012, 3, 961–969. [Google Scholar] [CrossRef]
- Marsh, D.J.; Ma, Y.; Dickson, K.A. Histone Monoubiquitination in Chromatin Remodelling: Focus on the Histone H2B Interactome and Cancer. Cancers 2020, 12, 3462. [Google Scholar] [CrossRef]
- Truran, P.P.; Johnson, S.J.; Bliss, R.D.; Lennard, T.W.; Aspinall, S.R. Parafibromin, galectin-3, PGP9.5, Ki67, and cyclin D1: Using an immunohistochemical panel to aid in the diagnosis of parathyroid cancer. World J. Surg. 2014, 38, 2845–2854. [Google Scholar] [CrossRef]
- Selvarajan, S.; Sii, L.H.; Lee, A.; Yip, G.; Bay, B.H.; Tan, M.H.; Teh, B.T.; Tan, P.H. Parafibromin expression in breast cancer: A novel marker for prognostication? J. Clin. Pathol. 2008, 61, 64–67. [Google Scholar] [CrossRef]
- Xia, P.; Wang, W.; Xu, X.Y.; Wang, J.P.; Takano, Y.; Zheng, H.C. Parafibromin expression in lung normal tissue and carcinoma: Its comparison with clinicopathological parameters of carcinoma. Histol. Histopathol. 2011, 26, 1039–1047. [Google Scholar] [PubMed]
- Zheng, H.C.; Takahashi, H.; Li, X.H.; Hara, T.; Masuda, S.; Guan, Y.F.; Takano, Y. Downregulated parafibromin expression is a promising marker for pathogenesis, invasion, metastasis and prognosis of gastric carcinomas. Virchows Arch. 2008, 452, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, H.C.; Wei, Z.L.; Xu, X.Y.; Nie, X.C.; Yang, X.; Takahashi, H.; Takano, Y. Parafibromin expression is an independent prognostic factor for colorectal carcinomas. Hum. Pathol. 2011, 42, 1089–1102. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Smits, R.; Hao, H.; He, C. Wnt/beta-Catenin Signaling in Liver Cancers. Cancers 2019, 11, 926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, D.; Cheng, Z.; Liu, H.; Wang, X.; Han, T.; Sun, W.; Li, X.; Yang, W.; Chen, C.; Xia, M.; et al. Shp2 promotes liver cancer stem cell expansion by augmenting beta-catenin signaling and predicts chemotherapeutic response of patients. Hepatology 2017, 65, 1566–1580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, C.; Takahashi-Kanemitsu, A.; Kikuchi, I.; Ben, C.; Hatakeyama, M. Transcriptional Co-activator Functions of YAP and TAZ Are Inversely Regulated by Tyrosine Phosphorylation Status of Parafibromin. iScience 2018, 2, 103. [Google Scholar] [CrossRef] [Green Version]
- Zheng, H.C.; Gong, B.C.; Zhao, S. The clinicopathological and prognostic significances of CDC73 expression in cancers: A bioinformatics analysis. Oncotarget 2017, 8, 95270–95279. [Google Scholar] [CrossRef]
- Yang, H.; Gu, J.; Zheng, Q.; Li, M.; Lian, X.; Miao, J.; Jiang, J.; Wei, W. RPB5-mediating protein is required for the proliferation of hepatocellular carcinoma cells. J. Biol. Chem. 2011, 286, 11865–11874. [Google Scholar] [CrossRef] [Green Version]
- Porzionato, A.; Macchi, V.; Barzon, L.; Masi, G.; Iacobone, M.; Parenti, A.; Palu, G.; De Caro, R. Immunohistochemical assessment of parafibromin in mouse and human tissues. J. Anat. 2006, 209, 817–827. [Google Scholar] [CrossRef]
- Zhu, J.J.; Cui, Y.; Cui, K.; Li, X.; Zhang, Z.Y. Distinct roles of parafibromin in the extracellular environment, cytoplasm and nucleus of osteosarcoma cells. Am. J. Transl. Res. 2016, 8, 2426–2431. [Google Scholar]
- Kim, H.; Choi, G.H.; Na, D.C.; Ahn, E.Y.; Kim, G.I.; Lee, J.E.; Cho, J.Y.; Yoo, J.E.; Choi, J.S.; Park, Y.N. Human hepatocellular carcinomas with “Stemness”-related marker expression: Keratin 19 expression and a poor prognosis. Hepatology 2011, 54, 1707–1717. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Komuta, M.; Yasui, Y.; Tamaki, N.; Hosokawa, T.; Ueda, K.; Kuzuya, T.; Itakura, J.; Nakanishi, H.; Takahashi, Y.; et al. Expression of keratin 19 is related to high recurrence of hepatocellular carcinoma after radiofrequency ablation. Oncology 2011, 80, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Rhee, H.; Nahm, J.H.; Kim, H.; Choi, G.H.; Yoo, J.E.; Lee, H.S.; Koh, M.J.; Park, Y.N. Poor outcome of hepatocellular carcinoma with stemness marker under hypoxia: Resistance to transarterial chemoembolization. Mod. Pathol. 2016, 29, 1038–1049. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinicopathologic Parameters | Parafibromin Expression | p Value | |||
|---|---|---|---|---|---|
| + | ++ | +++ | ++++ | ||
| (n = 8) | (n = 21) | (n = 14) | (n = 7) | ||
| Age (mean ± SD 2), years | 53.8 ± 10.0 | 57.9 ± 6.9 | 49.6 ± 12.5 | 58.0 ± 10.0 | 0.152 |
| Gender | 0.467 | ||||
| Male | 8 | 17 | 12 | 5 | |
| Female | 0 | 4 | 2 | 2 | |
| Tumor size | 0.978 | ||||
| ≤3 cm | 2 | 5 | 5 | 1 | |
| >3 cm | 6 | 16 | 9 | 6 | |
| Tumor multiplicity | 0.070 | ||||
| Unifocal | 7 | 15 | 7 | 7 | |
| Multifocal | 1 | 6 | 7 | 0 | |
| Microvessel invasion | 0.017 * | ||||
| Absent | 7 | 12 | 6 | 2 | |
| Present | 1 | 9 | 8 | 5 | |
| Portal vein invasion | 0.076 | ||||
| Absent | 8 | 18 | 10 | 5 | |
| Present | 0 | 3 | 4 | 2 | |
| Cirrhosis | 0.393 | ||||
| Absent | 5 | 7 | 6 | 2 | |
| Present | 3 | 14 | 8 | 5 | |
| Hepatitis virus | 0.005 * | ||||
| Absent | 3 | 0 | 0 | 0 | |
| Present | 5 | 21 | 14 | 7 | |
| Edmondson–Steiner grade | 0.000 * | ||||
| I | 1 | 2 | 0 | 0 | |
| II | 6 | 6 | 2 | 1 | |
| III | 1 | 13 | 11 | 4 | |
| IV | 0 | 0 | 1 | 2 | |
| Recurrence | 0.977 | ||||
| Absent | 3 | 15 | 8 | 3 | |
| Present | 5 | 6 | 6 | 4 | |
| Metastasis | 0.562 | ||||
| Absent | 4 | 15 | 8 | 3 | |
| Present | 4 | 6 | 6 | 4 | |
| 5-year survival | 0.005 * | ||||
| Alive | 5 | 9 | 5 | 2 | |
| Dead | 2 | 6 | 9 | 5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.-K. Parafibromin Is Highly Expressed in Hepatocellular Carcinoma and Its Expression Correlates with Poor Prognosis. J. Clin. Med. 2022, 11, 1773. https://doi.org/10.3390/jcm11071773
Kim M-K. Parafibromin Is Highly Expressed in Hepatocellular Carcinoma and Its Expression Correlates with Poor Prognosis. Journal of Clinical Medicine. 2022; 11(7):1773. https://doi.org/10.3390/jcm11071773
Chicago/Turabian StyleKim, Min-Kyung. 2022. "Parafibromin Is Highly Expressed in Hepatocellular Carcinoma and Its Expression Correlates with Poor Prognosis" Journal of Clinical Medicine 11, no. 7: 1773. https://doi.org/10.3390/jcm11071773
APA StyleKim, M.-K. (2022). Parafibromin Is Highly Expressed in Hepatocellular Carcinoma and Its Expression Correlates with Poor Prognosis. Journal of Clinical Medicine, 11(7), 1773. https://doi.org/10.3390/jcm11071773