
Response Assessment to Erythropoietin-Zeta (Epo-Alpha Biosimilar) Therapy in Low-Risk Myelodysplastic Syndromes

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Design and Method
2.1. Study Design
2.2. Patients
2.3. Treatment Flow
2.4. Response Evaluation
2.5. Statistical Analysis
2.6. Primary Endpoint
2.7. Sample Size
2.8. Secondary Endpoint
3. Results
3.1. Patient Characteristics
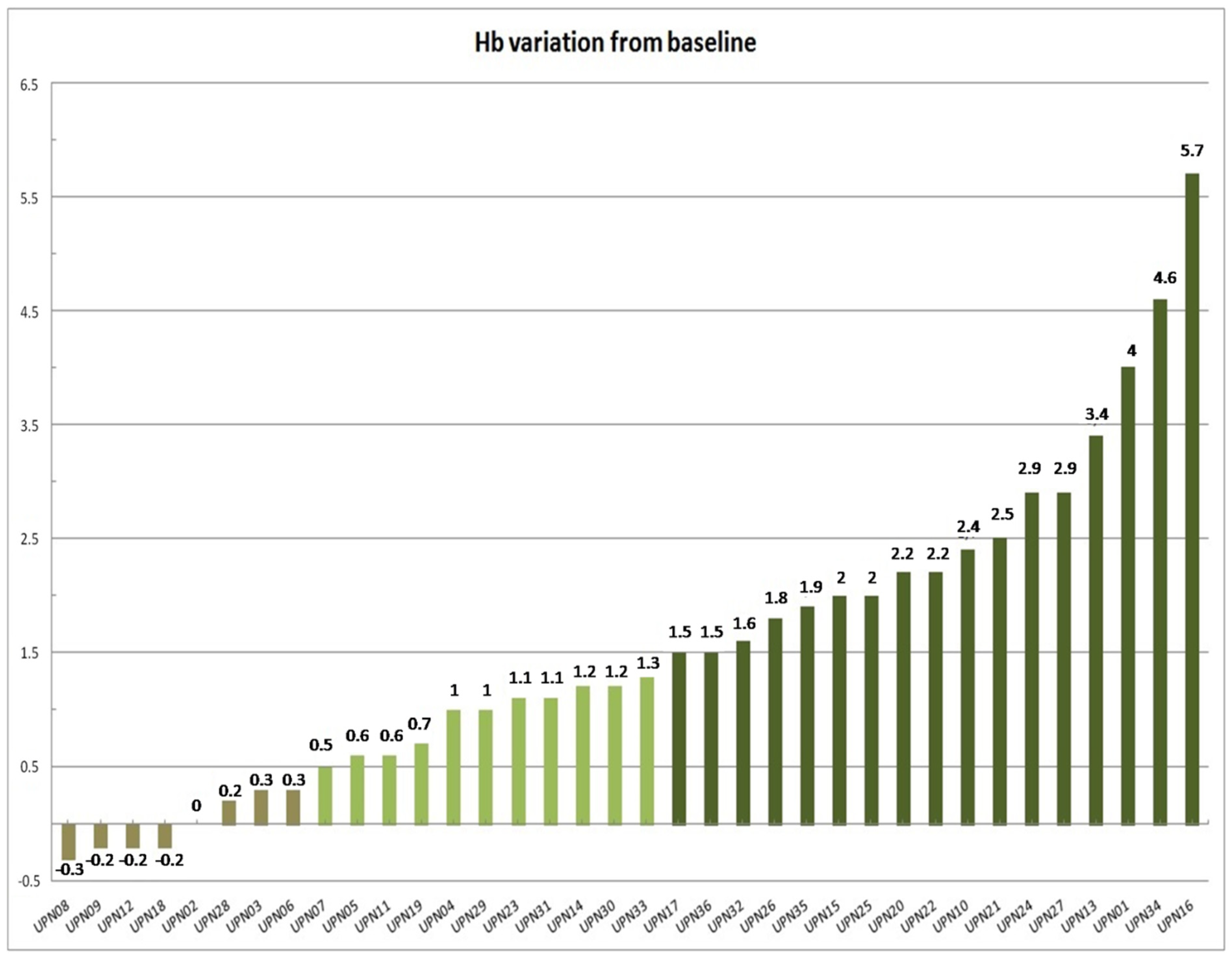
3.2. Erythroid Response
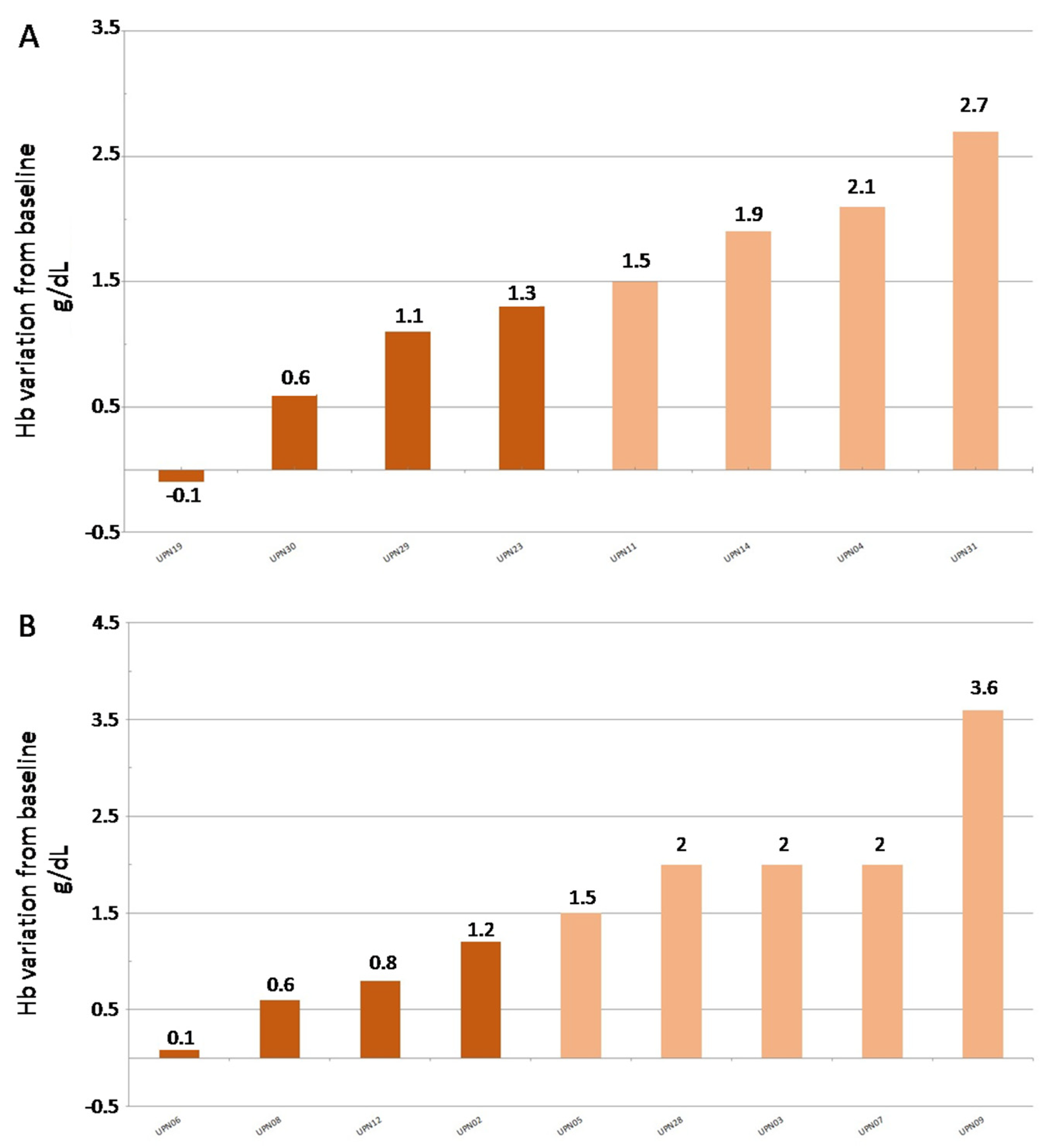
3.3. Erythroid Response at Week 24
3.4. Safety
3.5. Long Term Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Vardiman, J.W. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; International Agency for Research on Cancer: Lyon, France, 2008; ISBN 9789283224310. [Google Scholar]
- Oliva, E.N.; Finelli, C.; Santini, V.; Poloni, A.; Liso, V.; Cilloni, D.; Impera, S.; Terenzi, A.; Levis, A.; Cortelezzi, A.; et al. Quality of life and physicians’ perception in myelodysplastic syndromes. Am. J. Blood Res. 2012, 2, 136–147. [Google Scholar] [PubMed]
- Oliva, E.N.; Dimitrov, B.D.; Benedetto, F.; D’Angelo, A.; Nobile, F. Hemoglobin level threshold for cardiac remodeling and quality of life in myelodysplastic syndrome. Leuk. Res. 2005, 29, 1217–1219. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Santini, V.; Spiriti, M.A.A.; Giagounidis, A.; Schlag, R.; Radinoff, A.; Gercheva-Kyuchukova, L.; Anagnostopoulos, A.; Oliva, E.N.; Symeonidis, A.; et al. A phase 3 randomized, placebo-controlled study assessing the efficacy and safety of epoetin-α in anemic patients with low-risk MDS. Leukemia 2018, 32, 2648–2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platzbecker, U.; Symeonidis, A.; Oliva, E.N.; Goede, J.S.; Delforge, M.; Mayer, J.; Slama, B.; Badre, S.; Gasal, E.; Mehta, B.; et al. A phase 3 randomized placebo-controlled trial of darbepoetin alfa in patients with anemia and lower-risk myelodysplastic syndromes. Leukemia 2017, 31, 1944–1950. [Google Scholar] [CrossRef] [Green Version]
- Santini, V. Clinical Use of Erythropoietic Stimulating Agents in Myelodysplastic Syndromes. Oncologist 2011, 16, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Alessandrino, E.P.; Amadori, S.; Barosi, G.; Cazzola, M.; Grossi, A.; Liberato, L.N.; Locatelli, F.; Marchetti, M.; Morra, E.; Rebulla, P.; et al. Evidence- and consensus-based practice guidelines for the therapy of primary myelodysplastic syndromes. A statement from the italian society of hematology. Haematologica 2002, 87, 1286–1306. [Google Scholar] [PubMed]
- Moyo, V.; Lefebvre, P.; Duh, M.S.; Yektashenas, B.; Mundle, S. Erythropoiesis-stimulating agents in the treatment of anemia in myelodysplastic syndromes: A meta-analysis. Ann. Hematol. 2008, 87, 527–536. [Google Scholar] [CrossRef]
- Di Raimondo, F.; Longo, G.; Cacciola, E.; Milone, G.; Palumbo, G.A.; Cacciola, R.R.; Alessi, M.; Giustolisi, R. A good response rate to recombinant erythropoietin alone may be expected in selected myelodysplastic patients. A preliminary clinical study. Eur. J. Haematol. 1996, 56, 7–11. [Google Scholar] [CrossRef]
- Oliva, E.N.; Schey, C.; Hutchings, A.S. A review of anemia as a cardiovascular risk factor in patients with myelodysplastic syndromes. Am. J. Blood Res. 2011, 1, 160–166. [Google Scholar]
- Cannella, L.; Caocci, G.; Jacobs, M.; Vignetti, M.; Mandelli, F.; Efficace, F. Health-related quality of life and symptom assessment in randomized controlled trials of patients with leukemia and myelodysplastic syndromes: What have we learned? Crit. Rev. Oncol. Hematol. 2015, 96, 542–554. [Google Scholar] [CrossRef]
- Pereira, A.A.; Sarnak, M.J. Anemia as a risk factor for cardiovascular disease. Kidney Int. Suppl. 2003, 64, S32–S39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liumbruno, G.; Bennardello, F.; Lattanzio, A.; Piccoli, P.; Rossetti, G. Recommendations for the transfusion of red blood cells. Blood Transfus. 2009, 7, 49–64. [Google Scholar] [PubMed]
- Ludwig, H.; Fritz, E.; Kotzmann, H.; Höcker, P.; Gisslinger, H.; Barnas, U. Erythropoietin Treatment of Anemia Associated with Multiple Myeloma. N. Engl. J. Med. 1990, 322, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Osterborg, A. The role of recombinant human erythropoietin in the management of anaemic cancer patients: Focus on haematological malignancies. Med. Oncol. 2000, 17, S17–S22. [Google Scholar]
- Pullarkat, V. Objectives of iron chelation therapy in myelodysplastic syndromes: More than meets the eye? Blood 2009, 114, 5251–5255. [Google Scholar] [CrossRef] [Green Version]
- Malcovati, L.; Porta, M.G.D.; Pascutto, C.; Invernizzi, R.; Boni, M.; Travaglino, E.; Passamonti, F.; Arcaini, L.; Maffioli, M.; Bernasconi, P.; et al. Prognostic Factors and Life Expectancy in Myelodysplastic Syndromes Classified According to WHO Criteria: A Basis for Clinical Decision Making. J. Clin. Oncol. 2005, 23, 7594–7603. [Google Scholar] [CrossRef] [PubMed]
- Barosi, G.; Bosi, A.; Abbracchio, M.P.; Danesi, R.; Genazzani, A.; Corradini, P.; Pane, F.; Tura, S. Key concepts and critical issues on epoetin and filgrastim biosimilars: A position paper from the Italian Society of Hematology, Italian Society of Ex-perimental Hematology, and Italian Group for Bone Marrow Transplantation. Haematologica 2011, 96, 937–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schellekens, H. Biosimilar therapeutics—What do we need to consider? NDT Plus 2009, 2, i27–i36. [Google Scholar] [CrossRef] [PubMed]
- Weigang-Köhler, K.; Vetter, A.; Thyroff-Friesinger, U. HX575, Recombinant Human Epoetin Alfa, for the Treatment of Chemotherapy-Associated Symptomatic Anaemia in Patients with Solid Tumours. Oncol. Res. Treat. 2009, 32, 168–174. [Google Scholar] [CrossRef]
- Greenberg, P.; Cox, C.; Lebeau, M.M.; Fenaux, P.; Morel, P.; Sanz, G.; Sanz, M.; Vallespi, T.; Hamblin, T.; Oscier, D.; et al. International Scoring System for Evaluating Prognosis in Myelodysplastic Syndromes. Blood 1997, 89, 2079–2088. [Google Scholar] [CrossRef]
- Park, S.; Kelaidi, C.; Meunier, M.; Casadevall, N.; Gerds, A.T.; Platzbecker, U. The prognostic value of serum erythropoietin in patients with lower-risk myelodysplastic syndromes: A review of the literature and expert opinion. Ann. Hematol. 2020, 99, 7–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowen, D.; Culligan, D.; Jowitt, S.; Kelsey, S.; Mufti, G.; Oscier, D.; Parker, J.; UK MDS Guidelines Group. Guidelines for the diagnosis and therapy of adult myelodysplastic syndromes. Br. J. Haematol. 2003, 120, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Schellekens, H. Assessing the bioequivalence of biosimilars: The Retacrit® case. Drug Discov. Today 2009, 14, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Greenberg, P.L.; Bennett, J.M.; Lowenberg, B.; Wijermans, P.W.; Nimer, S.D.; Pinto, A.; Beran, M.; De Witte, T.M.; Stone, R.M.; et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006, 108, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundle, S.; Lefebvre, P.; Vekeman, F.; Duh, M.S.; Rastogi, R.; Moyo, V. An assessment of erythroid response to epoetin α as a single agent versus in combination with granulocyte- or granulocyte-macrophage-colony-stimulating factor in myelodys-plastic syndromes using a meta-analysis approach. Cancer 2009, 115, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Musto, P.; Falcone, A.; Sanpaolo, G.; Bodenizza, C.; La Sala, A.; Perla, G.; Carella, A.M. Efficacy of a single, weekly dose of recombinant erythropoietin in myelodysplastic syndromes. Br. J. Haematol. 2003, 122, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Stasi, R.; Brunetti, M.; Terzoli, E.; Abruzzese, E.; Amadori, S. Once-weekly dosing of recombinant human erythropoietin alpha in patients with myelodysplastic syndromes unresponsive to conventional dosing. Ann. Oncol. 2004, 15, 1684–1690. [Google Scholar] [CrossRef]
- Ross, S.D.; Allen, I.E.; Probst, C.A.; Sercus, B.; Crean, S.M.; Ranganathan, G. Efficacy and Safety of Erythropoiesis-Stimulating Proteins in Myelodysplastic Syndrome: A Systematic Review and Meta-Analysis. Oncologist 2007, 12, 1264–1273. [Google Scholar] [CrossRef] [Green Version]
- Brinks, V.; Hawe, A.; Basmeleh, A.H.H.; Joachin-Rodriguez, L.; Haselberg, R.; Somsen, G.W.; Jiskoot, W.; Schellekens, H. Quality of Original and Biosimilar Epoetin Products. Pharm. Res. 2010, 28, 386–393. [Google Scholar] [CrossRef] [Green Version]
- Mellstedt, H.; Niederwieser, D.; Ludwig, H. The challenge of biosimilars. Ann. Oncol. 2008, 19, 411–419. [Google Scholar] [CrossRef]
- Park, S.; Grabar, S.; Kelaidi, C.; Beyne-Rauzy, O.; Picard, F.; Bardet, V.; Coiteux, V.; Leroux, G.; Lepelley, P.; Daniel, M.-T.; et al. Predictive factors of response and survival in myelodysplastic syndrome treated with erythropoietin and G-CSF: The GFM experience. Blood 2008, 111, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Mougiou, A.; Kouraklis, A.; Chatzivassili, A.; Michalis, E.; Giannakoulas, N.; Manioudaki, E.; Lazaridou, A.; Bakaloudi, V.; Protopappa, M.; et al. Prolonged administration of erythropoietin increases erythroid response rate in myelodysplastic syndromes: A phase II trial in 281 patients. Br. J. Haematol. 2002, 118, 174–180. [Google Scholar] [CrossRef]
- Balleari, E.; Filiberti, R.A.; Salvetti, C.; Allione, B.; Angelucci, E.; Bruzzone, M.; Calzamiglia, T.; Cavaliere, M.; Cavalleri, M.; Cilloni, D.; et al. Effects of different doses of erythropoietin in patients with myelodysplastic syndromes: A propensity score-matched analysis. Cancer Med. 2019, 8, 7567–7576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golshayan, A.-R.; Jin, T.; Maciejewski, J.; Fu, A.Z.; Bershadsky, B.; Kattan, M.W.; Kalaycio, M.E.; Sekeres, M.A. Efficacy of growth factors compared to other therapies for low-risk myelodysplastic syndromes. Br. J. Haematol. 2007, 137, 125–132. [Google Scholar] [CrossRef]
- Jädersten, M.; Malcovati, L.; Dybedal, I.; Della Porta, M.G.; Invernizzi, R.; Montgomery, S.M.; Pascutto, C.; Porwit, A.; Cazzola, M.; Hellström-Lindberg, E. Erythropoietin and Granulocyte-Colony Stimulating Factor Treatment Associated With Improved Survival in Myelodysplastic Syndrome. J. Clin. Oncol. 2008, 26, 3607–3613. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.L.; Sun, Z.; Miller, K.B.; Bennett, J.M.; Tallman, M.S.; Dewald, G.; Paietta, E.; van der Jagt, R.; Houston, J.; Thomas, M.L.; et al. Treatment of myelodysplastic syndrome patients with erythropoietin with or without granulocyte colony-stimulating factor: Results of a prospective randomized phase 3 trial by the Eastern Cooperative Oncology Group (E1996). Blood 2009, 114, 2393–2400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buccisano, F.; Piccioni, A.L.; Nobile, C.; Criscuolo, M.; Niscola, P.; Tatarelli, C.; Fianchi, L.; Villivà, N.; Neri, B.; Carmosino, I.; et al. Real-life use of erythropoiesis-stimulating agents in myelodysplastic syndromes: A “Gruppo Romano Mielodisplasie (GROM)” multicenter study. Ann. Hematol. 2016, 95, 1059–1065. [Google Scholar] [CrossRef]
- Tatarelli, C.; Piccioni, A.L.; Maurillo, L.; Naso, V.; Battistini, R.; D’Andrea, M.; Criscuolo, M.; Nobile, C.; Villivà, N.; Mancini, S.; et al. Recombinant human erythropoietin in very elderly patients with myelodysplastic syndromes: Results from a retrospective study. Ann. Hematol. 2014, 93, 1413–1420. [Google Scholar] [CrossRef]
- Barzi, A.; Sekeres, M.A. Myelodysplastic syndromes: A practical approach to diagnosis and treatment. Clevel. Clin. J. Med. 2010, 77, 37–44. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Gender | MDS Subtype | BM Blasts | BM Fibrosis | Perypheral Cytopenias | Karyotype | Full Karyotype | IPSS Score | Risk Category |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | RCMD | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| 2 | F | RCMD | <5% | ABSENT | 2/3 | GOOD | 46, XX [20] | 0.5 | Int-1 |
| 3 | F | RCMD | <5% | NOT EVALUATED | 2/3 | GOOD | 46, XX [20] | 0.5 | Int-1 |
| 4 | F | RA | <5% | ABSENT | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 5 | F | RCMD | <5% | ABSENT | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 6 | F | RCMD | <5% | ABSENT | 2/3 | GOOD | 46, XX [20] | 0.5 | Int-1 |
| 7 | F | RCMD | <5% | ABSENT | 2/3 | GOOD | 46, XX [20] | 0.5 | Int-1 |
| 8 | M | RAEB-2 | 5–10% | ABSENT | 0/1 | GOOD | 46, XY [20] | 0.5 | Int-1 |
| 9 | M | RA | <5% | ABSENT | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| 10 | M | RA | <5% | ABSENT | 2/3 | GOOD | 46, XY [20] | 0.5 | Int-1 |
| 11 | M | MDS-U | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| 12 | F | RA | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 13 | F | RCMD | <5% | ABSENT | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 14 | M | RA | <5% | ABSENT | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| 15 | M | MDS-U | <5% | MF-1 | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| 16 | M | MDS-U | <5% | MF-1 | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| 17 | M | RAEB-1 | 5–10% | ABSENT | 0/1 | INTERMEDIATE | 47, XY, +8 [20] | Int-1 | |
| 18 | M | RA | <5% | NOT EVALUATED | 2/3 | GOOD | 46, XY [20] | 0.5 | Int-1 |
| 19 | M | RA | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XY [20] | Low | |
| 20 | M | RCMD | <5% | ABSENT | 2/3 | GOOD | 46, XY [20] | 0.5 | Int-1 |
| 21 | F | RA | <5% | NOT EVALUATED | 0/1 | INTERMEDIATE | 46, XX [20] | 0.5 | Int-1 |
| 22 | M | RCMD-RS | <5% | NOT EVALUATED | 2/3 | GOOD | 46, XY [20] | 0.5 | Int-1 |
| 23 | F | RA | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 24 | F | RCMD | <5% | ABSENT | 0/1 | GOOD | 46, XX [20] | 0 | Int-1 |
| 25 | F | RCMD | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 26 | M | RA | 5–10% | NOT EVALUATED | 2/3 | GOOD | 46, XY [20] | 1 | Int-1 |
| 27 | M | RA | <5% | ABSENT | 2/3 | GOOD | 46, XY [20] | 0.5 | Int-1 |
| 28 | M | RCMD | <5% | ABSENT | 0/1 | INTERMEDIATE | 47, XY, +8 [20] | 0.5 | Int-1 |
| 29 | F | RCMD-RS | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 30 | M | RCMD | <5% | MF-1 | 0/1 | INTERMEDIATE | 46, XY [20] | 0.5 | Int-1 |
| 31 | F | RA | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 32 | M | RA | <5% | NOT EVALUATED | 0/1 | INTERMEDIATE | 46, XY [20] | 1 | Int-1 |
| 33 | F | RCMD | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 1 | Low |
| 34 | F | MDS-U | <5% | ABSENT | 0/1 | GOOD | 46, XX [20] | 0 | Low |
| 35 | F | RA | <5% | NOT EVALUATED | 0/1 | GOOD | 46, XX [20] | 1 | Low |
| 36 | M | RCMD | <5% | ABSENT | 0/1 | GOOD | 46, XY [20] | 0 | Low |
| Age | RR | 0.65 |
| CI lower | 0.28 | |
| CI Upper | 1.53 | |
| ECOG | RR | 0.36 |
| CI lower | 0.06 | |
| CI Upper | 2.17 | |
| Number of Cytopenias | RR | 0.57 |
| CI lower | 0.13 | |
| CI Upper | 2.54 | |
| % Blasts | RR | 0.47 |
| CI lower | 0.039 | |
| CI Upper | 5.7 | |
| BM Fibrosis | RR | 0.38 |
| CI lower | 0.029 | |
| CI Upper | 5.2 | |
| IPSS | RR | 0.5 |
| CI lower | 1.13 | |
| CI Upper | 1.92 | |
| Histology | RR | 1 |
| CI lower | 0.262 | |
| CI Upper | 3.82 |
| Adverse Event | Grading | ||||
|---|---|---|---|---|---|
| I | II | III | IV | V | |
| Infection | 1 (3%) | 1 (3%) | |||
| Metabolic | 1 (3%) | ||||
| Vascular | 1 (3%) | 3 (9%) | |||
| Liver | 1 (3%) | ||||
| Constitutional symptoms | 1 (3%) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vetro, C.; Di Giacomo, V.; Mannina, D.; Magrin, S.; Mulè, A.; Mitra, M.E.; Siragusa, S.; Duminuco, A.; Garibaldi, B.; Vadalà, M.C.E.; et al. Response Assessment to Erythropoietin-Zeta (Epo-Alpha Biosimilar) Therapy in Low-Risk Myelodysplastic Syndromes. J. Clin. Med. 2022, 11, 1665. https://doi.org/10.3390/jcm11061665
Vetro C, Di Giacomo V, Mannina D, Magrin S, Mulè A, Mitra ME, Siragusa S, Duminuco A, Garibaldi B, Vadalà MCE, et al. Response Assessment to Erythropoietin-Zeta (Epo-Alpha Biosimilar) Therapy in Low-Risk Myelodysplastic Syndromes. Journal of Clinical Medicine. 2022; 11(6):1665. https://doi.org/10.3390/jcm11061665
Chicago/Turabian StyleVetro, Calogero, Valeria Di Giacomo, Donato Mannina, Silvana Magrin, Antonio Mulè, Maria Enza Mitra, Sergio Siragusa, Andrea Duminuco, Bruno Garibaldi, Maria Cristina Emanuela Vadalà, and et al. 2022. "Response Assessment to Erythropoietin-Zeta (Epo-Alpha Biosimilar) Therapy in Low-Risk Myelodysplastic Syndromes" Journal of Clinical Medicine 11, no. 6: 1665. https://doi.org/10.3390/jcm11061665
APA StyleVetro, C., Di Giacomo, V., Mannina, D., Magrin, S., Mulè, A., Mitra, M. E., Siragusa, S., Duminuco, A., Garibaldi, B., Vadalà, M. C. E., Di Raimondo, F., & Palumbo, G. A. (2022). Response Assessment to Erythropoietin-Zeta (Epo-Alpha Biosimilar) Therapy in Low-Risk Myelodysplastic Syndromes. Journal of Clinical Medicine, 11(6), 1665. https://doi.org/10.3390/jcm11061665