
Triple-Negative Apocrine Breast Carcinoma Has Better Prognosis despite Poor Response to Neoadjuvant Chemotherapy

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Study Population
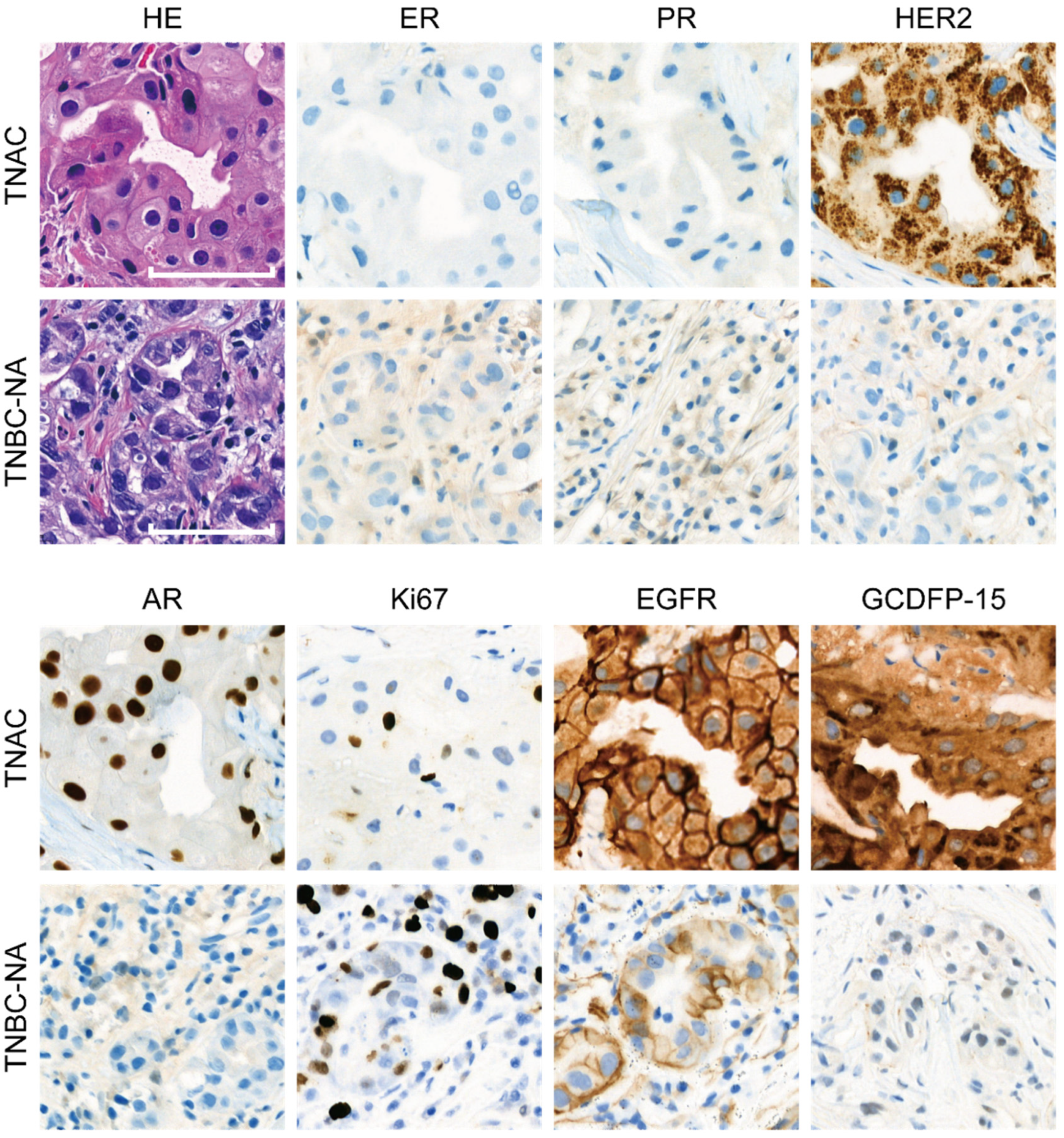
2.2. Immunohistochemical Staining
2.3. SEER Analysis
3. Results
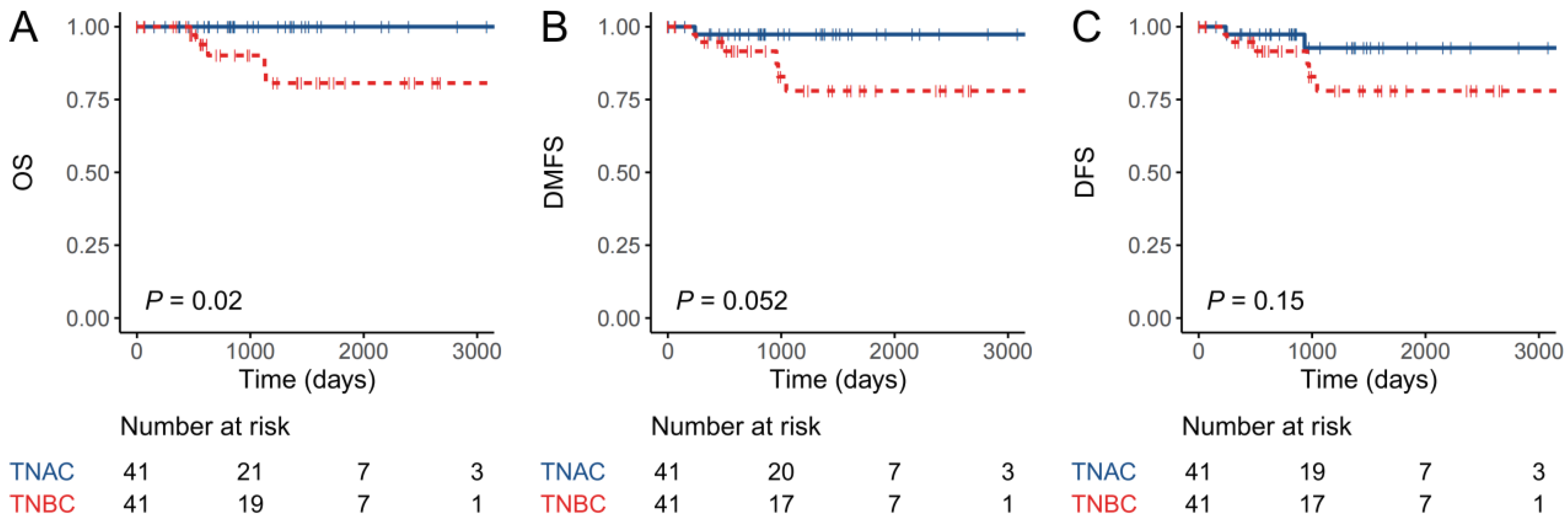
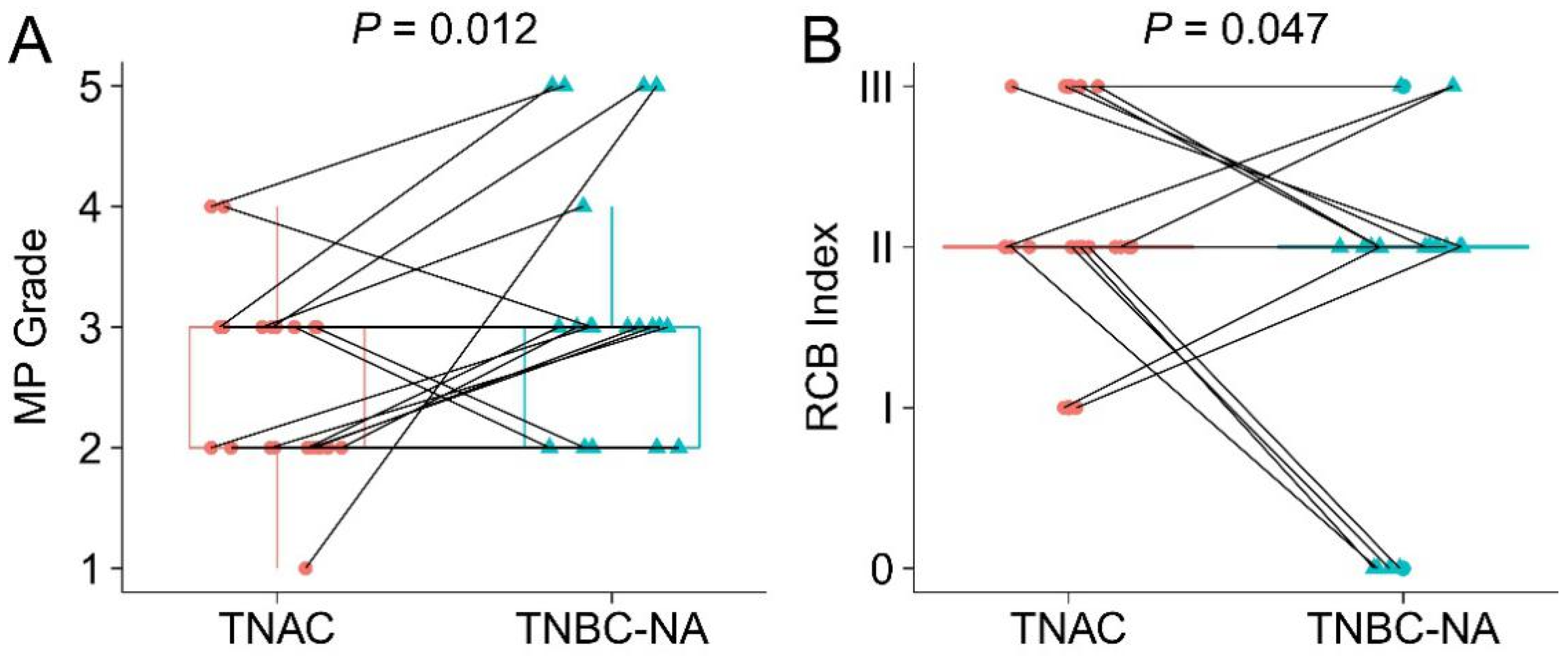
3.1. Patients with TNAC Have Better Short-Term Prognosis Than Those with TNBC-NA Despite a Poorer Response to Neoadjuvant Chemotherapy
3.2. Chemotherapy did Not Improve Breast-Cancer-Specific Survival for TNAC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dellapasqua, S.; Maisonneuve, P.; Viale, G.; Pruneri, G.; Mazzarol, G.; Ghisini, R.; Mazza, M.; Iorfida, M.; Rotmensz, N.; Veronesi, P.; et al. Immunohistochemically defined subtypes and outcome of apocrine breast cancer. Clin. Breast Cancer 2013, 13, 95–102. [Google Scholar] [CrossRef]
- Vranic, S.; Marchio, C.; Castellano, I.; Botta, C.; Scalzo, M.S.; Bender, R.P.; Payan-Gomez, C.; di Cantogno, L.V.; Gugliotta, P.; Tondat, F.; et al. Immunohistochemical and molecular profiling of histologically defined apocrine carcinomas of the breast. Hum. Pathol. 2015, 46, 1350–1359. [Google Scholar] [CrossRef]
- Astvatsaturyan, K.; Yue, Y.; Walts, A.E.; Bose, S. Androgen receptor positive triple negative breast cancer: Clinicopathologic, prognostic, and predictive features. PLoS ONE 2018, 13, e0197827. [Google Scholar] [CrossRef] [PubMed]
- Niemeier, L.A.; Dabbs, D.J.; Beriwal, S.; Striebel, J.M.; Bhargava, R. Androgen receptor in breast cancer: Expression in estrogen receptor-positive tumors and in estrogen receptor-negative tumors with apocrine differentiation. Mod. Pathol. 2010, 23, 205–212. [Google Scholar] [CrossRef]
- Vera-Badillo, F.E.; Templeton, A.J.; de Gouveia, P.; Diaz-Padilla, I.; Bedard, P.L.; Al-Mubarak, M.; Seruga, B.; Tannock, I.F.; Ocana, A.; Amir, E. Androgen receptor expression and outcomes in early breast cancer: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, djt319. [Google Scholar] [CrossRef]
- Bozovic-Spasojevic, I.; Zardavas, D.; Brohee, S.; Ameye, L.; Fumagalli, D.; Ades, F.; de Azambuja, E.; Bareche, Y.; Piccart, M.; Paesmans, M.; et al. The Prognostic Role of Androgen Receptor in Patients with Early-Stage Breast Cancer: A Meta-analysis of Clinical and Gene Expression Data. Clin. Cancer Res. 2017, 23, 2702–2712. [Google Scholar] [CrossRef]
- Burstein, M.D.; Tsimelzon, A.; Poage, G.M.; Covington, K.R.; Contreras, A.; Fuqua, S.A.; Savage, M.I.; Osborne, C.K.; Hilsenbeck, S.G.; Chang, J.C.; et al. Comprehensive genomic analysis identifies novel subtypes and targets of triple-negative breast cancer. Clin. Cancer Res. 2015, 21, 1688–1698. [Google Scholar] [CrossRef]
- Jiang, Y.Z.; Ma, D.; Suo, C.; Shi, J.; Xue, M.; Hu, X.; Xiao, Y.; Yu, K.D.; Liu, Y.R.; Yu, Y.; et al. Genomic and Transcriptomic Landscape of Triple-Negative Breast Cancers: Subtypes and Treatment Strategies. Cancer Cell 2019, 35, 428–440.e425. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.D.; Jovanovic, B.; Chen, X.; Estrada, M.V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS ONE 2016, 11, e0157368. [Google Scholar] [CrossRef] [PubMed]
- Masuda, H.; Baggerly, K.A.; Wang, Y.; Zhang, Y.; Gonzalez-Angulo, A.M.; Meric-Bernstam, F.; Valero, V.; Lehmann, B.D.; Pietenpol, J.A.; Hortobagyi, G.N.; et al. Differential response to neoadjuvant chemotherapy among 7 triple-negative breast cancer molecular subtypes. Clin. Cancer Res. 2013, 19, 5533–5540. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Moon, B.I.; Lim, W.; Park, S.; Cho, M.S.; Sung, S.H. Feasibility of Classification of Triple Negative Breast Cancer by Immunohistochemical Surrogate Markers. Clin. Breast Cancer 2018, 18, e1123–e1132. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Wu, M.; Peng, G.; Shi, D.; Zhang, J. Prognosis in triple-negative apocrine carcinomas of the breast: A population-based study. Cancer Med. 2019, 8, 7523–7531. [Google Scholar] [CrossRef] [PubMed]
- Arciero, C.A.; Diehl, A.H., 3rd; Liu, Y.; Sun, Q.; Gillespie, T.; Li, X.; Subhedar, P. Triple-negative apocrine carcinoma: A rare pathologic subtype with a better prognosis than other triple-negative breast cancers. J. Surg. Oncol. 2020, 122, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, D.R.; Bernales, S.; Jacobsen, B.M.; Cittelly, D.M.; Howe, E.N.; D’Amato, N.C.; Spoelstra, N.S.; Edgerton, S.M.; Jean, A.; Guerrero, J.; et al. Role of the androgen receptor in breast cancer and preclinical analysis of enzalutamide. Breast Cancer Res. 2014, 16, R7. [Google Scholar] [CrossRef] [PubMed]
- Montagna, E.; Cancello, G.; Pagan, E.; Bagnardi, V.; Munzone, E.; Dellapasqua, S.; Viale, G.; Mazzarol, G.; Veronesi, P.; Galimberti, V.; et al. Prognosis of selected triple negative apocrine breast cancer patients who did not receive adjuvant chemotherapy. Breast 2020, 53, 138–142. [Google Scholar] [CrossRef]
- Nagao, T.; Kinoshita, T.; Hojo, T.; Tsuda, H.; Tamura, K.; Fujiwara, Y. The differences in the histological types of breast cancer and the response to neoadjuvant chemotherapy: The relationship between the outcome and the clinicopathological characteristics. Breast 2012, 21, 289–295. [Google Scholar] [CrossRef]
- Dowsett, M.; Nielsen, T.O.; A’Hern, R.; Bartlett, J.; Coombes, R.C.; Cuzick, J.; Ellis, M.; Henry, N.L.; Hugh, J.C.; Lively, T.; et al. Assessment of Ki67 in breast cancer: Recommendations from the International Ki67 in Breast Cancer working group. J. Natl. Cancer Inst. 2011, 103, 1656–1664. [Google Scholar] [CrossRef]
- Honma, N.; Horii, R.; Iwase, T.; Saji, S.; Younes, M.; Ito, Y.; Akiyama, F. Ki-67 evaluation at the hottest spot predicts clinical outcome of patients with hormone receptor-positive/HER2-negative breast cancer treated with adjuvant tamoxifen monotherapy. Breast Cancer 2015, 22, 71–78. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Ogston, K.N.; Miller, I.D.; Payne, S.; Hutcheon, A.W.; Sarkar, T.K.; Smith, I.; Schofield, A.; Heys, S.D. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival. Breast 2003, 12, 320–327. [Google Scholar] [CrossRef]
- Symmans, W.F.; Peintinger, F.; Hatzis, C.; Rajan, R.; Kuerer, H.; Valero, V.; Assad, L.; Poniecka, A.; Hennessy, B.; Green, M.; et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol. 2007, 25, 4414–4422. [Google Scholar] [CrossRef] [PubMed]
- Mamounas, E.P.; Anderson, S.J.; Dignam, J.J.; Bear, H.D.; Julian, T.B.; Geyer, C.E., Jr.; Taghian, A.; Wickerham, D.L.; Wolmark, N. Predictors of locoregional recurrence after neoadjuvant chemotherapy: Results from combined analysis of National Surgical Adjuvant Breast and Bowel Project B-18 and B-27. J. Clin. Oncol. 2012, 30, 3960–3966. [Google Scholar] [CrossRef] [PubMed]
- Provenzano, E.; Bossuyt, V.; Viale, G.; Cameron, D.; Badve, S.; Denkert, C.; MacGrogan, G.; Penault-Llorca, F.; Boughey, J.; Curigliano, G.; et al. Standardization of pathologic evaluation and reporting of postneoadjuvant specimens in clinical trials of breast cancer: Recommendations from an international working group. Mod. Pathol. 2015, 28, 1185–1201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Zhang, H.; Chen, T.; Yang, Q. Dose invasive apocrine adenocarcinoma has worse prognosis than invasive ductal carcinoma of breast: Evidence from SEER database. Oncotarget 2017, 8, 24579–24592. [Google Scholar] [CrossRef] [PubMed]
- Saridakis, A.; Berger, E.R.; Harigopal, M.; Park, T.; Horowitz, N.; Le Blanc, J.; Zanieski, G.; Chagpar, A.; Greenup, R.; Golshan, M.; et al. Apocrine Breast Cancer: Unique Features of a Predominantly Triple-Negative Breast Cancer. Ann. Surg. Oncol. 2021, 28, 5610–5616. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.Y.; Zhang, W.W.; Sun, J.Y.; Li, F.Y.; He, Z.Y.; Wu, S.G. The Clinicopathological Features and Survival Outcomes of Different Histological Subtypes in Triple-negative Breast Cancer. J. Cancer 2018, 9, 296–303. [Google Scholar] [CrossRef]
- Bareche, Y.; Venet, D.; Ignatiadis, M.; Aftimos, P.; Piccart, M.; Rothe, F.; Sotiriou, C. Unravelling triple-negative breast cancer molecular heterogeneity using an integrative multiomic analysis. Ann. Oncol. 2018, 29, 895–902. [Google Scholar] [CrossRef]
- Sun, X.; Zuo, K.; Yao, Q.; Zhou, S.; Shui, R.; Xu, X.; Bi, R.; Yu, B.; Cheng, Y.; Tu, X.; et al. Invasive apocrine carcinoma of the breast: Clinicopathologic features and comprehensive genomic profiling of 18 pure triple-negative apocrine carcinomas. Mod. Pathol. 2020, 33, 2473–2482. [Google Scholar] [CrossRef]
- Gucalp, A.; Tolaney, S.; Isakoff, S.J.; Ingle, J.N.; Liu, M.C.; Carey, L.A.; Blackwell, K.; Rugo, H.; Nabell, L.; Forero, A.; et al. Phase II trial of bicalutamide in patients with androgen receptor-positive, estrogen receptor-negative metastatic Breast Cancer. Clin. Cancer Res. 2013, 19, 5505–5512. [Google Scholar] [CrossRef]
- Meattini, I.; Pezzulla, D.; Saieva, C.; Bernini, M.; Orzalesi, L.; Sanchez, L.J.; Desideri, I.; Francolini, G.; Bonomo, P.; Greto, D.; et al. Triple Negative Apocrine Carcinomas as a Distinct Subtype of Triple Negative Breast Cancer: A Case-control Study. Clin. Breast Cancer 2018, 18, e773–e780. [Google Scholar] [CrossRef] [PubMed]
- Vranic, S.; Gatalica, Z. An Update on the Molecular and Clinical Characteristics of Apocrine Carcinoma of the Breast. Clin. Breast Cancer 2021. [Google Scholar] [CrossRef] [PubMed]
- Iwase, H.; Kurebayashi, J.; Tsuda, H.; Ohta, T.; Kurosumi, M.; Miyamoto, K.; Yamamoto, Y.; Iwase, T. Clinicopathological analyses of triple negative breast cancer using surveillance data from the Registration Committee of the Japanese Breast Cancer Society. Breast Cancer 2010, 17, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, N.; Moran, M.S.; Li, Y.; Liang, Y.; Su, P.; Haffty, B.G.; Yang, Q. Special subtypes with favorable prognosis in breast cancer: A registry-based cohort study and network meta-analysis. Cancer Treat. Rev. 2020, 91, 102108. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathologic Complete Response after Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-analysis. Clin. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, S.; Chen, C.; Di, G.; Liu, G.; Wu, J.; Shao, Z. Pathological complete response as a surrogate for relapse-free survival in patients with triple negative breast cancer after neoadjuvant chemotherapy. Oncotarget 2017, 8, 18399–18408. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shao, Z.; Chaudhri, S.; Guo, M.; Zhang, L.; Rea, D. Neoadjuvant Chemotherapy in Triple Negative Breast Cancer: An Observational Study. Oncol. Res. 2016, 23, 291–302. [Google Scholar] [CrossRef]
- Huang, M.; O’Shaughnessy, J.; Zhao, J.; Haiderali, A.; Cortes, J.; Ramsey, S.D.; Briggs, A.; Hu, P.; Karantza, V.; Aktan, G.; et al. Association of Pathologic Complete Response with Long-Term Survival Outcomes in Triple-Negative Breast Cancer: A Meta-Analysis. Cancer Res. 2020, 80, 5427–5434. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; O’Shaughnessy, J.; Zhao, J.; Haiderali, A.; Cortes, J.; Ramsey, S.; Briggs, A.; Karantza, V.; Aktan, G.; Qi, C.Z.; et al. Evaluation of Pathologic Complete Response as a Surrogate for Long-Term Survival Outcomes in Triple-Negative Breast Cancer. J. Natl. Compr. Cancer Netw. 2020, 18, 1096–1104. [Google Scholar] [CrossRef]
- Conforti, F.; Pala, L.; Sala, I.; Oriecuia, C.; De Pas, T.; Specchia, C.; Graffeo, R.; Pagan, E.; Queirolo, P.; Pennacchioli, E.; et al. Evaluation of pathological complete response as surrogate endpoint in neoadjuvant randomised clinical trials of early stage breast cancer: Systematic review and meta-analysis. BMJ 2021, 375, e066381. [Google Scholar] [CrossRef]
- Carey, L.A.; Dees, E.C.; Sawyer, L.; Gatti, L.; Moore, D.T.; Collichio, F.; Ollila, D.W.; Sartor, C.I.; Graham, M.L.; Perou, C.M. The triple negative paradox: Primary tumor chemosensitivity of breast cancer subtypes. Clin. Cancer Res. 2007, 13, 2329–2334. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; He, X.; Yu, Q.; Eng, C. Androgen receptor-induced tumor suppressor, KLLN, inhibits breast cancer growth and transcriptionally activates p53/p73-mediated apoptosis in breast carcinomas. Hum. Mol. Genet. 2013, 22, 2263–2272. [Google Scholar] [CrossRef]
- Traina, T.A.; Miller, K.; Yardley, D.A.; Eakle, J.; Schwartzberg, L.S.; O’Shaughnessy, J.; Gradishar, W.; Schmid, P.; Winer, E.; Kelly, C.; et al. Enzalutamide for the Treatment of Androgen Receptor-Expressing Triple-Negative Breast Cancer. J. Clin. Oncol. 2018, 36, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoi, H.; Grellety, T.; Tredan, O.; Saghatchian, M.; Dalenc, F.; Mailliez, A.; L’Haridon, T.; Cottu, P.; Abadie-Lacourtoisie, S.; You, B.; et al. A phase II trial of abiraterone acetate plus prednisone in patients with triple-negative androgen receptor positive locally advanced or metastatic breast cancer (UCBG 12-1). Ann. Oncol. 2016, 27, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Santonja, A.; Sanchez-Munoz, A.; Lluch, A.; Chica-Parrado, M.R.; Albanell, J.; Chacon, J.I.; Antolin, S.; Jerez, J.M.; de la Haba, J.; de Luque, V.; et al. Triple negative breast cancer subtypes and pathologic complete response rate to neoadjuvant chemotherapy. Oncotarget 2018, 9, 26406–26416. [Google Scholar] [CrossRef]
- Shousha, S.; Bull, T.B.; Southall, P.J.; Mazoujian, G. Apocrine carcinoma of the breast containing foam cells. An electron microscopic and immunohistological study. Histopathology 1987, 11, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Fuchinoue, F.; Hirotani, Y.; Nakanishi, Y.; Yamaguchi, H.; Nishimaki, H.; Noda, H.; Tang, X.Y.; Iizuka, M.; Amano, S.; Sugitani, M.; et al. Overexpression of PGC1alpha and accumulation of p62 in apocrine carcinoma of the breast. Pathol. Int. 2015, 65, 19–26. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TNAC | TNBC-NA | p | |
|---|---|---|---|
| Age at diagnosis (y) | 1.000 | ||
| 20–49 | 6 (30.0) | 6 (30.0) | |
| 50–69 | 11 (55.0) | 11 (55.0) | |
| 70–89 | 3 (15.0) | 3 (15.0) | |
| T stage | 0.196 | ||
| T1 | 16 (80.0) | 11 (55.0) | |
| T2 | 4 (20.0) | 8 (40.0) | |
| T3 | 0 (0) | 0 (0) | |
| T4 | 0 (0) | 1 (5.0) | |
| N stage | |||
| N0 | 18 (90.0) | 14 (70.0) | 0.348 |
| N1 | 1 (5.0) | 4 (20.0) | |
| N2 | 1 (5.0) | ||
| N3 | 1 (5.0) | 1 (5.0) | |
| AJCC stage | 0.323 | ||
| IA | 14 (70.0) | 10 (50.0) | |
| IIA | 5 (25.0) | 5 (25.0) | |
| IIB | 0 (0) | 3 (15.0) | |
| IIIA | 0 (0) | 1 (5.0) | |
| IIIB | 0 (0) | 0 (0) | |
| IIIC | 1 (5.0) | 1 (5.0) | |
| Radiation | 0.500 | ||
| No | 15 (75.0) | 12 (60.0) | |
| Yes | 5 (25.0) | 8 (40.0) | |
| Surgery type | 1.000 | ||
| BCS * | 7 (35.0) | 6 (30.0) | |
| Mastectomy | 13 (65.0) | 14 (70.0) | |
| Laterality | 0.747 | ||
| Left | 7 (35.0) | 9 (45.0) | |
| Right | 13 (65.0) | 11 (55.0) | |
| Ki-67 (%) | <0.001 | ||
| 0–29 | 18 (90.0) | 2 (10.0) | |
| 30–59 | 2 (10.0) | 3 (15.0) | |
| 60–99 | 0 (0.0) | 15 (75.0) | |
| Histologic grade | 0.006 | ||
| I | 8 (40.0) | 1 (5.0) | |
| II | 5 (25.0) | 4 (20.0) | |
| III | 5 (25.0) | 15 (75.0) | |
| Missing | 2 (10.0) | ||
| TILs | 0.051 | ||
| 0–10 | 11 (61.1) | 6 (30.0) | |
| 11–40 | 6 (33.3) | 7 (35.0) | |
| 41–90 | 1 (5.6) | 7 (35.0) |
| TNAC | TNBC-NA | p | |
|---|---|---|---|
| Age at diagnosis (y) | |||
| 20–49 | 6 (28.6) | 6 (28.6) | 1.000 |
| 50–69 | 15 (71.4) | 15 (71.4) | |
| 70–89 | 0 (0.0) | 0 (0.0) | |
| T stage | |||
| T1 | 16 (76.2) | 13 (61.9) | 0.767 |
| T2 | 3 (14.3) | 5 (23.8) | |
| T3 | 1 (4.8) | 1 (4.8) | |
| T4 | 1 (4.8) | 2 (9.5) | |
| N stage | |||
| N0 | 16 (76.2) | 12 (57.1) | 0.065 |
| N1 | 0 (0) | 6 (28.6) | |
| N2 | 4 (19.0) | 2 (9.5) | |
| N3 | 1 (4.8) | 1 (4.8) | |
| AJCC stage | |||
| IA | 13 (61.9) | 8 (38.1) | 0.541 |
| IIA | 2 (9.5) | 6 (28.6) | |
| IIB | 1 (4.8) | 2 (9.5) | |
| IIIA | 3 (14.3) | 2 (9.5) | |
| IIIB | 1 (4.8) | 2 (9.5) | |
| IIIC | 1 (4.8) | 1 (4.8) | |
| Radiation | |||
| No | 12 (57.1) | 10 (47.6) | 0.757 |
| Yes | 9 (42.9) | 11 (52.4) | |
| Surgery type | |||
| BCS | 8 (38.1) | 6 (28.6) | 0.743 |
| Mastectomy | 13 (61.9) | 15 (71.4) | |
| Laterality | |||
| Left | 14 (66.7) | 13 (61.9) | 1.000 |
| Right | 7 (33.3) | 8 (38.1) | |
| Ki-67 (%) | |||
| 0–29 | 19 (90.5) | 4 (19.0) | <0.001 |
| 30–59 | 2 (9.5) | 7 (33.3) | |
| 60–99 | 0 (0.0) | 10 (47.6) | |
| Histologic grade | |||
| I | 6 (28.6) | 2 (9.5) | 0.164 |
| II | 11 (52.4) | 11 (52.4) | |
| III | 2 (9.5) | 7 (33.3) | |
| Missing | 2 (9.5) | 1 (4.8) | |
| TILs | |||
| 0–10 | 14 (73.7) | 9 (45.0) | 0.097 |
| 11–40 | 2 (10.5) | 8 (40.0) | |
| 41–90 | 3 (15.8) | 3 (15.0) |
| Neoadjuvant Therapy | Clinical Evaluation | T Stage | N Stage | MP Grade | RCB | Ki-67 (%) | Histologic Grade | TILs (%) | |
|---|---|---|---|---|---|---|---|---|---|
| TNAC-1 | ddEC/T1w | Unk/SD | 1 | 0 | 3 | II | 5 | I | 2 |
| TNAC-2 | AC-T | Unk | 4 | 2 | 2 | III | 30 | II | 15 |
| TNAC-3 | TP1w/CEF/DF | SD/SD/PR | 1 | 0 | 2 | II | 20 | I | 5 |
| TNAC-4 | TP/CEF/NP | SD/SD/PR | 1 | 2 | 2 | III | 10 | II | 40 |
| TNAC-5 | TPX | PR | 1 | 0 | 2 | II | 5 | II | 8 |
| TNAC-6 | TP1w | PR | 1 | 0 | 4 | I | 10 | II | 1 |
| TNAC-7 | ddEC/T1w | SD/PR | 1 | 0 | 3 | II | 20 | II | 1 |
| TNAC-8 | TP1w | SD | 1 | 0 | 3 | II | 10 | II | 60 |
| TNAC-9 | CEF/TP1w | Unk/PR | 1 | 0 | 3 | I | 10 | I | 3 |
| TNAC-10 | T1w/EC | Unk/PR | 2 | 0 | 4 | II | 5 | II | 5 |
| TNAC-11 | T1w/AC | Unk/SD | 2 | 2 | 2 | III | 15 | II | 10 |
| TNAC-12 | ddEC/ddT175 | Unk | 1 | 0 | 2 | II | 20 | I | 5 |
| TNAC-13 | TPX/AC | Unk/PR | 1 | 0 | 3 | II | 15 | I | 0 |
| TNAC-14 | CEF | SD | 1 | 2 | 2 | III | 20 | Unk | Unk |
| TNAC-15 | EC | SD | 1 | 0 | 2 | II | 20 | II | 3 |
| TNAC-16 | TP/NE/DCF/NP | Unk/Unk/Unk/PR | 1 | 0 | 2 | II | 5 | I | 0 |
| TNAC-17 | CEF/TP1w | Unk/PR | 1 | 3 | 2 | III | 25 | III | 3 |
| TNAC-18 | ddEC/ddT175 | Unk/PR | 1 | 0 | 3 | II | 20 | II | 45 |
| TNAC-19 | ddEC/T1w | Unk/SD | 2 | 0 | 3 | II | 5 | II | 80 |
| TNAC-20 | ddEC/T1w | PR/SD | 1 | 0 | 3 | II | 40 | Unk | Unk |
| TNAC-21 | TX | SD | 3 | 0 | 1 | II | 15 | III | 2 |
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| No Chemo | Chemo | p-Value | No Chemo | Chemo | p-Value | |
| Sample size | 151 | 291 | 87 | 87 | ||
| Age group | <0.001 | 1.000 | ||||
| <50 years | 5 (3.3) | 40 (13.7) | 3 (3.4) | 3 (3.4) | ||
| 50–69 years | 41 (27.2) | 191 (65.6) | 36 (41.4) | 36 (41.4) | ||
| 70+ years | 105 (69.5) | 60 (20.6) | 48 (55.2) | 48 (55.2) | ||
| Income | 0.579 | 0.456 | ||||
| USD 50,000–69,999 | 74 (49.0) | 129 (44.3) | 43 (49.4) | 35 (40.2) | ||
| USD 70,000+ | 56 (37.1) | 113 (38.8) | 30 (34.5) | 34 (39.1) | ||
| <USD 50,000 | 21 (13.9) | 49 (16.8) | 14 (16.1) | 18 (20.7) | ||
| Race | 0.542 | 0.765 | ||||
| Hispanic (All races) | 11 (7.3) | 25 (8.6) | 7 (8.0) | 6 (6.9) | ||
| Non-Hispanic Asian or Pacific Islander | 19 (12.6) | 37 (12.7) | 13 (14.9) | 16 (18.4) | ||
| Non-Hispanic Black | 26 (17.2) | 40 (13.7) | 13 (14.9) | 9 (10.3) | ||
| Non-Hispanic White | 95 (62.9) | 185 (63.6) | 54 (62.1) | 56 (64.4) | ||
| Others | 0 (0.0) | 4 (1.4) | 0 (0.0) | 0 (0.0) | ||
| Stage | <0.001 | 1.000 | ||||
| I | 81 (53.6) | 68 (23.4) | 44 (50.6) | 44 (50.6) | ||
| II | 25 (16.6) | 92 (31.6) | 18 (20.7) | 18 (20.7) | ||
| III | 5 (3.3) | 27 (9.3) | 3 (3.4) | 3 (3.4) | ||
| IV | 1 (0.7) | 5 (1.7) | 0 (0.0) | 0 (0.0) | ||
| Unk | 39 (25.8) | 99 (34.0) | 22 (25.3) | 22 (25.3) | ||
| Grade | <0.001 | 1.000 | ||||
| Well-differentiated; Grade I | 21 (13.9) | 12 (4.1) | 8 (9.2) | 8 (9.2) | ||
| Moderately differentiated; Grade II | 90 (59.6) | 159 (54.6) | 62 (71.3) | 62 (71.3) | ||
| Poorly differentiated; Grade III | 34 (22.5) | 106 (36.4) | 16 (18.4) | 16 (18.4) | ||
| Undifferentiated; anaplastic; Grade IV | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Unk | 5 (3.3) | 14 (4.8) | 1 (1.1) | 1 (1.1) | ||
| Sequence | 0.926 | 0.316 | ||||
| 1st of 2 or more primaries | 19 (12.6) | 39 (13.4) | 12 (13.8) | 18 (20.7) | ||
| One primary only | 132 (87.4) | 252 (86.6) | 75 (86.2) | 69 (79.3) | ||
| Surgery | 0.033 | 1.000 | ||||
| No | 9 (6.0) | 5 (1.7) | 0 (0.0) | 0 (0.0) | ||
| Yes | 142 (94.0) | 286 (98.3) | 87 | 87 | ||
| Radiation | 0.019 | 1.000 | ||||
| No | 77 (51.0) | 113 (38.8) | 39 (44.8) | 39 (44.8) | ||
| Yes | 74 (49.0) | 178 (61.2) | 48 (55.2) | 48 (55.2) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, T.; Liu, Y.; Wu, J.; Hu, X.L.; Zhao, G.; Liang, B.; Wang, S.; Long, M. Triple-Negative Apocrine Breast Carcinoma Has Better Prognosis despite Poor Response to Neoadjuvant Chemotherapy. J. Clin. Med. 2022, 11, 1607. https://doi.org/10.3390/jcm11061607
Hu T, Liu Y, Wu J, Hu XL, Zhao G, Liang B, Wang S, Long M. Triple-Negative Apocrine Breast Carcinoma Has Better Prognosis despite Poor Response to Neoadjuvant Chemotherapy. Journal of Clinical Medicine. 2022; 11(6):1607. https://doi.org/10.3390/jcm11061607
Chicago/Turabian StyleHu, Taobo, Yiqiang Liu, Jinbo Wu, Xuejiao Lina Hu, Guiyang Zhao, Baosheng Liang, Shu Wang, and Mengping Long. 2022. "Triple-Negative Apocrine Breast Carcinoma Has Better Prognosis despite Poor Response to Neoadjuvant Chemotherapy" Journal of Clinical Medicine 11, no. 6: 1607. https://doi.org/10.3390/jcm11061607
APA StyleHu, T., Liu, Y., Wu, J., Hu, X. L., Zhao, G., Liang, B., Wang, S., & Long, M. (2022). Triple-Negative Apocrine Breast Carcinoma Has Better Prognosis despite Poor Response to Neoadjuvant Chemotherapy. Journal of Clinical Medicine, 11(6), 1607. https://doi.org/10.3390/jcm11061607