
Acute Arterial Thrombosis of Lower Extremities in COVID-19 Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
Clinical Data
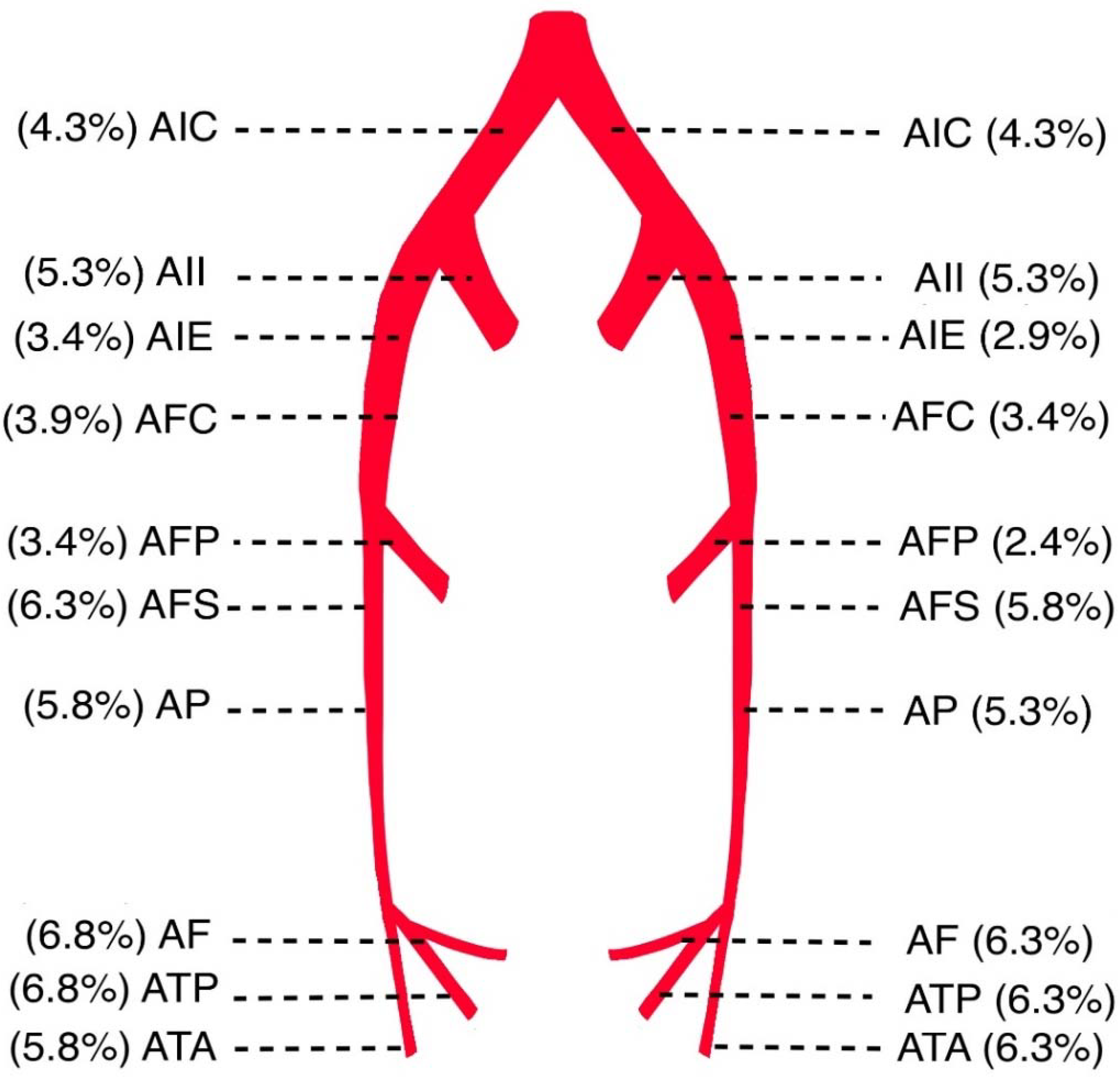
Parameters Related to Arterial Thrombosis
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Bonow, R.O.; Fonarow, G.C.; O’Gara, P.T.; Yancy, C.W. Association of Coronavirus Disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. 2020, 5, 51–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannis, D.; Ziogas, I.A.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J. Clin. Virol. 2020, 127, 104362. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.A.; Sheikh, F.N.; Jamal, S.; Ezeh, J.K.; Akhtar, A. Coronavirus (COVID-19): A review of clinical features, diagnosis, and treatment. Cureus 2020, 12, e7355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: A retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Branchford, B.R.; Carpenter, S.L. The role of inflammation in venous thromboembolism. Front. Pediatr. 2018, 6, 142. [Google Scholar] [CrossRef]
- Sönmez, O.; Ertaş, G.; Bacaksız, A.; Tasal, A.; Erdoğan, E.; Asoğlu, E.; Uyarel, H.; Göktekin, O. Relation of neutrophil-to-lymphocyte ratio with the presence and complexity of coronary artery disease: An observational study. Anadolu Kardiyol. Derg. 2013, 13, 662–667. [Google Scholar] [CrossRef]
- Spiezia, L.; Boscolo, A.; Poletto, F.; Cerutti, L.; Tiberio, I.; Campello, E.; Navalesi, P.; Simioni, P. COVID-19-related severe hypercoagulability in patients admitted to intensive care unit for acute respiratory failure. Thromb. Haemost. 2020, 120, 998–1000. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J. D-dimer is associated with severity of coronavirus disease 2019: A pooled analysis. Thromb. Haemost. 2020, 120, 876–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, B.M.; De Oliveira, M.H.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veerasuri, S.; Kulkarni, S.R.; Wilson, W.R.; Paravastu, S.C.V. Bilateral Acute Lower Limb Ischemia Secondary to COVID-19. Vasc. Endovasc. Surg. 2021, 55, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Callum, K.; Bradbury, A. ABC of arterial and venous disease: Acute limb ischaemia. BMJ 2000, 18, 764–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eliason, J.L.; Wainess, R.M.; Proctor, M.C.; Dimick, J.B.; Cowan, J.A., Jr.; Upchurch, G.R., Jr.; Stanley, J.C.; Henke, P.K. A national and single institutional experience in the contemporary treatment of acute lower extremity ischemia. Ann. Surg. 2003, 238, 382–389; discussion 389–390. [Google Scholar] [CrossRef]
- Ogawa, M.; Doo, F.X.; Somwarn, A.S.; Rondenko, A.; Kamath, A.; Friedman, B. Peripheral arterial occlusion due to COVID-19: CT angiography findings of nine patients. Clin. Imaging 2021, 73, 43–47. [Google Scholar] [CrossRef]
- Ali, M.A.M.; Spinler, S.A. COVID-19 and thrombosis: From bench to bedside. Trends Cardiovasc. Med. 2021, 31, 143–160. [Google Scholar] [CrossRef]
- Han, H.; Yang, L.; Liu, R.; Liu, F.; Wu, K.L.; Li, J.; Liu, X.H.; Zhu, C.L. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2020, 58, 1116–1120. [Google Scholar] [CrossRef] [Green Version]
- Bellosta, R.; Luzzani, L.; Natalini, G.; Pegorer, M.A.; Attisani, L.; Cossu, L.G.; Ferrandina, C.; Fossati, A.; Conti, E.; Bush, R.L.; et al. Acute limb ischemia in patients with COVID-19 pneumonia. J. Vasc. Surg. 2020, 72, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, M.; Umeton, R.P.; Keyhanian, K.; Mohit, B.; Rahimian, N.; Eshaghhosseiny, N.; Davoudi, V. SARS-CoV-2 and Acute Cerebrovascular Events: An Overview. J. Clin. Med. 2021, 10, 3349. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Cantador, E.; Núñez, A.; Sobrino, P.; Espejo, V.; Fabia, L.; Vela, L.; De Benito, L.; Botas, J. Incidence and consequences of systemic arterial thrombotic events in COVID-19 patients. J. Thromb. Thrombolysis 2020, 50, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Prozan, L.; Shusterman, E.; Ablin, J.; Mitelpunkt, A.; Weiss-Meilik, A.; Adler, A.; Choshen, G.; Kehat, O. Prognostic value of neutrophil-to-lymphocyte ratio in COVID-19 compared with Influenza and respiratory syncytial virus infection. Sci. Rep. 2021, 11, 21519. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef] [PubMed]
- Cheruiyot, I.; Kipkorir, V.; Ngure, B.; Misiani, M.; Munguti, J.; Ogeng’o, J. Arterial Thrombosis in Coronavirus Disease 2019 Patients: A Rapid Systematic Review. Ann. Vasc. Surg. 2021, 70, 273–281. [Google Scholar] [CrossRef]
- Etkin, Y.; Conway, A.M.; Silpe, J.; Qato, K.; Carroccio, A.; Manvar-Singh, P.; Giangola, G.; Deitch, J.S.; Davila-Santini, L.; Schor, J.A.; et al. Acute Arterial Thromboembolism in Patients with COVID-19 in the New York City Area. Ann. Vasc. Surg. 2021, 70, 290–294. [Google Scholar] [CrossRef]
- Singh, B.; Kaur, P.; Patel, P.; Nabati, C.; Ayad, S.; Shamoon, F.; Maroules, M. COVID-19 and arterial thrombosis: Report of 2 cases. Radiol. Case Rep. 2021, 16, 1603–1607. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total No. of Patients | n = 17 |
|---|---|
| Age, years (median) | 75.0 (61–90) |
| Gender, n (%) | |
| Male | 11 (64.7) |
| Female | 6 (35.3) |
| Blood type, n (%) | |
| O | 5 (29.4) |
| A | 10 (58.8) |
| AB | 2 (11.8) |
| Comorbidities, n (%) | |
| Arterial hypertension | 10 (50.0) |
| Diabetes mellitus type 2 | 3 (15.5) |
| Hypothyroidism | 3 (15.5) |
| Atrial fibrillation | 3 (15.5) |
| Rheumatoid arthritis | 1 (5.0) |
| COVID-19 day at admission | |
| Mean (SD) | 7.65 (3.45) |
| Arteriothrombosis diagnosis day | |
| Mean (SD) | 9.76 (2.68) |
| History of anticoagulant therapy, n (%) | 3 (16.7) |
| Patients with acute respiratory failure, n (%) | 10 (58.8) |
| Patients receiving oxygen therapy, n (%) | 12 (70.5) |
| Patients with oxygen therapy via HFNC, n (%) | 7 (41.2) |
| Characteristics, Mean (SD) | Patients Values | Patients with Pneumonia | Patients without Pneumonia | p |
|---|---|---|---|---|
| Neutrophils, ×109/L | 14.22 (6.72) | 15.88 (6.19) | 8.39 (5.67) | 0.025 * |
| Lymphocytes, ×109/L | 0.98 (0.55) | 0.88 (0.51) | 1.35 (0.55) | 0.018 * |
| LDH U/L | 725.6 (532.9) | 841.0 (552.7) | 321.8 (79.9) | 0.038 * |
| CRP, mg/L | 92.4 (78.7) | 111.0 (79.2) | 27.4 (25.4) | 0.016 * |
| D-dimer mg/L | 22.11 (11.08) | 24.78 (9.12) | 12.73 (13.59) | 0.170 |
| Thrombocytes ×109/L | 305.78 (114.67) | 297.07 (107.98) | 336.25 (149.61) | 0.611 |
| Creatine kinase U/L | 1301.28 (1356.16) | 1554.57 (1421.12) | 415.75 (568.07) | 0.031 * |
| NT-proBNP pg/mL | 1849.94 (2104.41) | 2042.71 (2361.44) | 1175.25 (387.48) | 0.556 |
| Troponin ng/L | 91.63 (129.25) | 96.22 (144.88) | 75.55 (57.04) | 0.758 |
| Neutrophils-lymphocyte ratio (NLR) | 22.4 (20.1) | 27.0 (20.5) | 6.1 (2.2) | 0.035 * |
| %PT | 73 (22) | 72 (22) | 78 (22) | 0.555 |
| INR | 1.22 (0.12) | 1.23 (1.13) | 1.19 (0.11) | 0.875 |
| All Patients | Patients with Pneumonia | Patients without Pneumonia | |
|---|---|---|---|
| n = 17 | n = 13 | n = 4 | |
| Patients with unilateral occlusions, n (%) | 1 (5.9) | 1 (5.9) | 0 |
| Patients with bilateral occlusions, n (%) | 16 (94.1) | 12 (70.6) | 4 (23.5) |
| Occlusions by stenosis degree, n (%) | |||
| Subocclusions | 126 (62.1) | 100 (49.3) | 26 (12.8) |
| Total occlusions (100%) | 77 (37.9) | 59 (29.1) | 18 (8.8) |
| Thrombus length, n (%) b | |||
| Short segment occlusions (<10 cm) | 36 (32.4) | 34 (30.6) | 2 (1.8) |
| Intermediate segment occlusions (10–20 cm) | 21 (18.9) | 13 (11.7) | 8 (7.2) |
| Long segment occlusions (>20 cm) | 54 (48.7) | 39 (35.1) | 15 (13.5) |
| Anticoagulant therapy before surgery, n (%) a | |||
| Prophylaxis dose | 14 (82.4) | 11 (64.7) | 3 (17.6) |
| Therapeutic dose | 3 (17.6) | 2 (11.8) | 1 (5.9) |
| Intervention, n (%) | |||
| Conservative (LMWH) | 2 (11.8) | 1 (5.9) | 1 (5.9) |
| Thrombectomy | 9 (52.9) | 6 (35.3) | 3 (17.6) |
| Amputation | 6 (35.3) | 6 (35.3) | 0 |
| Outcome, n (%) | |||
| Death | 10 (58.8) | 10 (58.8) | 0 |
| Discharge | 7 (41.2) | 3 (17.6) | 4 (23.5) |
| CXR chest X-ray, LMWH low molecular weight heparin. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glavinic, R.; Marcic, L.; Dumancic, S.; Pavicic Ivelja, M.; Jeličić, I.; Kalibovic Govorko, D.; Medvedec Mikić, I. Acute Arterial Thrombosis of Lower Extremities in COVID-19 Patients. J. Clin. Med. 2022, 11, 1538. https://doi.org/10.3390/jcm11061538
Glavinic R, Marcic L, Dumancic S, Pavicic Ivelja M, Jeličić I, Kalibovic Govorko D, Medvedec Mikić I. Acute Arterial Thrombosis of Lower Extremities in COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(6):1538. https://doi.org/10.3390/jcm11061538
Chicago/Turabian StyleGlavinic, Robert, Ljiljana Marcic, Stipe Dumancic, Mirela Pavicic Ivelja, Irena Jeličić, Danijela Kalibovic Govorko, and Ivana Medvedec Mikić. 2022. "Acute Arterial Thrombosis of Lower Extremities in COVID-19 Patients" Journal of Clinical Medicine 11, no. 6: 1538. https://doi.org/10.3390/jcm11061538
APA StyleGlavinic, R., Marcic, L., Dumancic, S., Pavicic Ivelja, M., Jeličić, I., Kalibovic Govorko, D., & Medvedec Mikić, I. (2022). Acute Arterial Thrombosis of Lower Extremities in COVID-19 Patients. Journal of Clinical Medicine, 11(6), 1538. https://doi.org/10.3390/jcm11061538