
Association of Hippocampal Subfield Volumes with Amyloid-Beta Deposition in Alzheimer’s Disease



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Acquisition of PET and MR Images
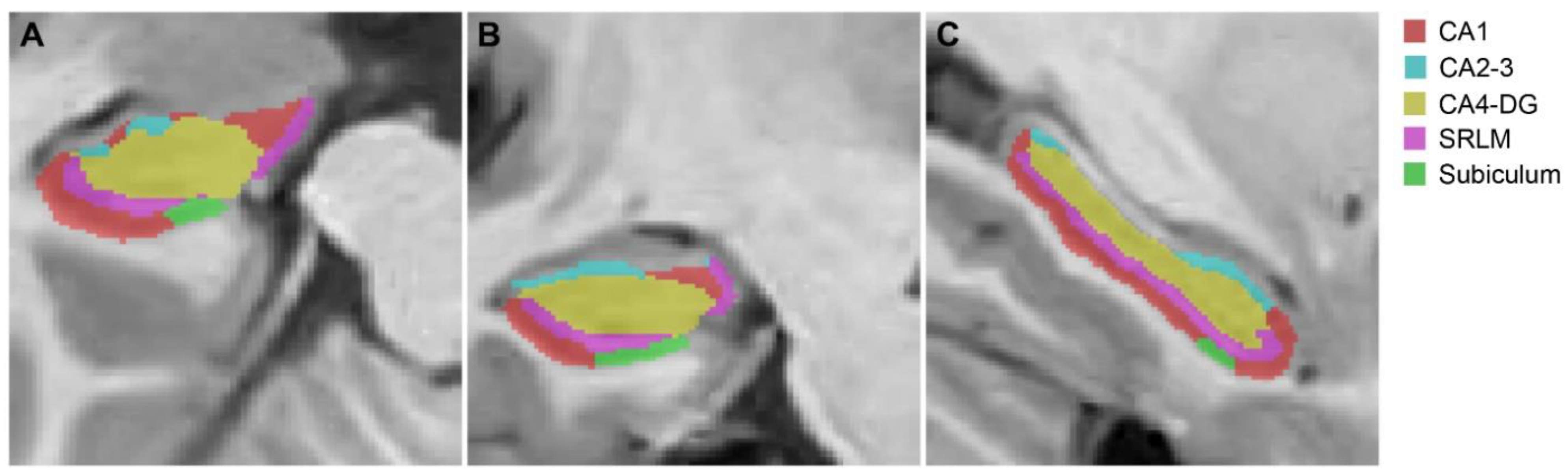
2.3. Image Processing Steps
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
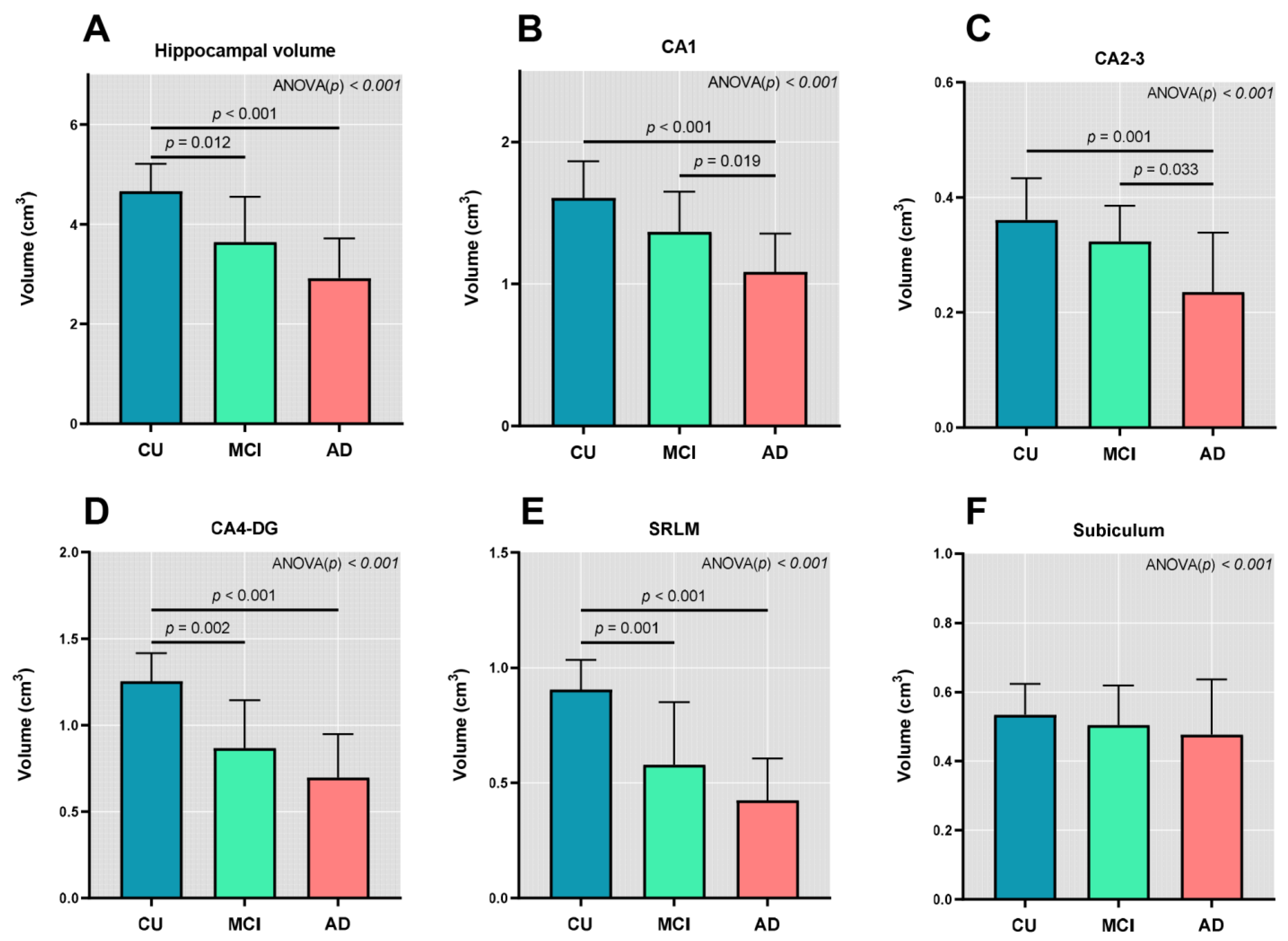
3.2. Hippocampal Subfields Volumes
3.3. Correlation between Hippocampal Subfield Volumes and Regional Aβ Deposition
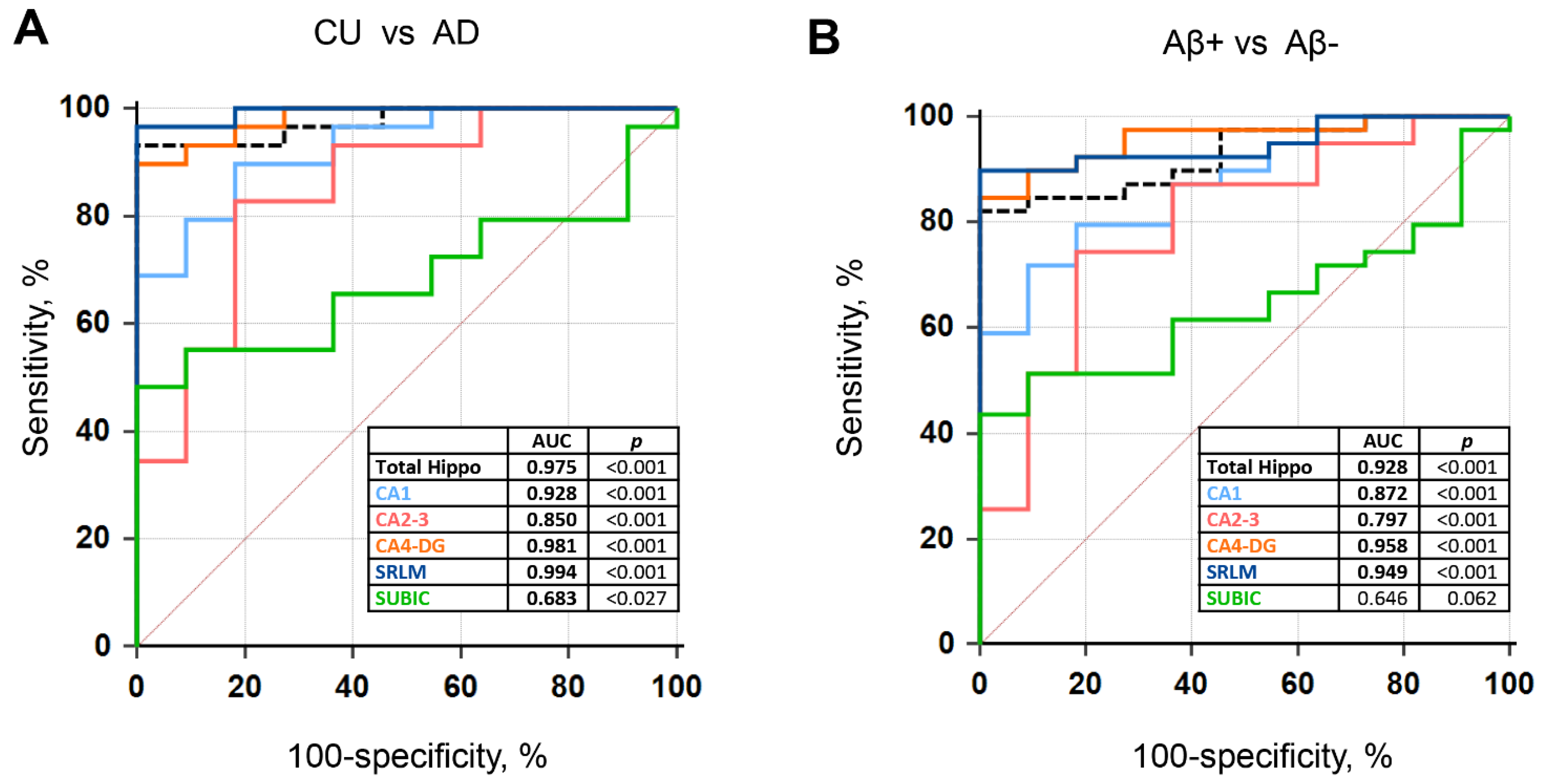
3.4. ROC Curves of the Hippocampal Subfield Volumes
3.5. Multiple Regressions Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eichenbaum, H.; Sauvage, M.; Fortin, N.; Komorowski, R.; Lipton, P. Towards a functional organization of episodic memory in the medial temporal lobe. Neurosci. Biobehav. Rev. 2012, 36, 1597–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battaglia, F.P.; Benchenane, K.; Sirota, A.; Pennartz, C.M.; Wiener, S.I. The hippocampus: Hub of brain network communication for memory. Trends Cogn. Sci. 2011, 15, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Lowe, V.J.; Senjem, M.L.; Weigand, S.D.; Kemp, B.J.; Shiung, M.M.; Knopman, D.S.; Boeve, B.F.; Klunk, W.E.; Mathis, C.A. 11C PiB and structural MRI provide complementary information in imaging of Alzheimer’s disease and amnestic mild cognitive impairment. Brain 2008, 131, 665–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, C.R.; Wiste, H.J.; Vemuri, P.; Weigand, S.D.; Senjem, M.L.; Zeng, G.A.; Bernstein, M.A.; Gunter, J.L.; Pankratz, V.S.; Aisen, P.S.; et al. Brain beta-amyloid measures and magnetic resonance imaging atrophy both predict time-to-progression from mild cognitive impairment to Alzheimer’s disease. Brain 2010, 133, 3336–3348. [Google Scholar] [CrossRef]
- Cardenas, V.A.; Chao, L.L.; Studholme, C.; Yaffe, K.; Miller, B.L.; Madison, C.; Buckley, S.T.; Mungas, D.; Schuff, N.; Weiner, M.W. Brain atrophy associated with baseline and longitudinal measures of cognition. Neurobiol. Aging 2011, 32, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R., Jr.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Wang, L.; Swank, J.S.; Glick, I.E.; Gado, M.H.; Miller, M.I.; Morris, J.C.; Csernansky, J.G. Changes in hippocampal volume and shape across time distinguish dementia of the Alzheimer type from healthy aging. Neuroimage 2003, 20, 667–682. [Google Scholar] [CrossRef]
- Kandel, E.R.; Schwartz, J.H.; Jessell, T.M.; Siegelbaum, S.; Hudspeth, A.J.; Mack, S. Principles of Neural Science; McGraw-Hill: New York, NY, USA, 2000; Volume 4, pp. 1490–1491. [Google Scholar]
- Dimsdale-Zucker, H.R.; Ritchey, M.; Ekstrom, A.D.; Yonelinas, A.P.; Ranganath, C. CA1 and CA3 differentially support spontaneous retrieval of episodic contexts within human hippocampal subfields. Nat. Commun. 2018, 9, 294. [Google Scholar] [CrossRef] [Green Version]
- Veldsman, M.; Nobis, L.; Alfaro-Almagro, F.; Manohar, S.; Husain, M. The human hippocampus and its subfield volumes across age, sex and APOE e4 status. Brain Commun. 2021, 3, fcaa219. [Google Scholar] [CrossRef]
- Nadal, L.; Coupe, P.; Helmer, C.; Manjon, J.V.; Amieva, H.; Tison, F.; Dartigues, J.F.; Catheline, G.; Planche, V. Differential annualized rates of hippocampal subfields atrophy in aging and future Alzheimer’s clinical syndrome. Neurobiol. Aging 2020, 90, 75–83. [Google Scholar] [CrossRef]
- Izzo, J.; Andreassen, O.A.; Westlye, L.T.; van der Meer, D. The association between hippocampal subfield volumes in mild cognitive impairment and conversion to Alzheimer’s disease. Brain Res. 2020, 1728, 146591. [Google Scholar] [CrossRef] [PubMed]
- Beach, T.G.; Monsell, S.E.; Phillips, L.E.; Kukull, W. Accuracy of the clinical diagnosis of Alzheimer disease at National Institute on Aging Alzheimer Disease Centers, 2005–2010. J. Neuropathol. Exp. Neurol. 2012, 71, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.T.; Dickson, D.W.; Trojanowski, J.Q.; Jack, C.R.; Boyle, P.A.; Arfanakis, K.; Rademakers, R.; Alafuzoff, I.; Attems, J.; Brayne, C.; et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): Consensus working group report. Brain 2019, 142, 1503–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, N.; Aarsland, D.; Honarpisheh, H.; Beyer, M.K.; Somme, J.H.; Elashoff, D.; Rongve, A.; Tysnes, O.B.; Thompson, P.M.; Apostolova, L.G. Comparing hippocampal atrophy in Alzheimer’s dementia and dementia with lewy bodies. Dement. Geriatr. Cogn. Disord. 2012, 34, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Coughlin, D.G.; Ittyerah, R.; Peterson, C.; Phillips, J.S.; Miller, S.; Rascovsky, K.; Weintraub, D.; Siderowf, A.D.; Duda, J.E.; Hurtig, H.I.; et al. Hippocampal subfield pathologic burden in Lewy body diseases vs. Alzheimer’s disease. Neuropathol. Appl. Neurobiol. 2020, 46, 707–721. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Sabri, O.; Sabbagh, M.N.; Seibyl, J.; Barthel, H.; Akatsu, H.; Ouchi, Y.; Senda, K.; Murayama, S.; Ishii, K.; Takao, M.; et al. Florbetaben PET imaging to detect amyloid beta plaques in Alzheimer’s disease: Phase 3 study. Alzheimers Dement. 2015, 11, 964–974. [Google Scholar] [CrossRef] [Green Version]
- Villemagne, V.L.; Ong, K.; Mulligan, R.S.; Holl, G.; Pejoska, S.; Jones, G.; O’Keefe, G.; Ackerman, U.; Tochon-Danguy, H.; Chan, J.G.; et al. Amyloid imaging with (18)F-florbetaben in Alzheimer disease and other dementias. J. Nucl. Med. 2011, 52, 1210–1217. [Google Scholar] [CrossRef] [Green Version]
- Romero, J.E.; Coupe, P.; Manjon, J.V. HIPS: A new hippocampus subfield segmentation method. Neuroimage 2017, 163, 286–295. [Google Scholar] [CrossRef] [Green Version]
- Winterburn, J.L.; Pruessner, J.C.; Chavez, S.; Schira, M.M.; Lobaugh, N.J.; Voineskos, A.N.; Chakravarty, M.M. A novel in vivo atlas of human hippocampal subfields using high-resolution 3 T magnetic resonance imaging. Neuroimage 2013, 74, 254–265. [Google Scholar] [CrossRef]
- Cho, H.; Choi, J.Y.; Hwang, M.S.; Kim, Y.J.; Lee, H.M.; Lee, H.S.; Lee, J.H.; Ryu, Y.H.; Lee, M.S.; Lyoo, C.H. In vivo cortical spreading pattern of tau and amyloid in the Alzheimer disease spectrum. Ann. Neurol. 2016, 80, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate - a Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Mueller, S.G.; Schuff, N.; Yaffe, K.; Madison, C.; Miller, B.; Weiner, M.W. Hippocampal atrophy patterns in mild cognitive impairment and Alzheimer’s disease. Hum. Brain Mapp. 2010, 31, 1339–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsia, A.Y.; Masliah, E.; McConlogue, L.; Yu, G.Q.; Tatsuno, G.; Hu, K.; Kholodenko, D.; Malenka, R.C.; Nicoll, R.A.; Mucke, L. Plaque-independent disruption of neural circuits in Alzheimer’s disease mouse models. Proc. Natl. Acad. Sci. USA 1999, 96, 3228–3233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boutet, C.; Chupin, M.; Lehericy, S.; Marrakchi-Kacem, L.; Epelbaum, S.; Poupon, C.; Wiggins, C.; Vignaud, A.; Hasboun, D.; Defontaines, B.; et al. Detection of volume loss in hippocampal layers in Alzheimer’s disease using 7 T MRI: A feasibility study. NeuroImage Clinl. 2014, 5, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Kerchner, G.A.; Hess, C.P.; Hammond-Rosenbluth, K.E.; Xu, D.; Rabinovici, G.D.; Kelley, D.A.; Vigneron, D.B.; Nelson, S.J.; Miller, B.L. Hippocampal CA1 apical neuropil atrophy in mild Alzheimer disease visualized with 7-T MRI. Neurology 2010, 75, 1381–1387. [Google Scholar] [CrossRef] [Green Version]
- de Flores, R.; La Joie, R.; Landeau, B.; Perrotin, A.; Mezenge, F.; de La Sayette, V.; Eustache, F.; Desgranges, B.; Chetelat, G. Effects of age and Alzheimer’s disease on hippocampal subfields: Comparison between manual and FreeSurfer volumetry. Hum. Brain Mapp 2015, 36, 463–474. [Google Scholar] [CrossRef]
- La Joie, R.; Perrotin, A.; de La Sayette, V.; Egret, S.; Doeuvre, L.; Belliard, S.; Eustache, F.; Desgranges, B.; Chetelat, G. Hippocampal subfield volumetry in mild cognitive impairment, Alzheimer’s disease and semantic dementia. Neuroimage Clin. 2013, 3, 155–162. [Google Scholar] [CrossRef]
- Hsu, P.J.; Shou, H.; Benzinger, T.; Marcus, D.; Durbin, T.; Morris, J.C.; Sheline, Y.I. Amyloid burden in cognitively normal elderly is associated with preferential hippocampal subfield volume loss. J. Alzheimers Dis. 2015, 45, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knierim, J.J. The hippocampus. Curr. Biol. 2015, 25, R1116–R1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.F.; Cai, L.; Zhou, J.N. Observation of the density and size of cells in hippocampus and vascular lesion in thalamus of GFAP-apoE transgenic mice. Neurosci. Bull. 2009, 25, 167–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, G.Z.; He, Y.C.; Ma, X.K.; Li, S.T.; Chen, D.J.; Gao, M.; Qiu, S.F.; Yin, J.X.; Shi, J.; Wu, J. Hippocampal synaptic and neural network deficits in young mice carrying the human APOE 4 gene. CNS Neurosci. Ther. 2017, 23, 748–758. [Google Scholar] [CrossRef] [Green Version]
- Samara, A.; Raji, C.A.; Li, Z.; Hershey, T. Comparison of Hippocampal Subfield Segmentation Agreement between 2 Automated Protocols across the Adult Life Span. AJNR Am. J. Neurol. 2021, 42, 1783–1789. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| CU | MCI | AD | |
|---|---|---|---|
| N | 11 | 10 | 29 |
| Age (years) | 65.8 ± 7.3 | 73.8 ± 9.4 a | 77.1 ± 8.4 b |
| Sex (M:F) | 6:5 | 7:3 | 13:16 |
| Duration of education (years) | 9.9 ± 5.0 | 10.6 ± 4.0 | 10.1 ± 5.1 |
| APOE ε4 genotype | 0/11 | 3/10 a | 12/29 b |
| MMSE | 27.5 ± 1.6 | 24.7 ± 2.5 a | 20.6 ± 4.6 b,c |
| CDR-SB | 0 | 2.0 ± 0.7 a | 4.6 ± 2.6 b,c |
| Intracranial Volume (cm3) | 1361 ± 134 | 1482 ± 140 | 1313 ± 106 c |
| Volume of hippocampus (cm3) | 4.66 ± 0.55 | 3.64 ± 0.91 a | 2.92 ± 0.80 b,c |
| 18FBB SUVR for global cortex | 1.39 ± 0.10 | 1.91 ± 0.45 a | 1.86 ± 0.35 b |
| CA1 | CA2–3 | CA4-DG | SRLM | SUBICULUM | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | p | R | p | R | p | R | p | R | p | |
| Global cortex | −0.186 | 0.195 | −0.218 | 0.129 | −0.393 | 0.005 | −0.459 | 0.001 | 0.012 | 0.934 |
| Prefrontal | −0.173 | 0.228 | −0.238 | 0.097 | −0.405 | 0.004 | −0.455 | 0.001 | 0.006 | 0.967 |
| Sensorimotor | −0.120 | 0.408 | −0.207 | 0.150 | −0.333 | 0.018 | −0.379 | 0.007 | 0.054 | 0.710 |
| Superior parietal | −0.197 | 0.171 | −0.235 | 0.101 | −0.392 | 0.005 | −0.446 | 0.001 | 0.008 | 0.957 |
| Inferior parietal | −0.253 | 0.077 | −0.269 | 0.059 | −0.435 | 0.002 | −0.499 | <0.001 | −0.035 | 0.812 |
| Precuneus | −0.203 | 0.157 | −0.232 | 0.105 | −0.409 | 0.003 | −0.480 | <0.001 | 0.030 | 0.836 |
| Occipital | −0.216 | 0.132 | −0.119 | 0.409 | −0.337 | 0.017 | −0.379 | 0.007 | −0.085 | 0.558 |
| Superior temporal | −0.181 | 0.207 | −0.200 | 0.164 | −0.354 | 0.012 | −0.456 | 0.001 | 0.056 | 0.701 |
| Middle temporal | −0.216 | 0.131 | −0.235 | 0.100 | −0.409 | 0.003 | −0.485 | <0.001 | 0.050 | 0.731 |
| Inferior temporal | −0.246 | 0.085 | −0.208 | 0.147 | −0.402 | 0.004 | −0.495 | <0.001 | 0.011 | 0.940 |
| Entorhinal | 0.174 | 0.226 | 0.171 | 0.235 | −0.012 | 0.932 | −0.124 | 0.390 | 0.215 | 0.134 |
| Parahippocampal | 0.058 | 0.688 | −0.007 | 0.962 | −0.164 | 0.254 | −0.274 | 0.054 | 0.186 | 0.197 |
| Amygdala | 0.103 | 0.475 | 0.175 | 0.223 | −0.011 | 0.938 | −0.130 | 0.369 | 0.028 | 0.846 |
| Anterior cingulate | −0.103 | 0.475 | −0.168 | 0.243 | −0.329 | 0.020 | −0.413 | 0.003 | 0.054 | 0.708 |
| Posterior cingulate | −0.149 | 0.303 | −0.158 | 0.274 | −0.368 | 0.009 | −0.451 | 0.001 | 0.029 | 0.839 |
| Insula | −0.127 | 0.381 | −0.172 | 0.232 | −0.326 | 0.021 | −0.411 | 0.003 | 0.037 | 0.797 |
| CA1 | CA2-3 | CA4-DG | SRLM | SUBICULUM | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B (SE) | p | B (SE) | p | B (SE) | p | B (SE) | p | B (SE) | p | |
| Age | −0.011 (0.005) | 0.036 | −0.004 (0.002) | 0.050 | −0.013 (0.005) | 0.010 | −0.011 (0.004) | 0.007 | −0.002 (0.003) | 0.594 |
| Female | −0.090 (0.089) | 0.320 | −0.012 (0.033) | 0.710 | 0.002 (0.083) | 0.983 | −0.021 (0.069) | 0.761 | −0.087 (0.052) | 0.107 |
| APOE4 | −0.193 (0.086) | 0.033 | −0.009 (0.032) | 0.786 | −0.034 (0.080) | 0.675 | −0.049 (0.066) | 0.468 | −0.080 (0.051) | 0.125 |
| Education | 0.004 (0.010) | 0.700 | −0.004 (0.004) | 0.266 | −0.008 (0.009) | 0.383 | −0.003 (0.008) | 0.716 | 0.003 (0.006) | 0.564 |
| MMSE | 0.030 (0.010) | 0.005 | 0.011 (0.004) | 0.005 | 0.032 (0.009) | 0.002 | 0.023 (0.007) | 0.004 | 0.010 (0.006) | 0.088 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, M.S.; Lee, N.; Kim, J.W.; Hong, J.Y. Association of Hippocampal Subfield Volumes with Amyloid-Beta Deposition in Alzheimer’s Disease. J. Clin. Med. 2022, 11, 1526. https://doi.org/10.3390/jcm11061526
Baek MS, Lee N, Kim JW, Hong JY. Association of Hippocampal Subfield Volumes with Amyloid-Beta Deposition in Alzheimer’s Disease. Journal of Clinical Medicine. 2022; 11(6):1526. https://doi.org/10.3390/jcm11061526
Chicago/Turabian StyleBaek, Min Seok, Narae Lee, Jin Woo Kim, and Jin Yong Hong. 2022. "Association of Hippocampal Subfield Volumes with Amyloid-Beta Deposition in Alzheimer’s Disease" Journal of Clinical Medicine 11, no. 6: 1526. https://doi.org/10.3390/jcm11061526
APA StyleBaek, M. S., Lee, N., Kim, J. W., & Hong, J. Y. (2022). Association of Hippocampal Subfield Volumes with Amyloid-Beta Deposition in Alzheimer’s Disease. Journal of Clinical Medicine, 11(6), 1526. https://doi.org/10.3390/jcm11061526