
Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratios in Preoperative Differential Diagnosis of Benign, Borderline, and Malignant Ovarian Tumors


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Menon, U.; Gentry-Maharaj, A.; Burnell, M.; Singh, N.; Ryan, A.; Karpinskyj, C.; Carlino, G.; Taylor, J.; Massingham, S.K.; Raikou, M.; et al. Ovarian cancer population screening and mortality after long-term follow-up in the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS): A randomised controlled trial. Lancet 2021, 397, 2182–2193. [Google Scholar] [CrossRef]
- Alcázar, J.L.; Galán, M.J.; Ceamanos, C.; García-Manero, M. Transvaginal Gray Scale and Color Doppler Sonography in Primary Ovarian Cancer and Metastatic Tumors to the Ovary. J. Ultrasound Med. 2003, 22, 243–247. [Google Scholar] [CrossRef]
- Valentin, L.; Ameye, L.; Testa, A.; Lécuru, F.; Bernard, J.-P.; Paladini, D.; Van Huffel, S.; Timmerman, D. Ultrasound characteristics of different types of adnexal malignancies. Gynecol. Oncol. 2006, 102, 41–48. [Google Scholar] [CrossRef]
- Canney, P.A.; Moore, M.; Wilkinson, P.M.; James, R.D. Ovarian cancer antigen CA125: A prospective clinical assessment of its role as a tumour marker. Br. J. Cancer 1984, 50, 765–769. [Google Scholar] [CrossRef]
- Spigel, S.C.; Mooney, L.R. Extreme thrombocytosis associated with malignancy. Cancer 1977, 39, 339–341. [Google Scholar] [CrossRef]
- Giannakeas, V.; Narod, S.A. Incidence of Cancer Among Adults With Thrombocytosis in Ontario, Canada. JAMA Netw. Open 2021, 4, e2120633. [Google Scholar] [CrossRef]
- Yoshida, A.; Sarian, L.O.; Marangoni, M.; Firmano, I.C.; Derchain, S.F. Diagnostic Value of the Neutrophil/Lymphocyte Ratio, Platelet/Lymphocyte Ratio, and Thrombocytosis in the Preoperative Investigation of Ovarian Masses. Rev. Bras. Ginecol. Obstet. 2020, 42, 397–403. [Google Scholar] [CrossRef]
- Yilmaz, E.; Coskun, E.I.; Sahin, N.; Ciplak, B.; Ekici, K. MPV, NLR, and platelet count: New hematologic markers in diagnosis of malignant ovarian tumor. Eur. J. Gynaecol. Oncol. 2017, 38, 346–349. [Google Scholar]
- Yildirim, M.A.; Seckin, K.D.; Togrul, C.; Baser, E.; Karsli, M.F.; Gungor, T.; Gulerman, H.C. Roles of Neutrophil/Lymphocyte and Platelet/Lymphocyte Ratios in the Early Diagnosis of Malignant Ovarian Masses. Asian Pac. J. Cancer Prev. 2014, 15, 6881–6885. [Google Scholar] [CrossRef][Green Version]
- Yildirim, M.; Cendek, B.D.; Avsar, A.F. Differentiation between benign and malignant ovarian masses in the preoperative period using neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios. Mol. Clin. Oncol. 2014, 3, 317–321. [Google Scholar] [CrossRef]
- Topcu, H.O.; Guzel, A.I.; Ozer, I.; Kokanali, M.K.; Gokturk, U.; Muftuoglu, K.H.; Doganay, M. Comparison of Neutrophil/Lymphocyte and Platelet/Lymphocyte Ratios for Predicting Malignant Potential of Suspicious Ovarian Masses in Gynecology Practice. Asian Pac. J. Cancer Prev. 2014, 15, 6239–6241. [Google Scholar] [CrossRef]
- Seckin, K.D.; Karslı, M.F.; Yucel, B.; Bestel, M.; Yıldırım, D.; Canaz, E.; Akbayır, O. The utility of tumor markers and neutrophil lymphocyte ratio in patients with an intraoperative diagnosis of mucinous borderline ovarian tumor. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 196, 60–63. [Google Scholar] [CrossRef]
- Polat, M.; Senol, T.; Ozkaya, E.; Pakay, G.O.; Cikman, M.S.; Konukcu, B.; Ozten, M.A.; Karateke, A. Neutrophil to lymphocyte and platelet to lymphocyte ratios increase in ovarian tumors in the presence of frank stromal invasion. Clin. Transl. Oncol. 2015, 18, 457–463. [Google Scholar] [CrossRef]
- Ozaksit, G.; Tokmak, A.; Kalkan, H.; Yesilyurt, H. Value of the Platelet to Lymphocyte Ratio in the Diagnosis of Ovarian Neoplasms in Adolescents. Asian Pac. J. Cancer Prev. 2015, 16, 2037–2041. [Google Scholar] [CrossRef]
- Bakacak, M.; Serin, S.; Ercan, O.; Kostu, B.; Bostancı, M.S.; Bakacak, Z.; Kıran, H.; Kıran, G. Utility of preoperative neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios to distinguish malignant from benign ovarian masses. J. Turk. Gynecol. Assoc. 2016, 17, 21–25. [Google Scholar] [CrossRef]
- Badora-Rybicka, A.; Nowara, E.; Starzyczny-Słota, D. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio before chemotherapy as potential prognostic factors in patients with newly diagnosed epithelial ovarian cancer. ESMO Open 2016, 1, e000039. [Google Scholar] [CrossRef]
- Raungkaewmanee, S.; Tangjitgamol, S.; Manusirivithaya, S.; Srijaipracharoen, S.; Thavaramara, T. Platelet to lymphocyte ratio as a prognostic factor for epithelial ovarian cancer. J. Gynecol. Oncol. 2012, 23, 265–273. [Google Scholar] [CrossRef]
- Ashrafganjoei, T.; Mohamadianamiri, M.; Farzaneh, F.; Hosseini, M.S.; Arab, M. Investigating Preoperative Hematologic Markers for Prediction of Ovarian Cancer Surgical Outcome. Asian Pac. J. Cancer Prev. 2016, 17, 1445–1448. [Google Scholar] [CrossRef]
- Cho, H.; Hur, H.W.; Kim, S.W.; Kim, S.; Kim, J.H.; Kim, Y.T.; Lee, K. Pre-treatment neutrophil to lymphocyte ratio is elevated in epithelial ovarian cancer and predicts survival after treatment. Cancer Immunol. Immunother. 2008, 58, 15–23. [Google Scholar] [CrossRef]
- Kuplay, H.; Erdoğan, S.B.; Bastopcu, M.; Arslanhan, G.; Baykan, D.B.; Orhan, G. The neutrophil-lymphocyte ratio and the platelet-lymphocyte ratio correlate with thrombus burden in deep venous thrombosis. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 8, 360–364. [Google Scholar] [CrossRef]
- Meshaal, M.S.; Nagi, A.; El-Damaty, A.M.F.; Elnaggar, W.; Gaber, M.; Rizk, H. Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as independent predictors of outcome in infective endocarditis (IE). Egypt. Heart J. 2019, 71, 13. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mukanova, U.; Yessirkepov, M.; Kitas, G.D. The Platelet-to-Lymphocyte Ratio as an Inflammatory Marker in Rheumatic Diseases. Ann. Lab. Med. 2019, 39, 345–357. [Google Scholar] [CrossRef]
- Russell, C.D.; Parajuli, A.; Gale, H.J.; Bulteel, N.S.; Schuetz, P.; de Jager, C.P.; Loonen, A.J.; Merekoulias, G.I.; Baillie, J.K. The utility of peripheral blood leucocyte ratios as biomarkers in infectious diseases: A systematic review and meta-analysis. J. Infect. 2019, 78, 339–348. [Google Scholar] [CrossRef]
- Psomiadou, V.; Prodromidou, A.; Galati, E.; Kostakis, I.D.; Maliaros, A.; Mamais, I.; Blontzos, N.; Lefkopoulos, F.; Iavazzo, C.; Vorgias, G. The role of inflammation biomarkers in differential diagnosis of pelvic tumours of ovarian origin: A single-centre observational study. Contemp. Oncol. 2021, 25, 7–11. [Google Scholar] [CrossRef]
- Quirk, J.T.; Natarajan, N. Ovarian cancer incidence in the United States, 1992–1999. Gynecol. Oncol. 2005, 97, 519–523. [Google Scholar] [CrossRef]
- Mink, P.J.; Sherman, M.E.; Devesa, S.S. Incidence patterns of invasive and borderline ovarian tumors among white women and black women in the United States. Cancer 2002, 95, 2380–2389. [Google Scholar] [CrossRef]
- Demont, F.; Fourquet, F.; Rogers, M.; Lansac, J. Epidemiology of apparently benign ovarian cysts. J. Gynecol. Obstet. Biol. Reprod. 2001, 30, S8–S11. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Jaiswal, M.; LaRusso, N.F.; Gores, G.J. Nitric oxide in gastrointestinal epithelial cell carcinogenesis: Linking inflammation to oncogenesis. Am. J. Physiol. Liver Physiol. 2001, 281, G626–G634. [Google Scholar] [CrossRef]
- Todoric, J.; Antonucci, L.; Karin, M. Targeting Inflammation in Cancer Prevention and Therapy. Cancer Prev. Res. 2016, 9, 895–905. [Google Scholar] [CrossRef]
- Gregory, A.D.; Houghton, A.M. Tumor-Associated Neutrophils: New Targets for Cancer Therapy. Cancer Res. 2011, 71, 2411–2416. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.A.; Labidi-Galy, S.I.; Terry, K.L.; Vitonis, A.F.; Welch, W.R.; Goodman, A.; Cramer, D.W. Prognostic significance and predictors of the neutrophil-to-lymphocyte ratio in ovarian cancer. Gynecol. Oncol. 2014, 132, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Afshar-Kharghan, V.; Schafer, A.I. Paraneoplastic thrombocytosis: The secrets of tumor self-promotion. Blood 2014, 124, 184–187. [Google Scholar] [CrossRef]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupaimoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic Thrombocytosis in Ovarian Cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Takahashi, T.; Nakamura, K.; Tsuyuoka, R.; Okuno, Y.; Enomoto, T.; Fukumoto, M.; Imura, H. Thrombocytosis in patients with tumors producing colony-stimulating factor. Blood 1992, 80, 2052–2059. [Google Scholar] [CrossRef]
- de Jong, M.C.; Mihai, R.; Khan, S. Neutrophil-to-Lymphocyte Ratio (NLR) and Platelet-to-Lymphocyte Ratio (PLR) as Possible Prognostic Markers for Patients Undergoing Resection of Adrenocortical Carcinoma. World J. Surg. 2021, 45, 754–764. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Früh, M. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer 2017, 111, 176–181. [Google Scholar] [CrossRef]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Kokcu, A.; Kurtoglu, E.; Celik, H.; Tosun, M.; Malatyalioglu, E.; Ozdemir, A.Z. May the platelet to lymphocyte ratio be a prognostic factor for epithelial ovarian cancer? Asian Pac. J. Cancer Prev. 2014, 15, 9781–9784. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, P.; Xu, Y.; Zhang, W.; Tong, L.; Guo, Z.; Ni, H. Preoperative neutrophil-to-lymphocyte ratio predicts response to first-line platinum-based chemotherapy and prognosis in serous ovarian cancer. Cancer Chemother. Pharmacol. 2014, 75, 255–262. [Google Scholar] [CrossRef]
- Nakamura, K.; Nagasaka, T.; Nishida, T.; Haruma, T.; Ogawa, C.; Kusumoto, T.; Seki, N.; Hiramatsu, Y. Neutrophil to lymphocyte ratio in the pre-treatment phase of final-line chemotherapy predicts the outcome of patients with recurrent ovarian cancer. Oncol. Lett. 2016, 11, 3975–3981. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Number of Patients |
|---|---|
| Benign ovarian tumor (n = 318) | |
| Histopathology Epithelial ovarian tumor (n = 200) | |
| Mucinous cystadenoma | 100 (31.4%) |
| Serous cystadenoma | 77 (24.2%) |
| Sero-mucinous cystadenoma | 15 (4.7%) |
| Mucinous cystadenofibroma | 2 (0.6%) |
| Serous cystadenofibroma | 3 (0.9%) |
| Sero-mucinous cystadenofibroma | 3 (0.9%) |
| Non-epithelial ovarian tumor (n = 118) | |
| Mature cystic teratoma | 99 (31.1%) |
| Fibroma | 10 (3.1%) |
| Fibrothecoma | 7 (2.2%) |
| Thecoma | 1 (0.3%) |
| Sclerosing stromal tumor | 1 (0.3%) |
| Borderline ovarian tumor (n = 108) | |
| Histopathology | |
| Mucinous borderline tumor | 83 (76.9%) |
| Serous borderline tumor | 19 (17.6%) |
| Sero-mucinous borderline tumor | 4 (3.7%) |
| Endometrioid borderline tumor | 2 (1.9%) |
| Malignant ovarian tumor (n = 204) | |
| Histopathology | |
| High-grade serous carcinoma | 71 (34.8%) |
| Endometrioid adenocarcinoma | 44 (21.6%) |
| Mucinous adenocarcinoma | 40 (19.6%) |
| Clear cell carcinoma | 25 (12.3%) |
| Mixed epithelial carcinoma | 8 (3.9%) |
| Low-grade serous carcinoma | 7 (3.4%) |
| Carcinosarcoma | 5 (2.5%) |
| Undifferentiated carcinoma | 3 (1.5%) |
| Sero-mucinous adenocarcinoma | 1 (0.5%) |
| Differentiation grade | |
| Grade 1 (well diff.) | 29 (14.2%) |
| Grade 2 (moderately diff.) | 93 (45.6%) |
| Grade 3 (poorly diff.) | 82 (40.2%) |
| Stage | |
| Stage I | |
| IA | 45 (22.1%) |
| IB | 5 (2.5%) |
| IC | 35 (17.2%) |
| Stage II | |
| IIA | 4 (2.0%) |
| IIB | 11 (5.4%) |
| IIC | 9 (4.4%) |
| Stage III | |
| IIIA | 3 (1.5%) |
| IIIB | 9 (4.4%) |
| IIIC | 68 (33.3%) |
| Stage IV | 15 (7.4%) |
| Pathology | Mean ± SD | p-Value (ANOVA) | Comparison between Groups a | p-Value (Post Hoc b) | |
|---|---|---|---|---|---|
| Age (n = 630) | Benign (n = 318) | 45.3 ± 16.5 | p < 0.001 | 1 vs. 2 | p = 0.487 |
| Borderline (n = 108) | 47.3 ± 17.2 | 1 vs. 3 | p < 0.001 | ||
| Malignant (n = 204) | 52.9 ± 12.0 | 2 vs. 3 | p = 0.010 | ||
| White blood cell (/µL) | Benign | 6831.4 ± 2529.2 | p = 0.007 | 1 vs. 2 | p = 0.966 |
| Borderline | 6760.2 ± 1946.2 | 1 vs. 3 | p = 0.014 | ||
| Malignant | 7470.6 ± 2517.8 | 2 vs. 3 | p = 0.050 | ||
| Hemoglobin (g/dL) | Benign | 12.7 ± 1.3 | p < 0.001 | 1 vs. 2 | p = 0.963 |
| Borderline | 12.8 ± 1.3 | 1 vs. 3 | p < 0.001 | ||
| Malignant | 12.0 ± 1.4 | 2 vs. 3 | p < 0.001 | ||
| Platelet count (/µL) | Benign | 256,323.9 ± 66,984.9 | p < 0.001 | 1 vs. 2 | p = 0.424 |
| Borderline | 245,027.8 ± 62,092.3 | 1 vs. 3 | p = 0.002 | ||
| Malignant | 280,828.4 ± 97,239.9 | 2 vs. 3 | p = 0.001 | ||
| Neutrophil count (/µL) | Benign | 4192.8 ± 2319.7 | p < 0.001 | 1 vs. 2 | p = 0.886 |
| Borderline | 4317.9 ± 1753.7 | 1 vs. 3 | p < 0.001 | ||
| Malignant | 5156.5 ± 2464.1 | 2 vs. 3 | p = 0.009 | ||
| Lymphocyte count (/µL) | Benign | 1992.0 ± 647.0 | p < 0.001 | 1 vs. 2 | p = 0.227 |
| Borderline | 1868.5 ± 615.2 | 1 vs. 3 | p < 0.001 | ||
| Malignant | 1660.5 ± 651.2 | 2 vs. 3 | p = 0.025 | ||
| NLR | Benign | 2.4 ± 2.2 | p < 0.001 | 1 vs. 2 | p = 0.648 |
| Borderline | 2.7 ± 2.5 | 1 vs. 3 | p < 0.001 | ||
| Malignant | 3.9 ± 3.4 | 2 vs. 3 | p = 0.002 | ||
| PLR | Benign | 141.8 ± 62.0 | p < 0.001 | 1 vs. 2 | p = 0.850 |
| Borderline | 146.9 ± 80.2 | 1 vs. 3 | p < 0.001 | ||
| Malignant | 194.8 ± 104.2 | 2 vs. 3 | p < 0.001 |
| Cut-Off | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|
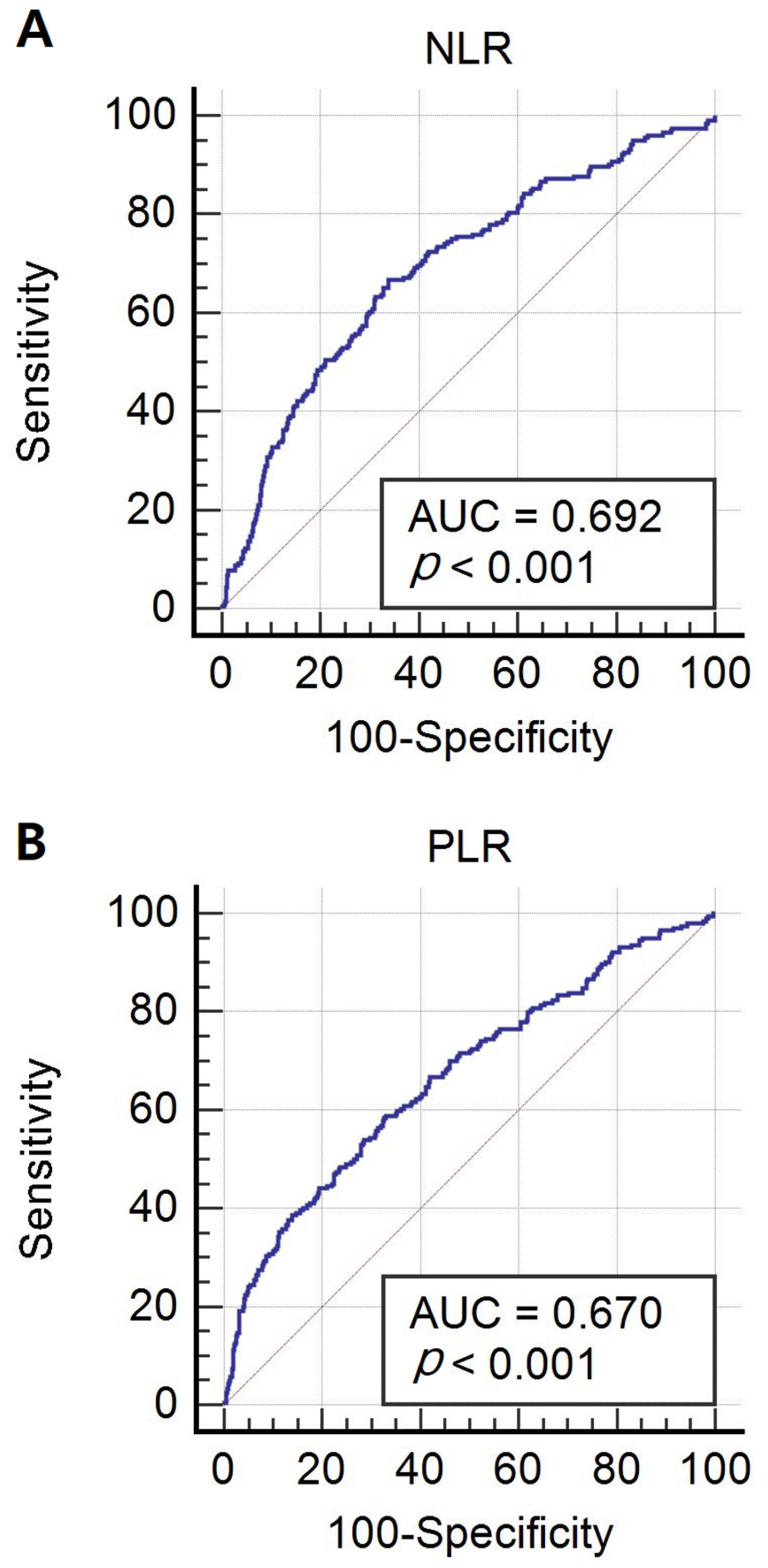
| NLR Benign or borderline vs. malignancy | 2.36 | 66.7 | 66.2 |
| PLR Benign or borderline vs. malignancy | 150.02 | 58.8 | 66.9 |
| Odds Ratio a | 95% CI | p-Value | |
|---|---|---|---|
| NLR ≥ 2.4 Malignancy vs. Benign or borderline | 3.796 | 2.667–5.403 | p < 0.001 |
| PLR ≥ 150.0 Malignancy vs. Benign or borderline | 2.857 | 2.026–4.030 | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, T.H.; Jeong, Y.Y.; Lee, S.J.; Choi, Y.S.; Ryu, J.M. Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratios in Preoperative Differential Diagnosis of Benign, Borderline, and Malignant Ovarian Tumors. J. Clin. Med. 2022, 11, 1355. https://doi.org/10.3390/jcm11051355
Yun TH, Jeong YY, Lee SJ, Choi YS, Ryu JM. Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratios in Preoperative Differential Diagnosis of Benign, Borderline, and Malignant Ovarian Tumors. Journal of Clinical Medicine. 2022; 11(5):1355. https://doi.org/10.3390/jcm11051355
Chicago/Turabian StyleYun, Tae Hui, Yoon Young Jeong, Sun Jae Lee, Youn Seok Choi, and Jung Min Ryu. 2022. "Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratios in Preoperative Differential Diagnosis of Benign, Borderline, and Malignant Ovarian Tumors" Journal of Clinical Medicine 11, no. 5: 1355. https://doi.org/10.3390/jcm11051355
APA StyleYun, T. H., Jeong, Y. Y., Lee, S. J., Choi, Y. S., & Ryu, J. M. (2022). Neutrophil–Lymphocyte and Platelet–Lymphocyte Ratios in Preoperative Differential Diagnosis of Benign, Borderline, and Malignant Ovarian Tumors. Journal of Clinical Medicine, 11(5), 1355. https://doi.org/10.3390/jcm11051355