
IL-1β Implications in Type 1 Diabetes Mellitus Progression: Systematic Review and Meta-Analysis


 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Protocol
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection Process
2.5. Data Extraction
2.6. Evaluation of Quality and Risk of Bias
2.7. Statistical Analysis
3. Results
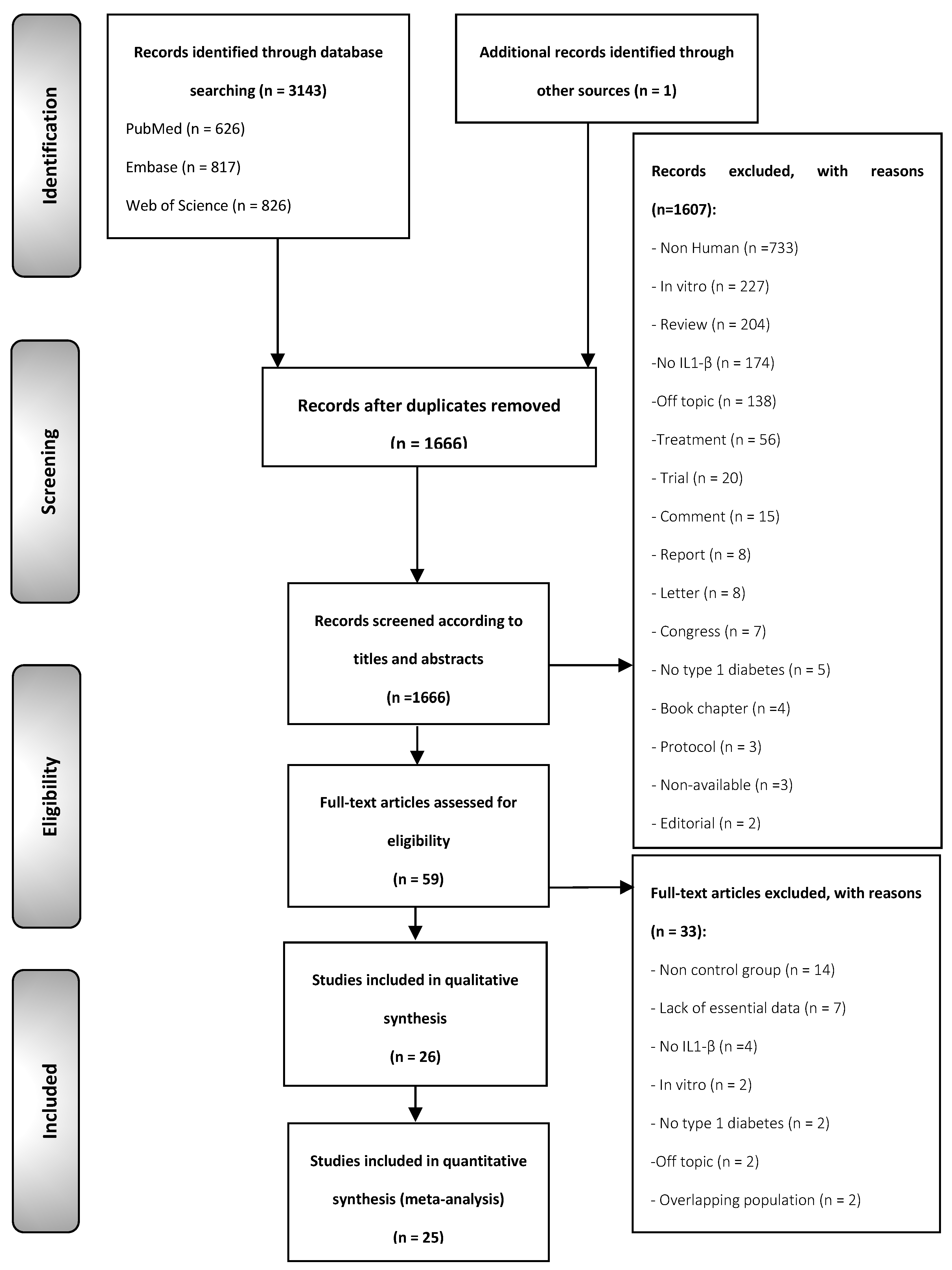
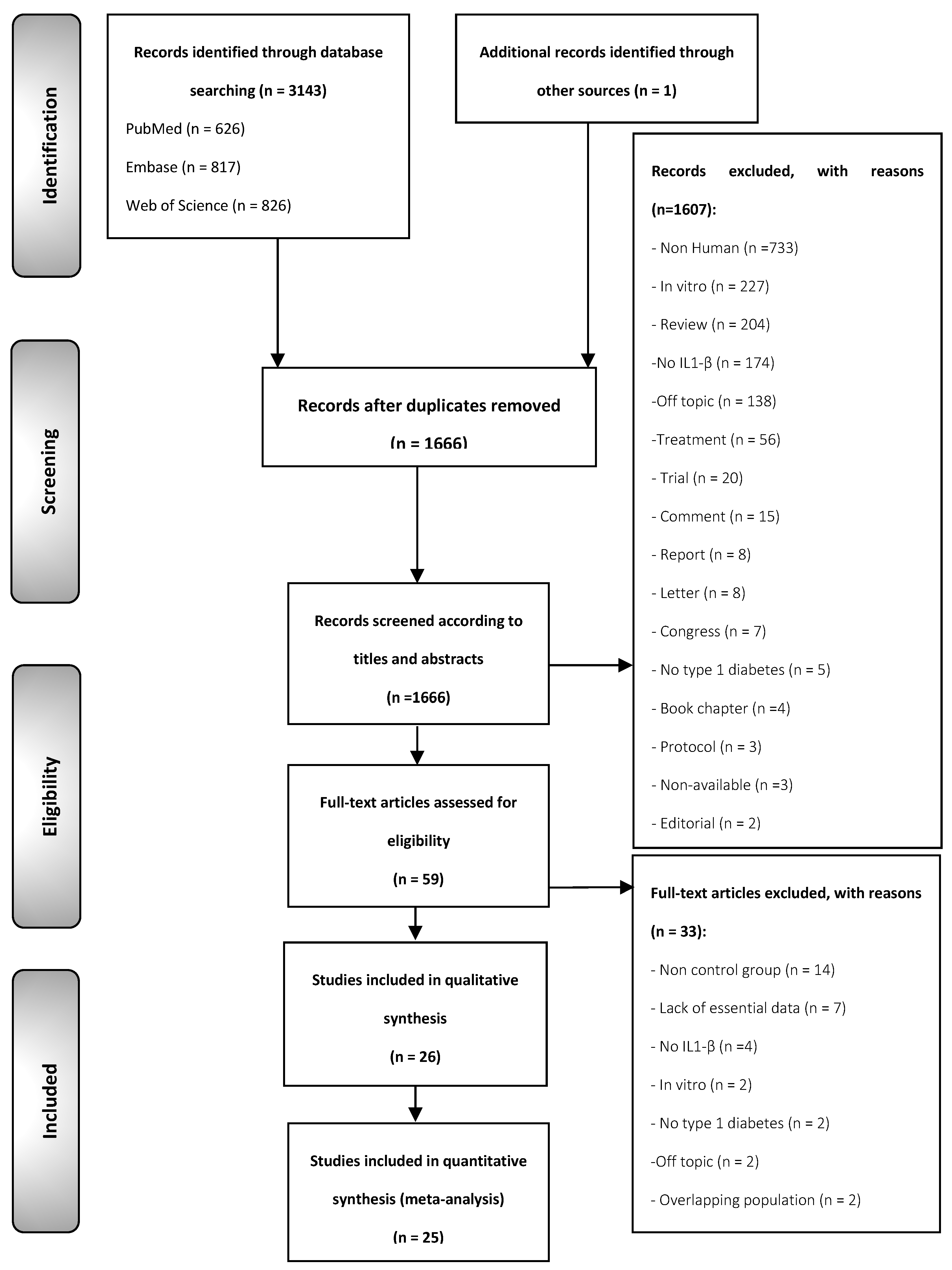
3.1. Results of the Literature Search
3.2. Study Characteristics
3.3. Qualitative Evaluation
3.4. Quantitative Evaluation (Meta-Analysis)
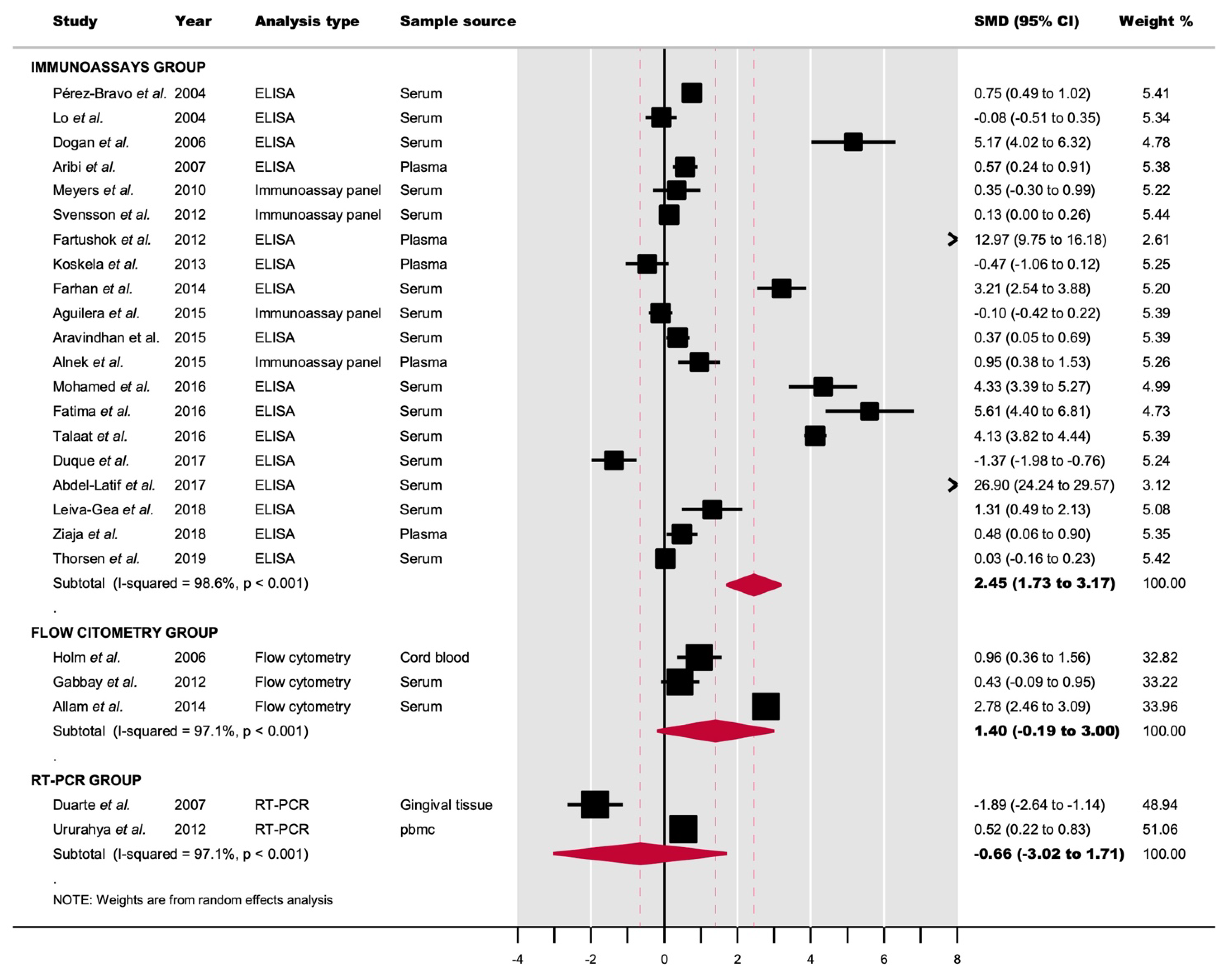
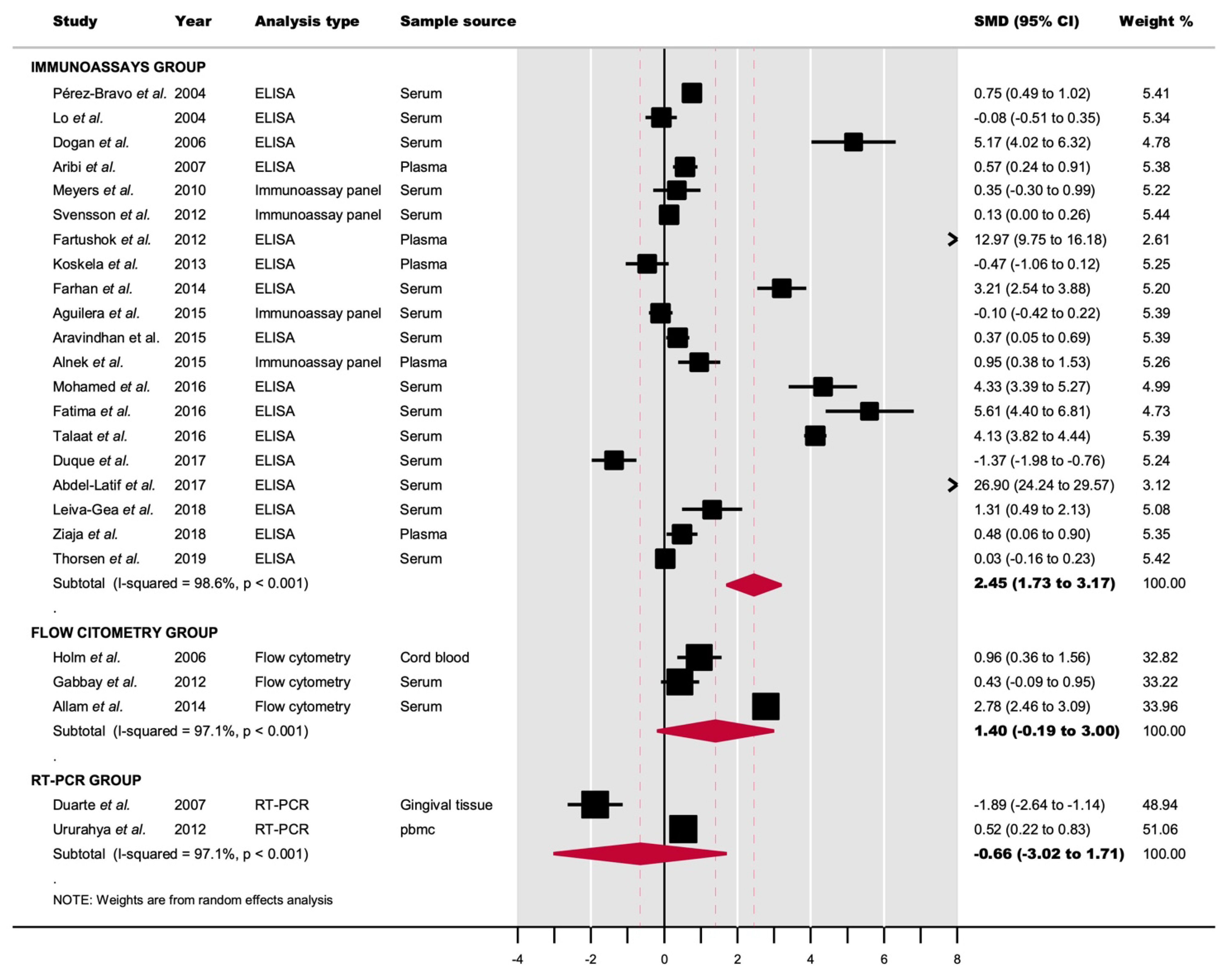
3.4.1. IL-1β Determination by Immunoassays
3.4.2. IL-1β Level Determination by Flow Cytometry
3.4.3. IL-1β mRNA Level Determination by qRT-PCR
3.4.4. Analysis of Subgroups
3.4.5. Meta-Regression
3.5. Quantitative Evaluation (Secondary Analyses)
3.5.1. Sensitivity Analysis
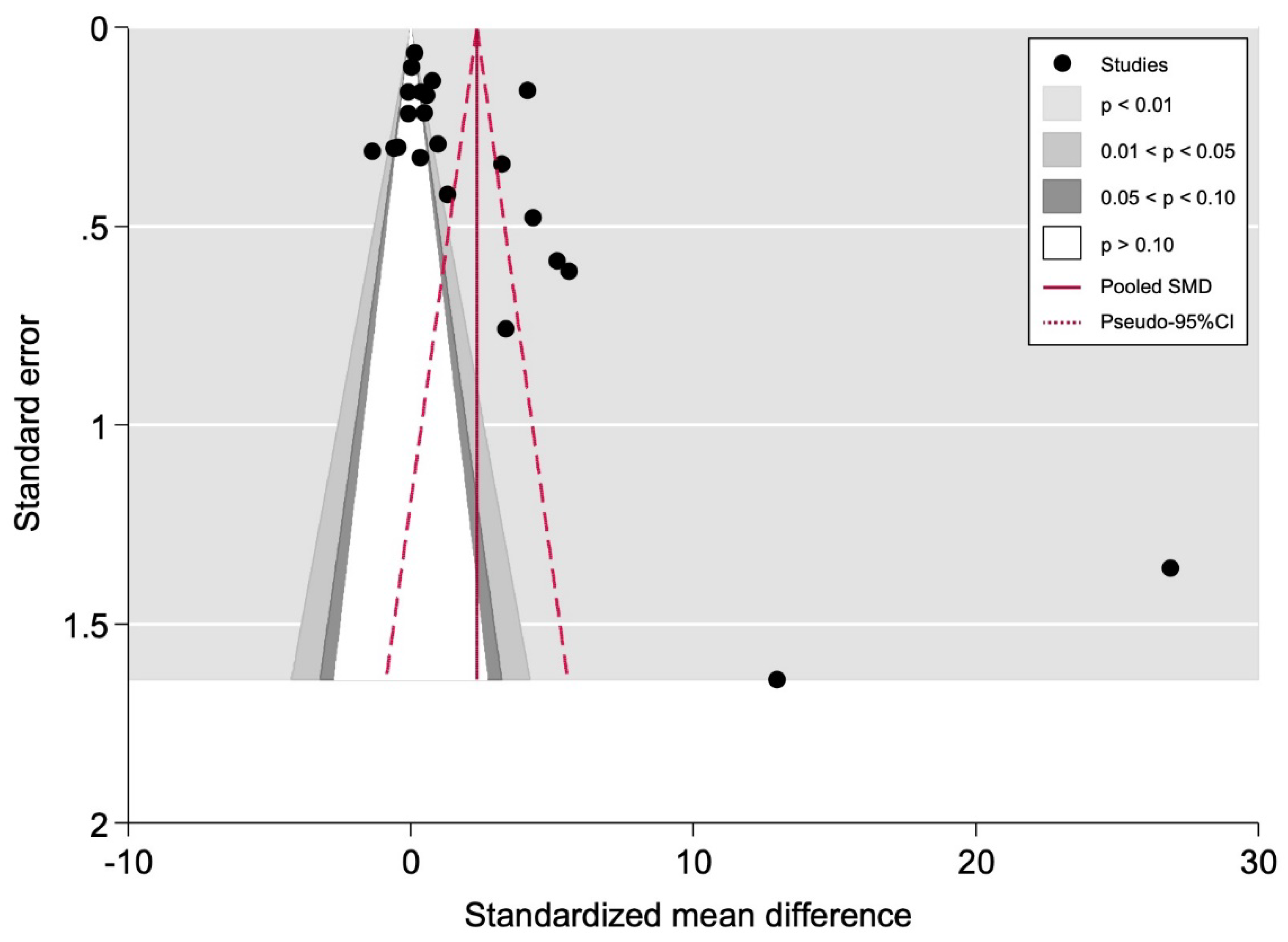
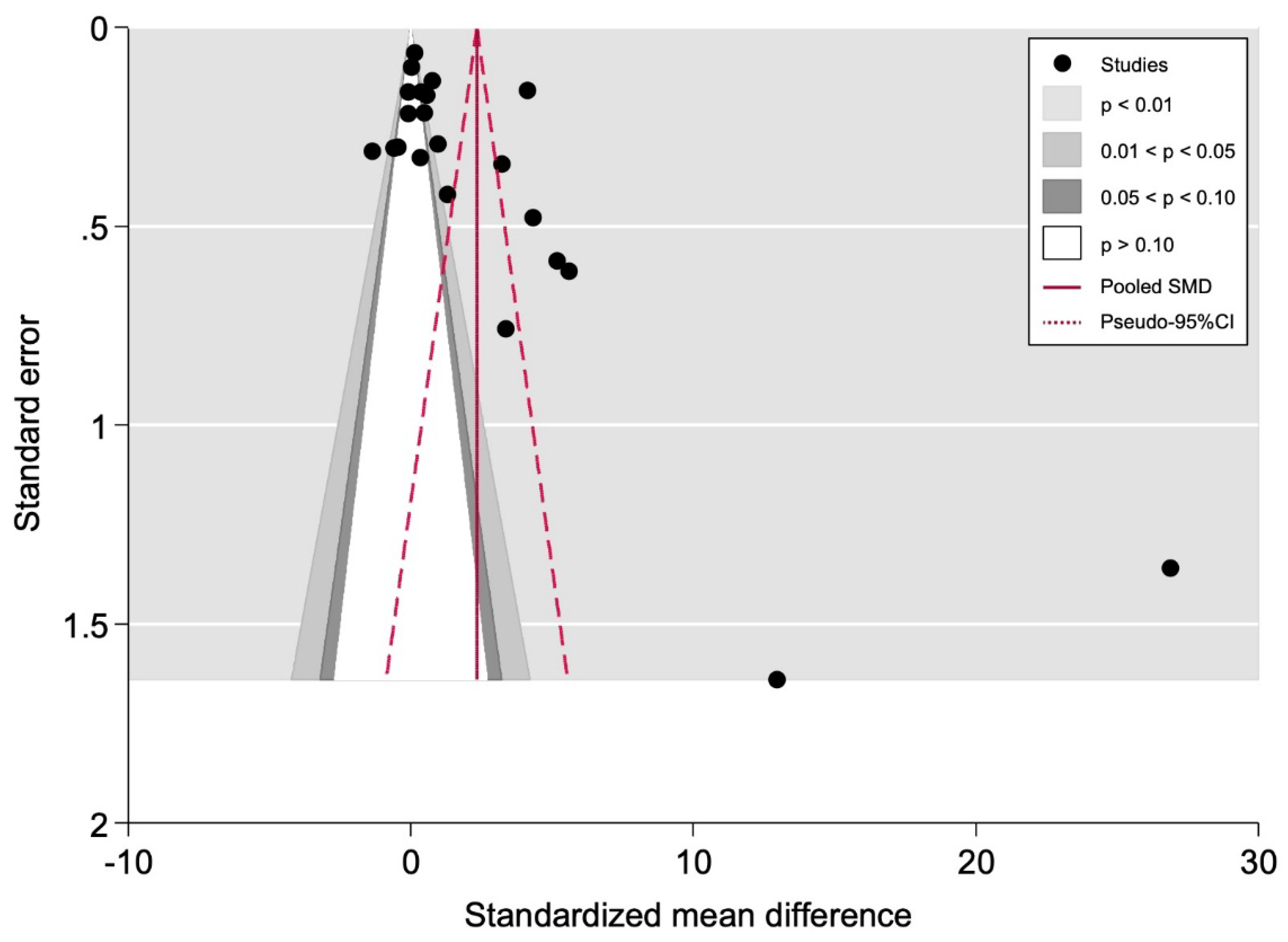
3.5.2. Small-Study Effects Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eizirik, D.L.; Colli, M.L.; Ortis, F. The role of inflammation in insulitis and Β-cell loss in type 1 diabetes. Nat. Rev. Endocrinol. 2009, 5, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Vaarala, O. Is the origin of type 1 diabetes in the gut? Immunol. Cell Biol. 2012, 90, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Uno, S.; Imagawa, A.; Okita, K.; Sayama, K.; Moriwaki, M.; Iwahashi, H.; Yamagata, K.; Tamura, S.; Matsuzawa, Y.; Hanafusa, T.; et al. Macrophages and dendritic cells infiltrating islets with or without beta cells produce tumour necrosis factor-α in patients with recent-onset type 1 diabetes. Diabetologia 2007, 50, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Donath, M.Y.; Dinarello, C.A.; Mandrup-Poulsen, T. Targeting innate immune mediators in type 1 and type 2 diabetes. Nat. Rev. Immunol. 2019, 19, 734–746. [Google Scholar] [CrossRef] [PubMed]
- Pankewycz, O.G.; Guan, J.-X.; Benedict, J.F. Cytokines as Mediators of Autoimmune Diabetes and Diabetic Complications. Endocr. Rev. 1995, 16, 164–176. [Google Scholar] [CrossRef]
- Singh, B.; Nikoopour, E.; Huszarik, K.; Elliott, J.F.; Jevnikar, A.M. Immunomodulation and regeneration of islet beta cells by cytokines in autoimmune type 1 diabetes. J. Interf. Cytokine Res. 2011, 31, 711–719. [Google Scholar] [CrossRef]
- Mandrup-Poulsen, T.; Pickersgill, L.; Donath, M.Y. Blockade of interleukin 1 in type 1 diabetes mellitus. Nat. Rev. Endocrinol. 2010, 6, 158–166. [Google Scholar] [CrossRef]
- Mohammadoo-Khorasani, M.; Salimi, S.; Tabatabai, E.; Sandoughi, M.; Zakeri, Z.; Farajian-Mashhadi, F. Interleukin-1β (IL-1β) & IL-4 gene polymorphisms in patients with systemic lupus erythematosus (SLE) & their association with susceptibility to SLE. Indian J. Med. Res. 2016, 143, 591–596. [Google Scholar] [CrossRef]
- Hu, S.L.; Huang, C.C.; Tseng, T.T.; Liu, S.C.; Tsai, C.H.; Fong, Y.C.; Tang, C.H. S1P facilitates IL-1β production in osteoblasts via the JAK and STAT3 signaling pathways. Environ. Toxicol. 2020, 35, 991–997. [Google Scholar] [CrossRef]
- Malhotra, S.; Costa, C.; Eixarch, H.; Keller, C.W.; Amman, L.; Martínez-Banaclocha, H.; Midaglia, L.; Sarró, E.; Machín-Díaz, I.; Villar, L.M.; et al. NLRP3 inflammasome as prognostic factor and therapeutic target in primary progressive multiple sclerosis patients. Brain 2020, 143, 1414–1430. [Google Scholar] [CrossRef]
- Moran, A.; Bundy, B.; Becker, D.J.; DiMeglio, L.A.; Gitelman, S.E.; Goland, R.; Greenbaum, C.J.; Herold, K.C.; Marks, J.B.; Raskin, P.; et al. Interleukin-1 antagonism in type 1 diabetes of recent onset: Two multicentre, randomised, double-blind, placebo-controlled trials. Lancet 2013, 381, 1905–1915. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.L.; Qiao, Y.C.; Pan, Y.H.; Xu, Y.; Huang, Y.C.; Wang, Y.H.; Geng, L.J.; Zhao, H.L.; Zhang, X.X. Correlation between serum interleukin-6 level and type 1 diabetes mellitus: A systematic review and meta-analysis. Cytokine 2017, 94, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.C.; Chen, Y.L.; Pan, Y.H.; Tian, F.; Xu, Y.; Zhang, X.; Zhao, H.L. The change of serum tumor necrosis factor alpha in patients with type 1 diabetes mellitus: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0176157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. J. Am. Med. Assoc. 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Welch, V.; Tugwell, P.; Petticrew, M.; de Montigny, J.; Ueffing, E.; Kristjansson, B.; McGowan, J.; Benkhalti Jandu, M.; Wells, G.A.; Brand, K.; et al. How effects on health equity are assessed in systematic reviews of interventions. Cochrane Database Syst. Rev. 2010, 2010, MR000028. [Google Scholar] [CrossRef] [Green Version]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, S.G.; Higgins, J.P.T. How should meta-regression analyses be undertaken and interpreted? Stat. Med. 2002, 21, 1559–1573. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. A non-parametric “trim and fill” method of assessing publication bias in meta-analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Palmer, T.M.; Sterne, J.A.C. Meta-Analysis in Stata: An Updated Collection from the Stata Journal, 2nd ed.; Stata Press: College Station, TX, USA, 2016. [Google Scholar]
- Thorsen, S.U.; Pipper, C.B.; Ellervik, C.; Pociot, F.; Kyvsgaard, J.N.; Svensson, J. Association between neonatal whole blood iron content and cytokines, adipokines, and other immune response proteins. Nutrients 2019, 11, 543. [Google Scholar] [CrossRef] [Green Version]
- Koskela, U.E.; Kuusisto, S.M.; Nissinen, A.E.; Savolainen, M.J.; Liinamaa, M.J. High vitreous concentration of IL-6 and IL-8, but not of adhesion molecules in relation to plasma concentrations in proliferative diabetic retinopathy. Ophthalmic Res. 2013, 49, 108–114. [Google Scholar] [CrossRef]
- Mateo-Gavira, I.; Vílchez-López, F.J.; García-Palacios, M.V.; Carral-San Laureano, F.; Visiedo-García, F.M.; Aguilar-Diosdado, M. Early blood pressure alterations are associated with pro-inflammatory markers in type 1 diabetes mellitus. J. Hum. Hypertens. 2017, 31, 151–156. [Google Scholar] [CrossRef]
- Zorena, K.; Raczyńska, D.; Raczyńska, K. Biomarkers in diabetic retinopathy and the therapeutic implications. Mediat. Inflamm. 2013, 2013, 193604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AboElAsrar, M.A.; Elbarbary, N.S.; Elshennawy, D.E.; Omar, A.M. Insulin-like growth factor-1 cytokines cross-talk in type 1 diabetes mellitus: Relationship to microvascular complications and bone mineral density. Cytokine 2012, 59, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Sawires, H.; Botrous, O.; Aboulmagd, A.; Madani, N.; Abdelhaleem, O. Transforming growth factor-β1 in children with diabetic nephropathy. Pediatr. Nephrol. 2019, 34, 81–85. [Google Scholar] [CrossRef]
- Wołoszyn-Durkiewicz, A.; Myśliwiec, M. The prognostic value of inflammatory and vascular endothelial dysfunction biomarkers in microvascular and macrovascular complications in type 1 diabetes. Pediatr. Endocrinol. Diabetes Metab. 2019, 25, 28–35. [Google Scholar] [CrossRef]
- Alexandraki, K.I.; Piperi, C.; Ziakas, P.D.; Apostolopoulos, N.V.; Makrilakis, K.; Syriou, V.; Diamanti-Kandarakis, E.; Kaltsas, G.; Kalofoutis, A. Cytokine secretion in long-standing diabetes mellitus type 1 and 2: Associations with low-grade systemic inflammation. J. Clin. Immunol. 2008, 28, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Li, H.Y.; Zhong, H.; Zhong, Z. Relationship between transforming growth factor-β1 and type 2 diabetic nephropathy risk in Chinese population. BMC Med. Genet. 2018, 19, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crinò, A.; Schiaffini, R.; Manfrini, S.; Mesturino, C.; Visalli, N.; Beretta Anguissola, G.; Suraci, C.; Pitocco, D.; Spera, S.; Corbi, S.; et al. A randomized trial of nicotinamide and vitamin E in children with recent onset type 1 diabetes (IMDIAB IX) Pozzillion behalf of the IMDIAB group. Eur. J. Endocrinol. 2004, 150, 719–724. [Google Scholar] [CrossRef] [Green Version]
- Cabrera, S.M.; Wang, X.; Chen, Y.G.; Jia, S.; Kaldunski, M.L.; Greenbaum, C.J.; Mandrup-Poulsen, T.; Hessner, M.J. Interleukin-1 antagonism moderates the inflammatory state associated with Type 1 diabetes during clinical trials conducted at disease onset. Eur. J. Immunol. 2016, 46, 1030–1046. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, F. Myostatin alters with exercise training in diabetic rats; possible interaction with glycosylated hemoglobin and inflammatory cytokines. Cytokine 2019, 120, 99–106. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Greenland, S. Can meta-analysis be salvaged? Am. J. Epidemiol. 1994, 140, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Lin, L. Bias caused by sampling error in meta-analysis with small sample sizes. PLoS ONE 2018, 13, e0204056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, J.H. Interleukin-1β induces pericyte apoptosis via the NF-κB pathway in diabetic retinopathy. Biochem. Biophys. Res. Commun. 2021, 546, 46–53. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Total | 26 studies * |
| Year of publication | 2004–2019 |
| Number of patients | |
| Total | 4179 patients * |
| Cases with T1DM | 2186 patients |
| Controls | 2047 patients |
| Sample size, range | 18–961 patients |
| IL-1β determination | |
| Immunoassays | 22 studies (18 by ELISA, 4 by panels) |
| Flow cytometry | 3 studies |
| qRT-PCR | 2 studies |
| Source of samples | |
| Serum | 17 studies |
| Plasma | 5 studies |
| Gingival crevicular fluid | 1 study |
| Vitreus humour | 1 study |
| Cord blood plasma | 1 study |
| Gingival tissue | 1 study |
| Peripheral blood leukocytes | 1 study |
| Geographical region | |
| Europe | 12 studies |
| Asia | 6 studies |
| South America | 5 studies |
| Africa | 3 study |
| North America | 1 study |
| Study | Selection | Control | Outcomes | Overall Quality | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativ eness of the T1DM patients | Selection of the non-T1DM subjects | Properly IL1b quantification | Glycemic control | Control of confounding factors | Assessment of T1DM progression | Appropriate follow up period | Adequacy of follow up | ||
| Pérez-Bravo et al. (2004) |  | | | | |  | | | High |
| Lo et al. (2004) |  | | | | |  | | | High |
| Holm et al. (2006) | | | | | | | | | High |
| Dogan et al. (2006) | | | | | | | | | High |
| Arabi et al. (2007) | | | | | | | | | High |
| Duarte et al. (2007) | | | | | | | | | High |
| Salvi et al. (2010) | | | | | | | | | High |
| Meyers et al. (2010) | | | | | | | | | High |
| Gabbay et al. (2012) | | | | | | | | | Moderate |
| Svensson et al. (2012) | | | | | | | | | High |
| Ururahy et al. (2012) | | | | | | | | | High |
| Fartushok et al. (2012) | | | | | | | | | High |
| Koskela et al. (2013) | | | | | | | | | High |
| Allam et al. (2014) | | | | | | | | | High |
| Farhan et al. (2014) | | | | | | | | | Moderate |
| Aguilera et al. (2015) | | | | | | | | | High |
| Aravindhan et al. (2015) | | | | | | | | | Moderate |
| Alnek et al. (2015) | | | | | | | | | High |
| Mohamed et al. (2016) | | | | | | | | | High |
| Fatima et al. (2016) | | | | | | | | | Moderate |
| Talaat et al. (2016) | | | | | | | | | High |
| Duque et al. (2017) | | | | | | | | | Moderate |
| Abdel-Latif et al. (2017) | | | | | | | | | High |
| Leiva-Gea et al. (2018) | | | | | | | | | High |
| Ziaja et al. (2018) | | | | | | | | | Moderate |
| Thorsen et al. (2019) | | | | | | | | | High |
| Pooled Data | Heterogeneity | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Meta-Analyses | No. of Studies | No. of Patients | Stat. Model | Wt | SMD (95% CI) | p-Value | Phet | I2 (%) | Supplementary Materialsa |
| Determination by immunoassays | |||||||||
| All b | 20 | 3490 | REM | D-L | 2.45 (1.73 to 3.17) | <0.001 | <0.001 | 98.6 | —— |
| Subgroup analysis by geographical area c | Figure S1, p. 11 | ||||||||
| Africa | 3 | 403 | REM | D-L | 10.41 (2.58 to 18.23) | 0.01 | <0.001 | 99.5 | |
| Asia | 5 | 885 | REM | D-L | 2.61 (0.56 to 4.66) | 0.01 | <0.001 | 99.0 | |
| Europe | 9 | 1875 | REM | D-L | 1.04 (0.49 to 1.59) | <0.001 | <0.001 | 95.0 | |
| North America | 1 | 38 | —— | —— | 0.35 (−0.30 to 0.99) | 0.29 | —— | —— | |
| South America | 2 | 289 | REM | D-L | −0.29 (−2.37 to 1.79) | 0.78 | < 0.001 | 97.4 | |
| Subgroup analysis by age c | Figure S2, p. 12 | ||||||||
| <18 years old | 14 | 2870 | REM | D-L | 2.81 (1.88 to 3.74) | <0.001 | <0.001 | 98.9 | |
| >18 years old | 6 | 620 | REM | D-L | 1.56 (0.48 to 2.65) | 0.002 | <0.001 | 96.5 | |
| Subgroup analysis by HbAc1 levels in patients <18 years old c,d | Figure S3, p. 13 | ||||||||
| <7 | 2 | 79 | REM | D-L | −0.04 (−2.67 to 2.58) | 0.97 | <0.001 | 96.2 | |
| >7 | 8 | 1138 | REM | D-L | 5.43 (3.31 to 7.56) | 0.001 | <0.001 | 99.1 | |
| Subgroup analysis by age matching c | Figure S4, p. 14 | ||||||||
| Matched | 15 | 3172 | REM | D-L | 3.06 (2.19 to 3.94) | <0.001 | <0.001 | 98.8 | |
| Unmatched | 5 | 318 | REM | D-L | 0.90 (−0.18 to 1.97) | 0.10 | <0.001 | 94.4 | |
| Subgroup analysis by sex matching c | Figure S5, p. 15 | ||||||||
| Matched | 11 | 2379 | REM | D-L | 0.55 (0.19 to 0.91) | 0.003 | <0.001 | 92.9 | |
| Unmatched | 3 | 224 | REM | D-L | 0.88 (−1.15 to 2.90) | 0.40 | <0.001 | 97.5 | |
| NA | 6 | 887 | REM | D-L | 8.66 (5.37 to 11.96) | <0.001 | <0.001 | 98.9 | |
| Subgroup analysis by sample source c | Figure S6, p. 16 | ||||||||
| Serum | 15 | 3111 | REM | D-L | 2.73 (1.85 to 3.61) | <0.001 | <0.001 | 98.9 | |
| Plasma | 5 | 379 | REM | D-L | 1.34 (0.28 to 2.41) | 0.01 | <0.001 | 94.3 | |
| Subgroup analysis by type of analysis c | Figure S7, p. 17 | ||||||||
| ELISA | 16 | 2235 | REM | D-L | 3.29 (2.27 to 4.30) | <0.001 | <0.001 | 98.8 | |
| Immunoassay panel | 4 | 1255 | REM | D-L | 0.25 (−0.08 to 0.58) | 0.14 | 0.02 | 70.5 | |
| Subgroup analysis by study design c | Figure S8, p. 18 | ||||||||
| Case-control | 16 | 2447 | REM | D-L | 2.77 (2.00 to 3.55) | <0.001 | <0.001 | 98.1 | |
| Cohort | 1 | 398 | — | — | 0.03 (−0.164 to 0.23) | 0.74 | — | — | |
| Cross-sectional | 3 | 645 | REM | D-L | 1.39 (−1.56 to 4.34) | 0.36 | <0.001 | 99.3 | |
| Univariable meta-regression e | |||||||||
| Sex (% of T1DM males) | 17 | 2928 | Random-effects Meta-regression | Coef = 0.011 (−0.619 to 0.641) | 0.97 | —— | —— | Figure S9, p. 19 | |
| Risk of bias (NOS score) | 20 | 3490 | Random-effects Meta-regression | Coef = 0.195 (−3.209 to 3.598) | 0.91 | —— | —— | Figure S10. p. 20 | |
| Determination by qRT-PCR | |||||||||
| All b | 2 | 216 | REM | D-L | −0.66 (−3.02 to 1.71) | 0.59 | <0.001 | 97.1 | —— |
| Determination by Flow Citometry | |||||||||
| All b | 3 | 455 | REM | D-L | 1.40 (−0.19 to 3.00) | 0.08 | <0.001 | 91.8 | —— |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cano-Cano, F.; Gómez-Jaramillo, L.; Ramos-García, P.; Arroba, A.I.; Aguilar-Diosdado, M. IL-1β Implications in Type 1 Diabetes Mellitus Progression: Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1303. https://doi.org/10.3390/jcm11051303
Cano-Cano F, Gómez-Jaramillo L, Ramos-García P, Arroba AI, Aguilar-Diosdado M. IL-1β Implications in Type 1 Diabetes Mellitus Progression: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(5):1303. https://doi.org/10.3390/jcm11051303
Chicago/Turabian StyleCano-Cano, Fátima, Laura Gómez-Jaramillo, Pablo Ramos-García, Ana I. Arroba, and Manuel Aguilar-Diosdado. 2022. "IL-1β Implications in Type 1 Diabetes Mellitus Progression: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 5: 1303. https://doi.org/10.3390/jcm11051303
APA StyleCano-Cano, F., Gómez-Jaramillo, L., Ramos-García, P., Arroba, A. I., & Aguilar-Diosdado, M. (2022). IL-1β Implications in Type 1 Diabetes Mellitus Progression: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(5), 1303. https://doi.org/10.3390/jcm11051303