
The Utility and Diagnostic Accuracy of Transient Elastography in Adults with Morbid Obesity: A Prospective Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Institutional Review Board Approval and Subjects’ Consenting
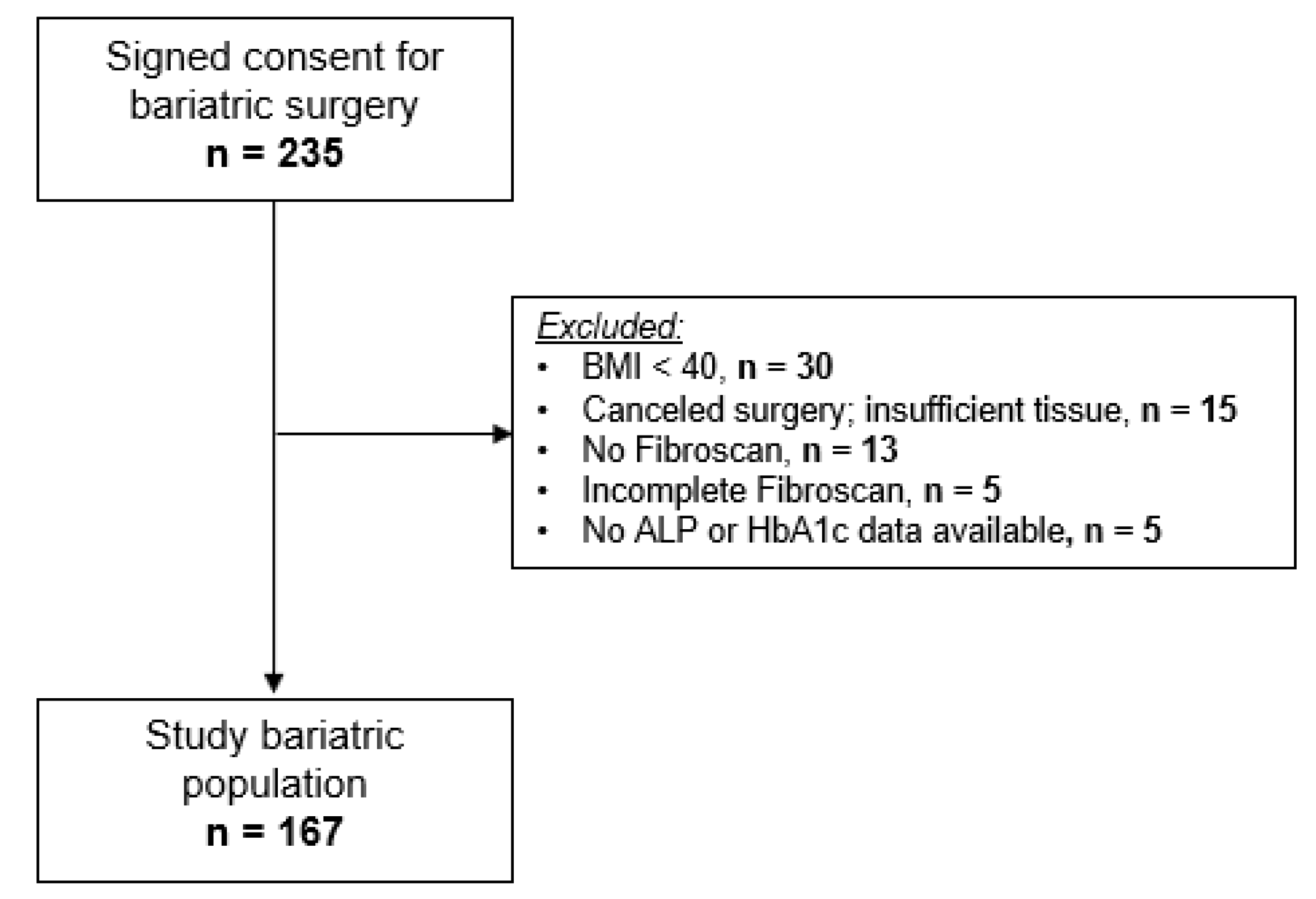
2.2. Study Subjects
2.3. Liver-Stiffness Measurement by Transient Elastography
2.4. Liver Tissue Sampling
2.5. Liver Biopsy Interpretation
2.6. Statistical Analysis
Developing a Model for Predicting Significant Fibrosis
3. Results
3.1. Subject Characteristics
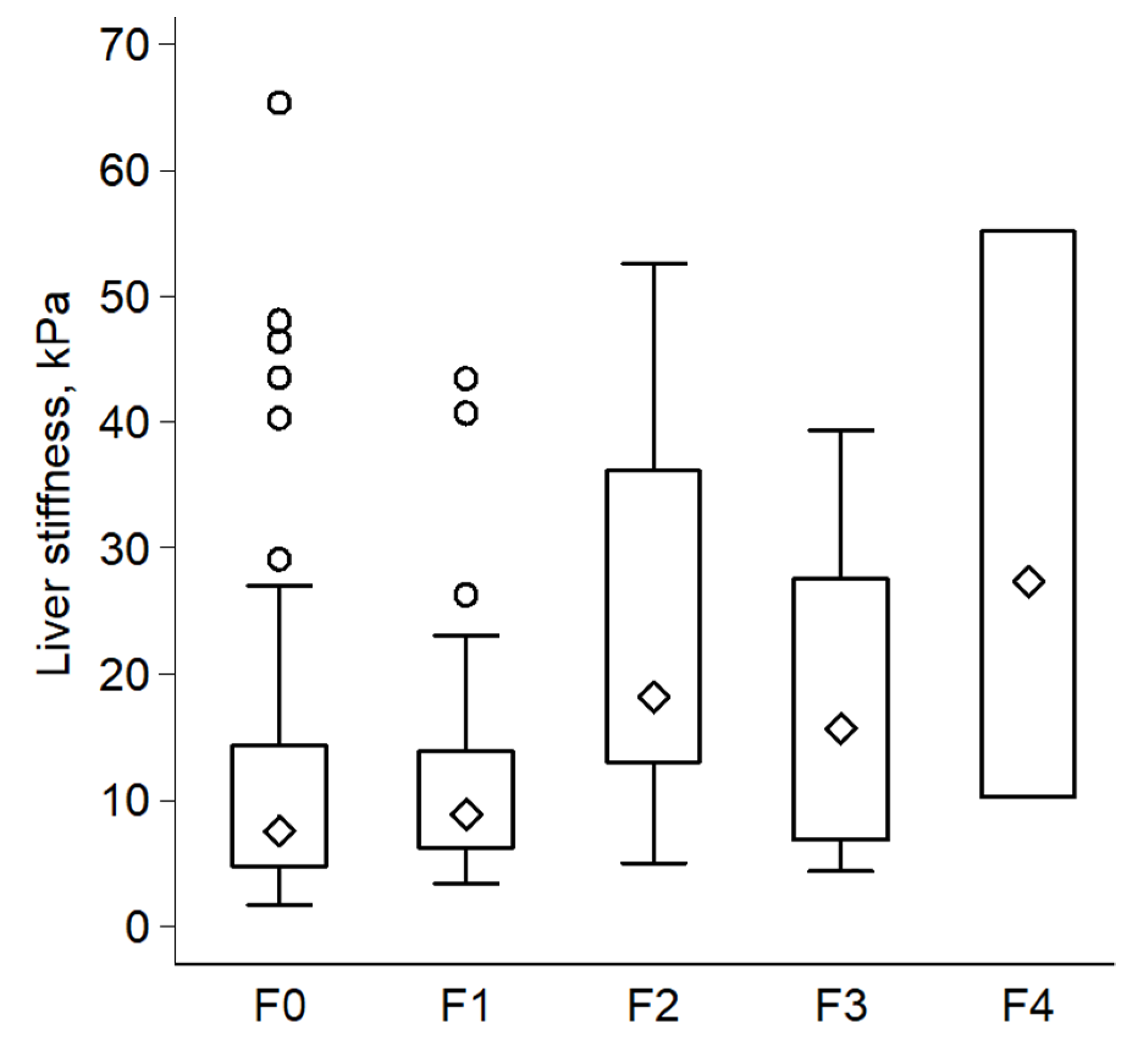
3.2. Fibroscan Measurements
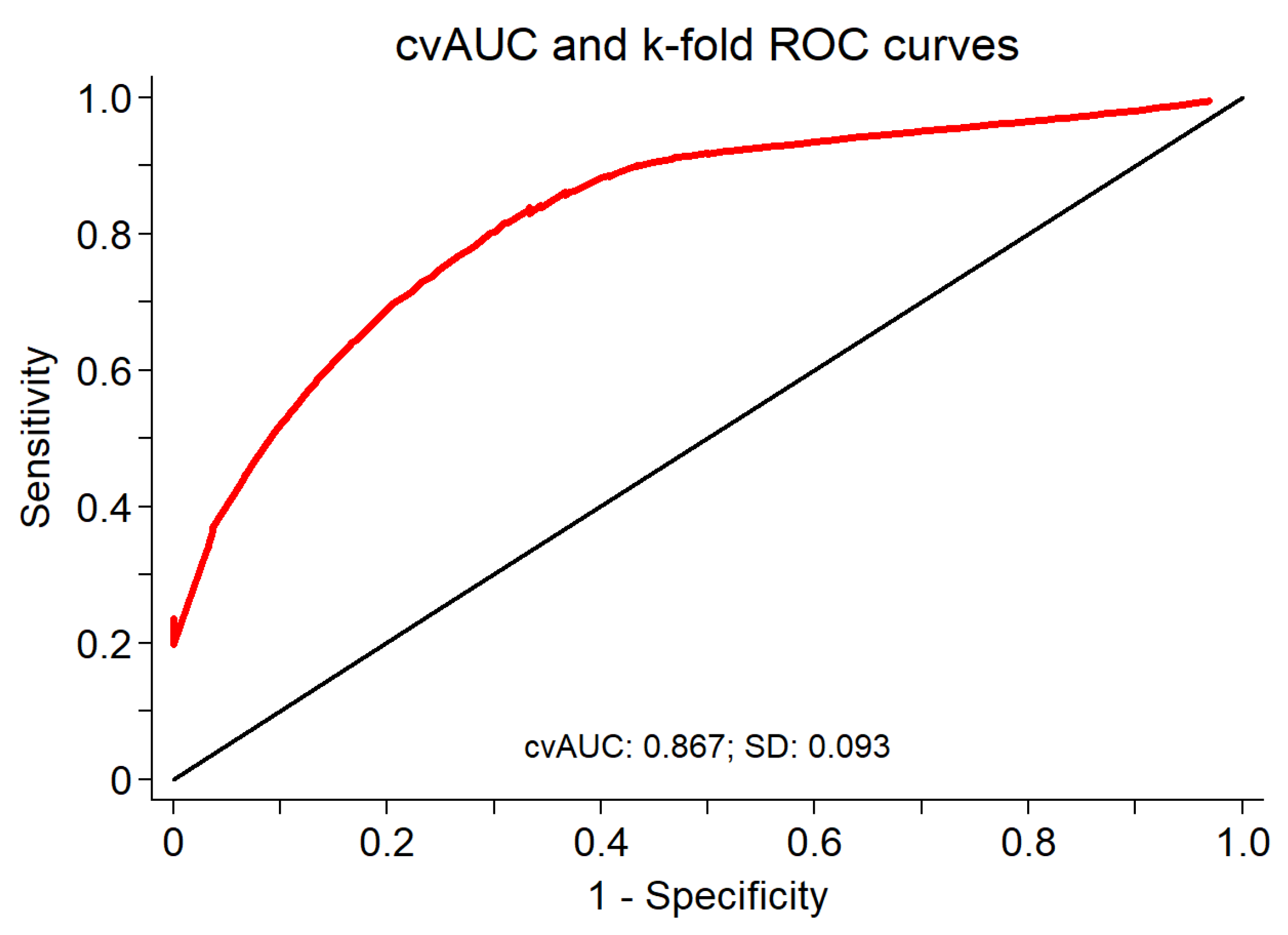
3.3. Diagnostic Performance and Cross Validation of LSM in Discriminating between Presence or Absence of F ≥ 2
3.4. Clinical Phenotyping of those with False-Positive Fibroscan Results
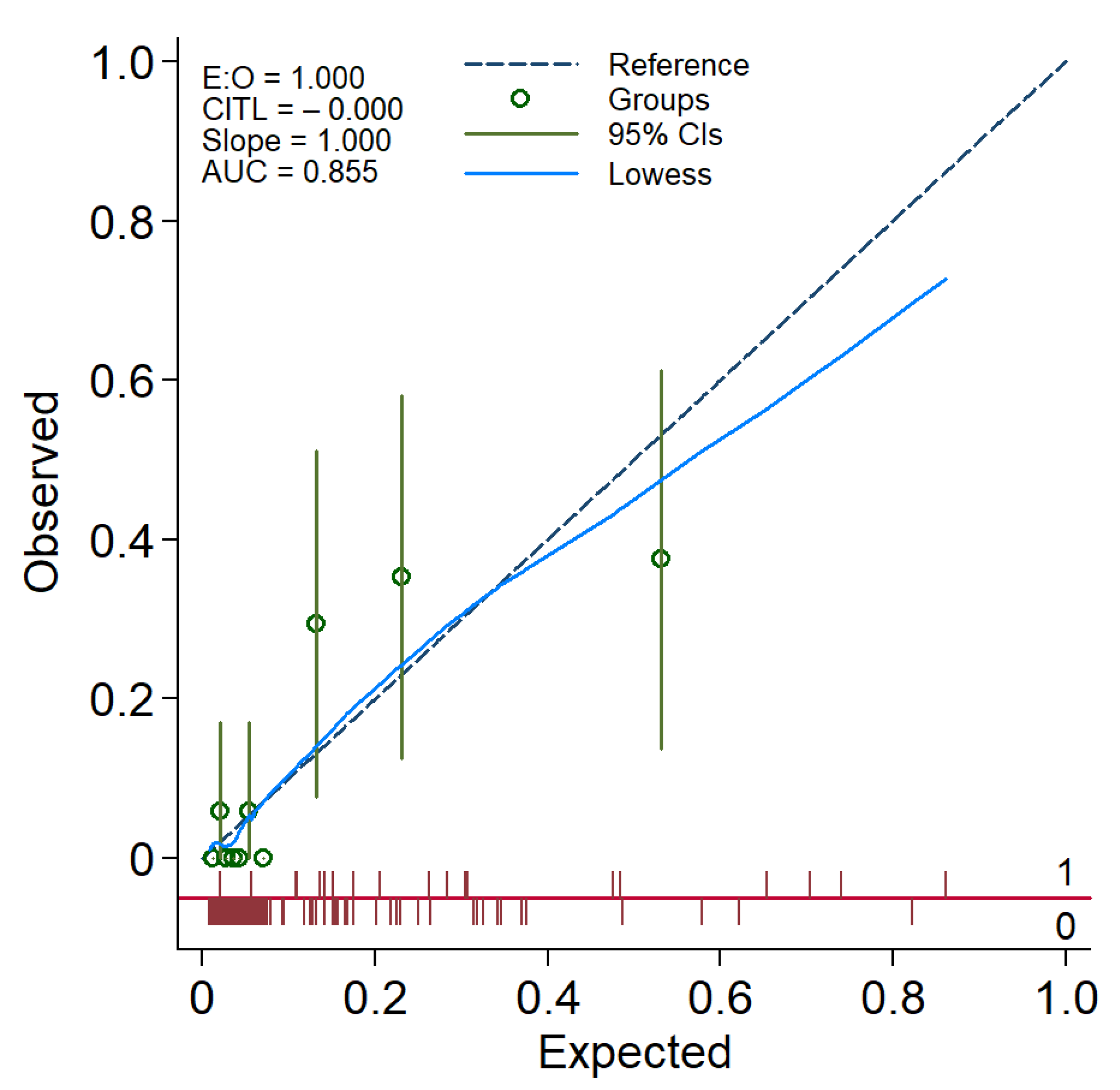
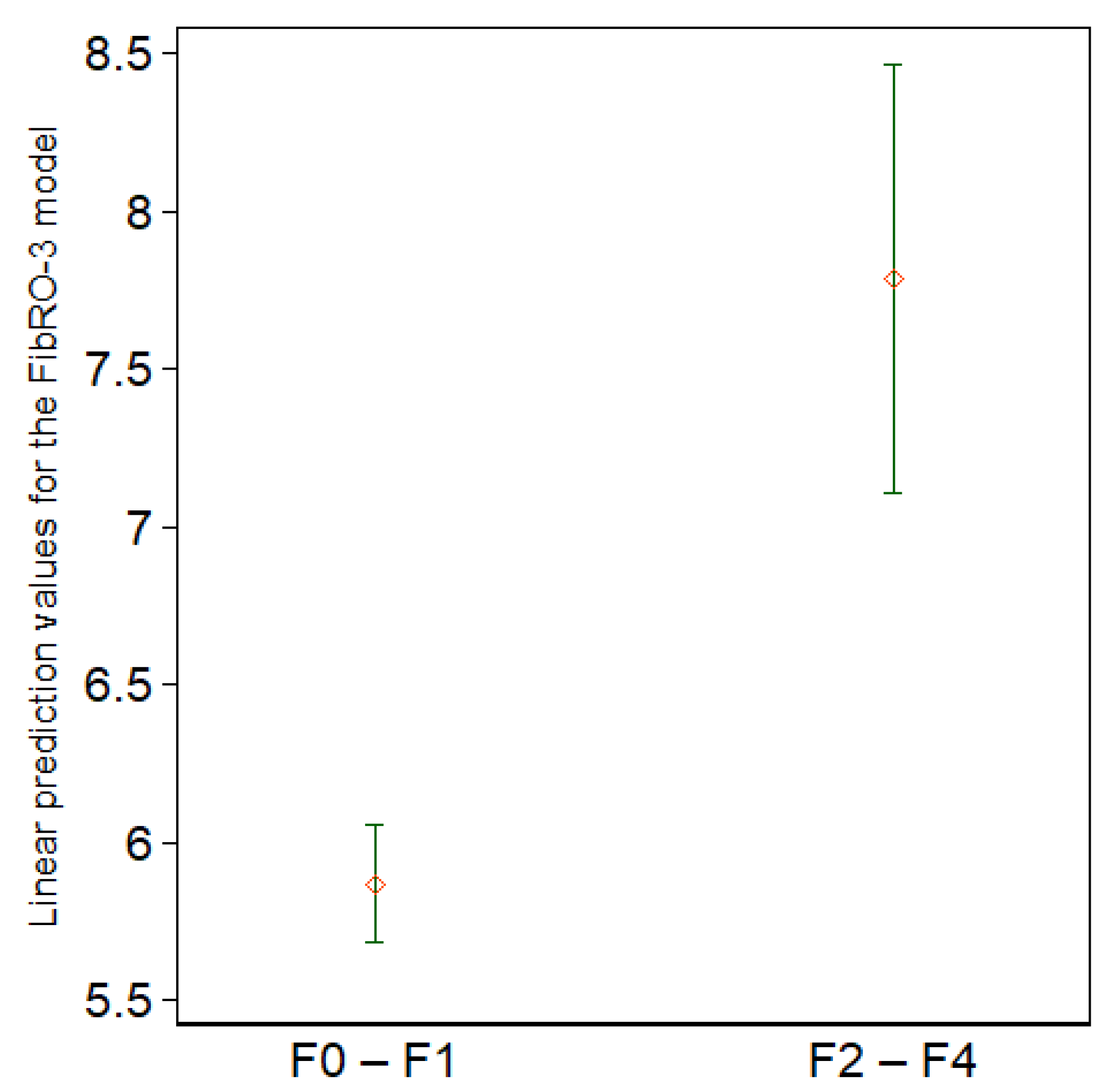
3.5. Predictive Model Building
4. Discussion
4.1. Main Findings
4.2. The Utility of Fibroscan in Patients with Morbid Obesity
4.3. Predictive Model: FibRO-3
4.4. Study Strengths
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.M. Non-alcoholic fatty liver disease—A global public health perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, R.J.; Aguilar, M.; Cheung, R.; Perumpail, R.B.; Harrison, S.A.; Younossi, Z.M.; Ahmed, A. Nonalcoholic Steatohepatitis Is the Second Leading Etiology of Liver Disease Among Adults Awaiting Liver Transplantation in the United States. Gastroenterology 2015, 148, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Stepanova, M.; Ong, J.P.; Jacobson, I.M.; Bugianesi, E.; Duseja, A.; Eguchi, Y.; Wong, V.W.; Negro, F.; Yilmaz, Y.; et al. Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates. Clin. Gastroenterol. Hepatol. 2018, 17, 748–755.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. state-level prevalence of adult obesity and severe obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef]
- Morita, S.; Neto, D.D.S.; Morita, F.H.A.; Morita, N.K.; Lobo, S.M.A. Prevalence of Non-alcoholic Fatty Liver Disease and Steatohepatitis Risk Factors in Patients Undergoing Bariatric Surgery. Obes. Surg. 2015, 25, 2335–2343. [Google Scholar] [CrossRef]
- Soresi, M.; Cabibi, D.; Giglio, R.V.; Martorana, S.; Guercio, G.; Porcasi, R.; Terranova, A.; Lazzaro, L.A.; Emma, M.R.; Augello, G.; et al. The Prevalence of NAFLD and Fibrosis in Bariatric Surgery Patients and the Reliability of Noninvasive Diagnostic Methods. BioMed Res. Int. 2020, 2020, 5023157. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Huang, J.L.W.; George, J.; Huang, J.; Leung, C.; Eslam, M.; Chan, H.L.Y.; Ng, S.C. The changing epidemiology of liver diseases in the Asia–Pacific region. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 57–73. [Google Scholar] [CrossRef]
- Wu, J.; You, J.; Yerian, L.; Shiba, A.; Schauer, P.R.; Sessler, D.I. Prevalence of Liver Steatosis and Fibrosis and the Diagnostic Accuracy of Ultrasound in Bariatric Surgery Patients. Obes. Surg. 2012, 22, 240–247. [Google Scholar] [CrossRef]
- Younossi, Z.; Tacke, F.; Arrese, M.; Sharma, B.C.; Mostafa, I.; Bugianesi, E.; Wong, V.W.-S.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Muir, A.J.; Dieterich, D.T.; Falck-Ytter, Y.T. American Gastroenterological Association Institute Technical Review on the Role of Elastography in Chronic Liver Diseases. Gastroenterology 2017, 152, 1544–1577. [Google Scholar] [CrossRef] [Green Version]
- Lassailly, G.; Caiazzo, R.; Buob, D.; Pigeyre, M.; Verkindt, H.; Labreuche, J.; Raverdy, V.; Leteurtre, E.; Dharancy, S.; Louvet, A.; et al. Bariatric Surgery Reduces Features of Nonalcoholic Steatohepatitis in Morbidly Obese Patients. Gastroenterology 2015, 149, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuffrè, M.; Colecchia, A.; Crocè, L.S. Elastography: Where are we now? Minerva Gastroenterol. 2021, 67, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.; Durango, E.; Dietrich, C.; Seitz, H.K.; Kunz, C.U.; Pomier-Layrargues, G.T.; Duarte-Rojo, A.; Beaton, M.; Elkhashab, M.; Myers, R.P. Direct comparison of the FibroScan XL and M probes for assessment of liver fibrosis in obese and nonobese patients. Hepatic. Med. Evid. Res. 2013, 5, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.L.-H.; Vergniol, J.; Lo, P.; Wong, V.W.-S.; Foucher, J.; Le Bail, B.; Choi, P.C.-L.; Chermak, F.; Leung, K.-S.; Merrouche, W.; et al. Non-invasive assessment of liver fibrosis with transient elastography (FibroScan®): Applying the cut-offs of M probe to XL probe. Ann. Hepatol. 2013, 12, 402–412. [Google Scholar] [CrossRef]
- Myers, R.P.; Pomier-Layrargues, G.; Kirsch, R.; Pollett, A.; Duarte-Rojo, A.; Wong, D.; Beaton, M.; Levstik, M.; Crotty, P.; Elkashab, M. Feasibility and diagnostic performance of the FibroScan XL probe for liver stiffness measurement in overweight and obese patients. Hepatology 2012, 55, 199–208. [Google Scholar] [CrossRef]
- Puthenpura, M.M.; Patel, V.; Fam, J.; Katz, L.; Tichansky, D.S.; Myers, S. The Use of Transient Elastography Technology in the Bariatric Patient: A Review of the Literature. Obes. Surg. 2020, 30, 5108–5116. [Google Scholar] [CrossRef]
- Giuffrè, M.; Giuricin, M.; Bonazza, D.; Rosso, N.; Giraudi, P.J.; Masutti, F.; Palmucci, S.; Basile, A.; Zanconati, F.; De Manzini, N.; et al. Optimization of Point-Shear Wave Elastography by Skin-to-Liver Distance to Assess Liver Fibrosis in Patients Undergoing Bariatric Surgery. Diagnostics 2020, 10, 795. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M. Nonalcoholic Fatty Liver Disease: Pathologic Patterns and Biopsy Evaluation in Clinical Research. Semin. Liver Dis. 2012, 32, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Brunt, E.M.; Janney, C.G.; Di Bisceglie, A.M. Neuschwander-Tetri BA, Bacon BR. Nonalcoholic steatohepatitis: A proposal for grading and staging the histological lesions. Am. J. Gastroenterol. 1999, 94, 2467–2474. [Google Scholar] [CrossRef]
- Brunt, E.M. Nonalcoholic steatohepatitis. Semin. Liver Dis. 2004, 24, 3–20. [Google Scholar] [PubMed] [Green Version]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased risk of mortality by fibrosis stage in nonalcoholic fatty liver disease: Systematic review and meta-analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, A.; Zahediasl, S. Normality Tests for Statistical Analysis: A Guide for Non-Statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, T.P. Modern Regression Methods Wiley Series in Probability and Statistics. In Applied Probability and Statistics; Wiley: New York, NY, USA, 1997; p. 529. [Google Scholar]
- Clayton, P. CUTPT: Stata Module for Empirical Estimation of Cutpoint for a Diagnostic Test. Statistical Software Components 2013. Available online: https://ideas.repec.org/c/boc/bocode/s457719.html (accessed on 10 February 2022).
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its Associated Cutoff Point. Biometr. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [Green Version]
- Luque-Fernandez, M.; Maringe, C.; Nelson, P. CVAUROC: Stata Module to Compute Cross-Validated Area under the Curve for ROC Analysis after Predictive Modelling for Binary Outcomes; Statistical Software Components; Boston College Department of Economics: Chestnut Hill, MA, USA, 2017. [Google Scholar]
- Hosmer, D.W.; Lemesbow, S. Goodness of fit tests for the multiple logistic regression model. Commun. Stat.-Theory Methods 1980, 9, 1043–1069. [Google Scholar] [CrossRef]
- Austin, P.C.; Steyerberg, E.W. Graphical assessment of internal and external calibration of logistic regression models by using loess smoothers. Stat. Med. 2014, 33, 517–535. [Google Scholar] [CrossRef]
- Kao, W.-Y.; Chang, I.-W.; Chen, C.-L.; Su, C.-W.; Fang, S.U.; Tang, J.-H.; Chang, C.-C.; Chang, Y.-J.; Wang, W. Fibroscan-Based Score to Predict Significant Liver Fibrosis in Morbidly Obese Patients with Nonalcoholic Fatty Liver Disease. Obes. Surg. 2020, 30, 1249–1257. [Google Scholar] [CrossRef]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.-H.; Wong, V.W.-S.; et al. FibroScan-AST (FAST) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: A prospective derivation and global validation study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Ensor, J.; Snell, K.; Martin, E. PMCALPLOT: Stata Module to Produce Calibration Plot of Prediction Model Performance; Statistical Software Components S458486; Boston College Department of Economics: Chestnut Hill, MA, USA, May 2018. [Google Scholar]
- Cleves, M.A. From the Help Desk: Comparing Areas under Receiver Operating Characteristic Curves from Two or more Probit or Logit Models. Stata J. 2002, 2, 301–313. [Google Scholar] [CrossRef]
- Weiss, J.; Rau, M.; Meertens, J.; Hering, I.; Reichert, L.; Kudlich, T.; Koschker, A.-K.; Jurowich, C.; Geier, A. Feasibility of liver stiffness measurement in morbidly obese patients undergoing bariatric surgery using XL probe. Scand. J. Gastroenterol. 2016, 51, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Castéra, L.; Vergniol, J.; Foucher, J.; Le Bail, B.; Chanteloup, E.; Haaser, M.; Darriet, M.; Couzigou, P.; de Lédinghen, V. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 2005, 128, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Cheah, M.C.; McCullough, A.J.; Goh, G.B.-B. Current Modalities of Fibrosis Assessment in Non-alcoholic Fatty Liver Disease. J. Clin. Transl. Hepatol. 2017, 5, 261–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlas, T.; Dietrich, A.; Peter, V.; Wittekind, C.; Lichtinghagen, R.; Garnov, N.; Linder, N.; Schaudinn, A.; Busse, H.; Prettin, C.; et al. Evaluation of Transient Elastography, Acoustic Radiation Force Impulse Imaging (ARFI), and Enhanced Liver Function (ELF) Score for Detection of Fibrosis in Morbidly Obese Patients. PLoS ONE 2015, 10, e0141649. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Choi, P.C.; Chan, A.W.; Lo, A.O.; Chim, A.M.; Wong, V.W. Association Between Anthropometric Parameters and Measurements of Liver Stiffness by Transient Elastography. Clin. Gastroenterol. Hepatol. 2013, 11, 295–302. [Google Scholar] [CrossRef]
- Petta, S.; DI Marco, V.; Cammà, C.; Butera, G.; Cabibi, D.; Craxì, A. Reliability of liver stiffness measurement in non-alcoholic fatty liver disease: The effects of body mass index. Aliment. Pharmacol. Ther. 2011, 33, 1350–1360. [Google Scholar] [CrossRef]
- Wai, C.-T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S.-F. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Ooi, G.J.; Burton, P.R.; Doyle, L.; Wentworth, J.M.; Bhathal, P.S.; Sikaris, K.; Cowley, M.; Roberts, S.K.; Kemp, W.; O’Brien, P.E.; et al. Modified thresholds for fibrosis risk scores in nonalcoholic fatty liver disease are necessary in the obese. Obes. Surg. 2017, 27, 115–125. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Subjects | F0–F1 | F2–F4 | p-Value |
|---|---|---|---|---|
| (n = 167) | (n = 148) | (n = 19) | ||
| Age | ||||
| Median | 46 | 45 | 53 | 0.037 |
| Min; Max | 22.9; 77.2 | 22.9; 77.2 | 29.0; 65.7 | |
| Gender, female | ||||
| Percentage | 83.2% | 82.4% | 89.5% | 0.45 |
| Frequency | 139 | 122 | 17 | |
| Tobacco use *, yes | ||||
| Percentage | 48.5% | 48.6% | 47.4% | 0.92 |
| Frequency | 80 | 71 | 9 | |
| Type 2 diabetes *, yes | ||||
| Percentage | 30.9% | 26.03% | 68.4% | <0.0001 |
| Frequency | 51 | 38 | 13 | |
| Hypertension *, yes | ||||
| Percentage | 53.3% | 50.7% | 73.7% | 0.059 |
| Frequency | 88 | 74 | 14 | |
| Hyperlipidemia *, yes | ||||
| Percentage | 44.9% | 41.5% | 63.2% | 0.09 |
| Frequency | 74 | 62 | 12 | |
| Body weight, kg | ||||
| Median | 131.9 | 131.2 | 143.4 | 0.52 |
| Min; Max | 93.4–238.9 | 93.4; 238.9 | 106.9; 173 | |
| Body mass index, kg/m2 | ||||
| Median | 48 | 48 | 53 | 0.22 |
| Min; Max | 40; 67.3 | 40; 67.3 | 40; 63 |
| Variable | All Subjects | F0–F1 | F2–F4 | p-Value |
|---|---|---|---|---|
| (n = 167) | (n = 148) | (n = 19) | ||
| Glucose, mg/dL | ||||
| Median | 94 | 92 | 120 | <0.0001 |
| Min; Max | 57; 211 | 57; 211 | 87; 181 | |
| HbA1c, % | ||||
| Median | 5.7 | 5.7 | 7.3 | <0.0001 |
| Min; Max | 4.3; 13.2 | 4.3; 13.2 | 5.3; 10.5 | |
| Albumin, g/dL | ||||
| Median | 4.3 | 4.3 | 4.6 | 0.08 |
| Min; Max | 3.4; 5.4 | 3.4; 5.3 | 4.0; 5.4 | |
| ALP, U/L | ||||
| Median | 67 | 66 | 88 | 0.0004 |
| Min; Max | 26; 157 | 26; 157 | 53; 127 | |
| AST, U/L | ||||
| Median | 26 | 25 | 38 | 0.002 |
| Min; Max | 9; 152 | 9; 152 | 17; 125 | |
| ALT, U/L | ||||
| Median | 28 | 27 | 42 | 0.008 |
| Min; Max | 9; 273 | 9; 186 | 14; 273 | |
| Hgb, g/dL | ||||
| Median | 13.6 | 13.6 | 14.1 | 0.14 |
| Min; Max | 9.5; 16.7 | 9.5; 16.4 | 12.0–16.7 | |
| Platelets, cells × 109 | ||||
| Median | 261 | 260 | 283 | 0.98 |
| Min; Max | 117; 510 | 138; 510 | 117; 437 | |
| TC, mg/dL | ||||
| Median | 160 | 160 | 171 | 0.92 |
| Min; Max | 77; 265 | 104; 265 | 77; 244 | |
| TG, mg/dL | ||||
| Median | 119 | 117 | 150 | 0.032 |
| Min; Max | 48; 329 | 48; 329 | 78; 243 | |
| LDL, mg/dL | ||||
| Median | 96 | 97 | 96 | 0.56 |
| Min; Max | 21; 205 | 35; 205 | 21; 167 | |
| HDL, mg/dL | ||||
| Median | 39 | 39 | 37 | 0.93 |
| Min; Max | 20; 82 | 20; 82 | 27; 64 |
| Variable | All Subjects | F0–F1 | F2–F4 | p-Value |
|---|---|---|---|---|
| (n = 167) | (n = 148) | (n = 19) | ||
| LSM, kPa | ||||
| Median | 8.3 | 7.7 | 18.2 | |
| IQR | 5–15.7 | 4.9–14.4 | 10.2–28 | 0.0004 |
| Min; Max | 1.7; 65.3 | 1.7; 65.3 | 4.3; 55.1 | |
| IQR/M | ||||
| Median | 0.19 | 0.19 | 0.19 | 0.52 |
| Min; Max | 0.06; 0.38 | 0.06; 0.38 | 0.09; 0.3 | |
| Valid measurements, yes | ||||
| Median | 14 | 14 | 14 | 0.76 |
| Min; Max | 9; 64 | 9; 64 | 12; 22 | |
| ≥10 valid measurements | ||||
| Percentage | 99.4% | 99.3% | 100% | 0.72 |
| Frequency | 166 | 147 | 19 | |
| Success rate, % | ||||
| Median | 58.8 | 58.1 | 63.4 | 0.48 |
| Min; Max | 0.95; 100.0 | 0.95; 100.0 | 6.7; 100.0 | |
| Success rate ≥ 60% | ||||
| Percentage | 55.7% | 54.7% | 63.2% | 0.49 |
| Frequency | 93 | 81 | 23 | |
| Reliable Fibroscan, yes | ||||
| Percentage | 52.7% | 52.03% | 57.9% | 0.63 |
| Frequency | 88 | 77 | 11 | |
| CAP, dB/m | ||||
| Median | 329 | 322 | 382 | 0.002 |
| Min; Max | 100; 400 | 100; 400 | 249; 400 |
| Fibrosis ≥ 2 | |||
|---|---|---|---|
| LSM ≥ 12.8 kPa | Absent | Present | Total |
| No | True Negative | False negative | |
| 105 | 5 | 110 | |
| Yes | False positive | True positive | |
| 43 | 14 | 57 | |
| Total | 148 | 19 | 167 |
| Variable | Group | p-Value | |
|---|---|---|---|
| False Positive (n = 43) | True Negative (n = 105) | ||
| Age | |||
| Median | 48 | 44 | 0.19 |
| Diabetes, yes | |||
| Percentage | 45.2% | 18.3% | 0.002 |
| Frequency | (19/42) | (19/104) | |
| Weight, kg | |||
| Median | 141.2 | 129.1 | 0.007 |
| BMI, kg/m2 | |||
| Median | 52.0 | 44.6 | 0.0005 |
| CAP, dB/m | |||
| Median | 371.0 | 310.0 | 0.0003 |
| BMI > 45 | |||
| Percentage | 86.1% | 53.3% | <0.0001 |
| Frequency | 37 | 56 | |
| BMI > 50 | |||
| Percentage | 60.5% | 29.5% | <0.0001 |
| Frequency | 26 | 31 | |
| BMI >55 | |||
| Percentage | 30.2% | 14.3% | 0.025 |
| Frequency | 13 | 15 | |
| BMI > 60 | |||
| Percentage | 16.3% | 6.7% | 0.07 |
| Frequency | 7 | 7 | |
| BMI > 65 | |||
| Percentage | 9.3% | 0.95% | 0.01 |
| Frequency | 4 | 4 | |
| Fibrosis stage 0 (histology) | |||
| Percentage | 83.7% | 80.0% | 0.65 |
| Frequency | 36 | 84 | |
| Fibrosis stage 1 (histology) | |||
| Percentage | 16.3% | 20.0% | 0.65 |
| Frequency | 7 | 21 | |
| Severe steatosis (≥66%) | |||
| Percentage | 16.3% | 18.1% | 0.79 |
| Frequency | 7 | 19 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, A.H.; Al Juboori, A.; Petroski, G.F.; Diaz-Arias, A.A.; Syed-Abdul, M.M.; Wheeler, A.A.; Ganga, R.R.; Pitt, J.B.; Spencer, N.M.; Hammoud, G.M.; et al. The Utility and Diagnostic Accuracy of Transient Elastography in Adults with Morbid Obesity: A Prospective Study. J. Clin. Med. 2022, 11, 1201. https://doi.org/10.3390/jcm11051201
Ali AH, Al Juboori A, Petroski GF, Diaz-Arias AA, Syed-Abdul MM, Wheeler AA, Ganga RR, Pitt JB, Spencer NM, Hammoud GM, et al. The Utility and Diagnostic Accuracy of Transient Elastography in Adults with Morbid Obesity: A Prospective Study. Journal of Clinical Medicine. 2022; 11(5):1201. https://doi.org/10.3390/jcm11051201
Chicago/Turabian StyleAli, Ahmad Hassan, Alhareth Al Juboori, Gregory F. Petroski, Alberto A. Diaz-Arias, Majid M. Syed-Abdul, Andrew A. Wheeler, Rama R. Ganga, James B. Pitt, Nicole M. Spencer, Ghassan M. Hammoud, and et al. 2022. "The Utility and Diagnostic Accuracy of Transient Elastography in Adults with Morbid Obesity: A Prospective Study" Journal of Clinical Medicine 11, no. 5: 1201. https://doi.org/10.3390/jcm11051201
APA StyleAli, A. H., Al Juboori, A., Petroski, G. F., Diaz-Arias, A. A., Syed-Abdul, M. M., Wheeler, A. A., Ganga, R. R., Pitt, J. B., Spencer, N. M., Hammoud, G. M., Rector, R. S., Parks, E. J., & Ibdah, J. A. (2022). The Utility and Diagnostic Accuracy of Transient Elastography in Adults with Morbid Obesity: A Prospective Study. Journal of Clinical Medicine, 11(5), 1201. https://doi.org/10.3390/jcm11051201