
Goal Attainment in an Individually Tailored and Home-Based Intervention in the Chronic Phase after Traumatic Brain Injury

 ,
,
Abstract
:1. Introduction
Aims
2. Materials and Methods
2.1. Participants
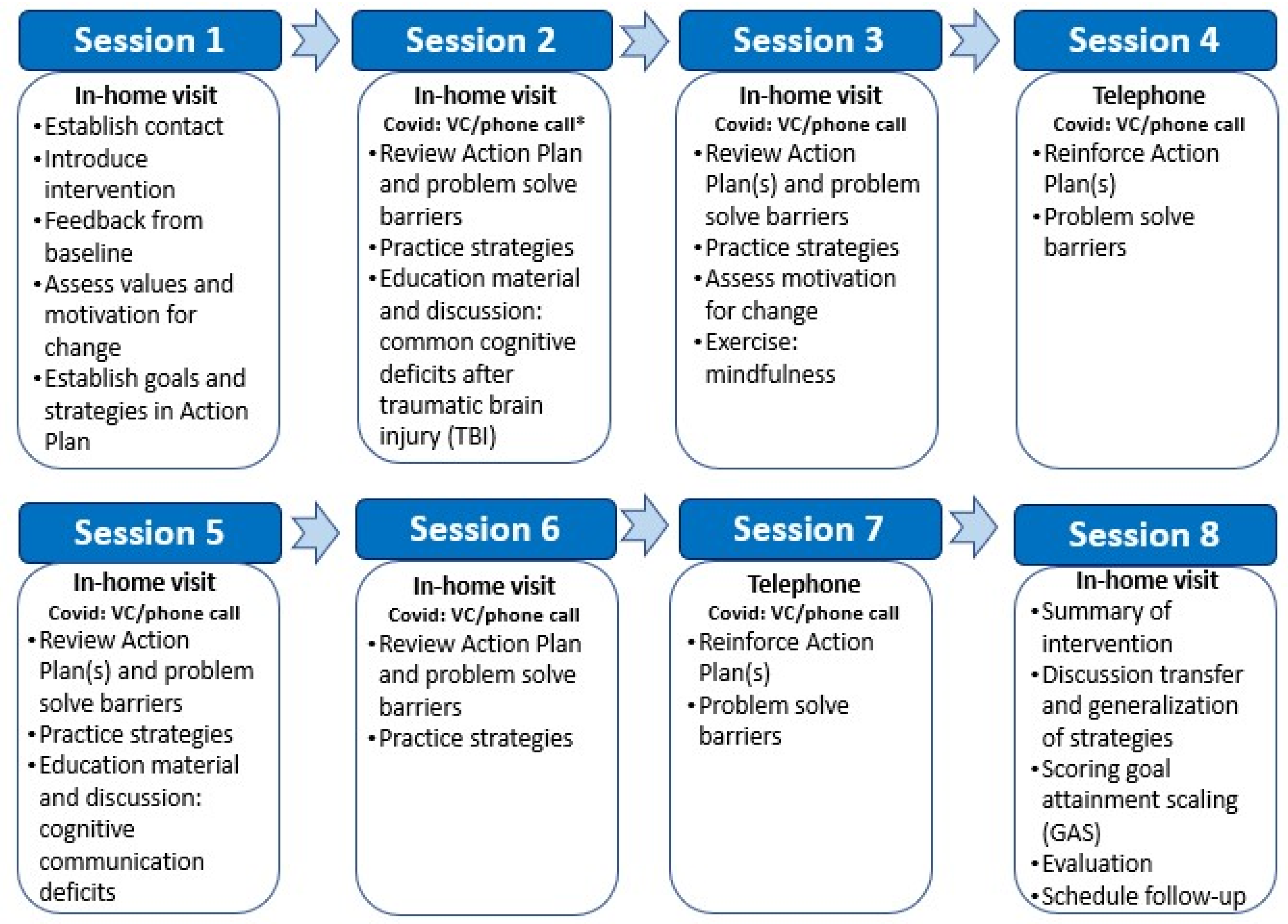
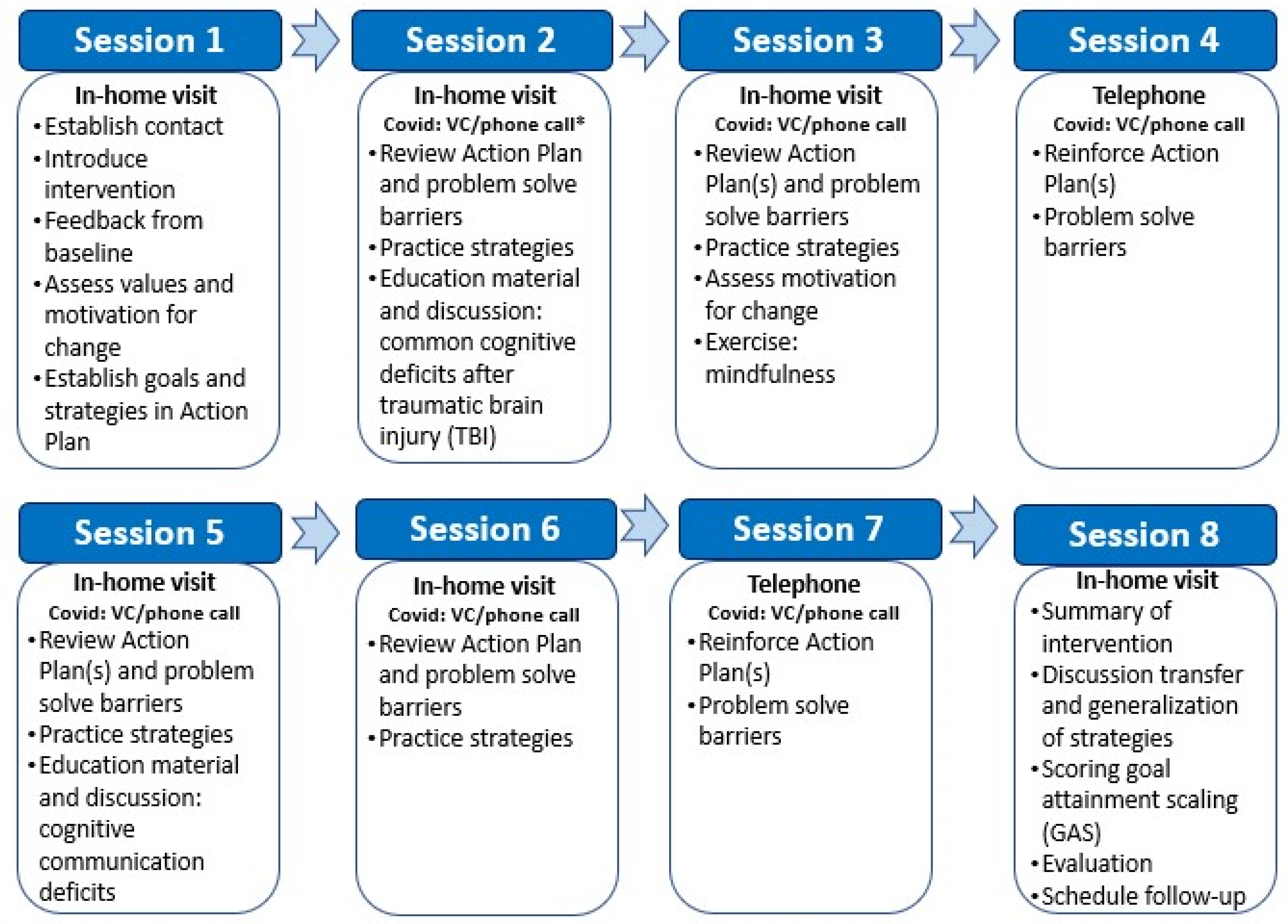
2.2. Intervention
2.3. Outcomes
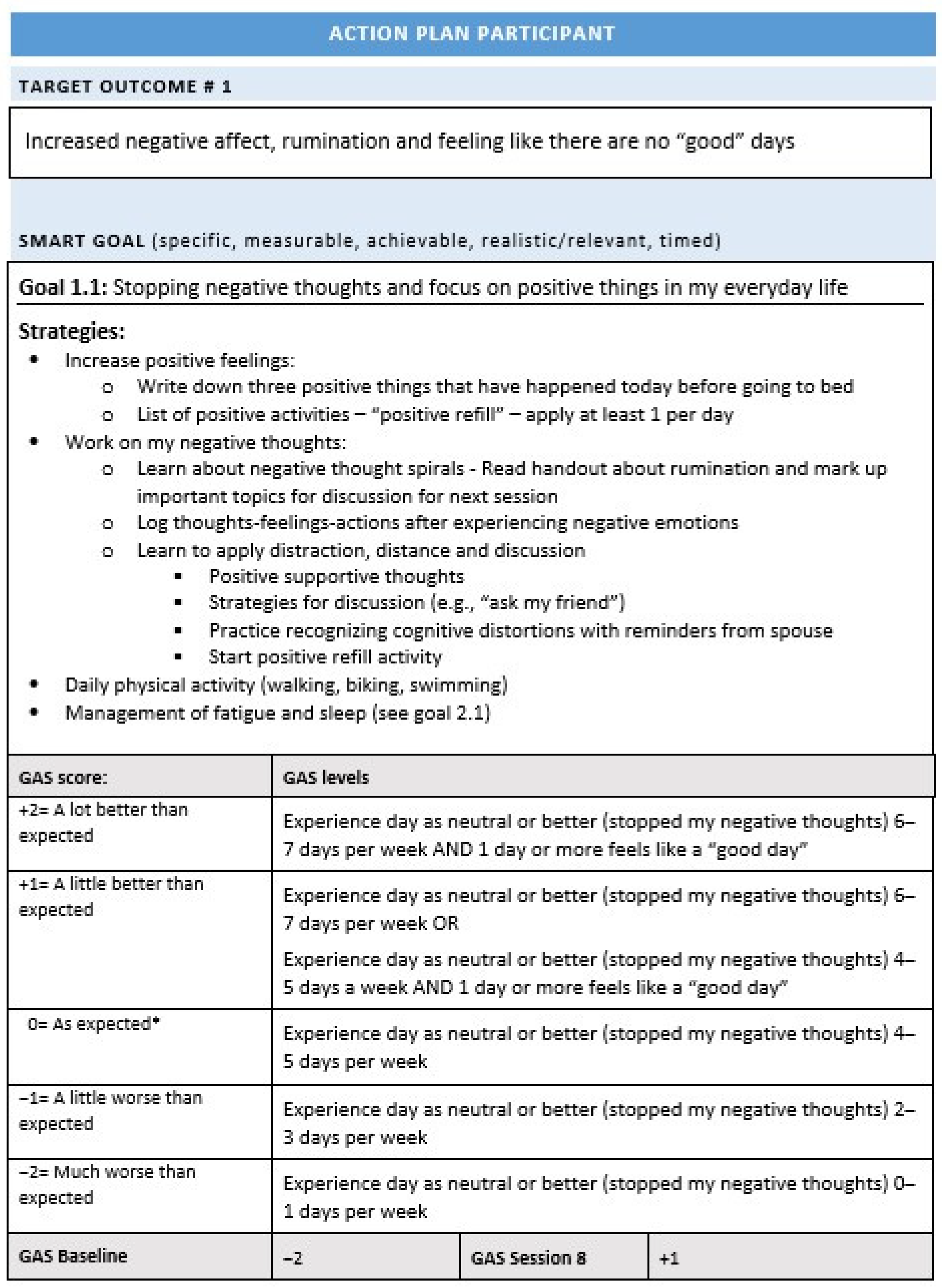
2.3.1. Goal Attainment Scaling
2.3.2. SMART Goal Categorization
2.3.3. Exploring Variables Associated with Goal Attainment
2.4. Statistical Methods
2.5. Ethics
3. Results
3.1. Participants
3.2. SMART Goals
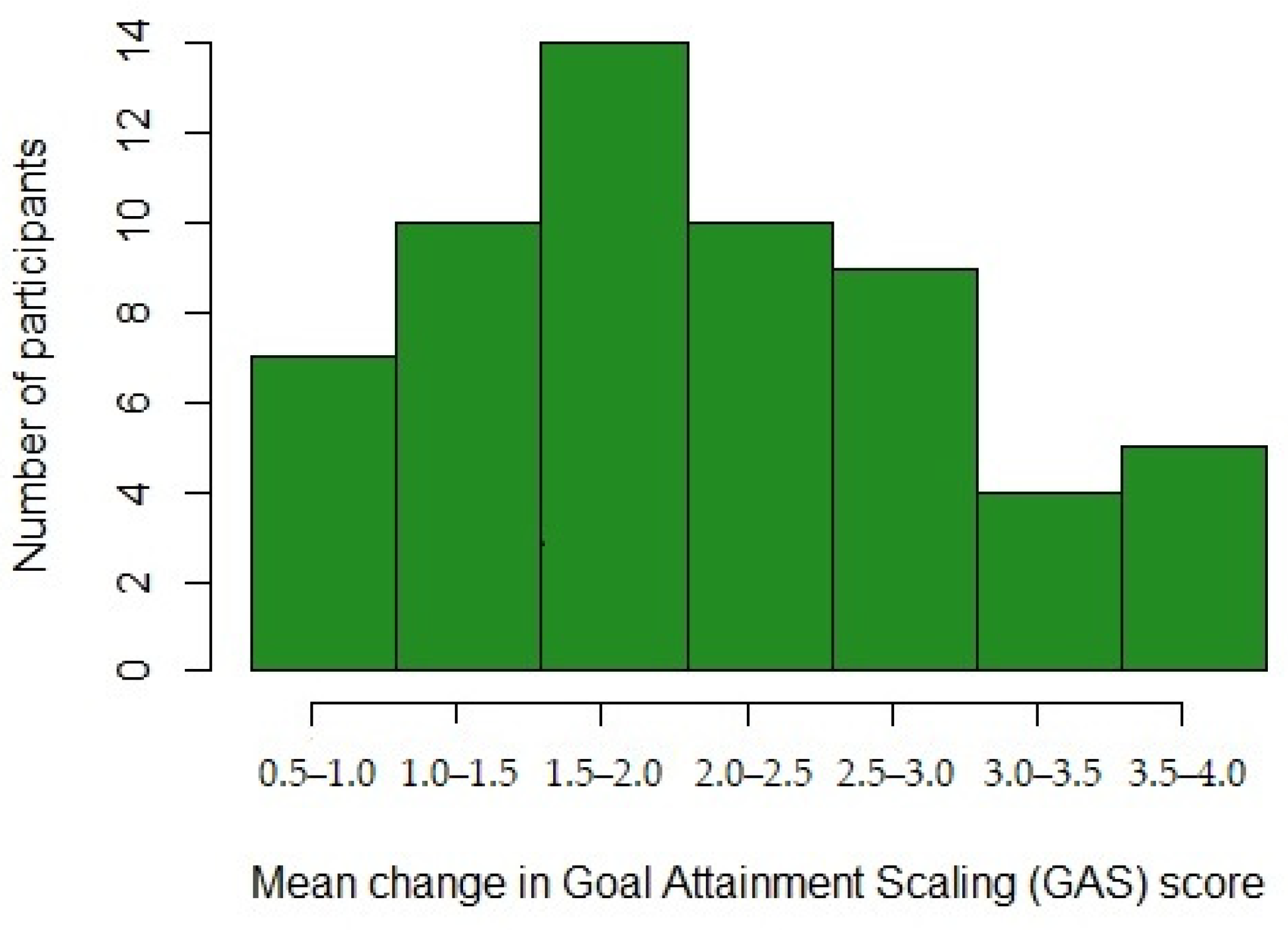
3.2.1. Goal Attainment
3.2.2. SMART Goal Domains and Categories
3.2.3. Indicators of Goal Attainment
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tagliaferri, F.; Compagnone, C.; Korsic, M.; Servadei, F.; Kraus, J. A systematic review of brain injury epidemiology in Europe. Acta Neurochir. 2005, 148, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Peeters, W.; Brande, R.V.D.; Polinder, S.; Brazinova, A.; Steyerberg, E.W.; Lingsma, H.F.; Maas, A.I.R. Epidemiology of traumatic brain injury in Europe. Acta Neurochir. 2015, 157, 1683–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, A.B.; Xu, L.; Daugherty, J.; Breiding, M.J. Surveillance report of traumatic brain injury-related emergency department visits, hospitalizations, and deaths, United States, 2014. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services; 2019. Available online: https://stacks.cdc.gov/view/cdc/78062 (accessed on 17 September 2021).
- Olver, J.; Ponsford, J.L.; Curran, C.A. Outcome following traumatic brain injury: A comparison between 2 and 5 years after injury. Brain Inj. 1996, 10, 841–848. [Google Scholar] [CrossRef]
- Brooks, J.C.; Strauss, D.J.; Shavelle, R.M.; Paculdo, D.; Hammond, F.M.; Harrison-Felix, C.L. Long-Term Disability and Survival in Traumatic Brain Injury: Results from the National Institute on Disability and Rehabilitation Research Model Systems. Arch. Phys. Med. Rehabil. 2013, 94, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Dikmen, S.S.; Machamer, J.; Powell, J.M.; Temkin, N.R. Outcome 3 to 5 years after moderate to severe traumatic brain injury. Arch. Phys. Med. Rehabil. 2003, 84, 1449–1457. [Google Scholar] [CrossRef]
- Ruttan, L.; Martin, K.; Liu, A.; Colella, B.; Green, R. Long-Term Cognitive Outcome in Moderate to Severe Traumatic Brain Injury: A Meta-Analysis Examining Timed and Untimed Tests at 1 and 4.5 or More Years After Injury. Arch. Phys. Med. Rehabil. 2008, 89, S69–S76. [Google Scholar] [CrossRef] [PubMed]
- Andelic, N.; Hammergren, N.; Bautz-Holter, E.; Sveen, U.; Brunborg, C.; Røe, C. Functional outcome and health-related quality of life 10 years after moderate-to-severe traumatic brain injury. Acta Neurol. Scand. 2009, 120, 16–23. [Google Scholar] [CrossRef]
- Forslund, M.; Perrin, P.; Sigurdardottir, S.; Howe, E.; van Walsem, M.; Arango-Lasprilla, J.; Lu, J.; Aza, A.; Jerstad, T.; Røe, C.; et al. Health-Related Quality of Life Trajectories across 10 Years after Moderate to Severe Traumatic Brain Injury in Norway. J. Clin. Med. 2021, 10, 157. [Google Scholar] [CrossRef]
- Miller, L. Family therapy of brain injury: Syndromes, strategies, and solutions. Am. J. Fam. Ther. 1993, 21, 111–121. [Google Scholar] [CrossRef]
- Brickell, T.A.; French, L.; Lippa, S.M.; Lange, R.T. Burden among caregivers of service members and veterans following traumatic brain injury. Brain Inj. 2018, 32, 1541–1548. [Google Scholar] [CrossRef]
- Saban, K.L.; Griffin, J.M.; Urban, A.; Janusek, M.A.; Pape, T.B.; Collins, E. Perceived health, caregiver burden, and quality of life in women partners providing care to Veterans with traumatic brain injury. J. Rehabil. Res. Dev. 2016, 53, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Doser, K.; Norup, A. Caregiver burden in Danish family members of patients with severe brain injury: The chronic phase. Brain Inj. 2016, 30, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Manskow, U.S.; Friborg, O.; Røe, C.; Braine, M.; Damsgard, E.; Anke, A. Patterns of change and stability in caregiver burden and life satisfaction from 1 to 2 years after severe traumatic brain injury: A Norwegian longitudinal study. NeuroRehabilitation 2017, 40, 211–222. [Google Scholar] [CrossRef] [Green Version]
- Masel, B.E.; DeWitt, D.S. Traumatic Brain Injury: A Disease Process, Not an Event. J. Neurotrauma 2010, 27, 1529–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrigan, J.D.; Hammond, F.M. Traumatic Brain Injury as a Chronic Health Condition. Arch. Phys. Med. Rehabil. 2013, 94, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.; Stewart, W.; Dams-O’Connor, K.; Diaz-Arrastia, R.; Horton, L.; Menon, D.K.; Polinder, S. The chronic and evolving neurological consequences of traumatic brain injury. Lancet Neurol. 2017, 16, 813–825. [Google Scholar] [CrossRef] [Green Version]
- Sigurdardottir, S.; Andelic, N.; Røe, C.; Schanke, A.-K. Trajectory of 10-Year Neurocognitive Functioning After Moderate–Severe Traumatic Brain Injury: Early Associations and Clinical Application. J. Int. Neuropsychol. Soc. 2020, 26, 654–667. [Google Scholar] [CrossRef]
- Forslund, M.V.; Perrin, P.B.; Røe, C.; Sigurdardottir, S.; Hellstrøm, T.; Berntsen, S.A.; Lu, J.; Arango-Lasprilla, J.C.; Andelic, N. Global Outcome Trajectories up to 10 Years After Moderate to Severe Traumatic Brain Injury. Front. Neurol. 2019, 10, 219. [Google Scholar] [CrossRef] [Green Version]
- Hoofien, D.; Gilboa, A.; Vakil, E.; Donovick, P.J. Traumatic brain injury (TBI) 10?20 years later: A comprehensive outcome study of psychiatric symptomatology, cognitive abilities and psychosocial functioning. Brain Inj. 2001, 15, 189–209. [Google Scholar] [CrossRef]
- Koskinen, S. Quality of life 10 years after a very severe traumatic brain injury (TBI): The perspective of the injured and the closest relative. Brain Inj. 1998, 12, 631–648. [Google Scholar] [CrossRef]
- Hammond, F.M.; Perkins, S.M.; Corrigan, J.D.; Nakase-Richardson, R.; Brown, A.W.; O’Neil-Pirozzi, T.M.; Zasler, N.D.; Greenwald, B.D. Functional Change from Five to Fifteen Years after Traumatic Brain Injury. J. Neurotrauma 2021, 38, 858–869. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.K.; Ng, S.; Dashner, J.; Baum, M.C.; Hammel, J.; Magasi, S.; Lai, J.-S.; Carlozzi, N.E.; Tulsky, D.S.; Miskovic, A.; et al. Relationships between environmental factors and participation in adults with traumatic brain injury, stroke, and spinal cord injury: A cross-sectional multi-center study. Qual. Life Res. 2017, 26, 2633–2645. [Google Scholar] [CrossRef] [PubMed]
- Whiteneck, G.G.; Gerhart, K.A.; Cusick, C.P. Identifying Environmental Factors That Influence the Outcomes of People with Traumatic Brain Injury. J. Head Trauma Rehabil. 2004, 19, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Cicerone, K.D.; Goldin, Y.; Ganci, K.; Rosenbaum, A.; Wethe, J.V.; Langenbahn, D.M.; Malec, J.F.; Bergquist, T.F.; Kingsley, K.; Nagele, D.; et al. Evidence-Based Cognitive Rehabilitation: Systematic Review of the Literature From 2009 Through 2014. Arch. Phys. Med. Rehabil. 2019, 100, 1515–1533. [Google Scholar] [CrossRef] [Green Version]
- Cicerone, K.D.; Mott, T.; Azulay, J.; Friel, J.C. Community integration and satisfaction with functioning after intensive cognitive rehabilitation for traumatic brain injury. Arch. Phys. Med. Rehabil. 2004, 85, 943–950. [Google Scholar] [CrossRef]
- Patterson, F.; Fleming, J.; Doig, E. Group-based delivery of interventions in traumatic brain injury rehabilitation: A scoping review. Disabil. Rehabil. 2016, 38, 1961–1986. [Google Scholar] [CrossRef]
- Evans, L.; Brewis, C. The efficacy of community-based rehabilitation programmes for adults with TBI. Int. J. Ther. Rehabil. 2008, 15, 446–458. [Google Scholar] [CrossRef] [Green Version]
- Andelic, N.; Soberg, H.L.; Berntsen, S.; Sigurdardottir, S.; Roe, C. Self-Perceived Health Care Needs and Delivery of Health Care Services 5 Years After Moderate-to-Severe Traumatic Brain Injury. PM&R 2014, 6, 1013–1021. [Google Scholar] [CrossRef]
- Andelic, N.; Røe, C.; Tenovuo, O.; Azouvi, P.; Dawes, H.; Majdan, M.; Ranta, J.; Howe, E.; Wiegers, E.; Tverdal, C.; et al. Unmet Rehabilitation Needs after Traumatic Brain Injury across Europe: Results from the CENTER-TBI Study. J. Clin. Med. 2021, 10, 1035. [Google Scholar] [CrossRef]
- Barnes, M.P. Principles of neurological rehabilitation. J. Neurol. Neurosurg. Psychiatry 2003, 74, iv3–iv7. [Google Scholar] [CrossRef] [Green Version]
- Yun, D.; Choi, J. Person-centered rehabilitation care and outcomes: A systematic literature review. Int. J. Nurs. Stud. 2019, 93, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.A. Neuropsychological Rehabilitation. Annu. Rev. Clin. Psychol. 2008, 4, 141–162. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.; Rosewilliam, S.; Soundy, A. Shared decision making within goal setting in rehabilitation settings: A systematic review. Patient Educ. Couns. 2016, 100, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Levack, W.M.M.; Taylor, K.; Siegert, R.J.; Dean, S.G.; McPherson, K.M.; Weatherall, M. Is goal planning in rehabilitation effective? A systematic review. Clin. Rehabil. 2006, 20, 739–755. [Google Scholar] [CrossRef]
- Levack, W.M.M.; Weatherall, M.; Hay-Smith, E.J.C.; Dean, S.; McPherson, K.; Siegert, R. Goal setting and strategies to enhance goal pursuit for adults with acquired disability participating in rehabilitation. Cochrane Database Syst. Rev. 2015, CD009727. [Google Scholar] [CrossRef] [Green Version]
- Doig, E.; Fleming, J.; Kuipers, P.; Cornwell, P.; Khan, A. Goal-directed outpatient rehabilitation following TBI: A pilot study of programme effectiveness and comparison of outcomes in home and day hospital settings. Brain Inj. 2011, 25, 1114–1125. [Google Scholar] [CrossRef]
- Powell, J.; Heslin, J.; Greenwood, R. Community based rehabilitation after severe traumatic brain injury: A randomised controlled trial. J. Neurol. Neurosurg. Psychiatry 2002, 72, 193–202. [Google Scholar] [CrossRef] [Green Version]
- McClain, C. Collaborative Rehabilitation Goal Setting. Top. Stroke Rehabil. 2005, 12, 56–60. [Google Scholar] [CrossRef]
- Wade, D.T. Goal setting in rehabilitation: An overview of what, why and how. Clin. Rehabil. 2009, 23, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Prescott, S.; Fleming, J.; Doig, E. Goal setting approaches and principles used in rehabilitation for people with acquired brain injury: A systematic scoping review. Brain Inj. 2015, 29, 1515–1529. [Google Scholar] [CrossRef]
- Hersh, D.; Worrall, L.; Howe, T.; Sherratt, S.; Davidson, B. SMARTERgoal setting in aphasia rehabilitation. Aphasiology 2012, 26, 220–233. [Google Scholar] [CrossRef]
- Hart, T.; Evans, J. Self-regulation and Goal Theories in Brain Injury Rehabilitation. J. Head Trauma Rehabil. 2006, 21, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Schönberger, M.; Humle, F.; Teasdale, T.W. The development of the therapeutic working alliance, patients’ awareness and their compliance during the process of brain injury rehabilitation. Brain Inj. 2006, 20, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Plant, S.; Tyson, S.; Kirk, S.; Parsons, J. What are the barriers and facilitators to goal-setting during rehabilitation for stroke and other acquired brain injuries? A systematic review and meta-synthesis. Clin. Rehabil. 2016, 30, 921–930. [Google Scholar] [CrossRef]
- Brands, I.; Stapert, S.; Wade, D.; Van Heugten, C.; Köhler, S. Life goal attainment in the adaptation process after acquired brain injury: The influence of self-efficacy and of flexibility and tenacity in goal pursuit. Clin. Rehabil. 2014, 29, 611–622. [Google Scholar] [CrossRef]
- Siegert, R.J.; McPherson, K.M.; Taylor, W.J. Toward a cognitive-affective model of goal-setting in rehabilitation: Is self-regulation theory a key step? Disabil. Rehabil. 2004, 26, 1175–1183. [Google Scholar] [CrossRef]
- Playford, E.D.; Siegert, R.J.; Levack, W.; Freeman, J. Areas of consensus and controversy about goal setting in rehabilitation: A conference report. Clin. Rehabil. 2009, 23, 334–344. [Google Scholar] [CrossRef]
- Scobbie, L.; Wyke, S.; Dixon, D. Identifying and applying psychological theory to setting and achieving rehabilitation goals. Clin. Rehabil. 2009, 23, 321–333. [Google Scholar] [CrossRef] [Green Version]
- Turner-Stokes, L. Goal attainment scaling (GAS) in rehabilitation: A practical guide. Clin. Rehabil. 2009, 23, 362–370. [Google Scholar] [CrossRef]
- Liu, C.; Mcneil, J.E.; Greenwood, R. Rehabilitation outcomes after brain injury: Disability measures or goal acheivement? Clin. Rehabil. 2004, 18, 398–404. [Google Scholar] [CrossRef]
- Kiresuk, T.J.; Sherman, R.E. Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Ment. Health J. 1968, 4, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.; Ponsford, J. Goal Attainment Scaling in brain injury rehabilitation: Strengths, limitations and recommendations for future applications. Neuropsychol. Rehabil. 2014, 24, 661–677. [Google Scholar] [CrossRef] [PubMed]
- Hurn, J.; Kneebone, I.; Cropley, M. Goal setting as an outcome measure: A systematic review. Clin. Rehabil. 2006, 20, 756–772. [Google Scholar] [CrossRef] [PubMed]
- Trevena-Peters, J.; McKay, A.; Ponsford, J. Activities of daily living retraining and goal attainment during posttraumatic amnesia. Neuropsychol. Rehabil. 2018, 29, 1655–1670. [Google Scholar] [CrossRef] [PubMed]
- Behn, N.; Marshall, J.; Togher, L.; Cruice, M. Feasibility and initial efficacy of project-based treatment for people with ABI. Int. J. Lang. Commun. Disord. 2019, 54, 465–478. [Google Scholar] [CrossRef]
- Winter, L.; Moriarty, H.J.; Robinson, K.; Piersol, C.; Vause-Earland, T.; Newhart, B.; Iacovone, D.B.; Hodgson, N.; Gitlin, L.N. Efficacy and acceptability of a home-based, family-inclusive intervention for veterans with TBI: A randomized controlled trial. Brain Inj. 2016, 30, 373–387. [Google Scholar] [CrossRef]
- Borgen, I.M.H.; Løvstad, M.; Andelic, N.; Hauger, S.; Sigurdardottir, S.; Søberg, H.L.; Sveen, U.; Forslund, M.V.; Kleffelgård, I.; Lindstad, M.; et al. Traumatic brain injury—Needs and treatment options in the chronic phase: Study protocol for a randomized controlled community-based intervention. Trials 2020, 21, 294. [Google Scholar] [CrossRef]
- Bovend’Eerdt, T.J.H.; Botell, R.; Wade, D. Writing SMART rehabilitation goals and achieving goal attainment scaling: A practical guide. Clin. Rehabil. 2009, 23, 352–361. [Google Scholar] [CrossRef]
- Malec, J.F. Goal Attainment Scaling in Rehabilitation. Neuropsychol. Rehabil. 1999, 9, 253–275. [Google Scholar] [CrossRef]
- Winter, L.; Moriarty, H.J.; Piersol, C.V.; Vause-Earland, T.; Robinson, K.; Newhart, B. Patient-and family-identified problems of traumatic brain injury: Value and utility of a target outcome approach to identifying the worst problems. J. Patient-Cent. Res. Rev. 2016, 3, 30–39. [Google Scholar] [CrossRef]
- Borgen, I.M.H.; Kleffelgård, I.; Hauger, S.L.; Forslund, M.V.; Søberg, H.L.; Andelic, N.; Sveen, U.; Winter, L.; Løvstad, M.; Røe, C. Patient-Reported Problem Areas in Chronic Traumatic Brain Injury. J. Head Trauma Rehabil. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Rimel, R.W.; Giordani, B.; Barth, J.T.; Jane, J.A. Moderate Head Injury: Completing the Clinical Spectrum of Brain Trauma. Neurosurgery 1982, 11, 344–351. [Google Scholar] [CrossRef]
- Wilson, J.L.; Pettigrew, L.E.; Teasdale, G.M. Structured Interviews for the Glasgow Outcome Scale and the Extended Glasgow Outcome Scale: Guidelines for Their Use. J. Neurotrauma 1998, 15, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Adult Intelligence Scale, 4th ed.; WAIS–IV; Pearson: London, UK, 2008. [Google Scholar]
- Migliore, S.; Ghazaryan, A.; Simonelli, I.; Pasqualetti, P.; Squitieri, F.; Curcio, G.; Landi, D.; Palmieri, M.G.; Moffa, F.; Filippi, M.M.; et al. Cognitive Impairment in Relapsing-Remitting Multiple Sclerosis Patients with Very Mild Clinical Disability. Behav. Neurol. 2017, 2017, 8140962. [Google Scholar] [CrossRef] [PubMed]
- Binder, L.M.; Iverson, G.L.; Brooks, B.L. To Err is Human: “Abnormal” Neuropsychological Scores and Variability are Common in Healthy Adults. Arch. Clin. Neuropsychol. 2009, 24, 31–46. [Google Scholar] [CrossRef] [Green Version]
- Delis, D.C.; Kramer, J.H.; Kaplan, E.; Ober, B.A. California Verbal Learning Test, 2nd ed.; Harcourt Assessment: San Antonio, TX, USA, 2000. [Google Scholar]
- Delis, D.C.; Kaplan, E.; Kramer, J.H. Delis-Kaplan Executive Function System; The Psychological Corporation: San Antonio, TX, USA, 2001. [Google Scholar]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.G.; Wade, D. The Rivermead Post Concussion Symptoms Questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Roth, R.M.; Isquith, P.K.; Gioia, G.A. Behavior Rating Inventory of Executive Function—Adult Version (BRIEF-A); Psychological Assessment Resources: Lutz, FL, USA, 2005. [Google Scholar]
- Evans, J.J. Goal setting during rehabilitation early and late after acquired brain injury. Curr. Opin. Neurol. 2012, 25, 651–655. [Google Scholar] [CrossRef]
- Herdman, K.A.; Vandermorris, S.; Davidson, S.; Au, A.; Troyer, A.K. Comparable achievement of client-identified, self-rated goals in intervention and no-intervention groups: Reevaluating the use of Goal Attainment Scaling as an outcome measure. Neuropsychol. Rehabil. 2018, 29, 1600–1610. [Google Scholar] [CrossRef]
- Whyte, J.; Hart, T. It’s More Than a Black Box; It’s a Russian Doll. Am. J. Phys. Med. Rehabil. 2003, 82, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Farace, E.; Alves, W.M. Do women fare worse: A metaanalysis of gender differences in traumatic brain injury outcome. J. Neurosurg. 2000, 93, 539–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colantonio, A.; Harris, J.E.; Ratcliff, G.; Chase, S.; Ellis, K. Gender differences in self reported long term outcomes following moderate to severe traumatic brain injury. BMC Neurol. 2010, 10, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemeier, J.P.; Perrin, P.; Holcomb, M.G.; Rolston, C.D.; Artman, L.K.; Lu, J.; Nersessova, K.S. Gender Differences in Awareness and Outcomes During Acute Traumatic Brain Injury Recovery. J. Women’s Health 2014, 23, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Plant, S.; Tyson, S.F. A multicentre study of how goal-setting is practised during inpatient stroke rehabilitation. Clin. Rehabil. 2017, 32, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Schönberger, M.; Ponsford, J.; Gould, K.R.; Johnston, L. The Temporal Relationship Between Depression, Anxiety, and Functional Status after Traumatic Brain Injury: A Cross-lagged Analysis. J. Int. Neuropsychol. Soc. 2011, 17, 781–787. [Google Scholar] [CrossRef]
- Curran, C.A.; Ponsford, J.L.; Crowe, S. Coping strategies and emotional outcome following traumatic brain injury: A compar-ison with orthopedic patients. J. Head Trauma Rehab. 2000, 15, 1256–1274. [Google Scholar] [CrossRef]
- Sherer, M.; Evans, C.C.; Leverenz, J.; Stouter, J.; Irby, J.W., Jr.; Eun-Lee, J.; Yablon, S.A. Therapeutic alliance in post-acute brain injury rehabilitation: Predictors of strength of alliance and impact of alliance on outcome. Brain Inj. 2007, 21, 663–672. [Google Scholar] [CrossRef]
- Tennant, A. Goal attainment scaling: Current methodological challenges. Disabil. Rehabil. 2007, 29, 1583–1588. [Google Scholar] [CrossRef]
- Kuipers, P.; Foster, M.; Carlson, G.; Moy, J. Classifying client goals in community-based ABI rehabilitation: A taxonomy for profiling service delivery and conceptualizing outcomes. Disabil. Rehabil. 2003, 25, 154–162. [Google Scholar] [CrossRef]
- Grill, E.; Lohmann, S.; Decker, J.; Müller, M.; Strobl, R.; Grill, E. The ICF forms a useful framework for classifying individual patient goals in post-acute rehabilitation. J. Rehabil. Med. 2011, 43, 151–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Assessment Domain | Measure Name | Score Used (Min.–Max.) |
|---|---|---|
| Global Outcome | GOSE [64] | Total score (3–8) |
| Cognitive functioning | ||
| Verbal and visual abstraction/reasoning | ||
| Similarities and Matrices, WAIS-IV [65] | A dichotomized impairment variable was established, where impairment was defined as at least two test results being ≤1.5 standard deviation below the normative mean (no/yes) [66,67] | |
| Verbal attention and working memory | Digit Span, WAIS-IV [65] | |
| Verbal learning and memory | CVLT-II [68] | |
| Processing speed, mental flexibility, and inhibition | Trail Making Tests 1–5 and Color Word Interference Tests 1–4, D-KEFS [69] | |
| Self-reported symptoms | ||
| Post-concussive symptoms | RPQ [70] | Total score (0–64) |
| Fatigue | RPQ item [70] | Item score (0, 2–4) |
| Depressive symptoms | PHQ-9 [71] | Total score (0–27) |
| Anxiety-related symptoms | GAD-7 [72] | Total score (0–21) |
| Overall psychiatric distress | PHQ-9 [71] and GAD-7 [72] | Score of ≥10 on either scale (no/yes) [71,72] |
| Self-reported executive dysfunction | BRIEF-A [73] | Global Executive Composite t-score (0–100) |
| Characteristics | Mean (SD)/Median (Range)/n(%) | |
|---|---|---|
| Demographics | ||
| Age, y | 43.12 (13.61) | |
| Gender, male | 43 (73%) | |
| Education, y | 12 (10–20) | |
| Marital status | Single | 21 (36%) |
| Married/domestic partner | 32 (54%) | |
| Other (widowed, divorced, separated) | 6 (10%) | |
| Injury-related factors | ||
| Injury severity (GCS) * | 8 (3–15) | |
| Mild | 16 (27%) | |
| Moderate | 9 (15%) | |
| Severe | 30 (51%) | |
| NA | 4 (7%) | |
| Cause of injury ** | Fall | 17 (29%) |
| Transport-related | 24 (40%) | |
| Violence | 4 (7%) | |
| Other † | 11 (19%) | |
| NA | 3 (5%) | |
| Time since injury ***, y | 4 (2–23) | |
| Work participation | ||
| Work percentage | 0 (0–100) | |
| Work status | Works full-time | 16 (27%) |
| Works part-time | 13 (22%) | |
| Disability/sick leave/retired | 30 (51%) |
| Below Expectation | At Expectation | Above Expectation | Total | |
|---|---|---|---|---|
| Domain/Category (number of participants) | n | n | n | n |
| Cognitive difficulties | 4 (11%) | 11 (29%) | 23 (60%) | 38 (100%) |
| Attention difficulties (n = 5, 9%) | 1 | 2 | 4 | 7 |
| Memory difficulties (n = 15, 25%) | 3 | 6 | 11 | 20 |
| Language difficulties (n = 1, 2%) | 0 | 0 | 1 | 1 |
| Cognitive aspects of executive functioning (n = 10, 17%) | 0 | 3 | 7 | 10 |
| Physical/somatic difficulties | 5 (9%) | 13 (25%) | 35 (66%) | 53 (100%) |
| Reduced capacity and fatigue (n = 21, 36%) | 2 | 7 | 13 | 22 |
| Pain (n = 4, 7%) | 0 | 0 | 4 | 4 |
| Sleep difficulties (n = 11, 19%) | 1 | 1 | 10 | 12 |
| Difficulties with motor functions (n = 6, 10%) | 0 | 5 | 3 | 8 |
| Difficulties with dizziness and balance (n = 7, 12%) | 2 | 0 | 5 | 7 |
| Emotional difficulties | 2 (6%) | 8 (23%) | 25 (71%) | 35 (100%) |
| Emotion perception and regulation (n = 3, 5%) | 0 | 0 | 3 | 3 |
| Irritability (n = 9, 15%) | 1 | 3 | 6 | 10 |
| Anxiety (n = 9, 15%) | 0 | 2 | 8 | 10 |
| Depressive thoughts and feelings (n = 8, 14%) | 0 | 2 | 6 | 8 |
| Difficulties with coping with stress (n = 3, 5%) | 1 | 1 | 1 | 3 |
| Difficulties with identity, acceptance, and sense of self (n = 1, 2%) | 0 | 0 | 1 | 1 |
| Social function and participation | 2 (8%) | 9 (36%) | 14 (56%) | 25 (100%) |
| Behavioral dysregulation (n= 1, 2%) | 0 | 0 | 1 | 1 |
| Social communication difficulties (n = 10, 17%) | 0 | 3 | 6 | 9 |
| Reduced self-sufficiency (n = 4, 7%) | 0 | 2 | 2 | 4 |
| Reduced social participation (n = 4, 7%) | 0 | 1 | 3 | 4 |
| Lack of meaningful activities (n = 6, 10%) | 2 | 3 | 2 | 7 |
| Total | 13 (8.6%) | 41 (27.2%) | 97 (64.2%) | 151 |
| Exploratory Variables | B | 95% CI | Significance | R Square | Decision |
|---|---|---|---|---|---|
| Demographic factors | |||||
| Age | 0.002 | −0.013 to 0.016 | 0.826 | 0.001 | Discard |
| Gender | 0.327 | −0.102 to 0.757 | 0.133 | 0.039 | Keep |
| Education (in years) | −0.042 | −0.125 to 0.040 | 0.306 | 0.018 | Discard |
| Percentage work participation (%) | 0.002 | −0.002 to 0.007 | 0.272 | 0.021 | Discard |
| Injury-related factors | |||||
| GCS score | 0.013 | −0.034 to 0.060 | 0.588 | 0.006 | Discard |
| Cause of injury (fall) | 0.039 | −0.125 to 0.204 | 0.633 | 0.004 | Discard |
| Months since injury | 0.000 | −0.003 to 0.004 | 0.886 | 0.000 | Discard |
| Functional status/symptoms at baseline | |||||
| Global functioning (GOSE) | −0.001 | −0.202 to 0.201 | 0.994 | 0.000 | Discard |
| Neuropsychology—overall impairment | −0.237 | −0.623 to 0.149 | 0.224 | 0.026 | Discard |
| Self-reported symptoms at baseline | |||||
| Post-concussion symptoms (RPQ total score) | 0.004 | −0.012 to 0.021 | 0.606 | 0.005 | Discard |
| Fatigue (RPQ item) | 0.047 | −0.093 to 0.187 | 0.506 | 0.008 | Discard |
| Depression (PHQ-9 total score) | −0.010 | −0.045 to 0.026 | 0.589 | 0.005 | Discard |
| Anxiety (GAD-7 total score) | −0.032 | −0.078 to 0.014 | 0.173 | 0.032 | Keep |
| Psychiatric symptoms (PHQ-9 and/or GAD-7 ≥ 10) | −0.072 | −0.483 to 0.339 | 0.726 | 0.002 | Discard |
| Executive dysfunction (BRIEF-A GEC t-score) | −0.023 | −0.044 to −0.002 | 0.032 | 0.080 | Keep |
| Intervention factors | |||||
| Treatment expectation at session 1 | 0.027 | −0.074 to 0.127 | 0.595 | 0.005 | Discard |
| Treatment expectation at session 3 | 0.125 | 0.019 to 0.230 | 0.022 | 0.090 | Keep |
| Family member participation | 0.099 | −0.312 to 0.509 | 0.633 | 0.004 | Discard |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borgen, I.M.H.; Hauger, S.L.; Forslund, M.V.; Kleffelgård, I.; Brunborg, C.; Andelic, N.; Sveen, U.; Søberg, H.L.; Sigurdardottir, S.; Røe, C.; et al. Goal Attainment in an Individually Tailored and Home-Based Intervention in the Chronic Phase after Traumatic Brain Injury. J. Clin. Med. 2022, 11, 958. https://doi.org/10.3390/jcm11040958
Borgen IMH, Hauger SL, Forslund MV, Kleffelgård I, Brunborg C, Andelic N, Sveen U, Søberg HL, Sigurdardottir S, Røe C, et al. Goal Attainment in an Individually Tailored and Home-Based Intervention in the Chronic Phase after Traumatic Brain Injury. Journal of Clinical Medicine. 2022; 11(4):958. https://doi.org/10.3390/jcm11040958
Chicago/Turabian StyleBorgen, Ida M. H., Solveig L. Hauger, Marit V. Forslund, Ingerid Kleffelgård, Cathrine Brunborg, Nada Andelic, Unni Sveen, Helene L. Søberg, Solrun Sigurdardottir, Cecilie Røe, and et al. 2022. "Goal Attainment in an Individually Tailored and Home-Based Intervention in the Chronic Phase after Traumatic Brain Injury" Journal of Clinical Medicine 11, no. 4: 958. https://doi.org/10.3390/jcm11040958
APA StyleBorgen, I. M. H., Hauger, S. L., Forslund, M. V., Kleffelgård, I., Brunborg, C., Andelic, N., Sveen, U., Søberg, H. L., Sigurdardottir, S., Røe, C., & Løvstad, M. (2022). Goal Attainment in an Individually Tailored and Home-Based Intervention in the Chronic Phase after Traumatic Brain Injury. Journal of Clinical Medicine, 11(4), 958. https://doi.org/10.3390/jcm11040958