
Risk of Death and Ischemic Stroke in Patients with Atrial Arrhythmia and Thrombus or Sludge in Left Atrial Appendage at One-Year Follow-Up

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Subsection
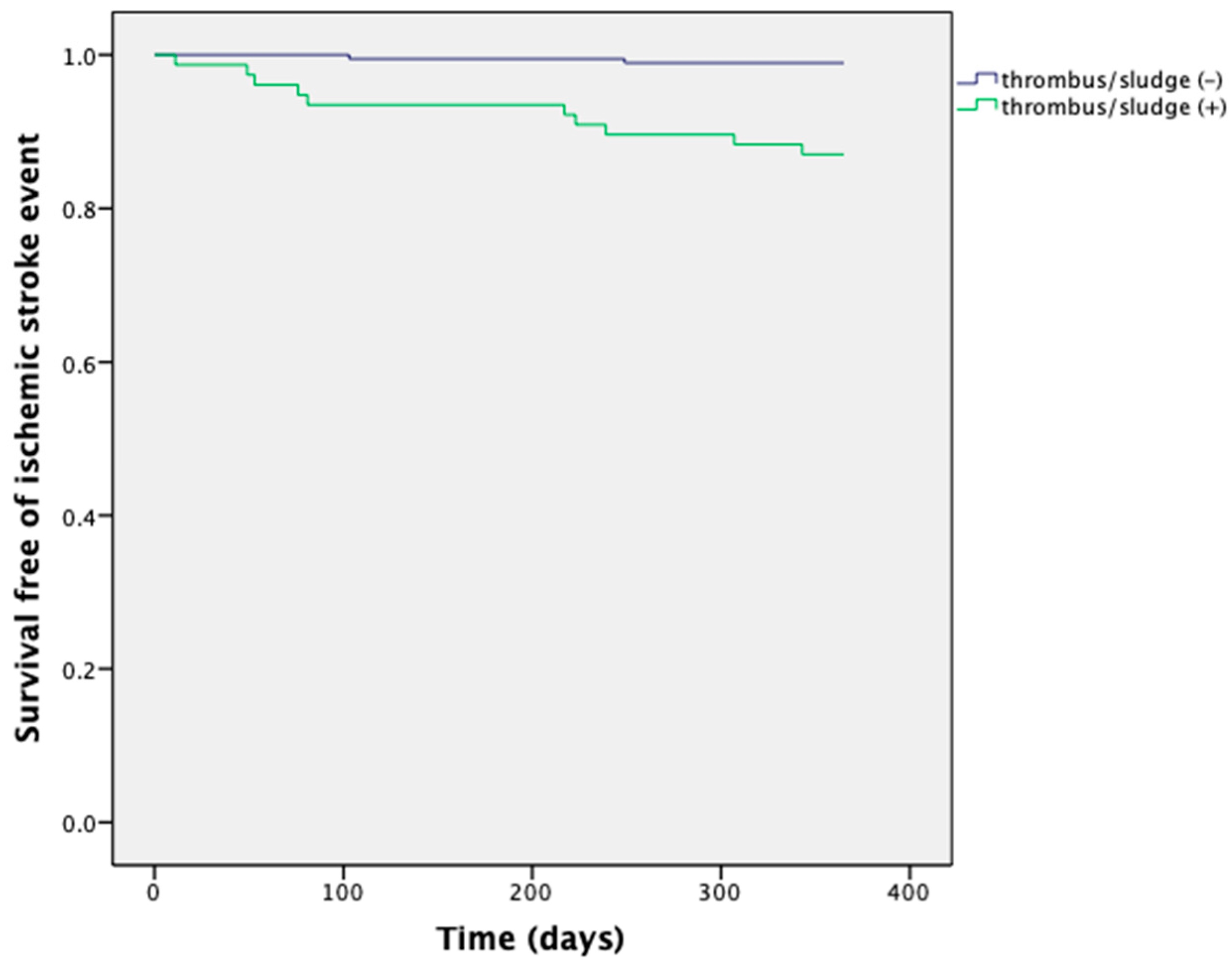
3.1.1. Risk of Ischemic Stroke and Annual Mortality
3.1.2. Differences in Risk of Ischemic Stroke and Annual Mortality between Sludge vs. Appendage Free from Thrombus and Sludge
3.1.3. No Significant Differences in Risk of Ischemic Stroke and Annual Mortality between Thrombus and Sludge
3.1.4. No Significant Differences in Risk Level between Successful and Unsuccessful Thrombus/Sludge Resolution
3.1.5. No Significant Differences in Risk Level between Patients Treated with LMWH vs. OAC
3.1.6. No Significant Differences in Risk Level between Patients Subjected to TOE Control vs. Those without Further TOE Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feinberg, W.M.; Blackshear, J.L.; Laupacis, A.; Kronmal, R.; Hart, R.G. Prevalence, age distribution, and gender of patients with atrial fibrillation. Analysis and implications. Arch. Intern. Med. 1995, 155, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Chug, S.S.; Roth, G.A.; Gillum, R.F.; Mensah, G.A. Global burden of atrial fibrillation in developed and developing nations. Glob. Heart 2014, 9, 113–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.; Wang, Y.L.; Shantsila, A.; Lip, G.Y. The global burden of atrial fibrillation and stroke: A systematic review of the Clinical epidemiology of atrial fibrillation in Asia. Chest 2017, 152, 810–820. [Google Scholar] [CrossRef]
- Lip, G.Y.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: The euro heart survey on atrial fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Steinberg, B.A.; Hellkamp, A.S.; Lokhnygina, Y.; Patel, M.R.; Breithardt, G.; Hankey, G.J.; Becker, R.C.; Singer, D.E.; Halperin, J.L.; Hacke, W. Higher risk of death and stroke in patients with persistent vs. paroxysmal atrial fibrillation: Results from the ROCKET-AF Trial. Eur. Heart J. 2015, 36, 288–296. [Google Scholar] [CrossRef] [Green Version]
- Watson, T.; Shantsila, E.; Lip, G.Y. Mechanisms of thrombogenesis in atrial fibrillation: Virchow’s triad revisited. Lancet 2009, 373, 155–166. [Google Scholar] [CrossRef]
- Sikorska, A.; Baran, J.; Pilichowska-Paszkiet, E.; Sikora-Frac, M.; Krynski, T.; Piotrowski, R.; Stec, S.; Zaborska, B.; Kulakowski, P. Risk of left atrial appendage thrombus in patients scheduled for ablation for atrial fibrillation: Beyond the CHA2DS2VASc score. Pol. Arch. Med. Wewnętrznej 2015, 125, 921–928. [Google Scholar] [CrossRef] [Green Version]
- Violi, F.; Pastori, D.; Pignatelli, P. Mechanisms And Management Of Thrombo-Embolism In Atrial Fibrillation. J. Atr. Fibrill. 2014, 7, 1112. [Google Scholar]
- Asher, C.R.; Klein, A.L. The ACUTE Trial. Transesophageal echocardiography to guide electrical cardioversion in atrial fibrillation. Assessment of Cardioversion Using Transesophageal Echocardiography. Clevel. Clin. J. Med. 2002, 69, 713–718. [Google Scholar] [CrossRef]
- Fatkin, D.; Scalia, G.; Jacobs, N.; Burstow, D.; Leung, D.; Walsh, W.; Feneley, M. Accuracy of biplane transesophageal echocardiography in detecting left atrial thrombus. Am. J. Cardiol. 1996, 77, 321–323. [Google Scholar] [CrossRef]
- Manning, W.J.; Weintraub, R.M.; Waksmonski, C.A.; Haering, J.M.; Rooney, P.S.; Maslow, A.D.; Johnson, R.G.; Douglas, P.S. Accuracy of transesophageal echocardiography for identifying left atrial thrombi: A prospective, intraoperative study. Ann. Intern. Med. 1995, 123, 817–822. [Google Scholar] [CrossRef]
- Hart, R.G.; Benavente, O.; McBride, R.; Pearce, L.A. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: A meta-analysis. Ann. Intern. Med. 1999, 131, 492–501. [Google Scholar] [CrossRef]
- Al-Saady, N.M.; Obel, O.A.; Camm, A.J. Left atrial appendage: Structure, function, and role in thromboembolism. Heart 1999, 82, 547–554. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidenbuchel, H.; Hendriks, J.; et al. ESC Scientific Document Group 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014, 64, 2246–2280. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.; Frison, L.; Halperin, J.L.; Lane, A. Identifying patients at high risk for stroke despite anticoagulation: A comparison of contemporary stroke risk stratification schemes in an anticoagulated atrial fibrillation cohort. Stroke J. Cereb. Circ. 2010, 41, 2731–2738. [Google Scholar] [CrossRef] [Green Version]
- Wallace, T.W.; Atwater, B.D.; Daubert, J.P.; Voora, D.; Crowley, A.L.; Bahnson, T.D.; Hranitzky, P.M. Prevalence and clinical characteristics associated with left atrial appendage thrombus in fully anticoagulated patients undergoing catheter-directed atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 2010, 21, 849–852. [Google Scholar] [CrossRef]
- Zylla, M.M.; Pohlmeier, M.; Hess, A.; Mereles, D.; Kieser, M.; Bruckner, T.; Scholz, E.; Zitron, E.; Schweizer, P.A.; Katus, H.A.; et al. Prevalence of intracardiac thrombi under phenprocoumon, direct oral anticoagulants (dabigatran and rivaroxaban), and bridging therapy in patients with atrial fibrillation and flutter. Am. J. Cardiol. 2015, 115, 635–640. [Google Scholar] [CrossRef]
- Kosmalska, K.; Rzyman, M.; Miekus, P.; Gilis-Malinowska, N.; Nowak, R.; Fijalkowski, M. Usefulness of transesophageal echocardiography before cardioversion in atrial arrhythmias. Cardiol. J. 2021, 28, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstron-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Pepi, M.; Evangelista, A.; Nihoyannopoulos, P.; Flachskampf, F.A.; Athanassopoulos, G.; Colonna, P.; Habib, G.; Ringelstein, E.B.; Sicari, R.; Caso, P.; et al. Recommendations for echocardiography use in the diagnosis and management of cardiac sources of embolism: European Association of Echocardiography (EAE) (a registered branch of the ESC). Eur. J. Echocardiogr. 2010, 11, 461–476. [Google Scholar] [CrossRef] [Green Version]
- Saric, M.; Armour, A.C.; Arnaout, M.S.; Chaudhry, F.A.; Grimm, R.A.; Kronzon, I.; Landeck, B.F.; Maganti, K.; Michelena, H.; Tolstrup, K. Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism. J. Am. Soc. Echocardiogr. 2016, 29, 1–42. [Google Scholar] [CrossRef] [Green Version]
- Flachskampf, F.A.; Badano, L.; Daniel, W.G.; Feneck, R.O.; Fox, K.F.; Fraser, A.G.; Pasquet, A.; Pepi, M.; Perez de Isla, L.; Zamorano, J.L. Recommendations for transoesophageal echocardiography: Update 2010. Eur. J. Echocardiogr. J. 2010, 11, 557–576. [Google Scholar] [CrossRef] [Green Version]
- Fatkin, D.; Loupas, T.; Jacobs, N.; Feneley, M.P. Quantification of blood echo- genicity: Evaluation of a semiquantitative method of grading spontaneous echo contrast. Ultrasound Med. Biol. 1995, 21, 1191–1198. [Google Scholar] [CrossRef]
- Scherr, D.; Dalal, D.; Chilukuri, K.; Dong, J.; Spragg, D.; Henrikson, C.A.; Nazarian, S.; Cheng, A.; Berger, R.D.; Abraham, T.P.; et al. Incidence and predictors of left atrial thrombus prior to catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 2009, 20, 379–384. [Google Scholar] [CrossRef]
- Lip, G.Y.; Hammerstingl, C.; Marin, F.; Cappato, R.; Meng, I.L.; Kirsch, B.; Eickels, M.; Cohen, A. Left atrial thrombus resolution in atrial fibrillation or flutter: Results of a prospective study with rivaroxaban (X-TRA) and a retrospective observational registry providing baseline data (CLOT-AF). Am. Heart J. 2016, 178, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Fatkin, D.; Kelly, R.P.; Feneley, M.P. Relations between left atrial appendage blood flow velocity, spontaneous echocardiographic contrast and thromboembolic risk in vivo. J. Am. Coll. Cardiol. 1994, 23, 961–969. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, P.; Schmidt, H.; Hammerstingl, C.; Luderitz, B.; Omran, H. Patients with atrial fibrillation and dense spontaneous echo contrast at high risk a prospective and serial follow-up over 12 months with transesophageal echocardiography and cerebral magnetic resonance imaging. J. Am. Coll. Cardiol. 2005, 45, 1807–1812. [Google Scholar] [CrossRef] [Green Version]
- Kaplon-Cieslicka, A.; Budnik, M.; Gawalko, M.; Wojcik, M.; Blaszczyk, R.; Uzieblo-Zyczkowska, B.; Krzesinski, P.; Starzyk, K.; Gorczyca, I.; Szymanska, A.; et al. The rationale and design of the LATTEE registry—The first multicenter project on the Scientific Platform of the “Club 30” of the Polish Cardiac Society. Kardiol. Pol. 2019, 22, 1078–1080. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Thrombus or Sludge (+) n = 77 | Thrombus or Sludge (−) n = 190 | p | |
|---|---|---|---|
| Clinical | |||
| Age (years) | 74.99 ± 8.17 | 73.01 ± 10.19 | 1.000 |
| Female sex, n (%) | 42 (54.54) | 82 (43.16) | 0.092 |
| BMI (kg/m2) | 29.06 ± 5.35 | 29.11 ± 4.94 | 0.942 |
| CHA2DS2VASc | 4.70 (4.00–6.00) | 4.00 (3.00–5.00) | 0.101 |
| CHA2DS2VASc > 3, n (%) | 61 (79.22) | 138 (72.63) | 0.264 |
| First episode of AF/AFL, n (%) | 23 (29.87) | 92 (48.42) | 0.006 |
| Atrial flutter, n (%) | 12 (15.58) | 41 (21.58) | 0.267 |
| Arterial hypertension, n (%) | 63 (81.82) | 147 (77.37) | 0.422 |
| Diabetes, n (%) | 35 (45.45) | 68 (35.79) | 0.142 |
| Previous stroke/TIA, n (%) | 17 (22.08) | 42 (22.11) | 0.996 |
| Congestive heart failure, n (%) | 39 (50.65) | 72 (37.89) | 0.056 |
| Current smoking, n (%) | 4 (5.19) | 7 (3.68) | 0.574 |
| Echocardiography | |||
| LVEF (%) | 43.36 ± 12.48 | 46.24 ± 11.72 | 0.075 |
| LA area (cm2) | 30.18 ± 10.26 | 27.05 ± 5.22 | 1.000 |
| LA spontaneous echocontrast, n (%) | 56 (72.73) | 62 (32.63) | <0.001 |
| Low LAA velocities < 20 cm/s, n (%) | 68 (88.31) | 113 (59.47) | <0.0001 |
| Aortic stenosis moderate-to-severe, n (%) | 4 (5.19) | 13 (6.84) | 0.618 |
| Aortic regurgitation moderate-to-severe, n (%) | 2 (2.60) | 6 (3.16) | 0.808 |
| Mitral stenosis moderate-to-severe, n (%) | 3 (3.90) | 1 (0.53) | 0.040 |
| Mitral regurgitation moderate-to-severe, n (%) | 18 (23.38) | 50 (26.32) | 0.618 |
| Laboratory | |||
| Creatinine (mg/dL) | 0.99 ± 0.38 | 1.01 ± 0.41 | 0.713 |
| Hematocrit (%) | 40.46 ± 4.54 | 40.63 ± 4.68 | 0.787 |
| Platelets (G/L) | 213.19 ± 54.87 | 220.07 ± 82.79 | 0.503 |
| INR | 1.90 ± 0.89 | 1.73 ± 0.72 | 1.000 |
| aPTT ratio | 1.34 ± 0.40 | 1.30 ± 0.33 | 1.000 |
| Anticoagulation | |||
| Anticoagulation, n (%) | 70 (90.91) | 168 (88.42) | 0.555 |
| NOAC, n (%) | 37 (48.05) | 122 (64.21) | 0.015 |
| Anticoagulation interruption in last three months, n (%) | 12 (15.58) | 11 (5.79) | 0.010 |
| Thrombus/Sludge (+) n = 77 | Thrombus/Sludge (−) n = 190 | p | |
|---|---|---|---|
| Ischemic stroke event (%) | 13 (17%) | 2 (1%) | <0.001 |
| One-year mortality (%) | 18 (23%) | 3 (1.6%) | <0.001 |
| Sludge (+) n = 19 | No Thrombus or Sludge n = 190 | p | |
| Ischemic stroke event (%) | 2 (11%) | 2 (1%) | 0.042 |
| One-year mortality (%) | 2 (11%) | 3 (1.6%) | 0.066 |
| Sludge n = 19 | Thrombus n = 58 | p | |
| Ischemic stroke event (%) | 2 (11%) | 9 (16%) | 0.722 |
| One-year mortality (%) | 3 (16%) | 14 (24%) | 0.539 |
| Thrombus resolution (+) n = 26 | Thrombus resolution (−) n = 16 | p | |
| Ischemic stroke event (%) | 2 (8%) | 2 (12%) | 0.628 |
| One-year mortality (%) | 4 (15%) | 4 (25%) | 0.454 |
| LMWH n = 11 | OAC n = 31 | p | |
| Ischemic stroke event (%) | 1 (9%) | 4 (13%) | 1.000 |
| One-year mortality (%) | 2 (18%) | 5 (16%) | 1.000 |
| TOE control (+) (Intension for thrombus resolution); n = 43 | TOE control (−) n = 34 | p | |
| Ischemic stroke event (%) | 4 (9%) | 7 (21%) | 0.198 |
| One-year mortality (%) | 7 (16%) | 10 (29%) | 0.181 |
| Sludge n = 19 | Thrombus n = 58 | p | |
|---|---|---|---|
| Clinical | |||
| Age (years) | 75.5 ± 9.3 | 74.8 ± 7.9 | 0.756 |
| Female sex, n (%) | 9 (47.4) | 33 (56.9) | 0.469 |
| BMI (kg/m2) | 27.7 ± 4.0 | 29.5 ± 5.7 | 0.197 |
| CHA2DS2VASc | 4.7 ± 1.4 5.0 (4.0–6.0) | 4.7 ± 1.5 5.0 (4.0–6.0) | 0.942 |
| CHA2DS2VASc > 3, n (%) | 16 (84.2) | 45 (78.9) | 0.618 |
| First episode of AF/AFL, n (%) | 6 (31.6) | 17 (31.5) | 0.994 |
| Atrial flutter, n (%) | 4 (21.1) | 8 (14.3) | 0.486 |
| Arterial hypertension, n (%) | 16 (84.2) | 47 (82.5) | 1.000 |
| Diabetes, n (%) | 9 (47.4) | 26 (45.6) | 0.894 |
| Previous stroke/TIA, n (%) | 3 (15.8) | 14 (24.6) | 0.537 |
| Congestive heart failure, n (%) | 10 (52.6) | 29 (50.9) | 0.895 |
| Current smoking, n (%) | 1 (5.3) | 3 (5.3) | 1.000 |
| Echocardiography | |||
| LVEF (%) | 44.0 ± 11.5 | 43.1 ± 12.9 | 0.779 |
| LA area (cm2) | 29.1 ± 4.9 | 30.7 ± 12.0 | 0.620 |
| LA presence of spontaneous echocontrast, n (%) | 16 (84.2) | 40 (70.2) | 0.229 |
| Low LAA velocities < 20 cm/s, n (%) | 19 (100.0) | 49 (86.0) | 0.189 |
| Aortic stenosis moderate-to-severe, n (%) | 2 (10.5) | 2 (3.4) | 0.253 |
| Aortic regurgitation moderate-to-severe, n (%) | 1 (5.3) | 1 (1.7) | 0.435 |
| Mitral stenosis moderate-to-severe, n (%) | 0 (0.0) | 3 (5.2) | 0.571 |
| Mitral regurgitation moderate-to-severe, n (%) | 4 (21.1) | 14 (24.1) | 1.000 |
| Laboratory | |||
| Creatinine (mg/dL) | 0.9 ± 0.3 | 1.0 ± 0.4 | 0.447 |
| Hematocrit (%) | 40.2 ± 4.4 | 40.5 ± 4.6 | 0.798 |
| Platelets (G/L) | 236.8 ± 62.4 | 205.0 ± 50.1 | 0.055 |
| INR | 1.8 ± 0.8 | 1.9 ± 0.9 | 0.645 |
| aPTT ratio | 1.3 ± 0.3 | 1.4 ± 0.4 | 0.603 |
| Anticoagulation | |||
| Anticoagulation, n (%) | 19 (100.0) | 52 (92.9) | 0.567 |
| NOAC, n (%) | 10 (52.6) | 27 (46.6) | 0.645 |
| Anticoagulation interruption in last three months, n (%) | 5 (26.3) | 7 (14.6) | 0.299 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosmalska, K.; Gilis-Malinowska, N.; Rzyman, M.; Danilowicz-Szymanowicz, L.; Fijalkowski, M. Risk of Death and Ischemic Stroke in Patients with Atrial Arrhythmia and Thrombus or Sludge in Left Atrial Appendage at One-Year Follow-Up. J. Clin. Med. 2022, 11, 1128. https://doi.org/10.3390/jcm11041128
Kosmalska K, Gilis-Malinowska N, Rzyman M, Danilowicz-Szymanowicz L, Fijalkowski M. Risk of Death and Ischemic Stroke in Patients with Atrial Arrhythmia and Thrombus or Sludge in Left Atrial Appendage at One-Year Follow-Up. Journal of Clinical Medicine. 2022; 11(4):1128. https://doi.org/10.3390/jcm11041128
Chicago/Turabian StyleKosmalska, Katarzyna, Natasza Gilis-Malinowska, Malgorzata Rzyman, Ludmila Danilowicz-Szymanowicz, and Marcin Fijalkowski. 2022. "Risk of Death and Ischemic Stroke in Patients with Atrial Arrhythmia and Thrombus or Sludge in Left Atrial Appendage at One-Year Follow-Up" Journal of Clinical Medicine 11, no. 4: 1128. https://doi.org/10.3390/jcm11041128
APA StyleKosmalska, K., Gilis-Malinowska, N., Rzyman, M., Danilowicz-Szymanowicz, L., & Fijalkowski, M. (2022). Risk of Death and Ischemic Stroke in Patients with Atrial Arrhythmia and Thrombus or Sludge in Left Atrial Appendage at One-Year Follow-Up. Journal of Clinical Medicine, 11(4), 1128. https://doi.org/10.3390/jcm11041128