
Riociguat in Patients with CTEPH and Advanced Age and/or Comorbidities

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Procedures
2.4. Statistical Analysis
3. Results
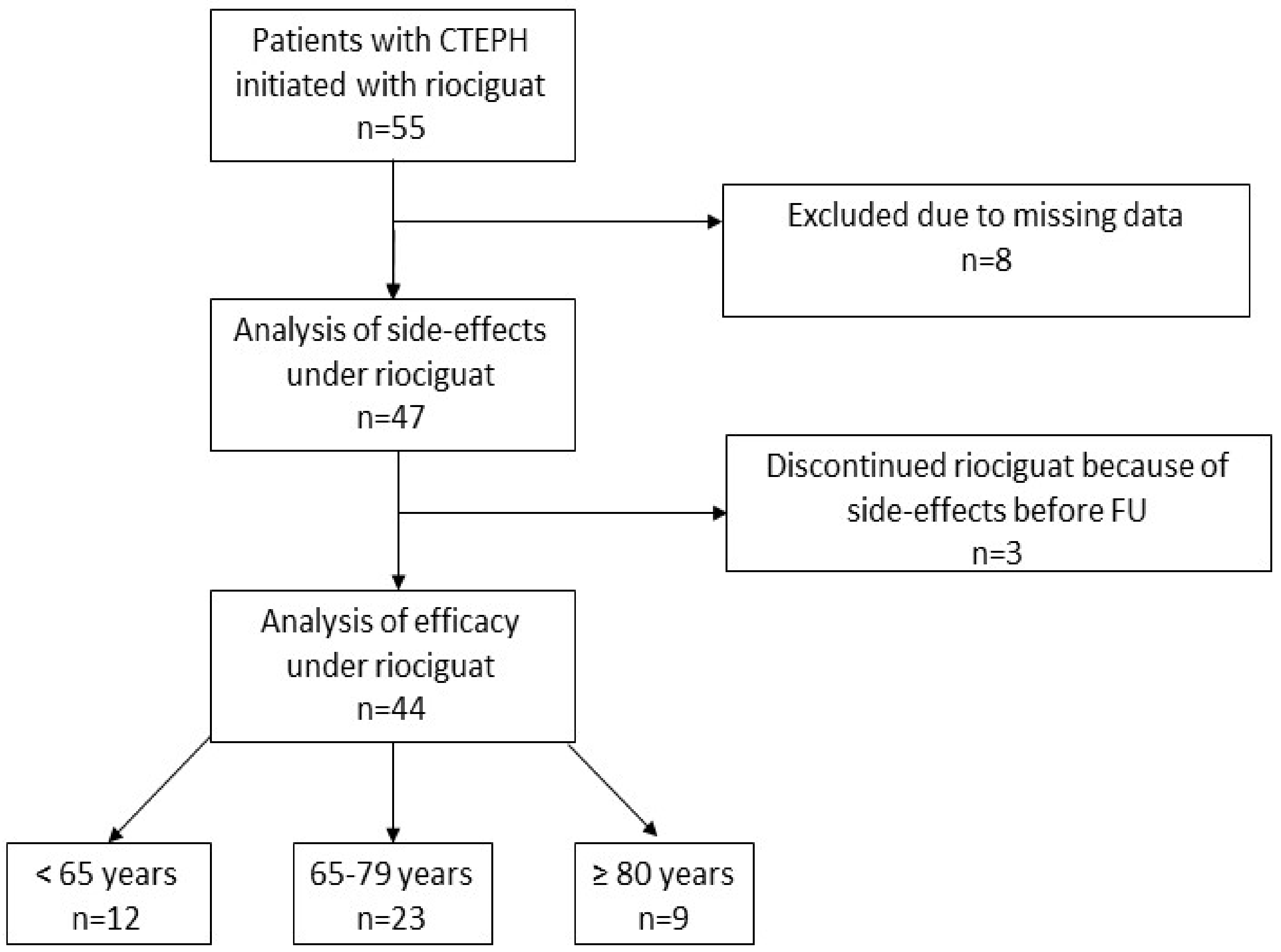
3.1. Study Cohort
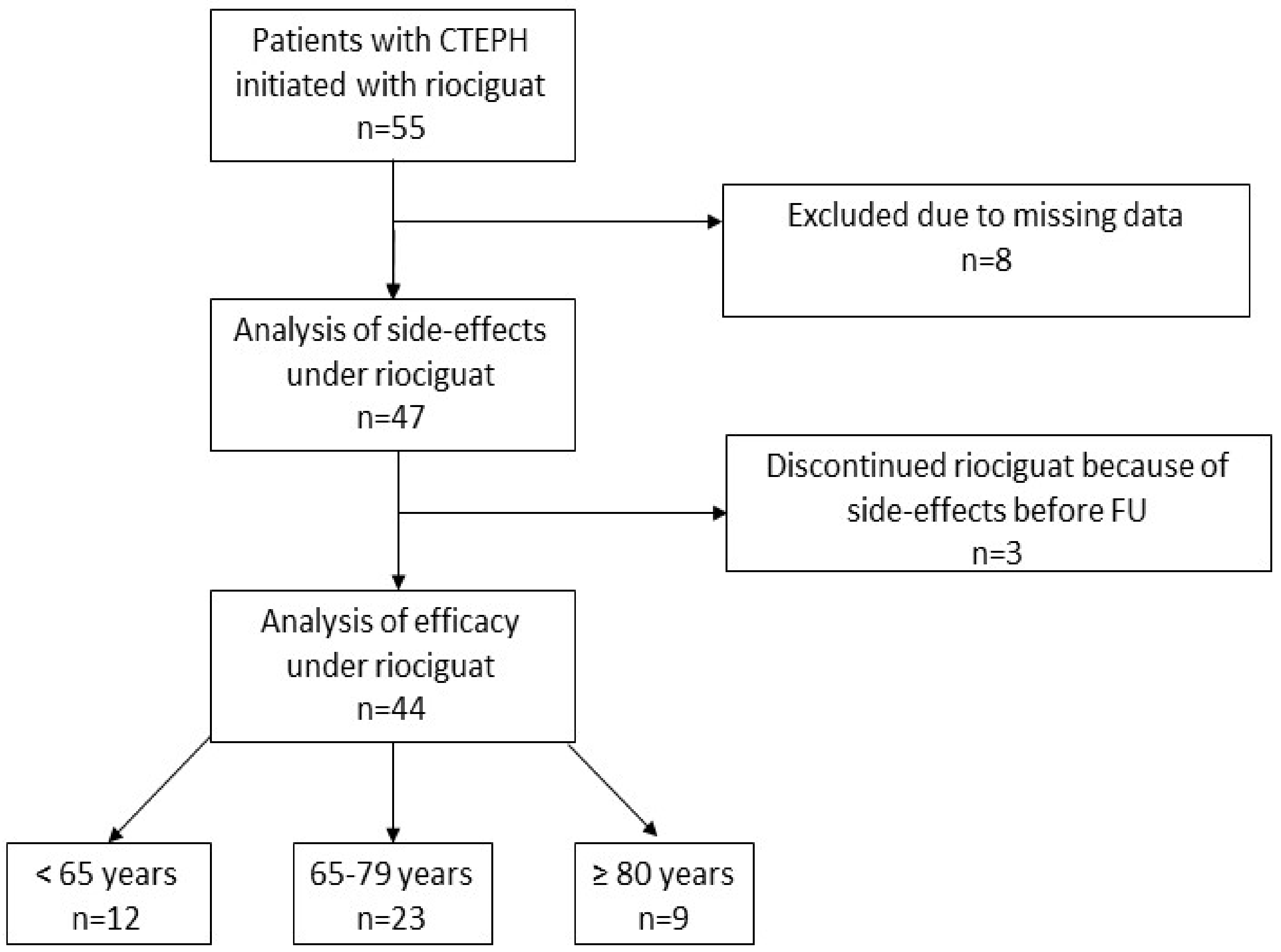
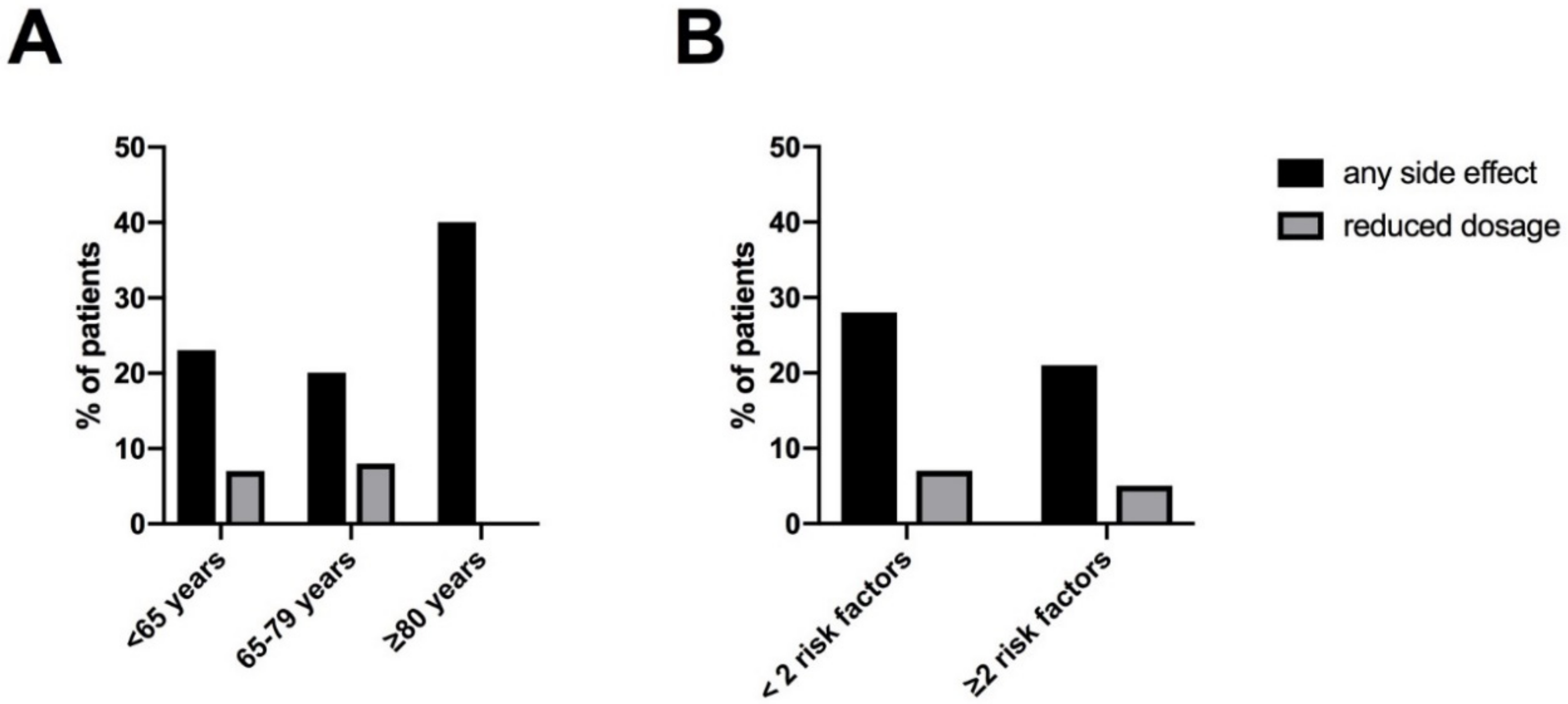
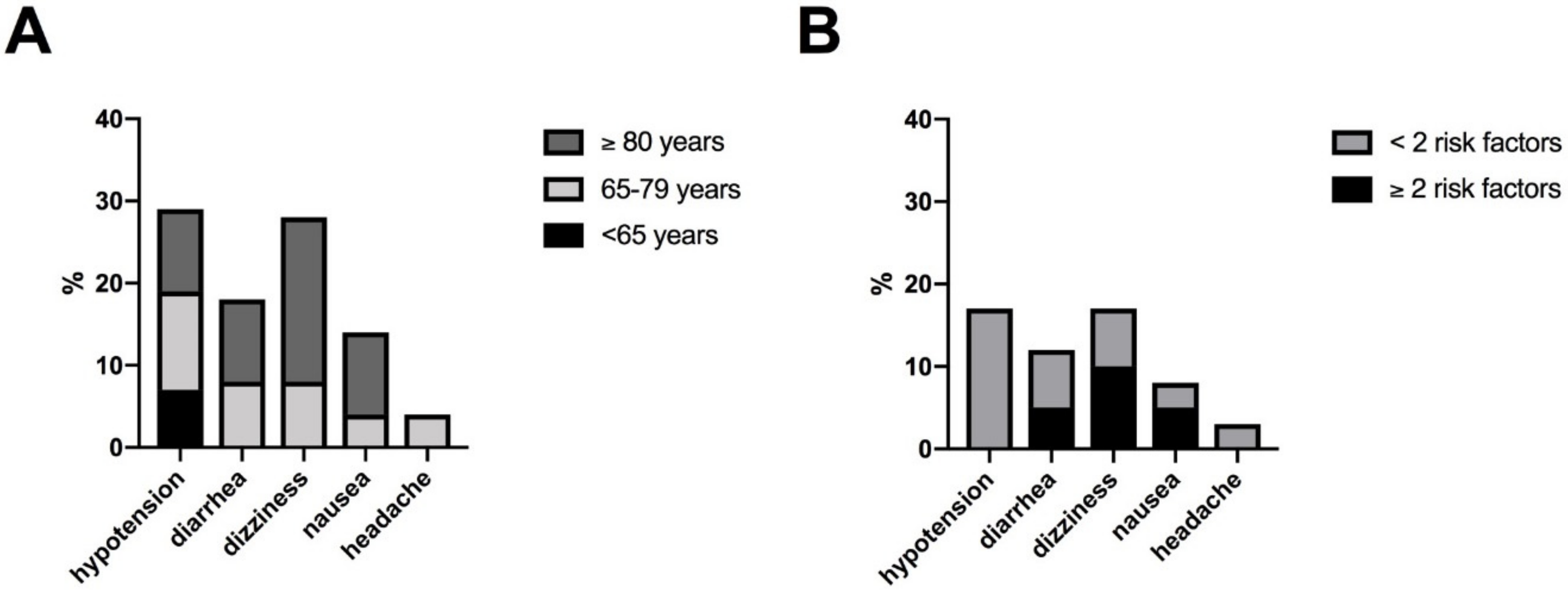
3.2. Safety
3.3. Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simonneau, G.; Montani, D.; Celermajer, D.S.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; Williams, P.G.; Souza, R. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801913. [Google Scholar] [CrossRef] [PubMed]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [PubMed]
- Stasch, J.P.; Pacher, P.; Evgenov, O.V. Soluble guanylate cyclase as an emerging therapeutic target in cardiopulmonary disease. Circulation 2011, 123, 2263–2273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghofrani, H.A.; Galie, N.; Grimminger, F.; Grunig, E.; Humbert, M.; Jing, Z.C.; Keogh, A.M.; Langleben, D.; Kilama, M.O.; Fritsch, A.; et al. Riociguat for the treatment of pulmonary arterial hypertension. N. Engl. J. Med. 2013, 369, 330–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghofrani, H.A.; D’Armini, A.M.; Grimminger, F.; Hoeper, M.M.; Jansa, P.; Kim, N.H.; Mayer, E.; Simonneau, G.; Wilkins, M.R.; Fritsch, A.; et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N. Engl. J. Med. 2013, 369, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Characteristics EMAEsop. Available online: https://www.ema.europa.eu/en/documents/product-information/adempas-epar-product-information_en.pdf (accessed on 27 November 2020).
- Hoeper, M.M.; Halank, M.; Wilkens, H.; Gunther, A.; Weimann, G.; Gebert, I.; Leuchte, H.H.; Behr, J. Riociguat for interstitial lung disease and pulmonary hypertension: A pilot trial. Eur. Respir. J. 2013, 41, 853–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghofrani, H.A.; Staehler, G.; Grunig, E.; Halank, M.; Mitrovic, V.; Unger, S.; Mueck, W.; Frey, R.; Grimminger, F.; Schermuly, R.T.; et al. Acute effects of riociguat in borderline or manifest pulmonary hypertension associated with chronic obstructive pulmonary disease. Pulm. Circ. 2015, 5, 296–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonderman, D.; Ghio, S.; Felix, S.B.; Ghofrani, H.A.; Michelakis, E.; Mitrovic, V.; Oudiz, R.J.; Boateng, F.; Scalise, A.V.; Roessig, L.; et al. Riociguat for patients with pulmonary hypertension caused by systolic left ventricular dysfunction: A phase IIb double-blind, randomized, placebo-controlled, dose-ranging hemodynamic study. Circulation 2013, 128, 502–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, D.P.; Biederman, A.; D’Armini, A.M.; Dartevelle, P.G.; Gan, H.L.; Klepetko, W.; Lindner, J.; Mayer, E.; Madani, M.M. Operability assessment in CTEPH: Lessons from the CHEST-1 study. J. Thorac. Cardiovasc. Surg. 2016, 152, 669–674.e663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yu, X.; Jin, Q.; Luo, Q.; Zhao, Z.; Zhao, Q.; Yan, L.; Liu, Z. Advances in targeted therapy for chronic thromboembolic pulmonary hypertension. Heart Fail. Rev. 2019, 24, 949–965. [Google Scholar] [CrossRef] [PubMed]
- Pepke-Zaba, J.; Jais, X.; Channick, R. Medical Therapy in Chronic Thromboembolic Pulmonary Hypertension. Ann. Am. Thorac. Soc. 2016, 13 (Suppl. S3), S248–S254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeper, M.M.; Al-Hiti, H.; Benza, R.L.; Chang, S.A.; Corris, P.A.; Gibbs, J.S.R.; Grünig, E.; Jansa, P.; Klinger, J.R.; Langleben, D.; et al. Switching to riociguat versus maintenance therapy with phosphodiesterase-5 inhibitors in patients with pulmonary arterial hypertension (REPLACE): A multicentre, open-label, randomised controlled trial. Lancet Respir. Med. 2021, 9, 573–584. [Google Scholar] [CrossRef]
- Wilkens, H.; Konstantinides, S.; Lang, I.M.; Bunck, A.C.; Gerges, M.; Gerhardt, F.; Grgic, A.; Grohé, C.; Guth, S.; Held, M.; et al. Chronic thromboembolic pulmonary hypertension (CTEPH): Updated Recommendations from the Cologne Consensus Conference 2018. Int. J. Cardiol. 2018, 272, 69–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeper, M.M.; Apitz, C.; Grünig, E.; Halank, M.; Ewert, R.; Kaemmerer, H.; Kabitz, H.J.; Kähler, C.; Klose, H.; Leuchte, H.; et al. Targeted therapy of pulmonary arterial hypertension: Updated recommendations from the Cologne Consensus Conference 2018. Int. J. Cardiol. 2018, 272, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitbon, O.; Howard, L. Management of pulmonary arterial hypertension in patients aged over 65 years. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2019, 21, K29–K36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeper, M.M.; Simonneau, G.; Corris, P.A.; Ghofrani, H.A.; Klinger, J.R.; Langleben, D.; Naeije, R.; Jansa, P.; Rosenkranz, S.; Scelsi, L.; et al. RESPITE: Switching to riociguat in pulmonary arterial hypertension patients with inadequate response to phosphodiesterase-5 inhibitors. Eur. Respir. J. 2017, 50, 1602425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, I.M.; Palazzini, M. The burden of comorbidities in pulmonary arterial hypertension. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 2019, 21, K21–K28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Thor, M.C.J.; Ten Klooster, L.; Snijder, R.J.; Post, M.C.; Mager, J.J. Long-term clinical value and outcome of riociguat in chronic thromboembolic pulmonary hypertension. Int. J. Cardiol. Heart Vasc. 2019, 22, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Grimminger, F.; Grünig, E.; Hoeper, M.M.; Humbert, M.; Jing, Z.C.; Keogh, A.M.; Langleben, D.; Rubin, L.J.; Fritsch, A.; et al. Comparison of hemodynamic parameters in treatment-naïve and pre-treated patients with pulmonary arterial hypertension in the randomized phase III PATENT-1 study. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2017, 36, 509–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Total | <65 Years | 65–79 Years | ≥80 Years | p-Value | |
|---|---|---|---|---|---|
| n = 47 | n = 13 | n = 24 | n = 10 | ||
| Female, n (%) | 29 (62) | 6 (46) | 18 (75) | 5 (50) | |
| Age (years) | 69 ± 14 | 51 ± 12 | 73 ± 5 | 82 ± 2 | <0.0001 |
| BMI (kg/m2) | 26 ± 5 | 25 ± 5 | 28 ± 6 | 24 ± 4 | 0.10 |
| BMI ≥ 30 kg/m2, n (%) | 12 (26) | 3 (23) | 7 (30) | 0 (0) | 0.16 |
| Surgical/Interventional treatment prior baseline and riociguat initiation, n (%) | |||||
| Pulmonary endarterectmoty (PEA) | 6 (13) | 1 (8) | 5 (21) | 0 (0) | |
| No PEA | 41 (87) | 12 (92) | 19 (79) | 10 (100) | |
| Technically inoperable | 17 (36) | 9 (69) | 6 (25) | 2 (20) | |
| Medically inoperable | 14 (30) | 3 (23) | 7 (29) | 4 (40) | |
| Surgery refused by patient | 8 (17) | 0 (0) | 6 (25) | 2 (20) | |
| No surgery for unknown reason | 2 (4) | 0 (0) | 0 (0) | 2 (20) | |
| No PEA, but balloon angioplasty | 1 (2) | 0 (0) | 1 (4) | 0 (0) | |
| Prior PH medication, n (%) | |||||
| None | 39 (83) | 10 (77) | 20 (83) | 9 (90) | 0.71 |
| ERA add on riociguat | 2 (4) | 2 (15) | 0 (0) | 0 (0) | 0.06 |
| Switch PDE 5-inhibitor to riociguat | 6 (13) | 2 (15) | 3 (13) | 1 (1) | 0.93 |
| Switch ERA to riociguat | 1 (2) | 0 (0) | 1 (4) | 0 (0) | 0.98 |
| Comorbidities, n (%) | |||||
| COPD | 6 (13) | 1 (8) | 3 (13) | 2 (20) | 0.77 |
| ILD | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - |
| Diabetes mellitus | 4 (9) | 0 (0) | 3 (13) | 1 (10) | 0.42 |
| OSAS | 3 (6) | 1 (8) | 2 (8) | 0 (0) | 0.65 |
| Atrial fibrillation | 14 (30) | 3 (23) | 10 (42) | 1 (10) | 0.15 |
| Coronary artery disease | 9 (19) | 3 (23) | 4 (16) | 2 (20) | 0.89 |
| Arterial hypertension | 25 (53) | 2 (15) | 16 (67) | 7 (70) | 0.0057 |
| WHO-FC, n (%) | n = 44 | n = 12 | n = 22 | ||
| II | 9 (20) | 3 (25) | 5 (23) | 1 (10) | |
| III | 33 (75) | 8 (67) | 16 (73) | 9 (90) | |
| IV | 2 (5) | 1 (8) | 1 (4) | 0 (0) | |
| Clinical parameters | n = 37–45 | n = 9–13 | n = 17–23 | ||
| Nt-proBNP (pg/mL) | 1252 (47; 14,429) | 1260 (148; 7043) | 1067 (47; 5317) | 2313 (158; 14,428) | 0.45 |
| 6 mwd (m) | 321 ± 117 | 404 ± 93 | 302 ± 113 | 271 ± 110 | 0.0211 |
| paO2 (mmHg) | 58 ± 9 | 59 ± 12 | 58 ± 7 | 56 ± 8 | 0.69 |
| Echocardiography | n = 33 | n = 10 | n = 15 | n = 8 | |
| TAPSE (mm) | 17 ± 4 | 16 ± 6 | 19 ± 3 | 14 ± 4 | 0.0301 |
| RHC | n = 39–47 | n = 11–13 | n = 19–24 | n = 9–10 | |
| mPAP (mmHg) | 45 ± 12 | 49 ± 13 | 42 ± 11 | 48 ± 13 | 0.21 |
| mRAP (mmHg) | 8 ± 4 | 8 ± 4 | 7 ± 4 | 9 ± 4 | 0.43 |
| CI (L/min/m2) | 2.6 ± 0.7 | 2.5 ± 0.6 | 2.8 ± 0.7 | 2.6 ± 0.6 | 0.51 |
| PVR (WE) | 8 ± 4 | 9 ± 4 | 8 ± 5 | 9 ± 4 | 0.73 |
| SvO2 (%) | 63 ± 7 | 63 ± 7 | 64 ± 4 | 61 ± 7 | 0.49 |
| PAWP (mmHg) | 10 ± 3 | 9 ± 3 | 9 ± 4 | 10 ± 4 | 0.72 |
| Baseline | Follow-Up | ∆ | p-Value | |
|---|---|---|---|---|
| RHC, n = 40 | ||||
| mPAP (mmHg) | 45 ± 12 | 39 ± 9 | −6 ± 9 | 0.003 |
| mRAP (mmHg) | 8 ± 4 | 7 ± 3 | −1 ± 4 | 0.10 |
| CI (L/min/m2) | 2.6 ± 0.6 | 3.0 ± 0.7 | 0.4 ± 0.8 | 0.006 |
| PVR (WE) | 8 ± 4 | 5 ± 2 | −3 ± 3 | <0.0001 |
| SvO2 (%) | 63 ± 6 | 66 ± 6 | 3 ± 6 | 0.0112 |
| PAWP (mmHg) | 9 ± 4 | 10 ± 4 | 0.9 ± 4 | 0.20 |
| WHO-FC, n = 41 | ||||
| I | 0 (0) | 3 (8) | 3 | |
| II | 9 (20) | 17 (41) | 8 | |
| III | 29 (71) | 19 (46) | −10 | |
| IV | 3 (9) | 2 (5) | −1 | |
| FC Score | 117 | 102 | −15 | |
| Clinical parameters | ||||
| Nt-proBNP (pg/mL), n = 37; (range) | 1260 (47; 14,429) | 697 (58; 5115) | −336 (−9314; 1668) | 0.0039 |
| 6 mwd (m), n = 32 | 316 ± 121 | 345 ± 114 | 29 ± 63 | 0.0152 |
| paO2 (mmHg), n = 39 | 58 ± 8 | 55 ± 8 | −3 ± 6 | 0.0013 |
| Echocardiography | ||||
| TAPSE (mm), n = 25 | 17 ± 4 | 20 ± 4 | 2 ± 4 | 0.0059 |
| RAA (cm2), n = 18 | 26 ± 6 | 24 ± 5 | −2 ± 6 | 0.19 |
| <65 Years | 65–79 Years | ≥80 Years | p-Value | |
|---|---|---|---|---|
| n = 12 | n = 23 | n = 9 | ||
| RHC | n = 11–12 | n = 17–23 | ||
| ∆mPAP (mmHg) | −10 ± 14 | −4 ± 8 | −10 ± 11 | 0.19 |
| ∆mRAP (mmHg) | 2 ± 2 | −1 ± 4 | −2 ± 4 | 0.42 |
| ∆CI (L/min/m2) | 0.3 ± 0.6 | 0.3 ± 0.9 | 0.6 ± 0.7 | 0.56 |
| ∆PVR (WE) | −3 ± 3 | −2 ± 3 | −4 ± 3 | 0.45 |
| ∆SvO2 (%) | 2 ± 6 | 2 ± 5 | 5 ± 6 | 0.39 |
| ∆PAWP (mmHg) | 2 ± 6 | 1 ± 4 | −1 ± 5 | 0.43 |
| WHO-FC, n (%) | n = 10 | n = 22 | n = 9 | |
| ∆I | 2 | 1 | 0 | |
| ∆II | 2 | 1 | 5 | |
| ∆III | −4 | −1 | −5 | |
| ∆IV | 0 | −1 | 0 | |
| ∆ FC Score (% of n) | −6 (60%) | −2 (9%) | −5 (55%) | |
| Clinical parameters | n = 7–12 | n = 6–22 | n = 8–9 | |
| ∆Nt-proBNP (pg/mL) | −1247 (1063; 3074) | −43 (4588; 1668) | −1015 (−9314; 588) | 0.07 |
| ∆6 mwd (m) | 22 ± 71 | 31 ± 65 | 30 ± 60 | 0.96 |
| ∆paO2 (mmHg) | −2 ± 7 | −3 ± 14 | −1 ± 4 | 0.89 |
| Echocardiography | n = 7–9 | n = 11–13 | n = 5–6 | |
| ∆TAPSE (mm) | 3 ± 4 | 2 ± 4 | 1 ± 3 | 0.63 |
| ∆RAA (cm2) | 0 ± 0 | −3 ± 7 | −1 ± 4 | 0.71 |
| <2 Risk Factors | ≥2 Risk Factors | p-Value | |
|---|---|---|---|
| n = 26 | n = 18 | ||
| RHC | n = 18–23 | n = 13–17 | |
| ∆mPAP (mmHg) | −6 ± 10 | −6 ± 9 | 0.98 |
| ∆mRAP (mmHg) | −1 ± 3 | −2 ± 4 | 0.37 |
| ∆CI (L/min/m2) | 0.4 ± 0.9 | 0.3 ± 0.6 | 0.97 |
| ∆PVR (WE) | −3 ± 3 | −3 ± 2 | 0.83 |
| ∆SvO2 (%) | 4 ± 6 | 1 ± 6 | 0.11 |
| ∆PAWP (mmHg) | 1 ± 5 | 1 ± 5 | 0.71 |
| WHO-FC, n (%) | n = 24 | n = 17 | |
| ∆I | 3 | 0 | |
| ∆II | 5 | 3 | |
| ∆III | −6 | −4 | |
| ∆IV | −2 | 1 | |
| ∆FC score (% of n) | −13 (54%) | −2 (12%) | |
| Clinical parameters | n = 21–25 | n = 11–14 | |
| ∆Nt-proBNP (pg/mL) | −400 (−9314; 701) | −90 (−4588; 1668) | 0.39 |
| ∆6 mwd (m) | 19 ± 60 | 47 ± 68 | 0.23 |
| ∆paO2 (mmHg) | −4 ± 6 | −4 ± 6 | 0.73 |
| Echocardiography | n = 16–25 | n = 9 | |
| ∆TAPSE (mm) | 3 ± 4 | 1 ± 3 | 0.09 |
| ∆RAA (cm2) | −2 ± 4 | −2 ± 8 | 0.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barnikel, M.; Kneidinger, N.; Arnold, P.; Waelde, A.; Behr, J.; Milger, K. Riociguat in Patients with CTEPH and Advanced Age and/or Comorbidities. J. Clin. Med. 2022, 11, 1084. https://doi.org/10.3390/jcm11041084
Barnikel M, Kneidinger N, Arnold P, Waelde A, Behr J, Milger K. Riociguat in Patients with CTEPH and Advanced Age and/or Comorbidities. Journal of Clinical Medicine. 2022; 11(4):1084. https://doi.org/10.3390/jcm11041084
Chicago/Turabian StyleBarnikel, Michaela, Nikolaus Kneidinger, Paola Arnold, Andrea Waelde, Jürgen Behr, and Katrin Milger. 2022. "Riociguat in Patients with CTEPH and Advanced Age and/or Comorbidities" Journal of Clinical Medicine 11, no. 4: 1084. https://doi.org/10.3390/jcm11041084
APA StyleBarnikel, M., Kneidinger, N., Arnold, P., Waelde, A., Behr, J., & Milger, K. (2022). Riociguat in Patients with CTEPH and Advanced Age and/or Comorbidities. Journal of Clinical Medicine, 11(4), 1084. https://doi.org/10.3390/jcm11041084