
IDELVION: A Comprehensive Review of Clinical Trial and Real-World Data

 , ,
, ,
Abstract
:1. Introduction
2. The PROLONG-9FP Clinical Trial Program
2.1. Pharmacokinetics
2.2. Population Pharmacokinetics
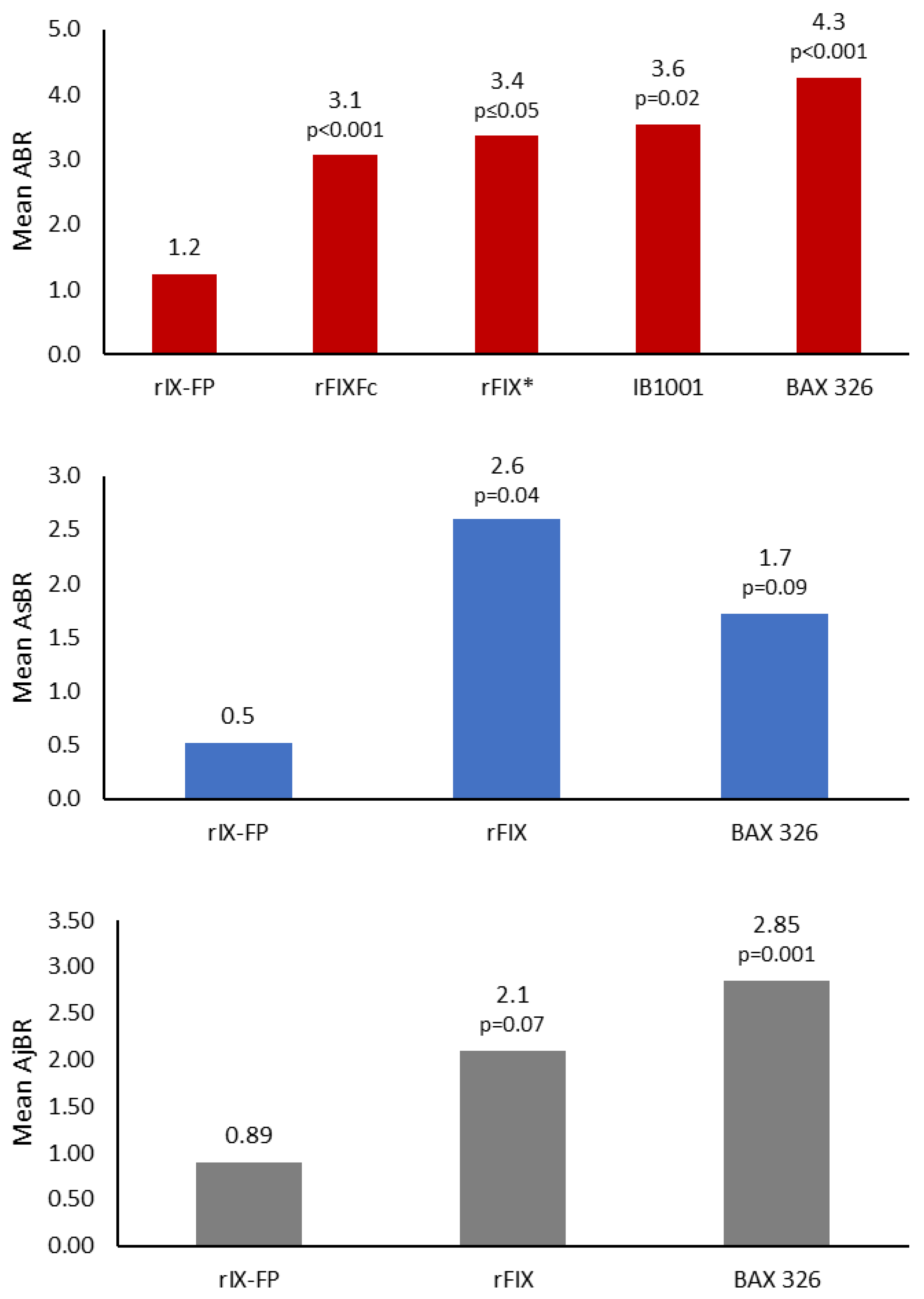
2.3. Efficacy
2.4. Consumption and Adherence
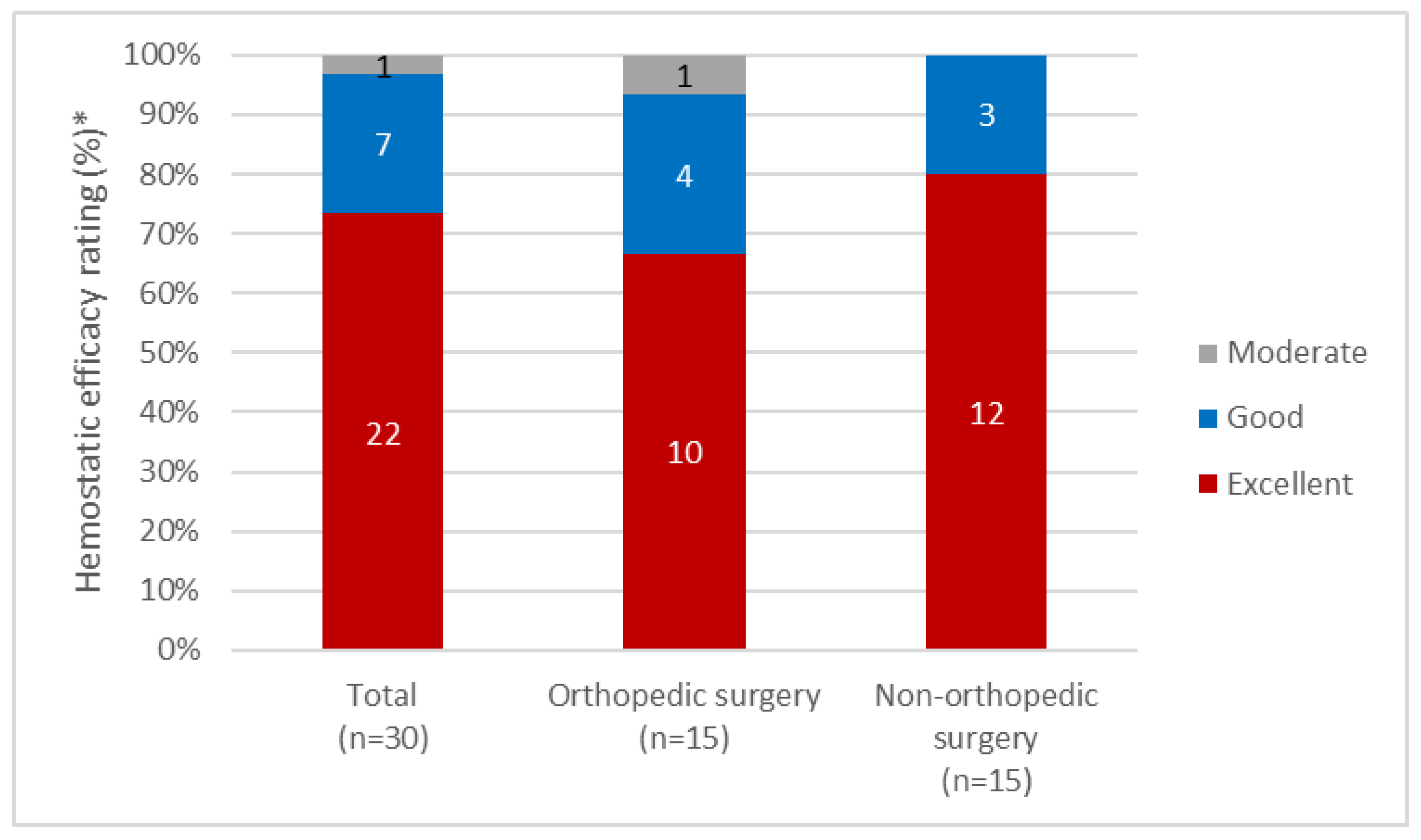
2.5. Use in Surgery
2.6. Health-Related Quality of Life
2.7. Safety
2.8. Clinical Study Data Summary
3. Clinical Experience
3.1. Biodistribution
3.2. rIX-FP in Patients with Mild/Moderate Hemophilia B
4. rIX-FP in the Clinic
4.1. Dosing
- Required dose (IU) = body weight (kg) × desired factor IX rise (% of normal or IU/dL) × {reciprocal of recovery (IU/kg per IU/dL)}
- ○
- Required increase in factor IX (IU/dL or % of normal) = dose (IU) × recovery (IU/dL per IU/kg)/body weight (kg)
4.2. Switching Patients to rIX-FP
4.3. Monitoring rIX-FP
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Srivastava, A.; Santagostino, E.; Dougall, A.; Kitchen, S.; Sutherland, M.; Pipe, S.W.; Carcao, M.; Mahlangu, J.; Ragni, M.V.; Windyga, J.; et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia 2020, 26, 1–158. [Google Scholar] [CrossRef] [PubMed]
- Stonebraker, J.S.; Bolton-Maggs, P.H.; Michael Soucie, J.; Walker, I.; Brooker, M. A study of variations in the reported haemophilia B prevalence around the world. Haemophilia 2012, 18, e91–e94. [Google Scholar] [CrossRef] [PubMed]
- Makris, M.; Oldenburg, J.; Mauser-Bunschoten, E.P.; Peerlinck, K.; Castaman, G.; Fijnvandraat, K.; The Subcommittee on Factor VIII, Factor IX and Rare Bleeding DIsorders. The definition, diagnosis and management of mild hemophilia A: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 2530–2533. [Google Scholar] [CrossRef] [PubMed]
- Castaman, G. The benefits of prophylaxis in patients with hemophilia B. Expert Rev. Hematol. 2018, 11, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Chia, J.; Louber, J.; Glauser, I.; Taylor, S.; Bass, G.T.; Dower, S.K.; Gleeson, P.A.; Verhagen, A.M. Half-life-extended recombinant coagulation factor IX-albumin fusion protein is recycled via the FcRn-mediated pathway. J. Biol. Chem. 2018, 293, 6363–6373. [Google Scholar] [CrossRef] [Green Version]
- Santagostino, E.; Negrier, C.; Klamroth, R.; Tiede, A.; Pabinger-Fasching, I.; Voigt, C.; Jacobs, I.; Morfini, M. Safety and pharmacokinetics of a novel recombinant fusion protein linking coagulation factor IX with albumin (rIX-FP) in hemophilia B patients. Blood 2012, 120, 2405–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenet, G.; Chambost, H.; Male, C.; Lambert, T.; Halimeh, S.; Chernova, T.; Mancuso, M.E.; Curtin, J.; Voigt, C.; Li, Y.; et al. Long-acting recombinant fusion protein linking coagulation factor IX with albumin (rIX-FP) in children. Results of a phase 3 trial. Thromb. Haemost. 2016, 116, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Santagostino, E.; Martinowitz, U.; Lissitchkov, T.; Pan-Petesch, B.; Hanabusa, H.; Oldenburg, J.; Boggio, L.; Negrier, C.; Pabinger, I.; von Depka Prondzinski, M.; et al. Long-acting recombinant coagulation factor IX albumin fusion protein (rIX-FP) in hemophilia B: Results of a phase 3 trial. Blood 2016, 127, 1761–1769. [Google Scholar] [CrossRef]
- Metzner, H.J.; Weimer, T.; Kronthaler, U.; Lang, W.; Schulte, S. Genetic fusion to albumin improves the pharmacokinetic properties of factor IX. Thromb. Haemost. 2009, 102, 634–644. [Google Scholar] [CrossRef]
- Nolte, M.W.; Nichols, T.C.; Mueller-Cohrs, J.; Merricks, E.P.; Pragst, I.; Zollner, S.; Dickneite, G. Improved kinetics of rIX-FP, a recombinant fusion protein linking factor IX with albumin, in cynomolgus monkeys and hemophilia B dogs. J. Thromb. Haemost. 2012, 10, 1591–1599. [Google Scholar] [CrossRef] [Green Version]
- Kenet, G.; Chambost, H.; Male, C.; Halimeh, S.; Lambert, T.; Li, Y.; Seifert, W.; Santagostino, E. Long-Term Safety and Efficacy of Recombinant Coagulation Factor IX Albumin Fusion Protein (rIX-FP) in Previously Treated Pediatric Patients with Hemophilia B: Results from a Phase 3b Extension Study. Thromb. Haemost. 2020, 120, 599–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IDELVION. (Albutrepenonacog Alfa) Summary of Product Characteristics. West Sussex, UK: CSL Behring UK Limited. 2020. Available online: https://www.ema.europa.eu/en/documents/product-information/idelvion-epar-product-information_en.pdf (accessed on 15 April 2021).
- IDELVION. (Coagulation Factor IX [Recombinant], Albumin Fusion Protein (rIX-FP) Highlights of Prescribing Information. Marburg, Germany: CSL Behring GmbH. 2020. Available online: https://labeling.cslbehring.com/PI/US/Idelvion/EN/Idelvion-Prescribing-Information.pdf (accessed on 15 April 2021).
- Mancuso, M.E.; Lubetsky, A.; Pan-Petesch, B.; Lissitchkov, T.; Nagao, A.; Seifert, W.; Li, Y.; Santagostino, E. Long-term safety and efficacy of rIX-FP prophylaxis with extended dosing intervals up to 21 days in adults/adolescents with hemophilia B. J. Thromb. Haemost. 2020, 18, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Martinowitz, U.; Lissitchkov, T.; Lubetsky, A.; Jotov, G.; Barazani-Brutman, T.; Voigt, C.; Jacobs, I.; Wuerfel, T.; Santagostino, E. Results of a phase I/II open-label, safety and efficacy trial of coagulation factor IX (recombinant), albumin fusion protein in haemophilia B patients. Haemophilia 2015, 21, 784–790. [Google Scholar] [CrossRef]
- Gill, J.C.; Roberts, J.; Li, Y.; Castaman, G. Sustained high trough factor IX activity levels with continued use of rIX-FP in adult and paediatric patients with haemophilia B. Haemophilia 2019, 25, e219–e222. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Roberts, J.; Bensen-Kennedy, D.; Jacobs, I.; Santagostino, E.; Voigt, C.; Feussner, A.; Morfini, M.; Sidhu, J. Population pharmacokinetics of a new long-acting recombinant coagulation factor IX albumin fusion protein for patients with severe hemophilia B. J. Thromb. Haemost. 2016, 14, 2132–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; McKeand, W.; Yuraszeck, T.; Seifert, W.; Feussner, A.; Santagostino, E.; Sidhu, J. Population Pharmacokinetic Analysis of Recombinant Fusion Protein Linking Coagulation Factor IX with Recombinant Albumin (rIX-FP) in Adult and Pediatric Patients with Severe Hemophilia B. Hamostaseologie 2019, 39, S1–S92. [Google Scholar] [CrossRef] [Green Version]
- Pan-Petesch, B.; Santagostino, E.; Leissinger, C.; Shapiro, A.; Oldenburg, J.; Seifert, W.; Escobar, M. Extended dosing intervals with rIX-FP prophylaxis reduces Factor IX consumption compared with previous prophylaxis regimens in clinical studies of haemophilia B patients. In Haemophilia; WILEY: Hoboken, NJ, USA, 2018; Abstract P062; Volume 24, pp. 60–61. [Google Scholar] [CrossRef] [Green Version]
- Mancuso, M.E.; Oldenburg, J.; Boggio, L.; Kenet, G.; Chan, A.; Altisent, C.; Seifert, W.; Santagostino, E. High adherence to prophylaxis regimens in haemophilia B patients receiving rIX-FP: Evidence from clinical trials and real-world practice. Haemophilia 2020, 26, 637–642. [Google Scholar] [CrossRef]
- Negrier, C.; Abdul Karim, F.; Lepatan, L.M.; Lienhart, A.; Lopez-Fernandez, M.F.; Mahlangu, J.; Pabinger, I.; Li, Y.; Wolko, D.; Voigt, C.; et al. Efficacy and safety of long-acting recombinant fusion protein linking factor IX with albumin in haemophilia B patients undergoing surgery. Haemophilia 2016, 22, e259–e266. [Google Scholar] [CrossRef]
- Curtin, J.; Santagostino, E.; Karim, F.A.; Li, Y.; Seifert, W.; Négrier, C. Simplifying surgery in haemophilia B: Low factor IX consumption and infrequent infusions in surgical procedures with rIX-FP. Thromb. Res. 2020, 188, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Pan-Petesch, B.; Nagao, A.; Abdul Karim, F.; Tosetto, A.; Alvarez-Roman, M.T.; Seifert, W.; Li, Y.; Negrier, C. Efficacy and safety of rIX-FP in surgery: An update from a phase 3b extension study. Thromb. Res. 2020, 193, 139–141. [Google Scholar] [CrossRef]
- von Mackensen, S.; Shah, J.; Seifert, W.; Kenet, G. Health-related quality of life in paediatric haemophilia B patients treated with rIX-FP. Haemophilia 2019, 25, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Yan, S.; Matsushita, T.; Alberio, L.; Bassett, P.; Santagostino, E. Systematic review and analysis of efficacy of recombinant factor IX products for prophylactic treatment of hemophilia B in comparison with rIX-FP. J. Med. Econ. 2019, 22, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.S.; Pasi, K.J.; Ragni, M.V.; Ozelo, M.C.; Valentino, L.A.; Mahlangu, J.N.; Josephson, N.C.; Perry, D.; Manco-Johnson, M.J.; Apte, S.; et al. Phase 3 Study of Recombinant Factor IX Fc Fusion Protein in Hemophilia B. N. Engl. J. Med. 2013, 369, 2313–2323. [Google Scholar] [CrossRef] [PubMed]
- Kavakli, K.; Smith, L.; Kuliczkowski, K.; Korth-Bradley, J.; You, C.W.; Fuiman, J.; Zupančić-Šalek, S.; Abdul Karim, F.; Rendo, P. Once-weekly prophylactic treatment vs. on-demand treatment with nonacog alfa in patients with moderately severe to severe haemophilia B. Haemophilia 2016, 22, 381–388. [Google Scholar] [CrossRef]
- Windyga, J.; Lissitchkov, T.; Stasyshyn, O.; Mamonov, V.; Rusen, L.; Lamas, J.L.; Oh, M.S.; Chapman, M.; Fritsch, S.; Pavlova, B.G.; et al. Pharmacokinetics, efficacy and safety of BAX326, a novel recombinant factor IX: A prospective, controlled, multicentre phase I/III study in previously treated patients with severe (FIX level <1%) or moderately severe (FIX level </= 2%) haemophilia B. Haemophilia 2014, 20, 15–24. [Google Scholar] [CrossRef]
- Collins, P.W.; Quon, D.V.K.; Makris, M.; Chowdary, P.; Kempton, C.L.; Apte, S.J.; Ramanan, M.V.; Hay, C.R.M.; Drobic, B.; Hua, Y.; et al. Pharmacokinetics, safety and efficacy of a recombinant factor IX product, trenonacog alfa in previously treated haemophilia B patients. Haemophilia 2018, 24, 104–112. [Google Scholar] [CrossRef]
- Oldenburg, J.; Yan, S.; Maro, G.; Krishnarajah, G.; Tiede, A. Assessing bleeding rates, related clinical impact and factor utilization in German hemophilia B patients treated with extended half-life rIX-FP compared to prior drug therapy. Curr. Med. Res. Opin. 2019, 36, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Hermans, C.; Marino, R.; Lambert, C.; Mangles, S.; Sommerer, P.; Rives, V.; Maro, G.; Malcangi, G. Real-World Utilisation and Bleed Rates in Patients with Haemophilia B Who Switched to Recombinant Factor IX Fusion Protein (rIX-FP): A Retrospective International Analysis. Adv. Ther. 2020, 37, 2988–2998. [Google Scholar] [CrossRef] [Green Version]
- Escobar, M.; Leissinger, C.; Yan, S.; Maro, G.; Krishnarajah, G. Comparison of rFIX utilization and bleed rates in US hemophilia B patients on rIX-FP and their prior rFIX drug. Abstract PB150. Res. Pract. Thromb. Haemost. 2018, 2, 69–70. [Google Scholar]
- Carcao, M.; Zak, M.; Abdul Karim, F.; Hanabusa, H.; Kearney, S.; Lu, M.-Y.; Persson, P.; Rangarajan, S.; Santagostino, E. Nonacog beta pegol in previously treated children with hemophilia B: Results from an international open-label phase 3 trial. J. Thromb. Haemost. 2016, 14, 1521–1529. [Google Scholar] [CrossRef] [Green Version]
- Castaman, G.; Bonetti, E.; Messina, M.; Morfini, M.; Rocino, A.; Scaraggi, F.A.; Tagariello, G.; Italian Association of Hemophilia Centers. Inhibitors in haemophilia B: The Italian experience. Haemophilia 2013, 19, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Zanon, E.; Pasca, S.; Simioni, P. The sudden and unexpected appearance of inhibitors in a previously treated severe haemophilia B patient after the switch to albutrepenonacog alpha. Haemophilia 2018, 24, e372–e375. [Google Scholar] [CrossRef] [PubMed]
- Stafford, D.W. Extravascular FIX and coagulation. Thromb. J. 2016, 14, 35. [Google Scholar] [CrossRef] [Green Version]
- Herzog, E.; Harris, S.; Henson, C.; McEwen, A.; Schenk, S.; Nolte, M.W.; Pragst, I.; Dickneite, G.; Schulte, S.; Zollner, S. Biodistribution of the recombinant fusion protein linking coagulation factor IX with albumin (rIX-FP) in rats. Thromb. Res. 2014, 133, 900–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansoor, A.; Mahabadi, N. Volume of Distribution; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Benet, L.; Sheiner, L. Pharmacokinetics: The dynamics of drug absorption, distribution, and elimination. In Goodman and Gilman’s The Pharmacologic Basis of Therapeutics; Macmillan: New York, NY, USA, 1996. [Google Scholar]
- European Medicines Agency. EMA Assessment Report for IDELVION. Available online: https://www.ema.europa.eu/documents/assessment-report/IDELVION-epar-public-assessment-report_en.pdf (accessed on 8 April 2021).
- Cooley, B.; Funkhouser, W.; Monroe, D.; Ezzell, A.; Mann, D.M.; Lin, F.-C.; Monahan, P.E.; Stafford, D.W. Prophylactic efficacy of BeneFIX vs Alprolix in hemophilia B mice. Blood 2016, 128, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Valentino, L.A.; Rusen, L.; Elezovic, I.; Smith, L.M.; Korth-Bradley, J.M.; Rendo, P. Multicentre, randomized, open-label study of on-demand treatment with two prophylaxis regimens of recombinant coagulation factor IX in haemophilia B subjects. Haemophilia 2014, 20, 398–406. [Google Scholar] [CrossRef]
- Malec, L.M.; Croteau, S.E.; Callaghan, M.U.; Sidonio, R.F., Jr. Spontaneous bleeding and poor bleeding response with extended half-life factor IX products: A survey of select US haemophilia treatment centres. Haemophilia 2020, 26, e128–e129. [Google Scholar] [CrossRef]
- Kleiboer, B.; Nielsen, B.; Ma, A.D.; Abajas, Y.; Monroe, D.M.; Key, N.S. Excessive breakthrough bleeding in haemophilia B patients on factor IX-albumin fusion protein prophylactic therapy: A single centre case series. Haemophilia 2020, 26, e23–e25. [Google Scholar] [CrossRef]
- Benson, G.; Auerswald, G.; Dolan, G.; Duffy, A.; Hermans, C.; Ljung, R.; Morfini, M.; Šalek, S.Z. Diagnosis and care of patients with mild haemophilia: Practical recommendations for clinical management. Blood Transfus. 2018, 16, 535–544. [Google Scholar] [CrossRef]
- Berntorp, E.; Dolan, G.; Hay, C.; Linari, S.; Santagostino, E.; Tosetto, A.; Castaman, G.; Álvarez-Román, M.; Parra Lopez, R.; Oldenburg, J.; et al. European retrospective study of real-life haemophilia treatment. Haemophilia 2017, 23, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Goto, M.; Takedani, H.; Yokota, K.; Haga, N. Strategies to encourage physical activity in patients with hemophilia to improve quality of life. J. Blood Med. 2016, 7, 85–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermans, C.; Kulkarni, R. Women with bleeding disorders. Haemophilia 2018, 24, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marliere, C.; Maindiaux, L.; Lambert, C.; Hermans, C. EHL-FIX in haemophilia B carriers with FIX deficiency. Haemophilia 2020, 26, e38–e40. [Google Scholar] [CrossRef] [PubMed]
- Rampotas, A.; Desborough, M.J.R.; Raza-Burton, S.; Taylor, S.; Wilkinson, A.; Hall, G.W.; Shapiro, S.; Curry, N. A single centre retrospective study of low dose prophylaxis with extended half-life factor IX for severe haemophilia B. Haemophilia 2020, 26, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Escobar, M.; Santagostino, E.; Mancuso, M.E.; Coppens, M.; Balasa, V.; Taylor, J.A.; Iorio, A.; Negrier, C. Switching patients in the age of long-acting recombinant products? Expert Rev. Hematol. 2019, 12, 1–13. [Google Scholar] [CrossRef]
- Ragni, M.V.; Croteau, S.E.; Morfini, M.; Cnossen, M.H.; Iorio, A.; The Subcommittee on Factor VIII, Factor IX and Rare Bleeding DIsorders. Pharmacokinetics and the transition to extended half-life factor concentrates: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1437–1441. [Google Scholar] [CrossRef]
- Iorio, A.; Blanchette, V.; Blatny, J.; Collins, P.; Fischer, K.; Neufeld, E. Estimating and interpreting the pharmacokinetic profiles of individual patients with hemophilia A or B using a population pharmacokinetic approach: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2017, 15, 2461–2465. [Google Scholar] [CrossRef]
- Iorio, A.; Edginton, A.N.; Blanchette, V.; Blatny, J.; Boban, A.; Cnossen, M.; Collins, P.; Croteau, S.E.; Fischer, K.; Hart, D.P.; et al. Performing and interpreting individual pharmacokinetic profiles in patients with Hemophilia A or B: Rationale and general considerations. Res. Pract. Thromb. Haemost. 2018, 2, 535–548. [Google Scholar] [CrossRef]
- McMaster University, Canada. WAPPS-Hemo. Available online: https://www.wapps-hemo.org/ (accessed on 13 May 2021).
- Dodt, J.; Hubbard, A.R.; Wicks, S.J.; Gray, E.; Neugebauer, B.; Charton, E.; Silvester, G. Potency determination of factor VIII and factor IX for new product labelling and postinfusion testing: Challenges for caregivers and regulators. Haemophilia 2015, 21, 543–549. [Google Scholar] [CrossRef]
- Bowyer, A.E.; Hillarp, A.; Ezban, M.; Persson, P.; Kitchen, S. Measuring factor IX activity of nonacog beta pegol with commercially available one-stage clotting and chromogenic assay kits: A two-center study. J. Thromb. Haemost. 2016, 14, 1428–1435. [Google Scholar] [CrossRef]
- Rosén, P.; Rosén, S.; Ezban, M.; Persson, E. Overestimation of N-glycoPEGylated factor IX activity in a one-stage factor IX clotting assay owing to silica-mediated premature conversion to activated factor IX. J. Thromb. Haemost. 2016, 14, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Sommer, J.M.; Buyue, Y.; Bardan, S.; Peters, R.T.; Jiang, H.; Kamphaus, G.D.; Gray, E.; Pierce, G.F. Comparative field study: Impact of laboratory assay variability on the assessment of recombinant factor IX Fc fusion protein (rFIXFc) activity. Thromb. Haemost. 2014, 112, 932–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, M.H.; Andersen, S.; Ezban, M. Factor IX-deficient plasma spiked with N9-GP behaves similarly to N9-GP post-administration clinical samples in N9-GP ELISA and FIX activity assays. Haemophilia 2015, 21, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, A.R.; Dodt, J.; Lee, T.; Mertens, K.; Seitz, R.; Srivastava, A.; Weinstein, M. Recommendations on the potency labelling of factor VIII and factor IX concentrates. J. Thromb. Haemost. 2013, 11, 988–989. [Google Scholar] [CrossRef]
- Horn, C.; Negrier, C.; Kalina, U.; Seifert, W.; Friedman, K.D. Performance of a recombinant fusion protein linking coagulation factor IX with recombinant albumin in one-stage clotting assays. J. Thromb. Haemost. 2019, 17, 138–148. [Google Scholar] [CrossRef] [Green Version]
- CSL Behring. Idelvion Prescribing Information. Available online: https://www.idelvion.com/prescribing-information (accessed on 21 January 2022).


{kind=link}
{kind=link}
{kind=link}
| Single Dose rIX-FP | Patients ≥ 12 Years of Age | Patients < 12 Years of Age | |||
|---|---|---|---|---|---|
| Phase I [6] | Phase II [15] | Phase III [8] | Phase IIIb Extension [14] | Phase III [7] | |
| Dose (IU/kg) | 50 | 25 | 50 | 100 | 50 |
| Mean terminal half-life, hours | 92 | 94.8 | 102 | 143 | 91 |
| Mean FIX activity at 7 days, IU/dL | 13.4 a | 5.6 b | >5.0 b | NR | >5.0 b |
| Mean incremental recovery, IU/dL per IU/kg | 1.38 | 1.52 | 1.27 | 1.02 | 1.01 |
| Mean clearance, mL/h per kg | 0.75 | NR | 0.77 | 0.66 | 1.11 |
| rIX-FP Prophylaxis | Patients ≥ 12 Years of Age | Patients < 12 Years of Age | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Phase III [8] | Phase IIIb Extension [14] | Phase III [7] | Phase IIIb Extension [11] | ||||||||
| Dose Regimen a | 7-Day | 10-Day b | 14-Day b | 7-Day | 10-Day | 14-Day | 21-Day c | 7-Day | 7-Day d | 10-Day e | 14-Day e |
| N | 40 | 7 | 21 | 22 | 17 | 41 | 11 | 27 | 21 | 8 | 8 |
| Median dose, IU/kg | 40 | 75 f | 75 f | 49.7 (range: 19–90) | 74.3 (range: 38–86) | 74.9 (range: 7–106) | 99.8 (range: 85, 111) | 47.2 (IQR: 40.6–55.8) | 49.0 (range: 22–86) | 74.0 (range: 40–82) | 73.7 (range: 56–82) |
| Mean consumption, IU/kg/month (SD) | 202.7 (47.9) | 201.5 (42.56) | 157.4 (16.3) | 206.4 (43.4) | 212.3 (26.3) | 158.0 (17.9) | 146.9 (5.5) | 205.1 (41.2) g,h | 231.2 (42.0) h | 224.2 (58.4) h | 185.4 (24.0) h |
| Median AsBR (Q1, Q3) | 0 (0, 0) | 0 (0, 0) | 0 (0, 1.0) | 0 (0, 1.7) | 0.3 (0, 1.1) | 0.4 (0, 1.7) | 0 (0, 0.5) | 0 (0, 0.9) | 0 (0, 0.5) | 0 (0, 2.8) | 1.1 (0, 3.4) |
| Median ABR (Q1, Q3) | 0.0 (0, 1.9) | 0 (0, 1.8) | 1.1 (0, 2.7) | 1.3 (0.4, 4.2) | 0.8 (0.3, 4.9) | 0.9 (0, 2.9) | 0.3 (0, 2.5) | 3.1 (0.9, 5.9) | 2.0 (0.7, 4.7) | 3.5 (0.8, 6.7) | 5.6 (2.0, 6.9) |
| Median AjBR (Q1, Q3) | 0 (0, 1.5) | 0 (0, 0.9) | 0 (0, 1.0) | 0.8 (0, 2.3) | 0.7 (0, 2.9) | 0.1 (0, 2.3) | 0 (0, 1.8) | 1.0 (0, 2.3) | 0.6 (0, 2.6) | 2.0 (0, 3.8) | 2.6 (0, 3.3) |
| Patients with zero spontaneous bleeds, n (%) | NR | NR | NR | 10 (46) | 9 (53) | 18 (44) | 7 (64) | 14 (52) | 14 (66.7) | 5 (62.5) | 3 (37.5) |
| Safety Data | Patients ≥ 12 Years of Age | Patients < 12 Years of Age | ||||
|---|---|---|---|---|---|---|
| Phase I [6] | Phase II [15] | Phase III [8] | Phase IIIb Extension [14] | Phase III [7] | Phase IIIb Extension [11] | |
| n | 25 | 17 | 63 | 59 | 27 | 24 |
| Mean EDs per patient | NR | 51.5 a | 64.8 | 107 a | 61.9 | 155 |
| Patients reporting TEAEs, n (%) | 13 (52) | 14 (82.4) | 54 (85.7) | 51 (86.4) | 26 (96.3) | 23 (95.8) |
| TEAEs, n | 22 | 46 | 347 | 330 | 152 | 215 |
| Mild, n | 21 | 46 | 283 | 320 | 126 | 206 |
| Moderate, n | 1 | 59 | 23 | |||
| Severe, n | 0 | 0 | 5 | 10 | 3 | 9 |
| TRAEs, n | 4 | 0 | 11 | 0 | 0 | 0 |
| Mild, n | 4 | - | 11 | - | - | - |
| Moderate, n | 0 | - | - | - | - | |
| Severe, n | 0 | - | 0 | - | - | - |
| Patients reporting TESAEs, n (%) | 0 | 0 | 2 (3.2) | 10 (16.9) | 4 (14.8) | 7 (29.1) |
| TESAEs, n | - | - | 2 | 16 | 6 | 14 |
| Mild, n | - | - | - | 5 | - | 4 |
| Moderate, n | - | - | - | 5 | - | 3 |
| Severe, n | - | - | - | 6 | - | 7 |
| TRSAEs, n | - | - | 0 | 1 | 0 | 0 |
| Patients who withdrew due to AE, n | 0 | 0 | 1 | 1 | 0 | 0 |
| Inhibitors or antibodies, n | 0 | 0 | 0 | 0 | 0 | 0 |
| Hypersensitivity, n | 0 | 0 | 1 | 0 | 0 | 0 |
| Injection site reactions, n (%) | 1 (4.0) | NR | 28 (0.7) | NR | 48 (4.0) | NR |
| Thromboembolic events or anaphylactic reactions, n | 0 | NR | 0 | 0 | 0 | 0 |
| Episodic Treatment and Perioperative Management of Bleeding | ||
|---|---|---|
| Type of Bleed/Surgical Intervention | FIX Level Required (%) (IU/dL) | Frequency and Duration of Dosing |
| Minor or moderate hemorrhage | 30–60 | Single dose should be sufficient for most minor bleeds Maintenance dose after 24–72 h if bleeding does not cease |
| Major hemorrhage | 60–100 | Every 24–72 h for 7–14 days until bleeding ceases Maintenance dose weekly |
| Minor surgery | 50–80 | Single dose may be sufficient for most minor surgeries Maintenance dose after 24–72 h if bleeding does not cease |
| Major surgery | 60–100 | Every 24–72 h for 7–14 days until bleeding ceases Maintenance dose 1–2 times per week |
| Routine long-term prophylaxis | ||
| Starting dose regimen | Patients ≥ 12 years of age | Patients < 12 years of age |
| EMA-recommended | 35–50 IU/kg every 7 days | 35–50 IU/kg every 7 days |
| FDA-approved | 25–40 IU/kg every 7 days | 40–55 IU/kg every 7 days |
| Patients of any age well-controlled on 7-day regimen | 50–75 IU/kg every 14 days | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escobar, M.; Mancuso, M.E.; Hermans, C.; Leissinger, C.; Seifert, W.; Li, Y.; McKeand, W.; Oldenburg, J. IDELVION: A Comprehensive Review of Clinical Trial and Real-World Data. J. Clin. Med. 2022, 11, 1071. https://doi.org/10.3390/jcm11041071
Escobar M, Mancuso ME, Hermans C, Leissinger C, Seifert W, Li Y, McKeand W, Oldenburg J. IDELVION: A Comprehensive Review of Clinical Trial and Real-World Data. Journal of Clinical Medicine. 2022; 11(4):1071. https://doi.org/10.3390/jcm11041071
Chicago/Turabian StyleEscobar, Miguel, Maria Elisa Mancuso, Cedric Hermans, Cindy Leissinger, Wilfried Seifert, Yanyan Li, William McKeand, and Johannes Oldenburg. 2022. "IDELVION: A Comprehensive Review of Clinical Trial and Real-World Data" Journal of Clinical Medicine 11, no. 4: 1071. https://doi.org/10.3390/jcm11041071
APA StyleEscobar, M., Mancuso, M. E., Hermans, C., Leissinger, C., Seifert, W., Li, Y., McKeand, W., & Oldenburg, J. (2022). IDELVION: A Comprehensive Review of Clinical Trial and Real-World Data. Journal of Clinical Medicine, 11(4), 1071. https://doi.org/10.3390/jcm11041071