
The Use of Intravenous Zoledronate May Reduce Retear Rate after Rotator Cuff Repair in Older Female Patients with Osteoporosis: A First In-Human Prospective Study



Abstract
:1. Introduction
2. Materials and Methods
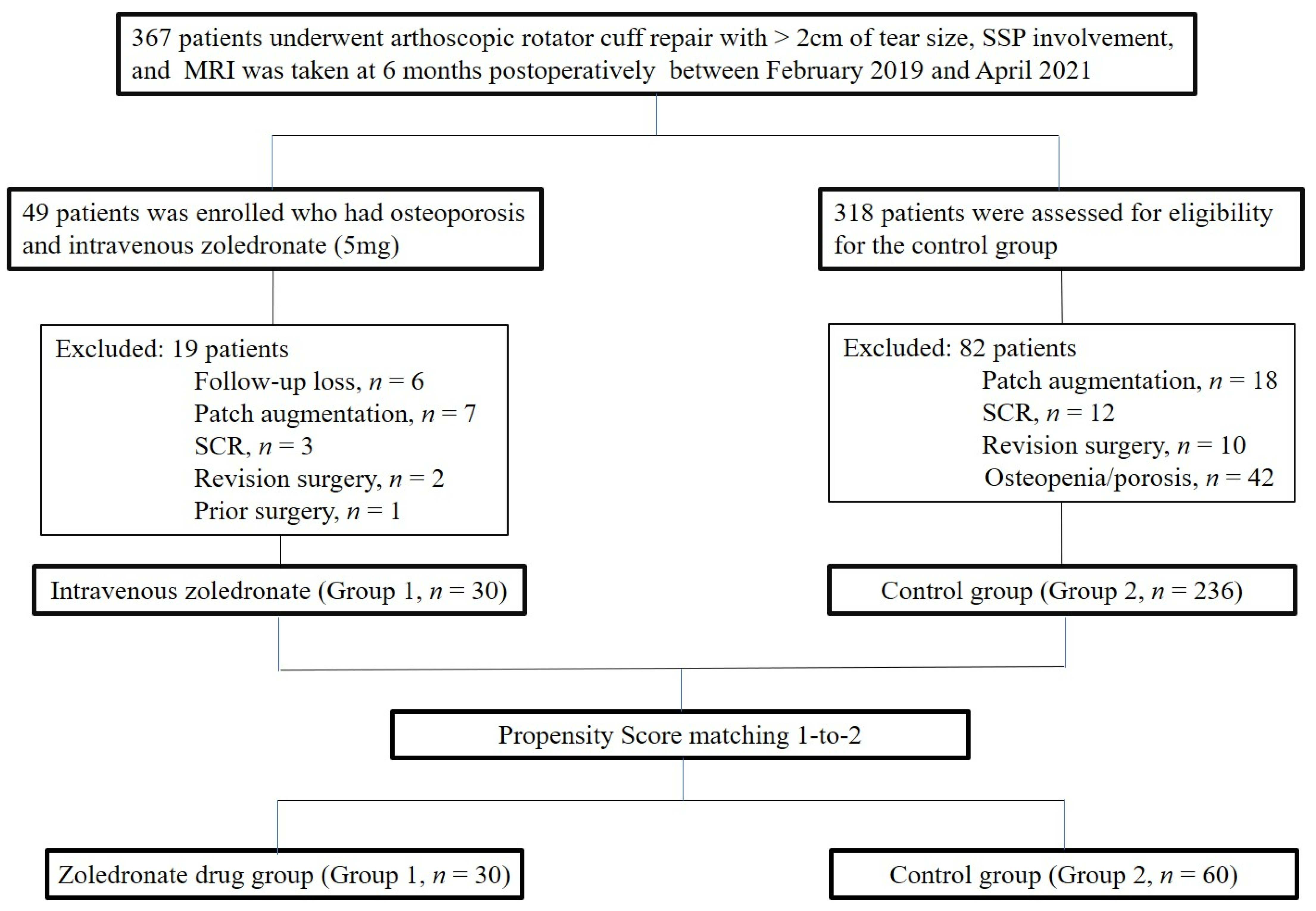
2.1. Study Design
2.2. Group Assignment
2.3. Outcome Assessment
2.4. Imaging Evaluation
2.5. Surgical Procedure and Rehabilitation
2.6. Statistics
3. Results
Functional and Radiographic Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Galatz, L.M.; Ball, C.M.; Teefey, S.A.; Middleton, W.D.; Yamaguchi, K. The Outcome and Repair Integrity of Completely Arthroscopically Repaired Large and Massive Rotator Cuff Tears. J. Bone Jt. Surg. 2004, 86, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-K.; Jung, K.-H.; Kim, J.-W.; Kim, U.-S.; Hwang, D.-H. Factors affecting rotator cuff integrity after arthroscopic repair for medium-sized or larger cuff tears: A retrospective cohort study. J. Shoulder Elb. Surg. 2018, 27, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Park, H.J.; Kim, S.H.; Oh, J.H. prognostic factors affecting rotator cuff healing after arthroscopic repair in small to medium-sized tears. Am. J. Sports Med. 2015, 43, 2386–2392. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.J.; Boyer, M.I.; Ditsios, K.; Burns, M.E.; Harwood, F.L.; Amiel, D.; Gelberman, R.H. The insertion site of the canine flexor digitorum profundus tendon heals slowly following injury and suture repair. J. Orthop. Res. 2002, 20, 447–453. [Google Scholar] [CrossRef]
- Chung, S.W.; Oh, J.H.; Gong, H.S.; Kim, J.Y.; Kim, S.H. Factors Affecting Rotator Cuff Healing After Arthroscopic Repair: Osteoporosis as one of the independent risk factors. Am. J. Sports Med. 2011, 39, 2099–2107. [Google Scholar] [CrossRef] [PubMed]
- Mall, N.A.; Tanaka, M.J.; Choi, L.S.; Paletta, G.A., Jr. Factors Affecting Rotator Cuff Healing. J. Bone Jt. Surg. 2014, 96, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Cancienne, J.M.; Brockmeier, S.F.; Kew, M.E.; Deasey, M.J.; Werner, B.C. The Association of Osteoporosis and Bisphosphonate Use with Revision Shoulder Surgery After Rotator Cuff Repair. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 2314–2320. [Google Scholar] [CrossRef]
- Plotkin, L.; Bivi, N.; Bellido, T. A bisphosphonate that does not affect osteoclasts prevents osteoblast and osteocyte apoptosis and the loss of bone strength induced by glucocorticoids in mice. Bone 2011, 49, 122–127. [Google Scholar] [CrossRef] [Green Version]
- Cadet, E.R.; Vorys, G.C.; Rahman, R.; Gardner, T.R.; Lee, F.Y.; Levine, W.N.; Bigliani, L.U.; Ahmad, C.S.; Park, S.-H. Improving bone density at the rotator cuff footprint increases supraspinatus tendon failure stress in a rat model. J. Orthop. Res. 2010, 28, 308–314. [Google Scholar] [CrossRef]
- Lui, P.; Lee, Y.; Mok, T.; Cheuk, Y.; Chan, K. Alendronate reduced peri-tunnel bone loss and enhanced tendon graft to bone tunnel healing in anterior cruciate ligament reconstruction. Eur. Cells Mater. 2013, 25, 78–96. [Google Scholar] [CrossRef]
- He, Y.; Bao, W.; Wu, X.-D.; Huang, W.; Chen, H.; Li, Z. Effects of Systemic or Local Administration of Zoledronate on Implant Osseointegration: A Preclinical Meta-Analysis. BioMed Res. Int. 2019, 2019, 9541485. [Google Scholar] [CrossRef] [PubMed]
- Schanda, J.E.; Keibl, C.; Heimel, P.; Monforte, X.; Tangl, S.; Feichtinger, X.; Teuschl, A.; Baierl, A.; Muschitz, C.; Redl, H.; et al. Zoledronic Acid Substantially Improves Bone Microarchitecture and Biomechanical Properties After Rotator Cuff Repair in a Rodent Chronic Defect Model. Am. J. Sports Med. 2020, 48, 2151–2160. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Liu, Y.; Guo, X.; Yang, H.; Xu, Y.; Geng, D. Effects of zoledronic acid on bone mineral density around prostheses and bone metabolism markers after primary total hip arthroplasty in females with postmenopausal osteoporosis. Osteoporos. Int. 2019, 30, 1581–1589. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Deloach, J.; Green, A.; Porucznik, C.A.; Powell, A.P. Minimal Clinically Important Differences in ASES and Simple Shoulder Test Scores After Nonoperative Treatment of Rotator Cuff Disease. J. Bone Jt. Surg. 2010, 92, 296–303. [Google Scholar] [CrossRef]
- Romeo, A.; Mazzocca, A.; Hang, D.W.; Shott, S.; Bach, B.R., Jr. Shoulder Scoring Scales for the Evaluation of Rotator Cuff Repair. Clin. Orthop. Relat. Res. 2004, 427, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Richards, R.R.; An, K.-N.; Bigliani, L.U.; Friedman, R.J.; Gartsman, G.M.; Gristina, A.G.; Iannotti, J.P.; Mow, V.C.; Sidles, J.A.; Zuckerman, J.D. A standardized method for the assessment of shoulder function. J. Shoulder Elb. Surg. 1994, 3, 347–352. [Google Scholar] [CrossRef]
- Conboy, V.B.; Morris, R.W.; Kiss, J.; Carr, A.J. An evaluation of the Constant-Murley shoulder assessment. J. Bone Jt. Surgery. Br. Vol. 1996, 78, 229–232. [Google Scholar] [CrossRef]
- Iannotti, J.P.; Deutsch, A.; Green, A.; Rudicel, S.; Christensen, J.; Marraffino, S.; Rodeo, S.A. Time to Failure After Rotator Cuff Repair: A Prospective Imaging Study. J. Bone Jt. Surg. 2013, 95, 965–971. [Google Scholar] [CrossRef]
- Sugaya, H.; Maeda, K.; Matsuki, K.; Moriishi, J. Repair Integrity and Functional Outcome After Arthroscopic Double-Row Rotator Cuff Repair. A prospective outcome study. J. Bone Jt. Surg. 2007, 89, 953–960. [Google Scholar] [CrossRef] [Green Version]
- DeOrio, J.K.; Cofield, R.H. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J. Bone Jt. Surg. 1984, 66, 563–567. [Google Scholar] [CrossRef]
- Cho, N.S.; Yi, J.W.; Lee, B.G.; Rhee, Y.G. Retear Patterns after Arthroscopic Rotator Cuff Repair: Single-row versus suture bridge technique. Am. J. Sports Med. 2009, 38, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, B.; Weishaupt, D.; Zanetti, M.; Hodler, J.; Gerber, C. Fatty degeneration of the muscles of the rotator cuff: Assessment by computed tomography versus magnetic resonance imaging. J. Shoulder Elb. Surg. 1999, 8, 599–605. [Google Scholar] [CrossRef]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Cho, N.S.; Rhee, Y.G. The Factors Affecting the Clinical Outcome and Integrity of Arthroscopically Repaired Rotator Cuff Tears of the Shoulder. Clin. Orthop. Surg. 2009, 1, 96–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goutallier, D.; Postel, J.-M.; Gleyze, P.; Leguilloux, P.; Van Driessche, S. Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J. Shoulder Elb. Surg. 2003, 12, 550–554. [Google Scholar] [CrossRef]
- Park, J.G.; Cho, N.S.; Song, J.H.; Baek, J.H.; Jeong, H.Y.; Rhee, Y.G. Rotator Cuff Repair in Patients over 75 Years of Age: Clinical Outcome and Repair Integrity. Clin. Orthop. Surg. 2016, 8, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.H.; Kim, D.H.; Jeong, H.J.; Park, J.H.; Rhee, S.-M. Effect of Recombinant Human Parathyroid Hormone on Rotator Cuff Healing After Arthroscopic Repair. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 1064–1071. [Google Scholar] [CrossRef]
- Amadori, D.; Aglietta, M.; Alessi, B.; Gianni, L.; Ibrahim, T.; Farina, G.; Gaion, F.; Bertoldo, F.; Santini, D.; Rondena, R.; et al. Efficacy and safety of 12-weekly versus 4-weekly zoledronic acid for prolonged treatment of patients with bone metastases from breast cancer (ZOOM): A phase 3, open-label, randomised, non-inferiority trial. Lancet Oncol. 2013, 14, 663–670. [Google Scholar] [CrossRef]
- Black, D.M.; Delmas, P.D.; Eastell, R.; Reid, I.; Boonen, S.; Cauley, J.A.; Cosman, F.; Lakatos, P.L.; Leung, P.C.; Man, Z.; et al. Once-Yearly Zoledronic Acid for Treatment of Postmenopausal Osteoporosis. N. Engl. J. Med. 2007, 356, 1809–1822. [Google Scholar] [CrossRef] [Green Version]
- Delmas, P.D.; Calvo, G.; Boers, M.; Abadie, E.; Avouac, B.; Kahan, A.; Kaufman, J.M.; Laslop, A.; Lekkerkerker, J.F.; Nilsson, P.; et al. The use of placebo-controlled and non-inferiority trials for the evaluation of new drugs in the treatment of postmenopausal osteoporosis. Osteoporos. Int. 2002, 13, 1–5. [Google Scholar] [CrossRef]
- Entezari, V.; Lazarus, M. Surgical Considerations in Managing Osteoporosis, Osteopenia, and Vitamin D Deficiency During Arthroscopic Rotator Cuff Repair. Orthop. Clin. North Am. 2019, 50, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, T.; Danks, L.; Sabokbar, A.; Athanasou, N.A. Osteoclast formation and activity in the pathogenesis of osteoporosis in rheumatoid arthritis. Rheumatology 2002, 41, 1232–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuliani, N.; Pedrazzoni, M.; Negri, G.; Passeri, G.; Impicciatore, M.; Girasole, G. Bisphosphonates Stimulate Formation of Osteoblast Precursors and Mineralized Nodules in Murine and Human Bone Marrow Cultures In Vitro and Promote Early Osteoblastogenesis in Young and Aged Mice In Vivo. Bone 1998, 22, 455–461. [Google Scholar] [CrossRef]
- Tingart, M.J.; Apreleva, M.; Lehtinen, J.; Zurakowski, D.; Warner, J.J.P. Anchor Design and Bone Mineral Density Affect the Pull-Out Strength of Suture Anchors in Rotator Cuff Repair: Which anchors are best to use in patients with low bone quality? Am. J. Sports Med. 2004, 32, 1466–1473. [Google Scholar] [CrossRef]
- Hjorthaug, G.A.; Søreide, E.; Nordsletten, L.; Madsen, J.E.; Reinholt, F.P.; Niratisairak, S.; Dimmen, S. Negative effect of zoledronic acid on tendon-to-bone healing. Acta Orthop. 2018, 89, 360–366. [Google Scholar] [CrossRef] [Green Version]
- Sung, C.-M.; Kim, R.J.; Hah, Y.-S.; Gwark, J.-Y.; Bin Park, H. In vitro effects of alendronate on fibroblasts of the human rotator cuff tendon. BMC Musculoskelet. Disord. 2020, 21, 19. [Google Scholar] [CrossRef]
- Kum, K.-Y.; Park, J.-H.; Yoo, Y.-J.; Choi, B.-K.; Lee, H.-J.; Lee, S.-J. The Inhibitory Effect of Alendronate and Taurine on Osteoclast Differentiation Mediated by Porphyromonas gingivalis Sonicates In Vitro. J. Endod. 2003, 29, 28–30. [Google Scholar] [CrossRef]
- Tripathi, K.D. Essentials of Medical Pharmacology, 7th ed.; Aypee Brothers Medical Publishers (P) Ltd.: New Delhi, India, 2013. [Google Scholar]
- Gambacciani, M.; Levancini, M. Featured Editorial Hormone replacement therapy and the prevention of postmenopausal osteoporosis. Menopausal Rev. 2014, 13, 213–220. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, Y.-H.; Moon, S.-H.; Lee, Y.-S. The Prevalence of Osteoporotic Vertebral Compression Fractures in Korean Post Menopausal Women Study Group Influence of Insurance Benefit Criteria on the Administration Rate of Osteoporosis Drugs in Postmenopausal Females. Clin. Orthop. Surg. 2014, 6, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Rutherford, O.M.; Jones, D.A. The Relationship of Muscle and Bone Loss and Activity Levels with Age in Women. Age Ageing 1992, 21, 286–293. [Google Scholar] [CrossRef]
- Szulc, P.; Beck, T.J.; Marchand, F.; Delmas, P.D. Low Skeletal Muscle Mass Is Associated With Poor Structural Parameters of Bone and Impaired Balance in Elderly Men-The MINOS Study. J. Bone Miner. Res. 2005, 20, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, A.M. Factors affecting healing after arthroscopic rotator cuff repair. World J. Orthop. 2015, 6, 211–220. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Group 1 | Group 2 | p Value |
|---|---|---|---|
| No. of patients | 30 | 60 | |
| Age, mean ± SD, year (range) | 73.7 ± 4.9 (66–84) | 72.0 ± 4.2 (64–84) | 0.094 |
| Sex, male/female, n | 0/30 | 0/60 | |
| Onset, mean ± SD, mo | 13.9 ± 29.6 | 12.9 ± 23.0 | 0.865 |
| Bone mineral density (T-score), mean ± SD | −3.6 ± 0.7 | −0.4 ± 0.8 | < 0.001 * |
| Preoperative fatty degeneration, mean ± SD | |||
| Supraspinatus | 2.3 ± 1.2 | 2.0 ± 1.5 | 0.262 |
| Infraspinatus | 1.0 ± 1.3 | 0.9 ± 1.2 | 0.767 |
| Subscapularis | 1.0 ± 1.0 | 1.0 ± 1.1 | 0.945 |
| Global fatty degeneration index | 1.4 ± 1.0 | 1.3 ± 1.1 | 0.521 |
| Tear size, mean ± SD, mm | 31.9 ± 8.3 | 29.8 ± 13.3 | 0.414 |
| Smoking history, yes/no, n | 0/30 | 0/60 | |
| Trauma history, yes/no, n | 8/22 | 20/40 | 0.632 |
| Regular exercise, yes/no, n | 27/3 | 52/8 | 0.746 |
| Factors | Group 1 | Group 2 | p Value |
|---|---|---|---|
| Clinical Outcomes | |||
| SST | |||
| preoperative | 4.4 ± 3.2 | 4.5 ± 2.4 | 0.855 |
| postoperative at 6 months | 6.3 ± 2.4 | 7.2 ± 2.4 | 0.109 |
| p-value | 0.004 * | <0.001 * | |
| UCLA | |||
| preoperative | 14.4 ± 6.3 | 15.4 ± 5.6 | 0.459 |
| postoperative at 6 months | 21.7 ± 6.6 | 25.3 ± 7.1 | 0.031 * |
| p-value | <0.001 * | <0.001 * | |
| ASES | |||
| preoperative | 44.6 ± 20.2 | 53.4 ± 17.6 | 0.039 * |
| postoperative at 6 months | 68.4 ± 14.2 | 75.6 ± 13.7 | 0.034 * |
| p-value | <0.001 * | <0.001 * | |
| CSS | |||
| preoperative | 38.1 ± 17.8 | 42.9 ± 15.8 | 0.208 |
| postoperative at 6 months | 54.4 ± 17.5 | 65.8 ± 15.9 | 0.006 * |
| p-value | 0.001 * | <0.001 * | |
| ROM | |||
| Forward flexion | |||
| preoperative | 155.7 ± 34.8 | 145.8 ± 49.6 | 0.338 |
| postoperative at 6 months | 168.1 ± 25.4 | 167.8 ± 31.7 | 0.966 |
| p-value | 0.228 | 0.001 * | |
| Internal rotation | |||
| preoperative | 3.9 ± 4.3 | 4.6 ± 4.6 | 0.706 |
| postoperative at 6 months | 9.4 ± 5.9 | 8.6 ± 6.1 | 0.554 |
| p-value | 0.003 * | <0.001 * | |
| Radiographic outcomes | |||
| Retear, % (n/N, 95%CI) | 13.3 (4/30) | 25 (15/60, −0.05~0.29 *) | 0.172 |
| Retear pattern, n, type I/II | 4/0 | 8/7 | 0.088 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Yoon, J.-Y.; Lee, Y.-B. The Use of Intravenous Zoledronate May Reduce Retear Rate after Rotator Cuff Repair in Older Female Patients with Osteoporosis: A First In-Human Prospective Study. J. Clin. Med. 2022, 11, 836. https://doi.org/10.3390/jcm11030836
Lee J-H, Yoon J-Y, Lee Y-B. The Use of Intravenous Zoledronate May Reduce Retear Rate after Rotator Cuff Repair in Older Female Patients with Osteoporosis: A First In-Human Prospective Study. Journal of Clinical Medicine. 2022; 11(3):836. https://doi.org/10.3390/jcm11030836
Chicago/Turabian StyleLee, Jae-Hoo, Jae-Young Yoon, and Yong-Beom Lee. 2022. "The Use of Intravenous Zoledronate May Reduce Retear Rate after Rotator Cuff Repair in Older Female Patients with Osteoporosis: A First In-Human Prospective Study" Journal of Clinical Medicine 11, no. 3: 836. https://doi.org/10.3390/jcm11030836
APA StyleLee, J.-H., Yoon, J.-Y., & Lee, Y.-B. (2022). The Use of Intravenous Zoledronate May Reduce Retear Rate after Rotator Cuff Repair in Older Female Patients with Osteoporosis: A First In-Human Prospective Study. Journal of Clinical Medicine, 11(3), 836. https://doi.org/10.3390/jcm11030836