
How Does Contraceptive Use Affect Women’s Sexuality? A Novel Look at Sexual Acceptability



{kind=link}
Abstract
:1. Introduction
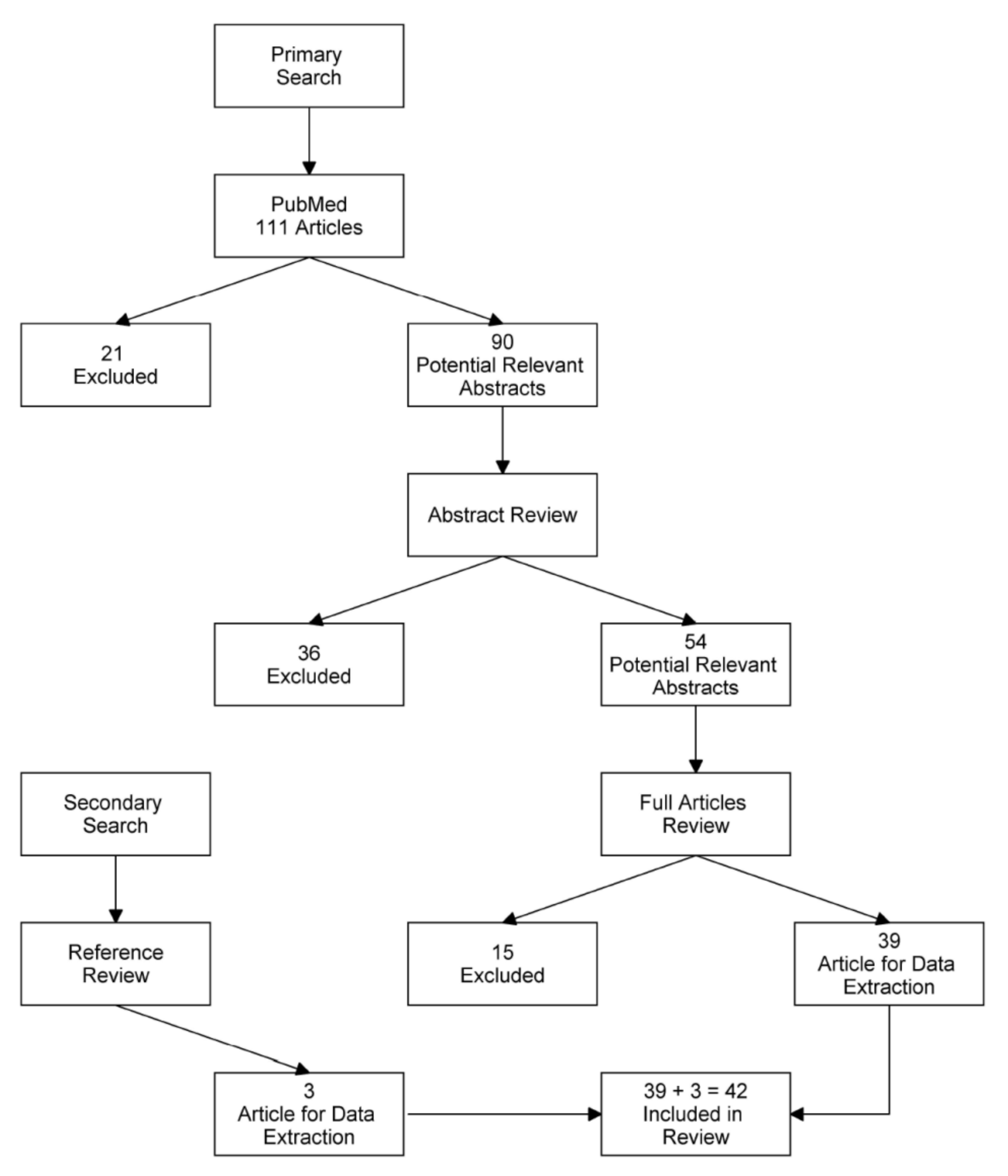
2. Materials and Methods
3. Results
3.1. Combined Oral Contraception and Sexuality
3.2. Vaginal Ring and Sexuality
3.3. Progestin-Only Pill (POP) and Sexuality
3.4. Intrauterine Devices and Sexuality
3.5. Progestin Contraceptive Implant and Sexuality
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Sonfield, A.; Hasstedt, K.; Kavanaugh, M.L.; Anderson, R. The Social and Economic Benefits of Women’s Ability to Determine Whether and When to Have Children; Guttmacher Institute: New York, NY, USA, 2013. [Google Scholar]
- Apter, D. Contraception options: Aspects unique to adolescent and young adult. Best Pr. Res. Clin. Obstet. Gynaecol. 2018, 48, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Elaut, E.; Buysse, A.; de Sutter, P.; Gerris, J.; de Cuypere, G.; T’Sjoen, G. Cycle-Related Changes in Mood, Sexual Desire, and Sexual Activity in Oral Contraception-Using and Nonhormonal-Contraception-Using Couples. J. Sex Res. 2016, 53, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Agnello, C.; Malandrino, C.; Presti, L.L.; Cicero, C.; Cianci, S. Do Hormones Influence Women’s Sex? Sexual Activity over the Menstrual Cycle. J. Sex. Med. 2014, 11, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, T.G.; Armstrong, D.T. Induction of vaginal mucification in rats with testosterone and 17β-hydroxy-5α-androstan-3-one. Steroids 1976, 27, 423–430. [Google Scholar] [CrossRef]
- Traish, A.M.; Vignozzi, L.; Simon, J.A.; Goldstein, I.; Kim, N.N. Role of Androgens in Female Genitourinary Tissue Structure and Function: Implications in the Genitourinary Syndrome of Menopause. Sex. Med. Rev. 2018, 6, 558–571. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.T.; Belkin, Z.R.; Krapf, J.M.; Song, W.; Khera, M.; Jutrzonka, S.L.; Kim, N.N.; Burrows, L.J.; Goldstein, I. Poly-morphisms of the androgen receptor gene and hormonal contraceptive induced provoked vestibulodynia. J. Sex. Med. 2014, 11, 2764–2771. [Google Scholar] [CrossRef]
- Curlin, M.; Bursac, D. Cervical mucus: From biochemical structure to clinical implications. Front. Biosci. 2013, 5, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Basson, R. Human sexual response. Handb. Clin. Neurol. 2015, 130, 11–18. [Google Scholar]
- Davis, A.R.; Castaño, P.M. Oral contraceptives and libido in women. Annu. Rev. Sex Res. 2004, 15, 297–320. [Google Scholar]
- Dobbins, J.G. Implication of a time-dependent model of sexual intercourse within the menstrual cycle. J. Biosoc. Sci. 1980, 12, 133–140. [Google Scholar] [CrossRef]
- Burrows, L.J.; Basha, M.; Goldstein, A.T. The Effects of Hormonal Contraceptives on Female Sexuality: A Review. J. Sex. Med. 2012, 9, 2213–2223. [Google Scholar] [CrossRef]
- Caruso, S.; Rugolo, S.; Agnello, C.; Romano, M.; Cianci, A. Quality of Sexual Life in Hyperandrogenic Women Treated with an Oral Contraceptive Containing Chlormadinone Acetate. J. Sex. Med. 2009, 6, 3376–3384. [Google Scholar] [CrossRef]
- Both, S.; Lew-Starowicz, M.; Luria, M.; Sartorius, G.; Maseroli, E.; Tripodi, F.; Lowenstein, L.; Nappi, R.E.; Corona, G.; Reisman, Y.; et al. Hormonal Contraception and Female Sexuality: Position Statements from the European Society of Sexual Medicine (ESSM). J. Sex. Med. 2019, 16, 1681–1695. [Google Scholar] [CrossRef]
- Casado-Espada, N.M.; de Alarcón, R.; de La Iglesia-Larrad, J.I.; Bote-Bonaechea, B.; Montejo, Á.L. Hormonal Contraceptives, Female Sexual Dysfunction, and Managing Strategies: A Review. J. Clin. Med. 2019, 8, 908. [Google Scholar] [CrossRef] [Green Version]
- Shifren, J.L. The Role of Androgens in Female Sexual Dysfunction. Mayo Clin. Proc. 2004, 79, S19–S24. [Google Scholar] [CrossRef]
- Toit, R.L.-D.; Perkins, M.S.; Hapgood, J.P.; Africander, D. Comparing the androgenic and estrogenic properties of progestins used in contraception and hormone therapy. Biochem. Biophys. Res. Commun. 2017, 491, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Caruso, S.; Malandrino, C.; Cicero, C.; Ciancio, F.; Cariola, M.; Cianci, A. Quality of Sexual Life of Women on Oral Contraceptive Continued-Regimen: Pilot Study. J. Sex. Med. 2013, 10, 460–466. [Google Scholar] [CrossRef]
- Kuhl, H. Pharmacology of estrogens and progestogens: Influence of different routes of administration. Climacteric 2005, 8, 3–63. [Google Scholar] [CrossRef]
- Di Carlo, C.; Gargano, V.; Sparice, S.; Tommaselli, G.A.; Bifulco, G.; Nappi, C. Effects of an oral contraceptive containing estradiol valerate and dienogest on circulating androgen levels and acne in young patients with PCOS: An observational preliminary study. Gynecol. Endocrinol. 2013, 29, 1048–1050. [Google Scholar] [CrossRef] [Green Version]
- Caruso, S.; Cianci, S.; Cariola, M.; Fava, V.; di Pasqua, S.; Cianci, A. Improvement of Low Sexual Desire Due to Antiandrogenic Combined Oral Contraceptives After Switching to an Oral Contraceptive Containing 17β-Estradiol. J. Women’s Health 2017, 26, 728–734. [Google Scholar] [CrossRef]
- De Leo, V.; di Sabatino, A.; Musacchio, M.C.; Morgante, G.; Scolaro, V.; Cianci, A.; Petraglia, F. Effect of oral contraceptives on markers of hyperandrogenism and SHBG in women with polycystic ovary syndrome. Contraception 2010, 82, 276–280. [Google Scholar] [CrossRef]
- Davis, S.R.; Bitzer, J.; Giraldi, A.; Palacios, S.; Parke, S.; Serrani, M.; Mellinger, U.; Nappi, R.E. Change to either a nonandrogenic or androgenic progestin-containing oral contraceptive preparation is associated with improved sexual function in women with oral contraceptive-associated sexual dysfunction. J. Sex. Med. 2013, 10, 3069–3079. [Google Scholar] [CrossRef]
- Caruso, S.; Agnello, C.; Romano, M.; Cianci, S.; Presti, L.L.; Malandrino, C.; Cianci, A. Preliminary study on the effect of four-phasic estradiol valerate and dienogest (E2V/DNG) oral contraceptive on the quality of sexual life. J. Sex. Med. 2011, 8, 2841–2850. [Google Scholar] [CrossRef]
- Burrows, L.J.; Goldstein, A.T. The Treatment of Vestibulodynia with Topical Estradiol and Testosterone. Sex. Med. 2013, 1, 30–33. [Google Scholar] [CrossRef] [Green Version]
- Smith, N.K.; Jozkowski, K.N.; Sanders, S.A. Hormonal Contraception and Female Pain, Orgasm and Sexual Pleasure. J. Sex. Med. 2014, 11, 462–470. [Google Scholar] [CrossRef]
- Caruso, S.; Agnello, C.; Intelisano, G.; Farina, M.; di Mari, L.; Cianci, A. Sexual behavior of women taking low-dose oral contraceptive containing 15 μg ethinylestradiol/60 μg gestodene. Contraception 2004, 69, 237–240. [Google Scholar] [CrossRef]
- Pastor, Z.; Holla, K.; Chmel, R. The influence of combined oral contraceptives on female sexual desire: A systematic review. Eur. J. Contracept. Reprod. Health Care 2013, 18, 27–43. [Google Scholar] [CrossRef]
- Graham, C.A.; Bancroft, J.; Doll, H.A.; Greco, T.; Tanner, A. Does oral contraceptive-induced reduction in free testosterone adversely affect the sexuality or mood of women? Psychoneuroendocrinology 2007, 32, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Wallwiener, C.W.; Wallwiener, L.-M.; Seeger, H.; Schönfisch, B.; Mueck, A.O.; Bitzer, J.; Zipfel, S.; Brucker, S.Y.; Taran, F.-A.; Wallwiener, M. Are hormonal components of oral contraceptives associated with impaired female sexual function? A questionnaire-based online survey of medical students in Germany, Austria, and Switzerland. Arch. Gynecol. Obstet. 2015, 292, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Bancroft, J.; Hammond, G.; Graham, C. Do oral contraceptives produce irreversible effects on women’s sexuality? J. Sex. Med. 2006, 3, 567. [Google Scholar] [CrossRef] [PubMed]
- Serati, M.; Bogani, G.; di Dedda, M.C.; Braghiroli, A.; Uccella, S.; Cromi, A.; Ghezzi, F. A comparison between vaginal estrogen and vaginal hyaluronic for the treatment of dyspareunia in women using hormonal contraceptive. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 191, 48–50. [Google Scholar] [CrossRef]
- Caruso, S.; Panella, M.; Giunta, G.; Matarazzo, M.G.; Cianci, A.; Cianci, S. Comparative randomized study on the sexual function and quality of life of women on contraceptive vaginal ring containing ethinylestradiol/etonogestrel 3.47/11.00 mg or 2.7/11.7 mg. Gynecol. Endocrinol. 2019, 35, 1–5. [Google Scholar] [CrossRef]
- Guida, M.; di Carlo, C.; Troisi, J.; Gallo, A.; Cibarelli, F.; Martini, E.; Tiranini, L.; Nappi, R.E. The sexuological impact of hormonal contraceptives based on their route of administration. Gynecol. Endocrinol. 2017, 33, 218–222. [Google Scholar] [CrossRef]
- Elaut, E.; Buysse, A.; de Sutter, P.; de Cuypere, G.; Gerris, J.; Deschepper, E.; T’Sjoen, G. Relation of androgen receptor sensitivity and mood to sexual desire in hormonal contraception users. Contraception 2012, 85, 470–479. [Google Scholar] [CrossRef]
- Caruso, S.; Cianci, S.; Malandrino, C.; Cicero, C.; Presti, L.L.; Cianci, A. Quality of sexual life of women using the contraceptive vaginal ring in extended cycles: Preliminary report. Eur. J. Contracept. Reprod. Health Care 2014, 19, 307–314. [Google Scholar] [CrossRef]
- Mohamed, A.M.M.; El-Sherbiny, W.S.M.; Mostafa, W.A.I. Combined contraceptive ring versus combined oral contraceptive (30-μg ethinylestradiol and 3-mg drospirenone). Int. J. Gynecol. Obstet. 2011, 114, 145–148. [Google Scholar] [CrossRef]
- Department of Reproductive Health; World Health Organization. Medical Eligibility Criteria for Contraceptive Use, 4th ed.; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Gracia, C.R.; Sammel, M.D.; Charlesworth, S.; Lin, H.; Barnhart, K.T.; Creinin, M.D. Sexual function in first-time contraceptive ring and contraceptive patch users. Fertil. Steril. 2010, 93, 21–28. [Google Scholar] [CrossRef]
- Graham, C.A.; Ramos, R.; Bancroft, J.; Maglaya, C.; Farley, T.M. The effects of steroidal contraceptives on the well-being and sexuality of women: A double-blind, placebo-controlled, two-centre study of combined and progestogen-only methods. Contraception 1995, 52, 363–369. [Google Scholar] [CrossRef]
- McCoy, N.L.; Matyas, J.R. Oral contraceptives and sexuality in university women. Arch. Sex. Behav. 1996, 25, 73–90. [Google Scholar] [CrossRef]
- Jung-Hoffman, C.; Kuhl, H. Divergent effects of two low-dose oral contraceptives on sex hormone-binding globulin and free testosterone. Am. J. Obstet. Gynecol. 1987, 156, 199–203. [Google Scholar] [CrossRef]
- Secura, G.M.; Allsworth, J.E.; Madden, T.; Mullersman, J.L.; Peipert, J.F. The Contraceptive CHOICE Project: Reducing barriers to long-acting reversible contraception. Am. J. Obstet. Gynecol. 2010, 203, 115.e1–115.e7. [Google Scholar] [CrossRef] [Green Version]
- Rose, S.B.; Lawton, B.A. Impact of long-acting reversible contraception on return for repeat abortion. Am. J. Obstet. Gynecol. 2012, 206, 37.e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Grunloh, D.S.; Casner, T.; Secura, G.M.; Peipert, J.F.; Madden, T.S.D. Characteristics Associated With Discontinuation of Long-Acting Reversible Contraception Within the First 6 Months of Use. Obstet. Gynecol. 2013, 122, 1214–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, J.N.; Higgins, J.A.; Adkins, D.E.; Stoddard, G.J.; Gawron, L.M.; Turok, D.K. The Impact of Sexual Satisfaction, Functioning, and Perceived Contraceptive Effects on Sex Life on IUD and Implant Continuation at 1 Year. Women’s Health Issues 2018, 28, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Gomez, A.M.; Clark, J.B. The relationship between contraceptive features preferred by young women and interest in IUDs: An exploratory analysis. Perspect. Sex. Reprod. Health 2014, 46, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Neri, M.; Piras, B.; Paoletti, A.M.; Vallerino, V.; Corda, V.; Ronchetti, C.; Taccori, V.; Pilloni, M.; Zedda, P.; Capobianco, G.; et al. Long-acting reversible contraception (LARC) with the intrauterine system with levonorgestrel (6mcg/d): Observational study on the acceptability, quality of life, and sexuality in Italian women. Gynecol. Endocrinol. 2018, 34, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Cianci, S.; Vitale, S.G.; Fava, V.; Cutello, S.; Cianci, A. Sexual function and quality of life of women adopting the levonorgestrel-releasing intrauterine system (LNG-IUS 13.5 mg) after abortion for unintended pregnancy. Eur. J. Contracept. Reprod. Health Care 2018, 23, 24–31. [Google Scholar] [CrossRef]
- Higgins, J.A.; Kramer, R.D.; Wright, K.Q.; Everett, B.; Turok, D.K.; Sanders, J.N. Sexual Functioning, Satisfaction, and Well-Being Among Contraceptive Users: A Three-Month Assessment From the HER Salt Lake Contraceptive Initiative. J. Sex Res. 2021, 9, 1–10. [Google Scholar] [CrossRef]
- Higgins, J.A.; Ryder, K.; Skarda, G.; Koepsel, E.; Bennett, E.A. The Sexual Acceptability of Intrauterine Contraception: A Qualitative Study of Young Adult Women. Perspect. Sex. Reprod. Health 2015, 47, 115–122. [Google Scholar] [CrossRef]
- Pekin, A.T.; Kerimoğlu, O.S.; Kebapcılar, A.G.; Yılmaz, S.A.; Benzer, N.; Celik, C. Depressive symptomatology and quality of life assessment among women using the levonorgestrel-releasing intrauterine system: An observational study. Arch. Gynecol. Obstet. 2014, 290, 507–511. [Google Scholar] [CrossRef]
- Higgins, J.A.; Smith, N.K. The Sexual Acceptability of Contraception: Reviewing the Literature and Building a New Concept. J. Sex Res. 2016, 53, 417–456. [Google Scholar] [CrossRef]
- Enzlin, P.; Weyers, S.; Janssens, D.; Poppe, W.; Eelen, C.; Pazmany, E.; Elaut, E.; Amy, J. Sexual Functioning in Women Using Levonorgestrel-Releasing Intrauterine Systems as Compared to Copper Intrauterine Devices. J. Sex. Med. 2012, 9, 1065–1073. [Google Scholar] [CrossRef]
- Malmborg, A.; Brynhildsen, J.; Hammar, M. A survey of young women’s perceptions of the influence of the Levonorgestrel-Intrauterine System or copper-intrauterine device on sexual desire. Sex. Reprod. Health 2019, 21, 75–80. [Google Scholar] [CrossRef]
- He, Y.R.; Li, Y.; Ma, L.; Wei, S.S.; Wu, H.Y.; Huang, J. Effects of LNG-IUS on sexual function and sexual quality in women of childbearing age. Zhonghua Yi Xue Za Zhi 2020, 100, 1255–1259. [Google Scholar]
- Ferreira, J.M.; Carreiro, A.V.; Fernandes, A.; Bahamondes, L. Sexual Function and Quality of Life in a Cohort of Brazilian Users of Two Kind of Intrauterine Contraceptives. Rev. Bras. Ginecol. Obstet. 2019, 41, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Apter, D. International Perspectives: IUDs and Adolescents. J. Pediatr. Adolesc. Gynecol. 2019, 32, S36–S42. [Google Scholar] [CrossRef]
- Caruso, S.; Vitale, S.G.; Fava, V.; di Pasqua, S.; Rapisarda, A.M.C.; Cianci, S. Quality of life of women using the etonogestrel long-acting reversible contraceptive implant after abortion for unplanned pregnancy. Eur. J. Contracept. Reprod. Health Care 2020, 25, 251–258. [Google Scholar] [CrossRef]
- Walsh-Buhi, E.R.; Helmy, H.L. Trends in long-acting reversible contraceptive (LARC) use, LARC use predictors, and dual-method use among a national sample of college women. J. Am. Coll. Health 2018, 66, 225–236. [Google Scholar] [CrossRef]
- Di Carlo, C.; Sansone, A.; de Rosa, N.; Gargano, V.; Tommaselli, G.A.; Nappi, C.; Bifulco, G. Impact of an implantable steroid contraceptive (etonogestrel-releasing implant) on quality of life and sexual function: A preliminary study. Gynecol. Endocrinol. 2014, 30, 53–56. [Google Scholar] [CrossRef]
- Higgins, J.A.; Hirsch, J.S. Pleasure, Power, and Inequality: Incorporating Sexuality into Research on Contraceptive Use. Am. J. Public Health 2008, 98, 1803–1813. [Google Scholar] [CrossRef]
- Fennell, J. “And Isn’t that the point?”: Pleasure and contraceptive decisions. Contraception 2014, 89, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.F.; Vargas, S.E.; Guillen, M.; Ramirez, J.J.; Carbone, S.L.; Getz, M.L.; Frimpong, Y.; Smith, K.A.; Shaw, J.G.; Tong, I.; et al. A Qualitative Study of the Contraceptive Effect on Women’s Sexual Experiences: Beyond Hormonal Effects. Obstet. Gynecol. 2019, 134, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, B.G. Female Sexual Function and Dysfunction in the Reproductive Years: The Influence of Endogenous and Exogenous Sex Hormones. J. Sex. Med. 2008, 5, 2282–2290. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, S.; Palermo, G.; Caruso, G.; Rapisarda, A.M.C. How Does Contraceptive Use Affect Women’s Sexuality? A Novel Look at Sexual Acceptability. J. Clin. Med. 2022, 11, 810. https://doi.org/10.3390/jcm11030810
Caruso S, Palermo G, Caruso G, Rapisarda AMC. How Does Contraceptive Use Affect Women’s Sexuality? A Novel Look at Sexual Acceptability. Journal of Clinical Medicine. 2022; 11(3):810. https://doi.org/10.3390/jcm11030810
Chicago/Turabian StyleCaruso, Salvatore, Gaia Palermo, Giuseppe Caruso, and Agnese Maria Chiara Rapisarda. 2022. "How Does Contraceptive Use Affect Women’s Sexuality? A Novel Look at Sexual Acceptability" Journal of Clinical Medicine 11, no. 3: 810. https://doi.org/10.3390/jcm11030810
APA StyleCaruso, S., Palermo, G., Caruso, G., & Rapisarda, A. M. C. (2022). How Does Contraceptive Use Affect Women’s Sexuality? A Novel Look at Sexual Acceptability. Journal of Clinical Medicine, 11(3), 810. https://doi.org/10.3390/jcm11030810