
External Validation of a Novel Comprehensive Trifecta System in Predicting Oncologic and Functional Outcomes of Partial Nephrectomy: Results of a Multicentric Series


 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hung, A.J.; Cai, J.; Simmons, M.N.; Gill, I.S. “Trifecta” in Partial Nephrectomy. J. Urol. 2013, 189, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Buffi, N.; Lista, G.; Larcher, A.; Lughezzani, G.; Ficarra, V.; Cestari, A.; Lazzeri, M.; Guazzoni, G.F. Margin, Ischemia, and Complications (MIC) Score in Partial Nephrectomy: A New System for Evaluating Achievement of Optimal Outcomes in Nephron-sparing Surgery. Eur. Urol. 2012, 62, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Khalifeh, A.; Autorino, R.; Hillyer, S.P.; Laydner, H.; Eyraud, R.; Panumatrassamee, K.; Long, J.A.; Kaouk, J.H. Comparative Outcomes and Assessment of Trifecta in 500 Robotic and Laparoscopic Partial Nephrectomy Cases: A Single Surgeon Experience. J. Urol. 2012, 189, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Larcher, A.; Muttin, F.; Peyronnet, B.; De Naeyer, G.; Khene, Z.-E.; Dell’Oglio, P.; Ferreiro, C.; Schatteman, P.; Capitanio, U.; D’Hondt, F.; et al. The Learning Curve for Robot-assisted Partial Nephrectomy: Impact of Surgical Experience on Perioperative Outcomes. Eur. Urol. 2018, 75, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Wang, X.; Xu, T.; Guzzo, T.J. Systematic Review and Meta-Analysis of Comparative Studies Reporting Perioperative Outcomes of Robot-Assisted Partial Nephrectomy versus Open Partial Nephrectomy. J. Endourol. 2017, 31, 893–909. [Google Scholar] [CrossRef] [PubMed]
- Brassetti, A.; Anceschi, U.; Bertolo, R.; Ferriero, M.; Tuderti, G.; Costantini, M.; Capitanio, U.; Larcher, A.; Antonelli, A.; Mottrie, A.; et al. Comprehensive long-term assessment of outcomes following robot-assisted partial nephrectomy for renal cell carcinoma: The ROMe’s achievement and its predicting nomogram. Minerva Urol. Nefrol. 2020, 72, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Anceschi, U.; Ferriero, M.C.; Tuderti, G.; Brassetti, A.; Bertolo, R.; Capitanio, U.; Larcher, A.; Garisto, J.; Antonelli, A.; Mottrie, A.; et al. Head to Head Impact of Margin, Ischemia, Complications, Score versus a Novel Trifecta Score on Oncologic and Functional Outcomes After Robotic-assisted Partial Nephrectomy: Results of a Multicenter Series. Eur. Urol. Focus 2020, 7, 1319–1399. [Google Scholar] [CrossRef]
- Simone, G.; De Nunzio, C.; Ferriero, M.; Cindolo, L.; Brookman-May, S.; Papalia, R.; Sperduti, I.; Collura, D.; Leonardo, C.; Anceschi, U.; et al. Trends in the use of partial nephrectomy for cT1 renal tumors: Analysis of a 10-yr European multicenter dataset. Eur. J. Surg. Oncol. 2016, 42, 1729–1735. [Google Scholar] [CrossRef]
- Ferriero, M.; Bove, A.M.; Tuderti, G.; Anceschi, U.; Brassetti, A.; Costantini, M.; Mastroianni, R.; Guaglianone, S.; Gallucci, M.; Simone, G. Impact of learning curve on perioperative outcomes of off-clamp minimally invasive partial nephrectomy: Propensity score matched comparison of outcomes between training versus expert series. Minerva Urol. Nefrol. 2020, 73, 564–571. [Google Scholar] [CrossRef]
- Krane, L.S.; Hemal, A.K. Emerging Technologies to Improve Techniques and Outcomes of Robotic Partial Nephrectomy: Striving toward the Pentafecta. Urol. Clin. N. Am. 2014, 41, 511–519. [Google Scholar] [CrossRef]
- Sri, D.; Thakkar, R.; Patel, H.R.H.; Lazarus, J.; Berger, F.; McArthur, R.; Lavigueur-Blouin, H.; Afshar, M.; Fraser-Taylor, C.; Le Roux, P.; et al. Robotic-assisted partial nephrectomy (RAPN) and standardization of outcome reporting: A prospective, observational study on reaching the “Trifecta and Pentafecta”. J. Robot. Surg. 2020, 15, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Brassetti, A.; Anceschi, U.; Bertolo, R.; Ferriero, M.; Tuderti, G.; Capitanio, U.; Larcher, A.; Garisto, J.; Antonelli, A.; Mottire, A.; et al. Surgical quality, cancer control and functional preservation: Introducing a novel trifecta for robot-assisted partial nephrectomy. Minerva Urol. Nefrol. 2020, 72, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Bravi, C.A.; Vertosick, E.; Benfante, N.; Tin, A.; Sjoberg, D.; Hakimi, A.A.; Touijer, K.; Montorsi, F.; Eastham, J.; Russo, P.; et al. Impact of Acute Kidney Injury and Its Duration on Long-term Renal Function After Partial Nephrectomy. Eur. Urol. 2019, 76, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.; Toussaint, N.D.; et al. Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder: Synopsis of the Kidney Disease: Improving Global Outcomes 2017 Clinical Practice Guideline Update. Ann. Intern. Med. 2018, 168, 422–430. [Google Scholar] [CrossRef]
- Mitropoulos, D.; Artibani, W.; Biyani, C.S.; Jensen, J.B.; Rouprêt, M.; Truss, M. Validation of the Clavien–Dindo Grading System in Urology by the European Association of Urology Guidelines Ad Hoc Panel. Eur. Urol. Focus 2018, 4, 608–613. [Google Scholar] [CrossRef]
- Kutikov, A.; Uzzo, R.G. The RENAL Nephrometry Score: A Comprehensive Standardized System for Quantitating Renal Tumor Size, Location and Depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef]
- Anceschi, U.; Brassetti, A.; Bertolo, R.; Tuderti, G.; Ferriero, M.C.; Mastroianni, R.; Flammia, R.S.; Costantini, M.; Kaouk, J.; Leonardo, C.; et al. On-clamp versus purely off-clamp robot-assisted partial nephrectomy in solitary kidneys: Comparison of perioperative outcomes and chronic kidney disease progression at two high- volume centers. Minerva Urol. Nefrol. 2020. [Google Scholar] [CrossRef]
- Dong, W.; Wu, J.; Suk-Ouichai, C.; Antonio, E.C.; Remer, E.; Li, J.; Zabell, J.; Isharwal, S.; Campbell, S.C. Ischemia and Functional Recovery from Partial Nephrectomy: Refined Perspectives. Eur. Urol. Focus 2018, 4, 572–578. [Google Scholar] [CrossRef]
- Zabell, J.; Isharwal, S.; Dong, W.; Abraham, J.; Wu, J.; Suk-Ouichai, C.; Palacios, D.A.; Remer, E.; Li, J.; Campbell, S.C. Acute Kidney Injury after Partial Nephrectomy of Solitary Kidneys: Impact on Long-Term Stability of Renal Function. J. Urol. 2018, 200, 1295–1301. [Google Scholar] [CrossRef]
- Simone, G.; Tuderti, G.; Anceschi, U.; Ferriero, M.; Costantini, M.; Minisola, F.; Vallati, G.; Pizzi, G.; Guaglianone, S.; Misuraca, L.; et al. “Ride the Green Light”: Indocyanine Green–marked Off-clamp Robotic Partial Nephrectomy for Totally Endophytic Renal Masses. Eur. Urol. 2018, 75, 1008–1014. [Google Scholar] [CrossRef]
- Mattevi, D.; Luciani, L.G.; Mantovani, W.; Cai, T.; Chiodini, S.; Vattovani, V.; Puglisi, M.; Malossini, G. Fluorescence-guided selective arterial clamping during RAPN provides better early functional outcomes based on renal scan compared to standard clamping. J. Robot. Surg. 2018, 13, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Simone, G.; Capitanio, U.; Tuderti, G.; Presicce, F.; Leonardo, C.; Ferriero, M.; Misuraca, L.; Costantini, M.; Larcher, A.; Minisola, F.; et al. On-clamp versus off-clamp partial nephrectomy: Propensity score-matched comparison of long-term functional outcomes. Int. J. Urol. 2019, 26, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, Z.A.; Uzzo, R.G.; Larcher, A.; Lane, B.R.; Ristau, B.; Capitanio, U.; Ryan, S.; Dey, S.; Correa, A.; Reddy, M.; et al. Comparison of functional outcomes of robotic and open partial nephrectomy in patients with pre-existing chronic kidney disease: A multicenter study. World J. Urol. 2018, 36, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Chalouhy, C.; Ruck, J.M.; Zhou, T.C.; Sirvastava, A.; Keehn, A.; Watts, K.L.; María, P.; Ghavamian, R. Robotic Partial Nephrectomy in Patients with Chronic Kidney Disease: Objective Measurement of Short- and Long-Term Renal Functional Outcomes. J. Endourol. 2018, 32, 630–634. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Cohort (n = 649) | Centre A (n = 335) | Centre B (n = 88) | Centre C (n = 226) | p |
|---|---|---|---|---|---|
| Age (yrs, median, IQR) | 64 (55–72) | 64 (55–72) | 63 (54.2–71) | 62.5 (54–72.5) | 0.710 |
| Gender (n,%) Male Female | 416 (64%) 233 (36%) | 216 (64.5%) 119 (35.5%) | 52 (59.1%) 36 (40.9%) | 148 (65.5%) 78 (34.5%) | 0.557 |
| ASA score (n,%) 1–2 3–4 | 514 (79.1%) 135 (20.9%) | 251 (74.9%) 84 (25.1%) | 72 (81.8%) 16 (18.2%) | 191 (84.5%) 35 (15.5%) | 0.01 |
| Diabetes (n,%) | 60 (9.2%) | 32 (9.5%) | 14 (15.9%) | 14 (6.2%) | 0.02 |
| Hypertension (n,%) | 197 (30.3%) | 122 (36.4%) | 46 (52.2%) | 29 (12.8%) | 0.001 |
| Surgical approach (n,%) Open Laparoscopic Robotic | 109 (16.7%) 59 (9.2%) 481 (74.1%) | 109 (32.5%) 57 (17%) 169 (50.4%) | - 2 (2.3%) 86 (97.7%) | - - 226 (100%) | 0.001 |
| Clinical tumor size (cm, median, IQR) | 3.3 (2.4–4.5) | 3.2 (2.2–4.2) | 3.9(2.6–5) | 3.2 (2.5–4.5) | 0.06 |
| RENAL score (n,%) 4–6 7–9 10–12 | 282 (43.4%) 241 (37.1%) 126 (19.5%) | 143 (42.6%) 120 (35.8%) 72 (21.7%) | 31 (34%) 42 (47.7%) 15 (17%) | 108 (47.8%) 79 (35%) 39 (17.2%) | 0.124 |
| Preoperative eGFR (mL/min/1.73 m2, median, IQR) | 83 (69–98.6) | 82.2 (69.3–95.3) | 90.2 (67–118) | 81.5 (70–97.7) | 0.001 |
| Preoperative cT stage (n,%) 1a 1b 2a 2b | 440 (67.8%) 168 (25.9%) 35 (5.4%) 6 (0.9%) | 248 (74%) 73 (21.7%) 14 (4.1%) - | 49 (55.6%) 31 (35.2%) 4 (4.5%) 4 (4.5%) | 143 (63.2%) 64 (28.3%) 17 (7.5%) 2 (1%) | 0.001 |
| Preoperative CKD stage (n,%) 1 2 3a 3b 4 5 | 232 (35.8%) 317 (48.6%) 68 (10.5%) 20 (3.1%) 10 (1.6%) 2 (0.4%) | 120 (35.8%) 165 (49.2%) 34 (10.1%) 8 (2.38%) 8 (2.38%) - | 45 (51.1%) 34 (38.6%) 7 (7.9%) 2 (2.2%) - | 67 (29.7%) 118 (52.3%) 27 (12%) 10 (4.4%) 2 (0.8%) 2 (0.8%) | 0.09 |
| Variable | Overall Cohort (n = 649) | Centre A (n = 335) | Centre B (n = 88) | Centre C (n = 226) | p |
|---|---|---|---|---|---|
| PSM (n,%) | 52 (8%) | 42 (12.5%) | 10 (11.3%) | 0 (%) | 0.001 |
| Hystology type (n,%) Benign Malignant | 166 (25.5%) 483 (74.5%) | 71 (21.2%) 264 (78.8%) | 22 (25%) 66 (75%) | 73 (32.3%) 153 (67.7%) | 0.01 |
| pT stage (n,%) 1a 1b 2a 2b 3a 3b | 388 (59.8%) 176 (27.2%) 55 (8.5%) 18 (2.8%) 9 (1.3%) 3 (0.4%) | 232 (69.2%) 67 (20%) 31 (9.2%) - 2 (0.6%) 3 (0.9%) | 41 (46.5%) 29 (32.9%) 10 (11.3%) 5 (5.6%) 3 (3.4%) - | 115 (50.8%) 80 (35.4%) 14 (6.2%) 13 (5.8%) 4 (1.8%) - | 0.001 |
| Overall perioperative complications (any, n,%) | 146 (22.4%) | 113 (33.7%) | 10 (11.3%) | 23 (10.2%) | 0.001 |
| Postoperative Clavien Grade (n,%) 1–2 3–5 | 106 (16.3%) 40 (6.1%) | 84 (25%) 29 (8.65%) | 5 (5.68%) 5 (5.68%) | 17 (7.5%) 6 (2.6%) | 0.001 0.01 |
| WIT (median, min, IQR) | 0 (0–20) | 20 (13–26) | - | - | 0.001 |
| Postoperative eGFR (mL/min/1.73 m2 median, IQR) | 80 (62.2–100.9) | 80.2 (60.9–103.4) | 91.7 (68.3–130–7) | 77 (58.2–91) | 0.001 |
| ΔeGFR (mL/min/1.73 m2 median, IQR) | 3.3 (−14.5; +18.06) | 0 (−19; +19) | −4.5 (−17.8; +7.6) | 8.38 (0–19) | 0.001 |
| Variable | Overall Cohort (n = 649) | Centre A (n = 335) | Centre B (n = 88) | Centre C (n = 226) | p |
|---|---|---|---|---|---|
| Follow-up (months, median, IQR) | 22.7 (12.5–76.5) | 73.4 (43.9–118.4) | 16.4 (13.8–19.8) | 9.2 (4.2–15.8) | 0.001 |
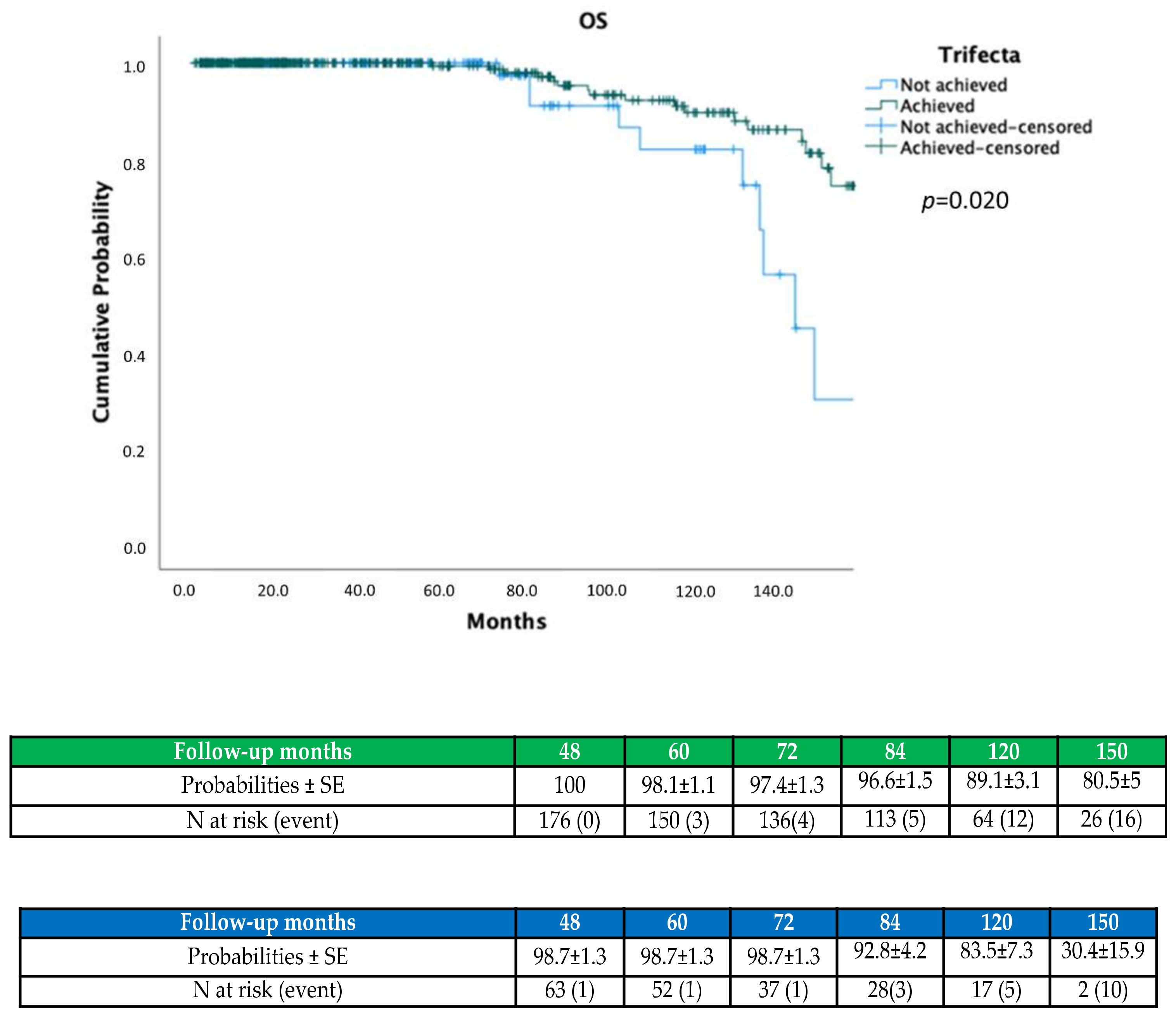
| OS (n,%) | 617 (95%) | 304 (90.7%) | 88 (100%) | 225 (99.6%) | 0.001 |
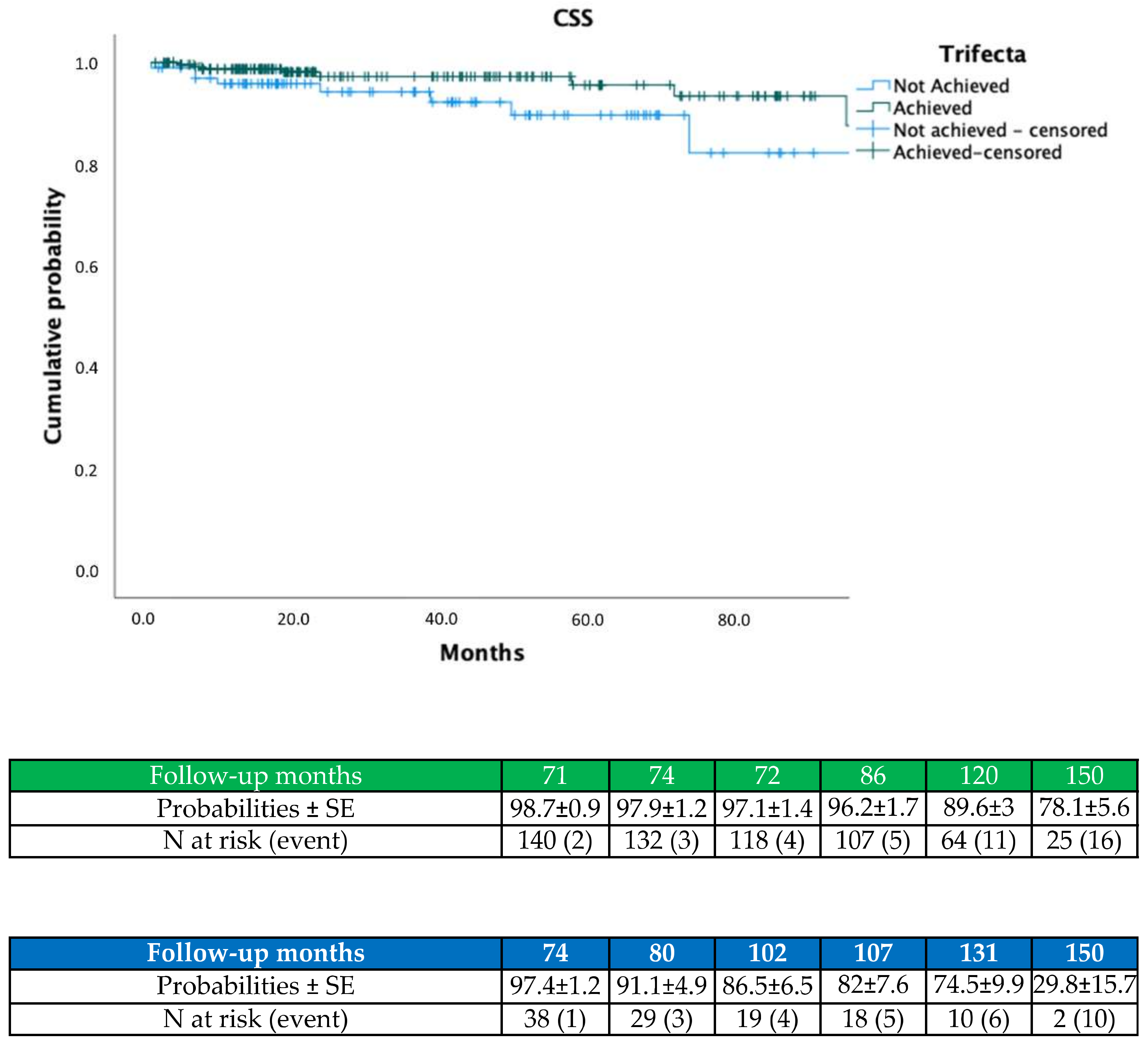
| CSS (n,%) | 607 (93.5%) | 299 (89.2%) | 84 (95.5%) | 224 (99.1%) | 0.001 |
| Recurrence (n,%) * Local Renal | 35 (7.2%) 7 (1.4%) | 30 (6.2%) 6 (1.2%) | 3 (0.6%) 1 (0.2%) | 2 (0.4%) - | 0.001 |
| eGFR at last follow-up (mL/min/1.73 m2, median, IQR) | 63.2(49.2–76.1) | 57.3 (45.4–71.4) | 69.2 (59.6–85.6) | 70.1 (59.6–85.8) | 0.001 |
| Newly onset CKD 3b (n,%) | 49 (7.5%) | 43 (12.8%) | 5 (5.7%) | 3 (1.3%) | 0.004 |
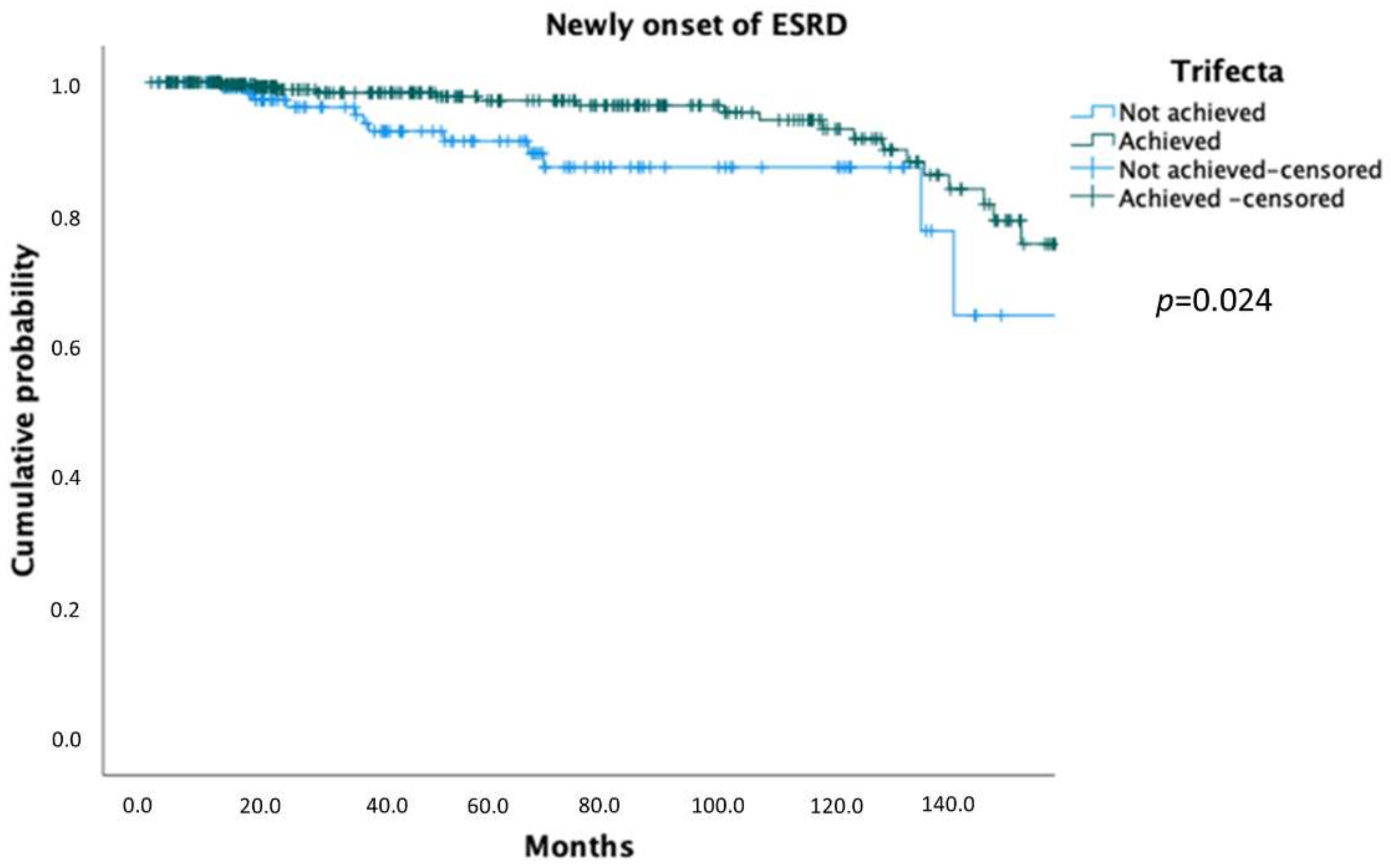
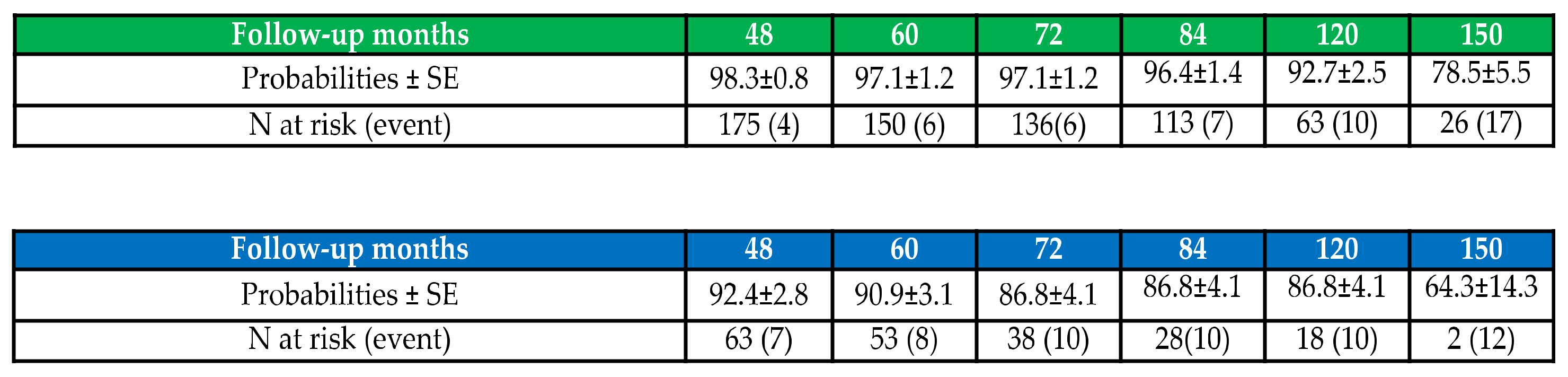
| Newly onset ESRD (n,%) | 33 (5%) | 28 (8.4%) | 4 (4.5%) | 1 (0.4%) | 0.02 |
| CKD stages at last follow-up (n,%) 1 2 3a 3b 4 5 | 102 (15.8%) 301 (46.4%) 142 (21.8%) 64 (9.8%) 26 (4.1%) 14 (2.1%) | 18 (5.4%) 141 (42.1%) 100 (29.9%) 45 (13.4%) 20 (6%) 11 (3.3%) | 17 (19.3%) 48 (54.5%) 13 (14.8%) 6 (6.8%) 3 (3.4%) 1 (1.1%) | 67 (29.7%) 112 (49.6%) 29 (12.9%) 13 (5.7%) 3 (1.3%) 2 (0.8%) | 0.001 |
| Trifecta (n,%) ΔeGFR ≤ 30 Negative surgical margins No Clavien ≥ 3 | 498 (76.7%) 571 (87.9%) 597 (93.2%) 609 (93.8%) | 230 (68.6%) 283 (84.4%) 293 (87.4%) 306 (91.3%) | 68 (77.3%) 82 (93.1%) 78 (88.6%) 83 (94.3%) | 200 (88.4%) 206 (91.1%) 226 (100%) 220 (97.3%) | 0.001 |
| Variable | Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95.0% CI | HR | 95.0% CI | |||||
| Lower | Higher | p Value | Lower | Higher | p Value | |||
| Age | 1.04 | 1.01 | 1.07 | 0.02 | 1.04 | 1.01 | 1.08 | 0.01 |
| Gender | 0.80 | 0.36 | 1.75 | 0.578 | - | - | - | - |
| Diabetes | 1.19 | 0.36 | 3.96 | 0.769 | - | - | - | - |
| Hypertension | 1.13 | 0.54 | 2.35 | 0.739 | - | - | - | - |
| ASA score 1–2 3–4 | 0.89 | 0.34 | 2.36 | 0.829 | - | - | - | - |
| pT stage | 0.85 | 0.31 | 2.29 | 0.756 | - | - | - | - |
| RENAL (cat) 4–6 vs. 7–9 4–6 vs. 10–12 | 1.06 1.55 | 0.45 0.51 | 2.49 4.75 | 0.884 0.435 | - | - | - | - |
| Preoperative CKD stage | 0.52 | 0.11 | 2.38 | 0.403 | - | - | - | - |
| Trifecta | 0.42 | 0.19 | 0.91 | 0.029 | 0.34 | 0.15 | 0.76 | 0.009 |
| Variable | Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95.0% CI | HR | 95.0% CI | |||||
| Lower | Higher | p Value | Lower | Higher | p Value | |||
| Age | 1.01 | 0.97 | 1.04 | 0.715 | - | - | - | - |
| Gender | 0.77 | 0.35 | 1.70 | 0.515 | - | - | - | - |
| Diabetes | 0.47 | 0.06 | 3.48 | 0.459 | - | - | - | - |
| Hypertension | 1.14 | 0.52 | 2.54 | 0.740 | - | - | - | - |
| ASA score 1–2 3–4 | 1.59 | 0.55 | 4.61 | 0.391 | - | - | - | - |
| RENAL (cat) 4–6 vs. 7–9 4–6 vs. 10–12 | 1.90 2.19 | 0.43 0.47 | 8.37 10.09 | 0.396 0.316 | - | - | - | - |
| pT stage | 1.15 | 0.82 | 1.60 | 0.429 | 1.16 | 0.83 | 1.62 | 0.339 |
| Preoperative CKD stage | 1.12 | 0.76 | 1.66 | 0.569 | - | - | - | - |
| Trifecta | 0.36 | 0.17 | 0.77 | 0.008 | 0.36 | 0.17 | 0.77 | 0.008 |
| Variable | Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95.0% CI | HR | 95.0% CI | |||||
| Lower | Higher | p Value | Lower | Higher | p Value | |||
| Age | 1.01 | 0.97 | 1.04 | 0.580 | - | - | - | - |
| Gender | 1.13 | 0.56 | 2.28 | 0.721 | - | - | - | - |
| Diabetes | 3.14 | 1.40 | 7.02 | 0.005 | 1.29 | 0.50 | 3.29 | 0.595 |
| Hypertension | 1.73 | 0.87 | 3.44 | 0.116 | - | - | - | - |
| ASA score 1–2 3–4 | 1.31 | 0.58 | 2.96 | 0.503 | - | - | - | - |
| RENAL (cat) 4–6 vs. 7–9 4–6 vs. 10–12 | 1.23 1.30 | 0.57 0.42 | 2.68 4.01 | 0.589 0.639 | - | - | - | - |
| Hilar control | 1.52 | 0.61 | 3.82 | 0.363 | - | - | - | - |
| Warm Ischemia Time | 1.01 | 0.98 | 1.05 | 0.339 | - | - | - | - |
| Preoperative CKD stage CKD 3a vs. CKD 1–2 CKD 3a vs. CKD 3b | 0.04 0.11 | 0.01 0.02 | 0.13 0.44 | <0.001 0.002 | 4.55 13.1 | 1.51 4.07 | 13.7 42.6 | 0.007 <0.001 |
| Trifecta | 0.47 | 0.22 | 0.98 | 0.045 | 0.41 | 0.19 | 0.87 | 0.02 |
| Development Cohort | External Validation Cohort | ||
|---|---|---|---|
| pCKD ≥ 3b | AUC restricted model | 0.915 | 0.907 |
| AUC full model * | 0.920 | 0.946 | |
| OM | AUC restricted model | 0.858 | 0.503 |
| AUC full model * | 0.859 | 0.593 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anceschi, U.; Flammia, R.S.; Mattevi, D.; Tufano, A.; Brassetti, A.; Ferriero, M.C.; Tuderti, G.; Misuraca, L.; Bove, A.M.; Mastroianni, R.; et al. External Validation of a Novel Comprehensive Trifecta System in Predicting Oncologic and Functional Outcomes of Partial Nephrectomy: Results of a Multicentric Series. J. Clin. Med. 2022, 11, 796. https://doi.org/10.3390/jcm11030796
Anceschi U, Flammia RS, Mattevi D, Tufano A, Brassetti A, Ferriero MC, Tuderti G, Misuraca L, Bove AM, Mastroianni R, et al. External Validation of a Novel Comprehensive Trifecta System in Predicting Oncologic and Functional Outcomes of Partial Nephrectomy: Results of a Multicentric Series. Journal of Clinical Medicine. 2022; 11(3):796. https://doi.org/10.3390/jcm11030796
Chicago/Turabian StyleAnceschi, Umberto, Rocco Simone Flammia, Daniele Mattevi, Antonio Tufano, Aldo Brassetti, Maria Consiglia Ferriero, Gabriele Tuderti, Leonardo Misuraca, Alfredo Maria Bove, Riccardo Mastroianni, and et al. 2022. "External Validation of a Novel Comprehensive Trifecta System in Predicting Oncologic and Functional Outcomes of Partial Nephrectomy: Results of a Multicentric Series" Journal of Clinical Medicine 11, no. 3: 796. https://doi.org/10.3390/jcm11030796
APA StyleAnceschi, U., Flammia, R. S., Mattevi, D., Tufano, A., Brassetti, A., Ferriero, M. C., Tuderti, G., Misuraca, L., Bove, A. M., Mastroianni, R., Marsiliani, D., Puglisi, M., Cai, T., Leonardo, C., Gallucci, M., Malossini, G., Luciani, L. G., & Simone, G. (2022). External Validation of a Novel Comprehensive Trifecta System in Predicting Oncologic and Functional Outcomes of Partial Nephrectomy: Results of a Multicentric Series. Journal of Clinical Medicine, 11(3), 796. https://doi.org/10.3390/jcm11030796