
Serum Sulfatide Levels as a Biomarker of Active Glomerular Lesion in Patients with Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single Center Pilot Study

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
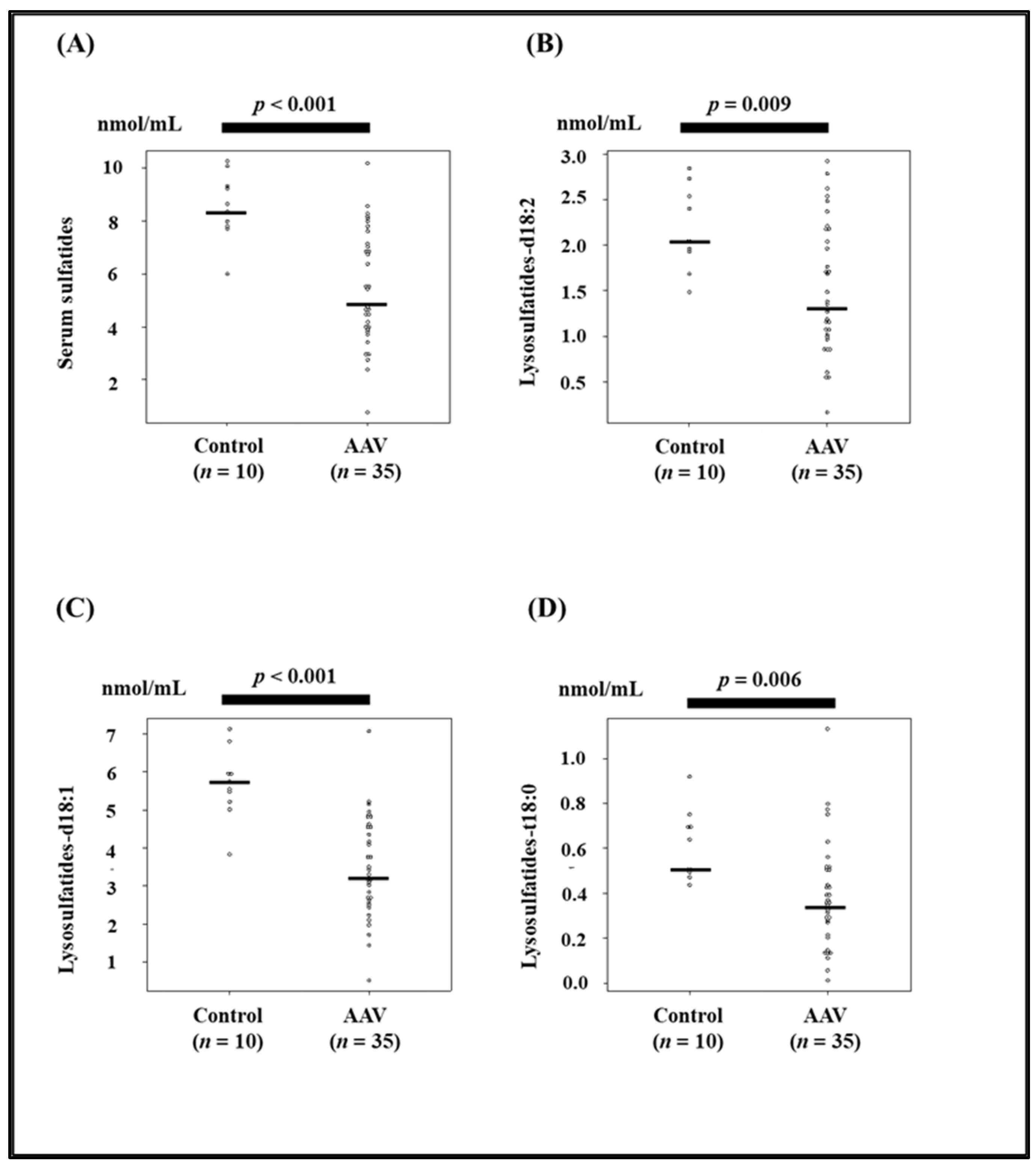
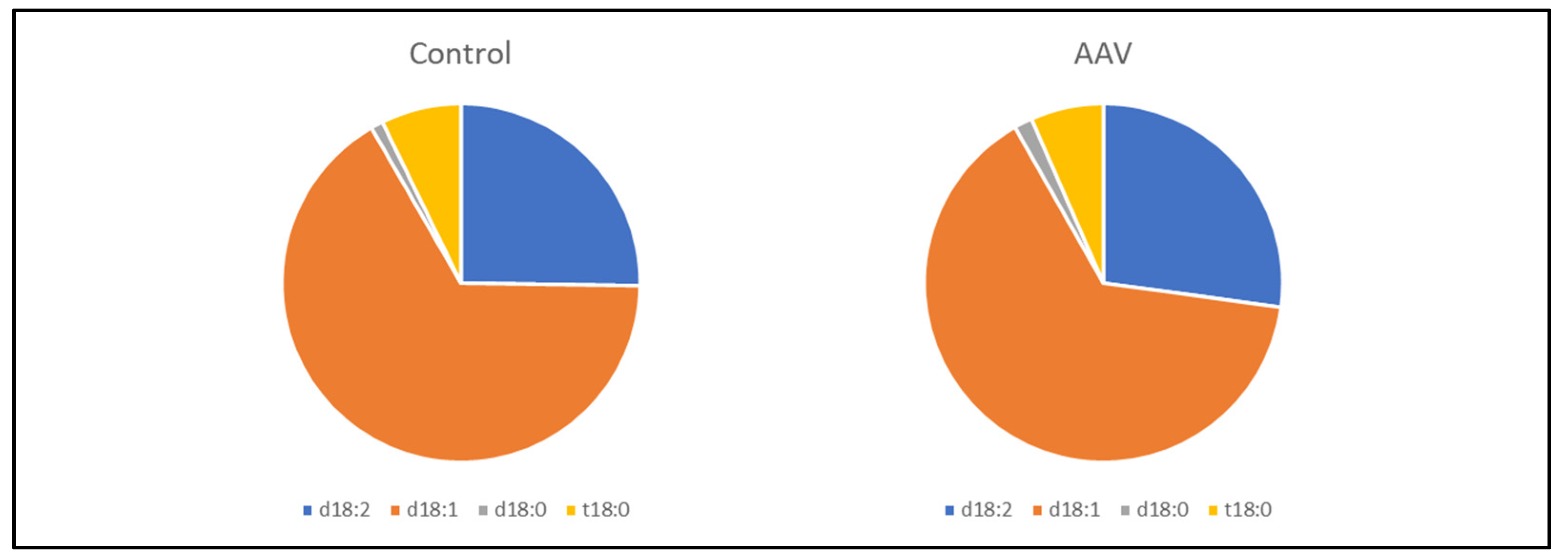
3.1. Comparison of Serum Sulfatide Levels and Clinical Characteristics between Control and AAV Patients
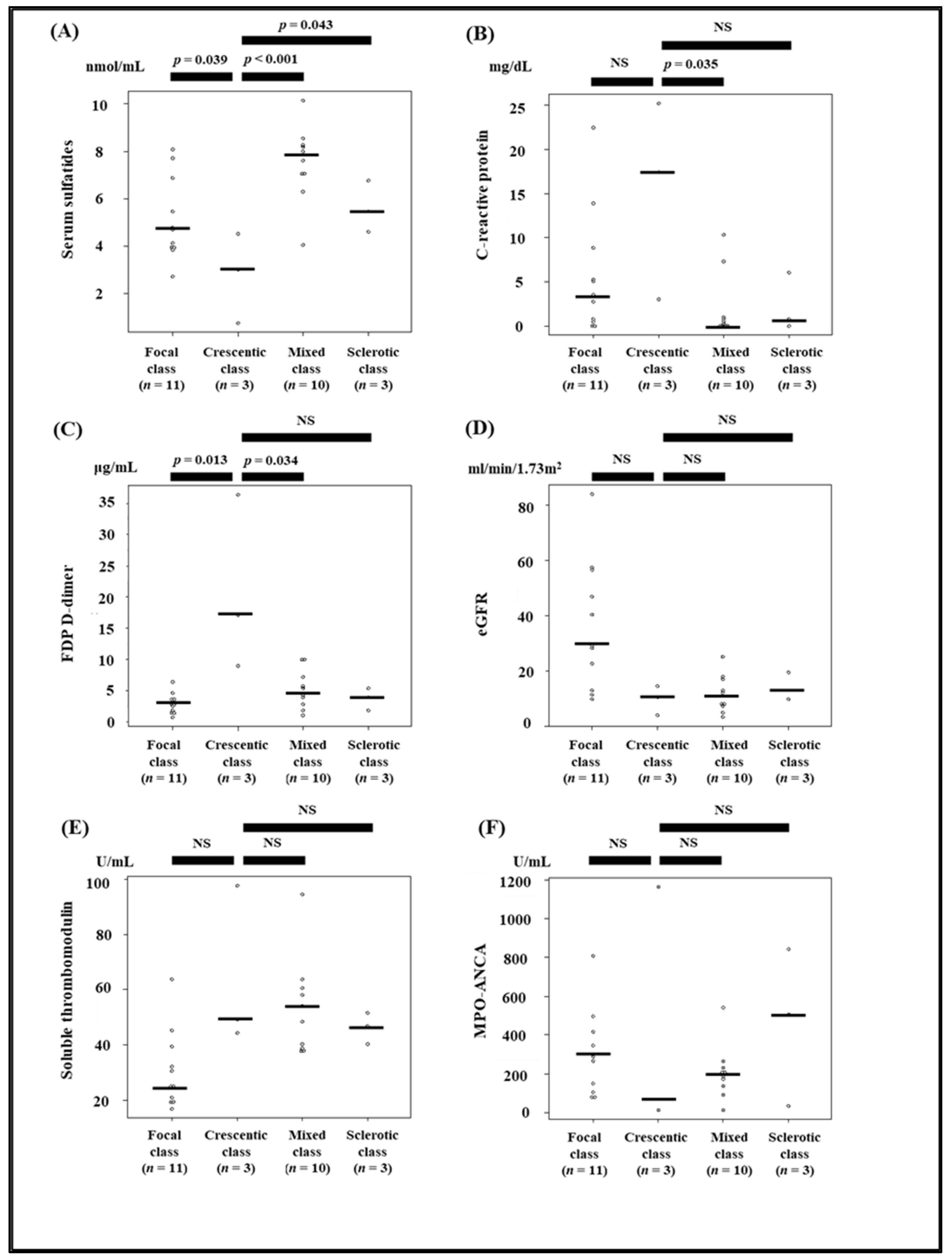
3.2. Comparison of Clinical Parameters between the Histopathologic Classes of ANCA-Associated Glomerulonephritis
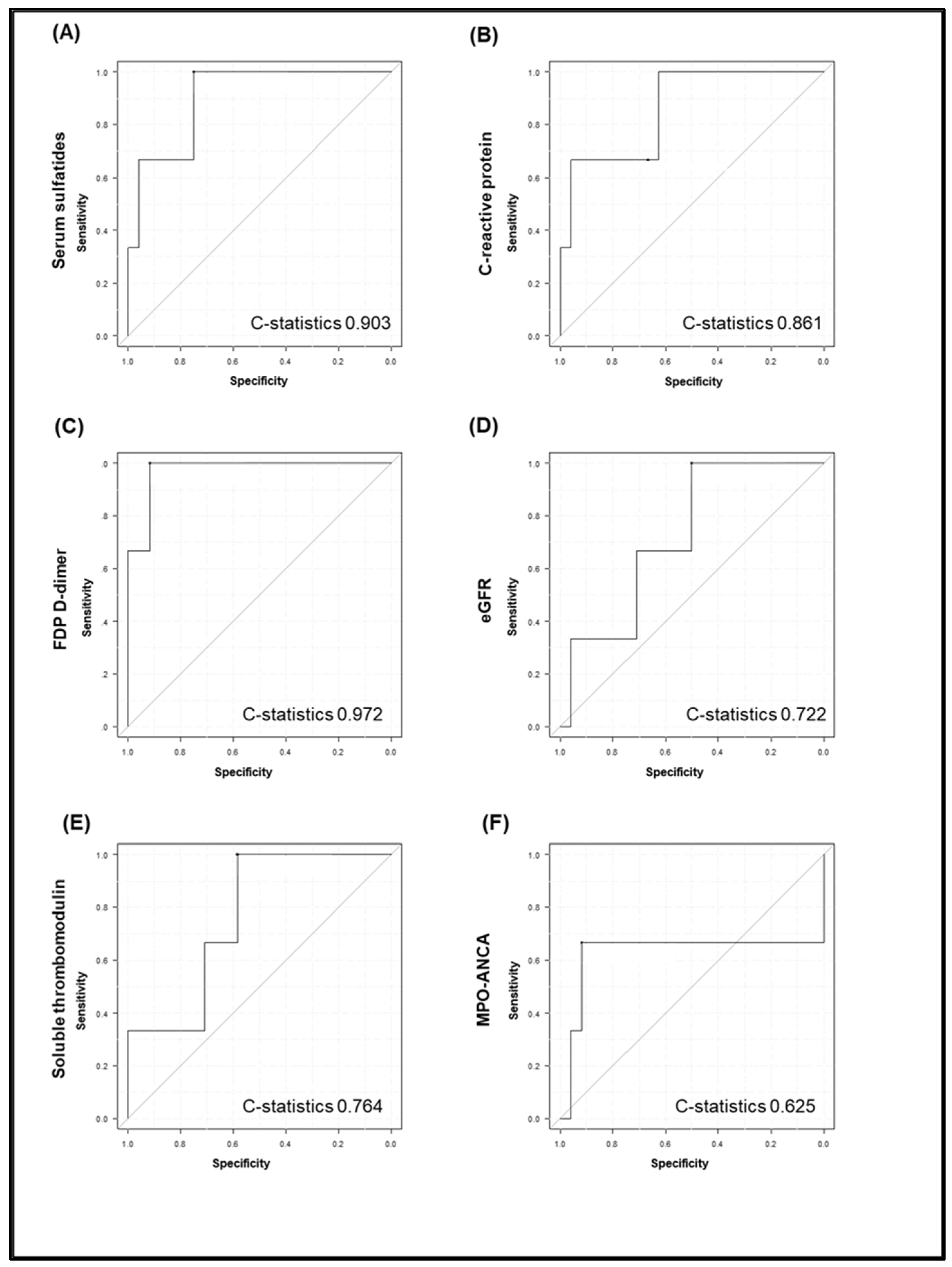
3.3. Comparison between Serum Sulfatides, C-Reactive Protein, FDP D-Dimer, eGFR, and Soluble Thrombomodulin, MPO-ANCA and Kidney Histopathological Findings
3.4. Correlation between Serum Sulfatide Levels and Clinical Parameters
3.5. Association between Serum Sulfatide Level and Clinical Outcomes/Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pagnoux, C. Updates in ANCA-associated vasculitis. Eur. J. Rheumatol. 2016, 3, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Kitching, A.R.; Anders, H.J.; Basu, N.; Brouwer, E.; Gordon, J.; Jayne, D.R.; Kullman, J.; Lyons, P.A.; Merkel, P.A.; Savage, C.O.S.; et al. ANCA-associated vasculitis. Nat. Rev. Dis Primers 2020, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Harada, M.; Ishi, W.; Masubuchi, T.; Ichikawa, T.; Kobayashi, M. Relationship between immunosuppressive therapy and the development of infectious complications among patients with anti-neutrophil cytoplasmic antibody-associated vasculitis: A single-center, retrospective observational study. Cureus 2019, 11, e5676. [Google Scholar] [CrossRef] [PubMed]
- Berden, A.E.; Ferrario, F.; Hagen, E.C.; Jayne, D.R.; Jennette, J.C.; Joh, K.; Neumann, I.; Noël, L.H.; Pusey, C.D.; Waldherr, R.; et al. Histopathologic classification of ANCA-associated glomerulonephritis. J. Am. Soc. Nephrol. 2010, 21, 1628–1636. [Google Scholar] [CrossRef]
- Van Daalen, E.E.; Wester Trejo, M.A.C.; Göçeroǧlu, A.; Ferrario, F.; Joh, K.; Noël, L.H.; Ogawa, Y.; Wilhelmus, S.; Ball, M.J.; Honsova, E.; et al. Developments in the histopathological classification of ANCA-associated glomerulonephritis. Clin. J. Am. Soc. Nephrol. 2020, 15, 1103–1111. [Google Scholar] [CrossRef]
- Harada, M.; Yamaguchi, A.; Sonoda, K.; Yamada, Y.; Aomura, D.; Kamimura, Y.; Hashimoto, K.; Ichikawa, T.; Kobayashi, M.; Kamijo, Y. Comparison of the factors associated with the short-term prognosis between elderly and non-elderly patients with anti-neutrophil cytoplasmic antibody-associated vasculitis: A retrospective observational study. Clin. Exp. Rheumatol. 2021. Online ahead of print. [Google Scholar]
- Nakazawa, D.; Masuda, S.; Tomaru, U.; Ishizu, A. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis. Nat. Rev. Rheumatol. 2019, 15, 91–101. [Google Scholar] [CrossRef]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Nakajima, T.; Kamijo, Y.; Yuzhe, H.; Kimura, T.; Tanaka, N.; Sugiyama, E.; Nakamura, K.; Kyogashima, M.; Hara, A.; Aoyama, T. Peroxisome proliferator-activated receptor α mediates enhancement of gene expression of cerebroside sulfotransferase in several murine organs. Glycoconj. J. 2013, 30, 553–560. [Google Scholar] [CrossRef]
- Yamada, Y.; Harada, M.; Hashimoto, K.; Guo, R.; Nakajima, T.; Kashihara, T.; Yamada, M.; Aoyama, T.; Kamijo, Y. Impact of chronic kidney dysfunction on serum sulfatides and its metabolic pathway in mice. Glycoconj. J. 2019, 36, 1–11. [Google Scholar] [CrossRef]
- Guo, R.; Hu, X.; Yamada, Y.; Harada, M.; Nakajima, T.; Kashihara, T.; Yamada, M.; Aoyama, T.; Kamijo, Y. Effects of hypertension and antihypertensive treatments on sulfatide levels in serum and its metabolism. Hypertens. Res. 2019, 42, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Merten, M.; Thiagarajan, P. Role for sulfatides in platelet aggregation. Circulation 2001, 104, 2955–2960. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Takahashi, T.; Suzuki, T. Role of sulfatide in normal and pathological cells and tissues. J. Lipid Res. 2012, 53, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Taketomi, T. Occurrence of sulfatide as a major glycosphingolipid in WHHL rabbit serum lipoproteins. J. Biochem. 1987, 102, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Kutsukake, Y.; Uemura, K.I.; Taketomi, T. Anticoagulant activity of sulfatide and its anti-thrombotic effect in rabbit. J. Biochem. 1993, 113, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Uemura, K.; Taketomi, T. Sulfatide prolongs blood-coagulation time and bleeding time by forming a complex with fibrinogen. Glycoconj. J. 1996, 13, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Kyogashima, M.; Sakai, T.; Onaya, J.; Hara, A. Roles of galactose and sulfate residues in sulfatides for their antagonistic functions in the blood coagulation system. Glycoconj. J. 2001, 18, 245–251. [Google Scholar] [CrossRef]
- Kyogashima, M. The role of sulfatide in thrombogenesis and haemostasis. Arch. Biochem. Biophys. 2004, 426, 157–162. [Google Scholar] [CrossRef]
- Hu, R.; Li, G.; Kamijo, Y.; Aoyama, T.; Nakajima, T.; Inoue, T.; Node, K.; Kannagi, R.; Kyogashima, M.; Hara, A. Serum sulfatides as a novel biomarker for cardiovascular disease in patients with end-stage renal failure. Glycoconj. J. 2007, 24, 565–571. [Google Scholar] [CrossRef]
- Li, G.; Hu, R.; Guo, Y.; He, L.; Zuo, Q.; Wang, Y. Circulating sulfatide, a novel biomarker for ST-segment elevation myocardial infarction. J. Atheroscler. Thromb. 2019, 26, 84–92. [Google Scholar] [CrossRef]
- Li, G.; Hu, R. Association between serum sulfatide and carotid intima media thickness in patients with familial hypercholesterolemia. Glycoconj. J. 2014, 31, 587–592. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Miao, D.; Li, D.Y.; Chen, M.; Zhao, M.H. Platelets are activated in ANCA-associated vasculitis via thrombin-PARs pathway and can activate the alternative complement pathway. Arthritis Res. Ther. 2017, 19, 252. [Google Scholar] [CrossRef] [PubMed]
- Tomasson, G.; Lavalley, M.; Tanriverdi, K.; Finkielman, J.D.; Davis, J.C., Jr.; Hoffman, G.S.; McCune, W.J.; St Clair, E.W.; Specks, U.; Spiera, R.; et al. Relationship between markers of platelet activation and inflammation with disease activity in Wegener’s granulomatosis. J. Rheumatol. 2011, 38, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Berti, A.; Matteson, E.L.; Crowson, C.S.; Specks, U.; Cornec, D. Risk of cardiovascular disease and venous thromboembolism among patients with incident ANCA-associated vasculitis: A 20-year population-based cohort study. Mayo Clin. Proc. 2018, 93, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Alpa, M.; Ferrero, B.; Cavallo, R.; Perna, A.; Naretto, C.; Gennaro, M.; Di Simone, D.; Bellizia, L.; Mansouri, M.; Rossi, D.; et al. Anti-GM1 and anti-sulfatide antibodies in patients with systemic lupus erythematosus, Sjogren’s syndrome, mixed cryoglobulinemia and idiopathic systemic vasculitis. Clin. Exp. Rheumatol. 2007, 25, 556–562. [Google Scholar] [PubMed]
- Watts, R.; Lane, S.; Hanslik, T.; Hauser, T.; Hellmich, B.; Koldingsnes, W.; Mahr, A.; Segelmark, M.; Cohen-Tervaert, J.W.; Scott, D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann. Rheum. Dis. 2007, 66, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Hu, R.; Kamijo, Y.; Nakajima, T.; Aoyama, T.; Inoue, T.; Node, K.; Kannagi, R.; Kyogashima, M.; Hara, A. Establishment of a quantitative, qualitative, and high-throughput analysis of sulfatides from small amounts of sera by matrix-assisted laser desorption ionization-time of flight mass spectrometry. Anal. Biochem. 2007, 362, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Martin, F.A.; Murphy, R.P.; Cummins, P.M. Thrombomodulin and the vascular endothelium: Insights into functional, regulatory, and therapeutic aspects. Am. J. Physiol. Heart Circ. Physiol. 2013, 304, H1585–H1597. [Google Scholar] [CrossRef] [PubMed]
- Ristagno, G.; Fumagalli, F.; Bottazzi, B.; Mantovani, A.; Olivari, D.; Novelli, D.; Latini, R. Pentraxin 3 in cardiovascular disease. Front. Immunol. 2019, 10, 823. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Chang, D.Y.; Wu, L.H.; Liu, G.; Chen, M.; Kallenberg, C.G.; Zhao, M.H. Re-evaluation of the histopathologic classification of ANCA-associated glomerulonephritis: A study of 121 patients in a single center. Nephrol. Dial. Transpl. 2012, 27, 2343–2349. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yamagata, K.; Usui, J.; Nagata, M.; Sugiyama, H.; Sada, K.E.; Muso, E.; Harigai, M.; Amano, K.; Atsumi, T.; Fujimoto, S.; et al. Histopathological classification of anti-neutrophil cytoplasmic antibody-associated glomerulonephritis in a nationwide Japanese prospective 2-year follow-up cohort study. Clin. Exp. Nephrol. 2019, 23, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and Validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef]
- Yamagata, K.; Usui, J.; Saito, C.; Yamaguchi, N.; Hirayama, K.; Mase, K.; Kobayashi, M.; Koyama, A.; Sugiyama, H.; Nitta, K.; et al. ANCA-associated systemic vasculitis in Japan: Clinical features and prognostic changes. Clin. Exp. Nephrol. 2012, 16, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Kanbe, H.; Kamijo, Y.; Nakajima, T.; Tanaka, N.; Sugiyama, E.; Wang, L.; Fang, Z.Z.; Hara, A.; Gonzalez, F.J.; Aoyama, T. Chronic ethanol consumption decreases serum sulfatide levels by suppressing hepatic cerebroside sulfotransferase expression in mice. Arch. Toxicol. 2014, 88, 367–379. [Google Scholar] [CrossRef]
- Kamijo, Y.; Wang, L.; Matsumoto, A.; Nakajima, T.; Hashimoto, K.; Higuchi, M.; Kyogashima, M.; Aoyama, T.; Hara, A. Long-term improvement of oxidative stress via kidney transplantation ameliorates serum sulfatide levels. Clin. Exp. Nephrol. 2012, 16, 959–967. [Google Scholar] [CrossRef]
- Wang, L.; Kamijo, Y.; Matsumoto, A.; Nakajima, T.; Higuchi, M.; Kannagi, R.; Kyogashima, M.; Aoyama, T.; Hara, A. Kidney transplantation recovers the reduction level of serum sulfatide in ESRD patients via processes correlated to oxidative stress and platelet count. Glycoconj. J. 2011, 28, 125–135. [Google Scholar] [CrossRef][Green Version]
- Yuzhe, H.; Kamijo, Y.; Hashimoto, K.; Harada, M.; Kanno, T.; Sugiyama, E.; Kyogashima, M.; Oguchi, T.; Nakajima, T.; Kanno, Y.; et al. Serum sulfatide abnormality is associated with increased oxidative stress in hemodialysis patients. Hemodial. Int. 2015, 19, 429–438. [Google Scholar] [CrossRef]
- Tedesco, M.; Gallieni, M.; Pellegata, F.; Cozzolino, M.; Alberici, F. Update on ANCA-associated vasculitis: From biomarkers to therapy. J. Nephrol. 2019, 32, 871–882. [Google Scholar] [CrossRef]
- Monach, P.A.; Tomasson, G.; Specks, U.; Stone, J.H.; Cuthbertson, D.; Krischer, J.; Ding, L.; Fervenza, F.C.; Fessler, B.J.; Hoffman, G.S.; et al. Circulating markers of vascular injury and angiogenesis in antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum. 2011, 63, 3988–3997. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AAV (n = 35) | Control (n = 10) | p-Value | |||
|---|---|---|---|---|---|
| Age (years) | 74 ± 11 | 57 ± 8 | * <0.001 | ||
| Male (n,%) | 20 | 57.1 | 3 | 30.0 | 0.17 |
| BMI (kg/m2) | 22.4 ± 3.7 | 23.4 ± 3.4 | 0.43 | ||
| Systolic BP (mmHg) | 143 ± 27 | 113 ± 8 | * 0.002 | ||
| Diastolic BP (mmHg) | 80 ± 14 | 70 ± 8 | * 0.041 | ||
| Heart rate (beats/min) | 75 ± 14 | 71 ± 9 | 0.38 | ||
| Diabetes mellitus (n,%) | 10 | 28.6 | 2 | 20.0 | 0.71 |
| Hypertension (n,%) | 24 | 68.6 | 1 | 10.0 | * 0.002 |
| Smoking history (n,%) | 20 | 54.3 | 4 | 40.0 | 0.49 |
| Malignancy (n,%) | 8 | 22.9 | 0 | 0.0 | 0.17 |
| Laboratory data | |||||
| Total protein (g/dL) | 6.3 ± 0.8 | 7.1 ± 0.4 | * 0.005 | ||
| Albumin (g/dL) | 2.8 ± 0.7 | 4.3 ± 0.3 | * <0.001 | ||
| BUN (mg/dL) | 47.4 (31.3–75.4) | 14.5 (13.5–16.8) | * <0.001 | ||
| Cre (mg/dL) | 3.4 (2.0–5.1) | 0.7 (0.6–0.9) | * <0.001 | ||
| eGFR (mL/min/1.73 m2) | 12.7 (8.1–23.7) | 72.3 (76.6) | * <0.001 | ||
| CRP (mg/dL) | 2.89 (0.38–8.18) | 0.04 (0.02–0.11) | * <0.001 | ||
| Total cholesterol (mg/dL) | 176 ± 36 | 222 ± 39 | * 0.001 | ||
| HDL-C (mg/dL) | 40 ± 15 | 61 ± 18 | * 0.001 | ||
| LDL-C (mg/dL) | 103 ± 28 | 127 ± 28 | * 0.023 | ||
| Triglycerides (mg/dL) | 120 (100–167) | 153 (81–183) | 0.69 | ||
| Soluble TM (U/mL) | 44.1 (35.2–56.6) | 13.8 (11.6–15.9) | * <0.001 | ||
| Pentraxin3 (ng/mL) | 6.8 (5.6–39.1) | 1.6 (1.2–2.2) | * <0.001 | ||
| Serum sulfatides (nmol/mL) | 5.44 ± 2.14 | 8.53 ± 1.28 | * <0.001 | ||
| Lysosulfatides-d18:2 (nmol/mL) | 1.52 ± 0.71 | 2.16 ± 0.44 | * 0.009 | ||
| Lysosulfatides-d18:1 (nmol/mL) | 3.47 ± 1.31 | 5.67 ± 0.91 | * <0.001 | ||
| Lysosulfatides-t18:0 (nmol/mL) | 0.38 ± 0.23 | 0.61 ± 0.16 | * 0.006 | ||
| White blood cell count (/µL) | 6800 (5650–10,890) | 5480 (4332–7462) | 0.10 | ||
| Hemoglobin (g/dL) | 9.7 ± 1.6 | 14.1 ± 1.2 | *<0.001 | ||
| Platelet count (×104/µL) | 29.9 ± 12.2 | 26.8 ± 5.3 | 0.45 | ||
| Hematuria (n,%) | 34 | 97.1 | 1 | 10.0 | * <0.001 |
| Proteinuria (n,%) | 32 | 91.4 | 0 | 0.0 | * <0.001 |
| Clinical events | |||||
| ESKD (n,%) | 12 | 34.3 | - | - | - |
| All-cause death (n,%) | 2 | 5.7 | - | - | - |
| AAV-related data | |||||
| MPO-ANCA (n,%) | 35 | 100 | - | - | - |
| PR3-ANCA (n,%) | 0 | 0 | - | - | - |
| MPO-ANCA titer (U/mL) | 316 ± 326 | - | - | - | |
| Interstitial lung lesion (n,%) | 19 | 54.3 | - | - | - |
| Alveolar hemorrhage (n,%) | 6 | 17.1 | - | - | - |
| Neurological disorder (n,%) | 4 | 11.4 | - | - | - |
| BVAS | 18 | 11–26 | - | - | - |
| Treatment pattern | |||||
| PSL (maximum) (mg/kg/day) | 0.71 | - | - | - | |
| mPSL pulse (n,%) | 28 | 80.0 | - | - | - |
| CY (n,%) | 7 | 20.0 | - | - | - |
| Rituximab (n,%) | 6 | 17.1 | - | - | - |
| Plasma exchange (n,%) | 7 | 20.0 | - | - | - |
| TMP-SMX (n,%) | 34 | 97.1 | - | - | - |
| Histopathologic Classification of ANCA-Associated Glomerulonephritis | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Focal | Crescentic | Mixed | Sclerotic | p-Value | |||||
| n = 11 | n = 3 | n = 10 | n = 3 | ||||||
| Age (years) | 73 ± 7 | 62 ± 16 | 71 ± 10 | 71 ± 16 | 0.51 | ||||
| Male (n,%) | 6 | 54.5 | 1 | 33.3 | 6 | 60.0 | 1 | 33.3 | 0.84 |
| BMI (kg/m2) | 22.3 (20.4–23.6) | 22.6 (22.6–24.8) | 22.5 (20.4–23.7) | 19.9 (19.4–25.2) | 0.76 | ||||
| Systolic BP (mmHg) | 129 ± 25 | 136 ± 26 | 159 ± 30 | 142 ± 27 | 0.13 | ||||
| Diastolic BP (mmHg) | 73 ± 11 | 81 ± 19 | 88 ± 16 | 82 ± 12 | 0.13 | ||||
| Heart rate (/min) | 73 ± 12 | 96 ± 17 | 74 ± 11 | 78 ± 15 | 0.06 | ||||
| Diabetes mellitus (n,%) | 5 | 45.4 | 0 | 0 | 3 | 30.0 | 0 | 0 | 0.36 |
| Hypertension (n,%) | 8 | 72.7 | 1 | 33.3 | 7 | 70.0 | 2 | 66.7 | 0.73 |
| Smoking history (n,%) | 6 | 54.5 | 1 | 33.3 | 7 | 70.0 | 1 | 33.3 | 0.63 |
| Malignancy (n,%) | 1 | 9.1 | 1 | 33.3 | 3 | 30.0 | 0 | 0 | 0.40 |
| Laboratory data | |||||||||
| Total protein (g/dL) | 6.6 ± 0.8 | 6.1 ± 0.4 | 6.3 ± 0.5 | 7.4 ± 0.3 | 0.06 | ||||
| Albumin (g/dL) | 2.9 ± 0.5 | 2.0 ± 1.0 | 3.1 ± 0.6 | 3.1 ± 0.7 | 0.12 | ||||
| eGFR (mL/min/1.73 m2) | 29.2 (17.6–51.8) | 10.9 (7.3–12.8) | 10.1 (7.4–15.7) | 13.3 (11.6–16.4) | * 0.016 | ||||
| CRP (mg/dL) | 3.4 (0.6–7.0) | 17.3 (10.2–21.3) | 0.4 (0.1–0.9) | 0.8 (0.5–3.4) | 0.11 | ||||
| Soluble TM (U/mL) | 25.3 (20.1–35.9) | 49.4 (46.8–73.6) | 51.2 (39.1–59.6) | 47.2 (43.6–49.6) | * 0.014 | ||||
| Bold is Pentraxin3 (ng/mL) | 6.8 (2.9–22.0) | 55.4 (46.8–76.5) | 6.4 (5.3–10.2) | 5.0 (5.0–22.5) | 0.14 | ||||
| Serum sulfatides (nmol/mL) | 5.1 ± 1.7 | 2.7 ± 1.9 | 7.5 ± 1.6 | 5.6 ± 1.1 | * <0.001 | ||||
| White blood cell count (/µL) | 8790 (6310–14,450) | 4828 (2928–7749) | 6400 (5862–8430) | 5810 (4455–6855) | 0.23 | ||||
| Hemoglobin (g/dL) | 10.8 ± 1.4 | 9.1 ± 2.0 | 9.6 ± 1.3 | 8.1 ± 0.4 | * 0.028 | ||||
| Platelet count (×104/µL) | 36.3 ± 12.2 | 30.4 ± 2.8 | 25.6 ± 7.4 | 41.2 ± 15.9 | 0.07 | ||||
| FDP D-dimer (µg/mL) | 2.9 (1.7–3.5) | 17.2 (13.1–26.8) | 4.9 (3.1–6.7) | 3.8 (2.8–4.5) | * 0.017 | ||||
| Hematuria (n,%) | 11 | 100 | 3 | 100 | 9 | 90.0 | 3 | 100 | 0.59 |
| Proteinuria (n,%) | 11 | 100 | 3 | 100 | 10 | 100 | 3 | 100 | - |
| Clinical events | |||||||||
| ESKD (n,%) | 1 | 9.1 | 2 | 66.7 | 3 | 30.0 | 0 | 0 | 0.12 |
| All cause death (n,%) | 0 | 0 | 0 | 0 | 1 | 10.0 | 0 | 0 | 0.59 |
| AAV-related data | |||||||||
| MPO-ANCA (n,%) | 11 | 100 | 3 | 100 | 10 | 100 | 3 | 100 | - |
| PR3-ANCA (n,%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - |
| MPO-ANCA titer (U/mL) | 289 (128–383) | 72 (41–616) | 194 (145–229) | 507 (268–674) | 0.60 | ||||
| Interstitial lung lesion (n,%) | 6 | 54.5 | 3 | 100 | 5 | 50.0 | 1 | 33.3 | 0.50 |
| Alveolar hemorrhage (n,%) | 2 | 18.2 | 1 | 33.3 | 1 | 10.0 | 0 | 0 | 0.86 |
| Neurological disorder (n,%) | 2 | 18.2 | 0 | 0 | 1 | 10.0 | 0 | 0 | 1.00 |
| BVAS | 18 ± 4 | 21 ± 4 | 18 ± 2 | 16 ± 4 | 0.33 | ||||
| Treatment pattern | |||||||||
| PSL (maximum) (mg/kg/day) | 0.74 ± 0.11 | 0.63 ± 0.14 | 0.75 ± 0.15 | 0.70 ± 0.14 | 0.57 | ||||
| mPSL pulse (n,%) | 9 | 81.8 | 3 | 100 | 10 | 100 | 2 | 66.7 | 0.42 |
| CY (n,%) | 3 | 27.3 | 0 | 0 | 2 | 20.0 | 2 | 66.7 | 0.43 |
| Rituximab (n,%) | 1 | 9.1 | 0 | 0 | 3 | 30.0 | 1 | 33.3 | 0.40 |
| Plasma exchange (n,%) | 2 | 18.2 | 1 | 33.3 | 2 | 20.0 | 0 | 0 | 1.00 |
| TMP-SMX (n,%) | 11 | 100 | 3 | 100 | 10 | 100 | 3 | 100 | - |
| r | p Value | |
|---|---|---|
| Serum sulfatides | ||
| Active glomerular crescent (%) | −0.265 | 0.18 |
| Global sclerosis (%) | 0.151 | 0.45 |
| C-reactive protein | ||
| Active glomerular crescent (%) | 0.161 | 0.42 |
| Global sclerosis (%) | −0.272 | 0.17 |
| FDP D-dimer | ||
| Active glomerular crescent (%) | 0.641 | * <0.001 |
| Global sclerosis (%) | −0.008 | 0.97 |
| eGFR | ||
| Active glomerular crescent (%) | −0.549 | * 0.003 |
| Global sclerosis (%) | −0.473 | * 0.013 |
| Soluble thrombomodulin | ||
| Active glomerular crescent (%) | 0.583 | * 0.001 |
| Global sclerosis (%) | 0.327 | 0.10 |
| MPO-ANCA titer | ||
| Active glomerular crescent (%) | 0.080 | 0.69 |
| Global sclerosis (%) | −0.072 | 0.72 |
| Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Serum sulfatides | 1.03 | 0.14–11.1 | 0.88 |
| C-reactive protein | 1.01 | 0.90–1.12 | 0.92 |
| FDP D-dimer | 0.99 | 0.89–1.11 | 0.91 |
| eGFR | 0.91 | 0.83–0.99 | * 0.028 |
| Soluble thrombomodulin | 1.07 | 1.00–1.14 | * 0.041 |
| MPO-ANCA titer | 1.00 | 0.99–1.01 | 0.13 |
| Serum Sulfatide Levels | ||
|---|---|---|
| r | p Value | |
| Age (years) | −0.036 | 0.84 |
| BMI (kg/m2) | 0.006 | 0.98 |
| Systolic BP (mmHg) | 0.296 | 0.08 |
| Diastolic BP (mmHg) | 0.143 | 0.41 |
| Heart rate (beats/min) | −0.197 | 0.26 |
| BVAS | −0.102 | 0.56 |
| Alb (g/dL) | 0.510 | * 0.002 |
| eGFR (mL/min/1.73 m2) | 0.011 | 0.95 |
| C-reactive protein (mg/dL) | −0.713 | * <0.001 |
| White blood cell count (/µL) | −0.208 | 0.23 |
| Hemoglobin (g/dL) | 0.111 | 0.53 |
| Platelet count (×104/µL) | −0.036 | 0.84 |
| Total cholesterol (mg/dL) | 0.722 | * <0.001 |
| HDL-C (mg/dL) | 0.559 | * <0.001 |
| LDL-C (mg/dL) | 0.527 | * 0.001 |
| Triglyceride (mg/dL) | 0.064 | 0.71 |
| Fibrinogen (mg/dL) | −0.098 | 0.58 |
| FDP-D dimer (μg/mL) | −0.306 | 0.07 |
| Soluble thrombomodulin (U/mL) | 0.052 | 0.76 |
| Pentraxin3 (ng/mL) | −0.460 | * 0.005 |
| MPO-ANCA titer (U/mL) | 0.039 | 0.82 |
| Odds Ratio | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Death | 1.02 | 0.52–2.00 | 0.96 |
| End stage kidney diseases | 1.07 | 0.74–1.56 | 0.71 |
| Alveolar hemorrhage | 1.09 | 0.72–1.66 | 0.67 |
| Interstitial lung lesion | 0.91 | 0.66–1.25 | 0.56 |
| Nerve disorder | 0.73 | 0.42–1.28 | 0.28 |
| Thrombotic complications | 0.88 | 0.49–1.56 | 0.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harada, M.; Nakajima, T.; Yamada, Y.; Aomura, D.; Yamaguchi, A.; Sonoda, K.; Tanaka, N.; Hashimoto, K.; Kamijo, Y. Serum Sulfatide Levels as a Biomarker of Active Glomerular Lesion in Patients with Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single Center Pilot Study. J. Clin. Med. 2022, 11, 762. https://doi.org/10.3390/jcm11030762
Harada M, Nakajima T, Yamada Y, Aomura D, Yamaguchi A, Sonoda K, Tanaka N, Hashimoto K, Kamijo Y. Serum Sulfatide Levels as a Biomarker of Active Glomerular Lesion in Patients with Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single Center Pilot Study. Journal of Clinical Medicine. 2022; 11(3):762. https://doi.org/10.3390/jcm11030762
Chicago/Turabian StyleHarada, Makoto, Takero Nakajima, Yosuke Yamada, Daiki Aomura, Akinori Yamaguchi, Kosuke Sonoda, Naoki Tanaka, Koji Hashimoto, and Yuji Kamijo. 2022. "Serum Sulfatide Levels as a Biomarker of Active Glomerular Lesion in Patients with Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single Center Pilot Study" Journal of Clinical Medicine 11, no. 3: 762. https://doi.org/10.3390/jcm11030762
APA StyleHarada, M., Nakajima, T., Yamada, Y., Aomura, D., Yamaguchi, A., Sonoda, K., Tanaka, N., Hashimoto, K., & Kamijo, Y. (2022). Serum Sulfatide Levels as a Biomarker of Active Glomerular Lesion in Patients with Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single Center Pilot Study. Journal of Clinical Medicine, 11(3), 762. https://doi.org/10.3390/jcm11030762