
Prevention and Treatment of Grade C Postoperative Pancreatic Fistula

Abstract
1. Introduction
2. Risk Factors for Grade C POPF
3. The Relationship between Infection and Grade C POPF
3.1. Different Sources of Infection between PD and DP
3.2. Hypothesis 1: Intestinal Microorganisms Develop Grade C POPF in PD
3.3. Hypothesis 2: Some Intestinal Microbes Enter the Abdominal Cavity by Bacterial Translocation
4. Operation Technique
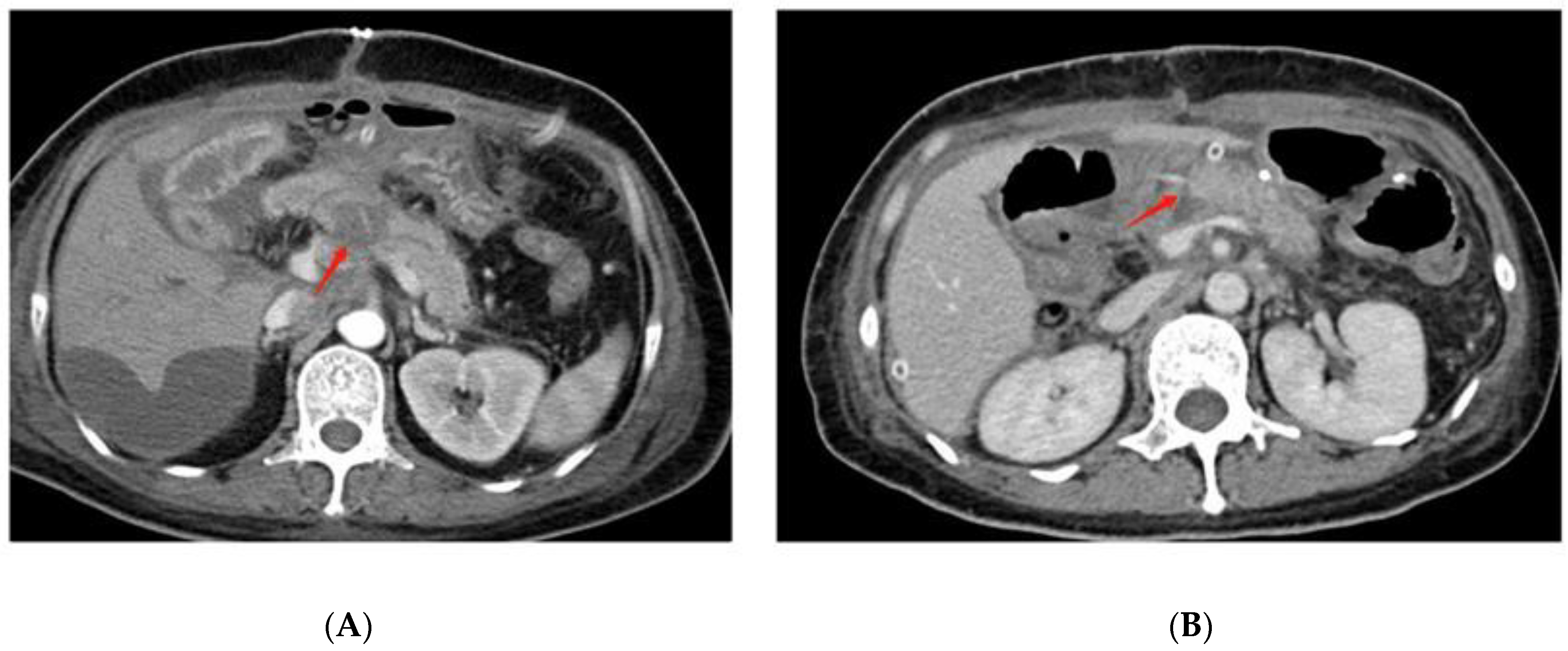
4.1. Pancreaticojejunostomy Dehiscence Is Found in Grade C POPF after PD on Radiographic Examination
4.2. Reconstruction Methods
4.3. Anastomotic Techniques
4.4. Stent or No-Stent
4.5. Two-Stage Surgical Procedure
5. Perioperative Management According to BT Theory
5.1. Mechanical Bowel Preparation Disturbs the Intestinal Mucosal Immune Barrier
5.2. Avoid Excessive Fluid after Surgery to Reduce Intestinal Edema
5.3. Oral Nutrition Is Beneficial for Maintaining Intestinal Mucosal Immunity
6. Surgical Treatment for Grade C POPF
6.1. Debridement and Open Drainage
6.2. Completion Pancreatectomy
6.3. Revision of the Pancreatic Anastomosis
6.4. The Bridge Stent Technique
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kleespies, A.; Albertsmeier, M.; Obeidat, F.; Seeliger, H.; Jauch, K.-W.; Bruns, C.J. The challenge of pancreatic anastomosis. Langenbeck’s Arch. Surg. 2008, 393, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhu, F.; Shen, M.; Tian, R.; Shi, C.J.; Wang, X.; Jiang, J.X.; Hu, J.; Wang, M.; Qin, R.Y. Systematic review and meta-analysis comparing three techniques for pancreatic remnant closure following distal pancreatectomy. Br. J. Surg. 2015, 102, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Lubrano, J.; Bachelier, P.; Paye, F.; Le Treut, Y.P.; Chiche, L.; Sa-Cunha, A.; Turrini, O.; Menahem, B.; Launoy, G.; Delpero, J.-R. Severe postoperative complications decrease overall and disease free survival in pancreatic ductal adenocarcinoma after pancreaticoduodenectomy. Eur. J. Surg. Oncol. 2018, 44, 1078–1082. [Google Scholar] [CrossRef]
- Yekebas, E.F.; Wolfram, L.; Cataldegirmen, G.; Habermann, C.R.; Bogoevski, D.; Koenig, A.M.; Kaifi, J.; Schurr, P.G.; Bubenheim, M.; Nolte-Ernsting, C.; et al. Postpancreatectomy hemorrhage: Diagnosis and treatment: An analysis in 1669 consecutive pancreatic resections. Ann. Surg. 2007, 246, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Chen, Y.-L.; Dong, J.-H.; Chen, M.-Y.; Cai, S.-W.; Huang, Z.-Q. Post-pancreaticoduodenectomy hemorrhage risk factors, managements and outcomes. Hepatobiliary Pancreat. Dis. Int. 2014, 13, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Dervenis, C.; Butturini, G.; Fingerhut, A.; Yeo, C.; Izbicki, J.; Neoptolemos, J.; Sarr, M.; Traverso, W.; Buchler, M. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005, 138, 8–13. [Google Scholar] [CrossRef]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Hilal, M.A.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef]
- Fu, S.-J.; Shen, S.-L.; Li, S.-Q.; Hu, W.-J.; Hua, Y.-P.; Kuang, M.; Liang, L.-J.; Peng, B.-G. Risk factors and outcomes of postoperative pancreatic fistula after pancreatico-duodenectomy: An audit of 532 consecutive cases. BMC Surg. 2015, 15, 34. [Google Scholar] [CrossRef]
- Pedrazzoli, S. Pancreatoduodenectomy (PD) and postoperative pancreatic fistula (POPF): A systematic review and analysis of the POPF-related mortality rate in 60,739 patients retrieved from the English literature published between 1990 and 2015. Medicine 2017, 96, e6858. [Google Scholar] [CrossRef]
- Fuks, D.; Piessen, G.; Huet, E.; Tavernier, M.; Zerbib, P.; Michot, F.; Scotté, M.; Triboulet, J.-P.; Mariette, C.; Chiche, L.; et al. Life-threatening postoperative pancreatic fistula (grade C) after pancreaticoduodenectomy: Incidence, prognosis, and risk factors. Am. J. Surg. 2009, 197, 702–709. [Google Scholar] [CrossRef]
- Denbo, J.W.; Orr, W.S.; Zarzaur, B.L.; Behrman, S.W. Toward defining grade C pancreatic fistula following pancreaticoduodenectomy: Incidence, risk factors, management and outcome. HPB 2012, 14, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Luu, A.M.; Krasemann, L.; Fahlbusch, T.; Belyaev, O.; Janot-Matuschek, M.; Uhl, W.; Braumann, C. Facing the surgeon’s nightmare: Incidence and management of postoperative pancreatic fistulas grade C after pancreaticoduodenectomy based on the updated definition of the International Study Group of Pancreatic Surgery (ISGPS). J. Hepato-Biliary-Pancreat. Sci. 2020, 27, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Hirono, S.; Shimokawa, T.; Nagakawa, Y.; Shyr, Y.; Kawai, M.; Matsumoto, I.; Satoi, S.; Yoshitomi, H.; Okabayashi, T.; Motoi, F.; et al. Risk factors for pancreatic fistula grade C after pancreatoduodenectomy: A large prospective, multicenter Japan-Taiwan collaboration study. J. Hepato-Biliary-Pancreat. Sci. 2020, 27, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Kopljar, M.; Čoklo, M.; Krstačić, A.; Krstačić, G.; Jeleč, V.; Zovak, M.; Pavić, R.; Kondža, G. Retrorenal fat predicts grade C pancreatic fistula after pancreaticoduodenectomy. ANZ J. Surg. 2020, 90, 2472–2477. [Google Scholar] [CrossRef] [PubMed]
- Chiba, N.; Ochiai, S.; Yokozuka, K.; Gunji, T.; Sano, T.; Tomita, K.; Tsutsui, R.; Kawachi, S. Risk Factors for Life-threatening Grade C Postoperative Pancreatic Fistula After Pancreatoduodenectomy Compared to Grade B. Anticancer Res. 2019, 39, 2199–2205. [Google Scholar] [CrossRef]
- Hata, T.; Mizuma, M.; Motoi, F.; Nakagawa, K.; Masuda, K.; Ishida, M.; Morikawa, T.; Hayashi, H.; Kamei, T.; Naitoh, T.; et al. Early postoperative drainage fluid culture positivity from contaminated bile juice is predictive of pancreatic fistula after pancreaticoduodenectomy. Surg. Today 2020, 50, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Kato, D.; Sasaki, T.; Shiwaku, H.; Ishii, F.; Naito, S.; Yamashita, Y.; Hasegawa, S. Contaminated drainage fluid and pancreatic fistula after pancreatoduodenectomy: A retrospective study. Int. J. Surg. 2018, 52, 314–319. [Google Scholar] [CrossRef]
- Nappo, G.; Capretti, G.L.; Petitti, T.; Gavazzi, F.; Ridolfi, C.; Cereda, M.; Montorsi, M.; Zerbi, A. The evolution of post-operative pancreatic fistula (POPF) classification: A single-center experience. Pancreatology 2019, 19, 449–455. [Google Scholar] [CrossRef]
- McMillan, M.T.; Christein, J.D.; Callery, M.P.; Behrman, S.W.; Drebin, J.A.; Hollis, R.H.; Kent, T.S.; Miller, B.C.; Sprys, M.H.; Watkins, A.A.; et al. Comparing the burden of pancreatic fistulas after pancreatoduodenectomy and distal pancreatectomy. Surgery 2016, 159, 1013–1022. [Google Scholar] [CrossRef]
- McMillan, M.T.; Vollmer, C.M., Jr.; Asbun, H.J.; Ball, C.G.; Bassi, C.; Beane, J.D.; Berger, A.C.; Bloomston, M.; Callery, M.P.; Christein, J.D.; et al. The Characterization and Prediction of ISGPF Grade C Fistulas Following Pancreatoduodenectomy. J. Gastrointest. Surg. 2016, 20, 262–276. [Google Scholar] [CrossRef]
- Srivastava, S.; Sikora, S.; Kumar, A.; Saxena, R.; Kapoor, V. Outcome following pancreaticoduodenectomy in patients undergoing preoperative biliary drainage. Dig. Surg. 2001, 18, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Ohgi, K.; Sugiura, T.; Yamamoto, Y.; Okamura, Y.; Ito, T.; Uesaka, K. Bacterobilia may trigger the development and severity of pancreatic fistula after pancreatoduodenectomy. Surgery 2016, 160, 725–730. [Google Scholar] [CrossRef]
- Müssle, B.; Hempel, S.; Kahlert, C.; Distler, M.; Weitz, J.; Welsch, T. Prognostic Impact of Bacterobilia on Morbidity and Postoperative Management after Pancreatoduodenectomy: A Systematic Review and Meta-analysis. World J. Surg. 2018, 42, 2951–2962. [Google Scholar] [CrossRef]
- Li, G.-Q.; Zhang, T.; Yang, W.-G.; Zhong, H.-L.; Xiao, P.; Liu, L.-W.; Wang, Y.-W.; Chen, H.; Kong, R.; Wang, G.; et al. Gut microbiota patterns associated with somatostatin in patients undergoing pancreaticoduodenectomy: A prospective study. Cell Death Discov. 2020, 6, 94. [Google Scholar] [CrossRef]
- Langheinrich, M.; Wirtz, S.; Kneis, B.; Gittler, M.M.; Tyc, O.; Schierwagen, R.; Brunner, M.; Krautz, C.; Weber, G.F.; Pilarsky, C.; et al. Microbiome Patterns in Matched Bile, Duodenal, Pancreatic Tumor Tissue, Drainage, and Stool Samples: Association with Preoperative Stenting and Postoperative Pancreatic Fistula Development. J. Clin. Med. 2020, 9, 2785. [Google Scholar] [CrossRef] [PubMed]
- Loos, M.; Strobel, O.; Legominski, M.; Dietrich, M.; Hinz, U.; Brenner, T.; Heininger, A.; Weigand, M.A.; Büchler, M.W.; Hackert, T. Postoperative pancreatic fistula: Microbial growth determines outcome. Surgury 2018, 164, 1185–1190. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Jin, C.; Hao, S.; Fu, D. Drain Contamination after Distal Pancreatectomy: Incidence, Risk Factors, and Association with Postoperative Pancreatic Fistula. J. Gastrointest. Surg. 2019, 23, 2449–2458. [Google Scholar] [CrossRef]
- Abe, K.; Kitago, M.; Shinoda, M.; Yagi, H.; Abe, Y.; Oshima, G.; Hori, S.; Yokose, T.; Endo, Y.; Kitagawa, Y. High risk pathogens and risk factors for postoperative pancreatic fistula after pancreatectomy; a retrospective case-controlled study. Int. J. Surg. 2020, 82, 136–142. [Google Scholar] [CrossRef]
- Lacour, M.; Zunder, T.; Huber, R.; Sander, A.; Daschner, F.; Frank, U. The pathogenetic significance of intestinal Candida colonization—A systematic review from an interdisciplinary and environmental medical point of view. Int. J. Hyg. Environ. Health 2002, 205, 257–268. [Google Scholar] [CrossRef]
- Demir, E.; Abdelhai, K.; Demir, I.E.; Jäger, C.; Scheufele, F.; Schorn, S.; Rothe, K.; Friess, H.; Ceyhan, G.O. Association of bacteria in pancreatic fistula fluid with complications after pancreatic surgery. BJS Open 2020, 4, 432–437. [Google Scholar] [CrossRef]
- Van Buren, G.; Bloomston, M.; Schmidt, C.R.; Behrman, S.W.; Zyromski, N.J.; Ball, C.G.; Morgan, K.A.; Hughes, S.J.; Karanicolas, P.J.; Allendorf, J.D.; et al. A Prospective Randomized Multicenter Trial of Distal Pancreatectomy with and without Routine Intraperitoneal Drainage. Ann. Surg. 2017, 266, 421–431. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, R.; Kabir, C.; Maker, V.; Banulescu, M.; Wasserman, M.; Maker, A. Do Drains Contribute to Pancreatic Fistulae? Analysis of over 5000 Pancreatectomy Patients. J. Gastrointest. Surg. 2018, 22, 1007–1015. [Google Scholar] [CrossRef]
- Wolochow, H.; Hildebrand, G.J.; Lamanna, C. Translocation of Microorganisms Across the Intestinal Wall of the Rat: Effect of Microbial Size and Concentration. J. Infect. Dis. 1966, 116, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Brenchley, J.M.; Douek, D.C. Microbial Translocation Across the GI Tract. Annu. Rev. Immunol. 2012, 30, 149–173. [Google Scholar] [CrossRef] [PubMed]
- Deitch, E.A. Gut-origin sepsis: Evolution of a concept. Surgeon 2012, 10, 350–356. [Google Scholar] [CrossRef] [PubMed]
- MacFie, J.; O’Boyle, C.; Mitchell, C.J.; Buckley, P.M.; Johnstone, D.; Sudworth, P. Gut origin of sepsis: A prospective study investigating associations between bacterial translocation, gastric microflora, and septic morbidity. Gut 1999, 45, 223–228. [Google Scholar] [CrossRef]
- Komatsu, S.; Yokoyama, Y.; Nagino, M. Gut microbiota and bacterial translocation in digestive surgery: The impact of probiotics. Langenbeck’s Arch. Surg. 2017, 402, 401–416. [Google Scholar] [CrossRef]
- Shiomi, H.; Shimizu, T.; Endo, Y.; Murata, S.; Kurumi, Y.; Uji, Y.; Tani, T. Relations Among Circulating Monocytes, Dendritic Cells, and Bacterial Translocation in Patients with Intestinal Obstruction. World J. Surg. 2007, 31, 1806–1812. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, J.W.; Hur, Y.H.; Lee, B.K.; Cho, S.B.; Hwang, E.C.; Lee, S.J.; Yoon, E.J.; Seon, H.J. Multidetector CT findings differ between surgical grades of pancreatic fistula after pancreaticoduodenectomy. Eur. Radiol. 2019, 29, 2399–2407. [Google Scholar] [CrossRef]
- Yang, J.; Li, Y.-C.; Liu, X.-B.; Tan, C.-L. Infection and image findings to predict delayed hemorrhage in postoperative pancreatic fistula patients after pancreaticoduodenectomy. Asian J. Surg. 2022, 45, 1130–1131. [Google Scholar] [CrossRef]
- Keck, T.; Wellner, U.F.; Bahra, M.; Klein, F.; Sick, O.; Niedergethmann, M.; Wilhelm, T.J.; Farkas, S.A.; Börner, T.; Bruns, C.; et al. Pancreatogastrostomy versus Pancreatojejunostomy for RECOnstruction After PANCreatoduodenectomy (RECOPANC, DRKS 00000767): Perioperative and Long-term Results of a Multicenter Randomized Controlled Trial. Ann. Surg. 2016, 263, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Perivoliotis, K.; Sioka, E.; Tatsioni, A.; Stefanidis, I.; Zintzaras, E.; Zacharoulis, D. Pancreatogastrostomy versus Pancreatojejunostomy: An Up-to-Date Meta-Analysis of RCTs. Int. J. Surg. Oncol. 2017, 2017, 7526494. [Google Scholar] [CrossRef]
- Cheng, Y.; Briarava, M.; Lai, M.; Wang, X.; Tu, B.; Cheng, N.; Gong, J.; Yuan, Y.; Pilati, P.; Mocellin, S. Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction for the prevention of postoperative pancreatic fistula following pancreaticoduodenectomy. Cochrane Database Syst. Rev. 2017, 9, CD012257. [Google Scholar] [CrossRef]
- Ratnayake, C.B.; Wells, C.I.; Kamarajah, S.K.; Loveday, B.; Sen, G.; French, J.J.; White, S.; Pandanaboyana, S. Critical appraisal of the techniques of pancreatic anastomosis following pancreaticoduodenectomy: A network meta-analysis. Int. J. Surg. 2020, 73, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Feng, Y.-Y.; Qi, X.-G.; Hao, G.; Yu, Y.-Q.; Li, J.-T.; Peng, S.-Y. Pancreatogastrostomy vs pancreatojejunostomy after pancreaticoduodenectomy: An updated meta-analysis of RCTs and our experience. World J. Gastrointest. Surg. 2019, 11, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Zhang, Z.; Gu, C.; Liu, Q.; Liang, Z.; He, W.; Chen, J.; Lai, J. The optimal choice for pancreatic anastomosis after pancreaticoduodenectomy: A network meta-analysis of randomized control trials. Int. J. Surg. 2018, 57, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Lyu, Y.; Li, T.; Cheng, Y.; Wang, B.; Chen, L.; Zhao, S. Pancreaticojejunostomy Versus Pancreaticogastrostomy After Pancreaticoduodenectomy: An Up-to-date Meta-analysis of RCTs Applying the ISGPS (2016) Criteria. Surg. Laparosc. Endosc. Percutaneous Tech. 2018, 28, 139–146. [Google Scholar] [CrossRef]
- Wang, X.X.; Yan, Y.K.; Dong, B.L.; Li, Y.; Yang, X.J. Pancreatic outflow tract reconstruction after pancreaticoduodenectomy: A meta-analysis of randomized controlled trials. World J. Surg. Oncol. 2021, 19, 203. [Google Scholar] [CrossRef]
- Andrianello, S.; Marchegiani, G.; Malleo, G.; Masini, G.; Balduzzi, A.; Paiella, S.; Esposito, A.; Landoni, L.; Casetti, L.; Tuveri, M.; et al. Pancreaticojejunostomy with Externalized Stent vs Pancreaticogastrostomy with Externalized Stent for Patients with High-Risk Pancreatic Anastomosis: A Single-Center, Phase 3, Randomized Clinical Trial. JAMA Surg. 2020, 155, 313–321. [Google Scholar] [CrossRef]
- Senda, Y.; Shimizu, Y.; Natsume, S.; Ito, S.; Komori, K.; Abe, T.; Matsuo, K.; Sano, T. Randomized clinical trial of duct-to-mucosa versus invagination pancreaticojejunostomy after pancreatoduodenectomy. Br. J. Surg. 2018, 105, 48–57. [Google Scholar] [CrossRef]
- Lyu, Y.; Li, T.; Wang, B.; Cheng, Y.; Zhao, S. Selection of pancreaticojejunostomy technique after pancreaticoduodenectomy: Duct-to-mucosa anastomosis is not better than invagination anastomosis: A meta-analysis. Medicine 2018, 97, e12621. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Luo, W.; Qiu, J.; Liu, Y.; Zheng, L.; Zhang, T. Is Invagination Anastomosis More Effective in Reducing Clinically Relevant Pancreatic Fistula for Soft Pancreas after Pancreaticoduodenectomy Under Novel Fistula Criteria: A Systematic Review and Meta-Analysis. Front. Oncol. 2020, 10, 1637. [Google Scholar] [CrossRef] [PubMed]
- Kleespies, A.; Rentsch, M.; Seeliger, H.; Albertsmeier, M.; Jauch, K.; Bruns, C.J. Blumgart anastomosis for pancreaticojejunostomy minimizes severe complications after pancreatic head resection. Br. J. Surg. 2009, 96, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Casadei, R.; Ricci, C.; Ingaldi, C.; Alberici, L.; De Raffele, E.; Minni, F. Comparison of Blumgart Anastomosis with Duct-to-Mucosa Anastomosis and Invagination Pancreaticojejunostomy after Pancreaticoduodenectomy: A Single-Center Propensity Score Matching Analysis. J. Gastrointest. Surg. 2021, 25, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Menonna, F.; Napoli, N.; Kauffmann, E.F.; Iacopi, S.; Gianfaldoni, C.; Martinelli, C.; Amorese, G.; Vistoli, F.; Boggi, U. Additional modifications to the Blumgart pancreaticojejunostomy: Results of a propensity score-matched analysis versus Cattel-Warren pancreaticojejunostomy. Surgery 2021, 169, 954–962. [Google Scholar] [CrossRef]
- Ke, F.-Y.; Wu, X.-S.; Zhang, Y.; Zhang, H.-C.; Weng, M.-Z.; Liu, Y.-B.; Wolfgang, C.; Gong, W. Comparison of postoperative complications between internal and external pancreatic duct stenting during pancreaticoduodenectomy: A meta-analysis. Chin. J. Cancer Res. 2015, 27, 397–407. [Google Scholar] [CrossRef]
- Hong, S.; Wang, H.; Yang, S.; Yang, K. External stent versus no stent for pancreaticojejunostomy: A meta-analysis of randomized controlled trials. J. Gastrointest. Surg. 2013, 17, 1516–1525. [Google Scholar] [CrossRef]
- Patel, K.; Teta, A.; Sukharamwala, P.; Thoens, J.; Szuchmacher, M.; DeVito, P. External pancreatic duct stent reduces pancreatic fistula: A meta-analysis and systematic review. Int. J. Surg. 2014, 12, 827–832. [Google Scholar] [CrossRef]
- Pessaux, P.; Sauvanet, A.; Mariette, C.; Paye, F.; Muscari, F.; Cunha, A.S.; Sastre, B.; Arnaud, J.-P. External pancreatic duct stent decreases pancreatic fistula rate after pancreaticoduodenectomy: Prospective multicenter randomized trial. Ann. Surg. 2011, 253, 879–885. [Google Scholar] [CrossRef]
- Wang, G.; Li, L.; Ma, Y.; Qu, F.-Z.; Zhu, H.; Lv, J.-C.; Jia, Y.-H.; Wu, L.-F.; Sun, B. External Versus Internal Pancreatic Duct Drainage for the Early Efficacy after Pancreaticoduodenectomy: A Retrospectively Comparative Study. J. Investig. Surg. 2016, 29, 226–233. [Google Scholar] [CrossRef]
- Jiang, Y.; Chen, Q.; Shao, Y.; Gao, Z.; Jin, M.; Gao, B.; Zhou, B.; Yan, S. The prognostic value of external vs internal pancreatic duct stents after pancreaticoduodenectomy in patients with FRS ≥ 4: A retrospective cohort study. BMC Surg. 2021, 21, 81. [Google Scholar] [CrossRef] [PubMed]
- Stoop, T.F.; Ghorbani, P.; Scholten, L.; Bergquist, E.; Ateeb, Z.; van Dieren, S.; Holmberg, M.; Besselink, M.G.; Sparrelid, E.; Del Chiaro, M. Total pancreatectomy as an alternative to high-risk pancreatojejunostomy after pancreatoduodenectomy: A propensity score analysis on surgical outcome and quality of life. HPB 2022, 24, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Marchegiani, G.; Perri, G.; Burelli, A.; Zoccatelli, F.; Andrianello, S.; Luchini, C.; Donadello, K.; Bassi, C.; Salvia, R. High-risk Pancreatic Anastomosis versus Total Pancreatectomy after Pancreatoduodenectomy: Postoperative Outcomes and Quality of Life Analysis. Ann. Surg. 2022, 276, e905–e913. [Google Scholar] [CrossRef] [PubMed]
- Salvia, R.; Lionetto, G.; Perri, G.; Malleo, G.; Marchegiani, G. Total pancreatectomy and pancreatic fistula: Friend or foe? Updates Surg. 2021, 73, 1231–1236. [Google Scholar] [CrossRef]
- Aoki, T.; Sakamoto, Y.; Kohno, Y.; Akamatsu, N.; Kaneko, J.; Sugawara, Y.; Hasegawa, K.; Makuuchi, M.; Kokudo, N. Hepatopancreaticoduodenectomy for Biliary Cancer: Strategies for Near-zero Operative Mortality and Acceptable Long-term Outcome. Ann. Surg. 2018, 267, 332–337. [Google Scholar] [CrossRef]
- Hasegawa, K.; Kokudo, N.; Sano, K.; Seyama, Y.; Aoki, T.; Ikeda, M.; Hashimoto, T.; Beck, Y.; Imamura, H.; Sugawara, Y.; et al. Two-stage pancreatojejunostomy in pancreaticoduodenectomy: A retrospective analysis of short-term results. Am. J. Surg. 2008, 196, 3–10. [Google Scholar] [CrossRef]
- Yamazaki, S.; Takayama, T.; Mitsuka, Y.; Yoshida, N.; Shimamoto, N.; Higaki, T. Feasibility of Hyaluronate Carboxymethylcellulose-Based Bioresorbable Membrane in Two-Staged Pancreatojejunostomy. World J. Surg. 2020, 44, 902–909. [Google Scholar] [CrossRef]
- Holte, K.; Nielsen, K.G.; Madsen, J.L.; Kehlet, H. Physiologic Effects of Bowel Preparation. Dis. Colon Rectum 2004, 47, 1397–1402. [Google Scholar] [CrossRef]
- Cao, F.; Li, J.; Li, F. Mechanical bowel preparation for elective colorectal surgery: Updated systematic review and meta-analysis. Int. J. Color. Dis. 2012, 27, 803–810. [Google Scholar] [CrossRef]
- Rollins, K.E.; Javanmard-Emamghissi, H.; Lobo, D.N. Impact of mechanical bowel preparation in elective colorectal surgery: A meta-analysis. World J. Gastroenterol. 2018, 24, 519–536. [Google Scholar] [CrossRef]
- Toh, J.W.T.; Phan, K.; Hitos, K.; Pathma-Nathan, N.; El-Khoury, T.; Richardson, A.J.; Morgan, G.; Engel, A.; Ctercteko, G. Association of Mechanical Bowel Preparation and Oral Antibiotics before Elective Colorectal Surgery with Surgical Site Infection: A Network Meta-analysis. JAMA Netw. Open 2018, 1, e183226. [Google Scholar] [CrossRef] [PubMed]
- Lavu, H.; Kennedy, E.P.; Mazo, R.; Stewart, R.J.; Greenleaf, C.; Grenda, D.R.; Sauter, P.K.; Leiby, B.E.; Croker, S.P.; Yeo, C.J. Preoperative mechanical bowel preparation does not offer a benefit for patients who undergo pancreaticoduodenectomy. Surgery 2010, 148, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Deitch, E.A. Bacterial translocation or lymphatic drainage of toxic products from the gut: What is important in human beings? Surgery 2002, 131, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Tote, S.P.; Grounds, R.M. Performing perioperative optimization of the high-risk surgical patient. Br. J. Anaesth. 2006, 97, 4–11. [Google Scholar] [CrossRef]
- Yuan, J.; Sun, Y.; Pan, C.; Li, T. Goal-directed fluid therapy for reducing risk of surgical site infections following abdominal surgery—A systematic review and meta-analysis of randomized controlled trials. Int. J. Surg. 2017, 39, 74–87. [Google Scholar] [CrossRef]
- Heming, N.; Moine, P.; Coscas, R.; Annane, D. Perioperative fluid management for major elective surgery. Br. J. Surg. 2020, 107, e56–e62. [Google Scholar] [CrossRef]
- Gottin, L.; Martini, A.; Menestrina, N.; Schweiger, V.; Malleo, G.; Donadello, K.; Polati, E. Perioperative Fluid Administration in Pancreatic Surgery: A Comparison of Three Regimens. J. Gastrointest. Surg. 2020, 24, 569–577. [Google Scholar] [CrossRef]
- Gómez-Izquierdo, J.C.; Feldman, L.S.; Carli, F.; Baldini, G. Meta-analysis of the effect of goal-directed therapy on bowel function after abdominal surgery. Br. J. Surg. 2015, 102, 577–589. [Google Scholar] [CrossRef]
- Pearse, R.M.; Harrison, D.; Macdonald, N.; Gillies, M.A.; Blunt, M.; Ackland, G.; Grocott, M.; Ahern, A.; Griggs, K.; Scott, R.; et al. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: A randomized clinical trial and systematic review. JAMA 2014, 311, 2181–2190. [Google Scholar] [CrossRef]
- Wrzosek, A.; Jakowicka-Wordliczek, J.; Zajaczkowska, R.; Serednicki, W.T.; Jankowski, M.; Bala, M.M.; Swierz, M.J.; Polak, M.; Wordliczek, J. Perioperative restrictive versus goal-directed fluid therapy for adults undergoing major non-cardiac surgery. Cochrane Database Syst. Rev. 2019, 12, CD012767. [Google Scholar] [CrossRef]
- Chen, B.P.; Chen, M.; Bennett, S.; Lemon, K.; Bertens, K.A.; Balaa, F.K.; Martel, G. Systematic Review and Meta-analysis of Restrictive Perioperative Fluid Management in Pancreaticoduodenectomy. World J. Surg. 2018, 42, 2938–2950. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S.; Damiano, G.; Palumbo, V.D.; Spinelli, G.; Ficarella, S.; Monte, G.L.; Marrazzo, A.; Monte, A.I.L. Enteral Nutrition in Pancreaticoduodenectomy: A Literature Review. Nutrients 2015, 7, 3154–3165. [Google Scholar] [CrossRef] [PubMed]
- Sierzega, M.; Niekowal, B.; Kulig, J.; Popiela, T. Nutritional Status Affects the Rate of Pancreatic Fistula after Distal Pancreatectomy: A Multivariate Analysis of 132 Patients. J. Am. Coll. Surg. 2007, 205, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef]
- Cai, J.; Yang, G.; Tao, Y.; Han, Y.; Lin, L.; Wang, X. A meta-analysis of the effect of early enteral nutrition versus total parenteral nutrition on patients after pancreaticoduodenectomy. HPB 2020, 22, 20–25. [Google Scholar] [CrossRef]
- Adiamah, A.; Ranat, R.; Gomez, D. Enteral versus parenteral nutrition following pancreaticoduodenectomy: A systematic review and meta-analysis. HPB 2019, 21, 793–801. [Google Scholar] [CrossRef]
- Grižas, S.; Gulbinas, A.; Barauskas, G.; Pundzius, J. A comparison of the effectiveness of the early enteral and natural nutrition after pancreatoduodenectomy. Medicina 2008, 44, 678–686. [Google Scholar] [CrossRef]
- Li, J.; Kudsk, K.A.; Gocinski, B.; Dent, D.; Glezer, J.; Langkamp-Henken, B. Effects of Parenteral and Enteral Nutrition on Gut-Associated Lymphoid Tissue. J. Trauma Inj. Infect. Crit. Care 1995, 39, 44–52; discussion 51–42. [Google Scholar] [CrossRef]
- Lu, J.-W.; Liu, C.; Du, Z.-Q.; Liu, X.-M.; Lv, Y.; Zhang, X.-F. Early enteral nutritionvsparenteral nutrition following pancreaticoduodenectomy: Experience from a single center. World J. Gastroenterol. 2016, 22, 3821–3828. [Google Scholar] [CrossRef]
- Perinel, J.; Mariette, C.; Dousset, B.; Sielezneff, I.; Gainant, A.; Mabrut, J.-Y.; Bin-Dorel, S.; El Bechwaty, M.; Delaunay, D.; Bernard, L.; et al. Early Enteral Versus Total Parenteral Nutrition in Patients Undergoing Pancreaticoduodenectomy: A Randomized Multicenter Controlled Trial (Nutri-DPC). Ann. Surg. 2016, 264, 731–737. [Google Scholar] [CrossRef]
- Takagi, K.; Domagala, P.; Hartog, H.; Eijck, C.; Koerkamp, B.G. Current evidence of nutritional therapy in pancreatoduodenectomy: Systematic review of randomized controlled trials. Ann. Gastroenterol. Surg. 2019, 3, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, A.; Besselink, M.G.H.; Gouma, D.J.; Steenhagen, E.; Rinkes, I.H.M.B.; Molenaar, I.Q. Systematic review of five feeding routes after pancreatoduodenectomy. Br. J. Surg. 2013, 100, 589–598; discussion 599. [Google Scholar] [CrossRef] [PubMed]
- Adiamah, A.; Arif, Z.; Berti, F.; Singh, S.; Laskar, N.; Gomez, D. The Use of Prophylactic Somatostatin Therapy Following Pancreaticoduodenectomy: A Meta-analysis of Randomised Controlled Trials. World J. Surg. 2019, 43, 1788–1801. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.J.; Lee, O.; Jung, J.H.; Shin, S.H.; Heo, J.S.; Han, I.W. Prophylactic octreotide for postoperative pancreatic fistula in patients with pancreatoduodenectomy: Risk-stratified analysis. Medicine 2022, 101, e29303. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.S.; Joyce, D.; Brady, M.; Ms, A.G.; Attwood, K.; Kuvshinoff, B.; Hochwald, S.N.; Kukar, M. Risk-stratified analysis of pasireotide for patients undergoing pancreatectomy. J. Surg. Oncol. 2020, 122, 195–203. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Miyake, T.; Kokuryo, T.; Asahara, T.; Nomoto, K.; Nagino, M. Effect of Perioperative Synbiotic Treatment on Bacterial Translocation and Postoperative Infectious Complications after Pancreatoduodenectomy. Dig. Surg. 2016, 33, 220–229. [Google Scholar] [CrossRef]
- Tang, G.; Zhang, L.; Tao, J.; Wei, Z. Effects of Perioperative Probiotics and Synbiotics on Pancreaticoduodenectomy Patients: A Meta-Analysis of Randomized Controlled Trials. Front. Nutr. 2021, 8, 715788. [Google Scholar] [CrossRef]
- Zhou, Y.-M.; Zhou, X.; Wan, T.; Xu, D.; Si, X.-Y. An evidence-based approach to the surgical interventions for severe pancreatic fistula after pancreatoduodenectomy. Surgeon 2018, 16, 119–124. [Google Scholar] [CrossRef]
- Wroński, M.; Cebulski, W.; Witkowski, B.; Guzel, T.; Karkocha, D.; Lech, G.; Słodkowski, M. Surgical management of the grade C pancreatic fistula after pancreatoduodenectomy. HPB 2019, 21, 1166–1174. [Google Scholar] [CrossRef]
- Záruba, P.; Rousek, M.; Kočišová, T.; Havlová, K.; Ryska, M.; Pohnán, R. A comparison of surgical approaches in the treatment of grade C postoperative pancreatic fistula: A retrospective study. Front. Surg. 2022, 9, 927737. [Google Scholar] [CrossRef]
- Groen, J.V.; Smits, F.J.; Koole, D.; Besselink, M.G.; Busch, O.R.; Dulk, M.D.; van Eijck, C.H.J.; Koerkamp, B.G.; van der Harst, E.; de Hingh, I.H.; et al. Completion pancreatectomy or a pancreas-preserving procedure during relaparotomy for pancreatic fistula after pancreatoduodenectomy: A multicentre cohort study and meta-analysis. Br. J. Surg. 2021, 108, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Paye, F.; Lupinacci, R.M.; Kraemer, A.; Lescot, T.; Chafaï, N.; Tiret, E.; Balladur, P. Surgical treatment of severe pancreatic fistula after pancreaticoduodenectomy by wirsungostomy and repeat pancreatico-jejunal anastomosis. Am. J. Surg. 2013, 206, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Ribero, D.; Amisano, M.; Zimmitti, G.; Giraldi, F.; Ferrero, A.; Capussotti, L. External Tube Pancreatostomy Reduces the Risk of Mortality Associated with Completion Pancreatectomy for Symptomatic Fistulas Complicating Pancreaticoduodenectomy. J. Gastrointest. Surg. 2013, 17, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Dai, X.; Bu, X.; Gao, F.; Zhang, X. Pancreaticojejunal Bridge-Anastomosis: A Novel Option for Surgeon to Preserve Pancreatic Body and Tail in Urgent Reoperation for Intra-abdominal Massive Hemorrhage after Pancreaticoduodenectomy. World J. Surg. 2010, 34, 2457–2462. [Google Scholar] [CrossRef]
- Kent, T.S.; Callery, M.P.; Vollmer, C.M., Jr. The bridge stent technique for salvage of pancreaticojejunal anastomotic dehiscence. HPB 2010, 12, 577–582. [Google Scholar] [CrossRef]
- van Santvoort, H.C.; Besselink, M.G.; Bakker, O.J.; Hofker, H.S.; Boermeester, M.A.; Dejong, C.H.; van Goor, H.; Schaapherder, A.F.; van Eijck, C.H.; Bollen, T.L.; et al. A Step-up Approach or Open Necrosectomy for Necrotizing Pancreatitis. N. Engl. J. Med. 2010, 362, 1491–1502. [Google Scholar] [CrossRef]
- Morató, O.; Poves, I.; Ilzarbe, L.; Radosevic, A.; Vázquez-Sánchez, A.; Sánchez-Parrilla, J.; Burdio, F.; Grande, L. Minimally invasive surgery in the era of step-up approach for treatment of severe acute pancreatitis. Int. J. Surg. 2018, 51, 164–169. [Google Scholar] [CrossRef]
- Stoop, T.F.; Fröberg, K.; Sparrelid, E.; Del Chiaro, M.; Ghorbani, P. Surgical management of severe pancreatic fistula after pancreatoduodenectomy: A comparison of early versus late rescue pancreatectomy. Langenbeck’s Arch. Surg. 2022, 407, 3467–3478. [Google Scholar] [CrossRef]
- Yang, J.; Chen, Y.; Liu, X.; Zheng, Z.; Wang, X.; Li, Y.; Tan, C. Beyond successful hemostasis: CT findings and organ failure predict postoperative death in patients suffering from post-pancreatoduodenectomy hemorrhage. HPB 2022. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Possible Causes of Grade C Postoperative Pancreatic Fistula | Preventive Measures | |
|---|---|---|
| Intestinal juice spillover | Reconstruction methods | |
| Anastomotic techniques | ||
| Stent or no-stent | ||
| Bacterial translocation | Mucosal barrier breakdown | Avoid mechanical bowel preparation |
| Oral enteral nutrition | ||
| Edema of intestinal wall | Goal-directed fluid therapy | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, C.; Chen, Y.; Liu, X.; Zheng, Z.; Zhang, H.; Tan, C. Prevention and Treatment of Grade C Postoperative Pancreatic Fistula. J. Clin. Med. 2022, 11, 7516. https://doi.org/10.3390/jcm11247516
Xiang C, Chen Y, Liu X, Zheng Z, Zhang H, Tan C. Prevention and Treatment of Grade C Postoperative Pancreatic Fistula. Journal of Clinical Medicine. 2022; 11(24):7516. https://doi.org/10.3390/jcm11247516
Chicago/Turabian StyleXiang, Chengzhi, Yonghua Chen, Xubao Liu, Zhenjiang Zheng, Haoqi Zhang, and Chunlu Tan. 2022. "Prevention and Treatment of Grade C Postoperative Pancreatic Fistula" Journal of Clinical Medicine 11, no. 24: 7516. https://doi.org/10.3390/jcm11247516
APA StyleXiang, C., Chen, Y., Liu, X., Zheng, Z., Zhang, H., & Tan, C. (2022). Prevention and Treatment of Grade C Postoperative Pancreatic Fistula. Journal of Clinical Medicine, 11(24), 7516. https://doi.org/10.3390/jcm11247516