
An Orthotopic Resection Surgical Technique Using an Inferior Infracolic Approach for Laparoscopic Pancreaticoduodenectomy

Abstract
1. Introduction
2. Patients and Methods
Patients
3. Surgical Procedures
3.1. Patient Position and Trocar Distribution
3.2. Orthotopic Resection Surgical Technique
3.2.1. Exploration and Initial Processing
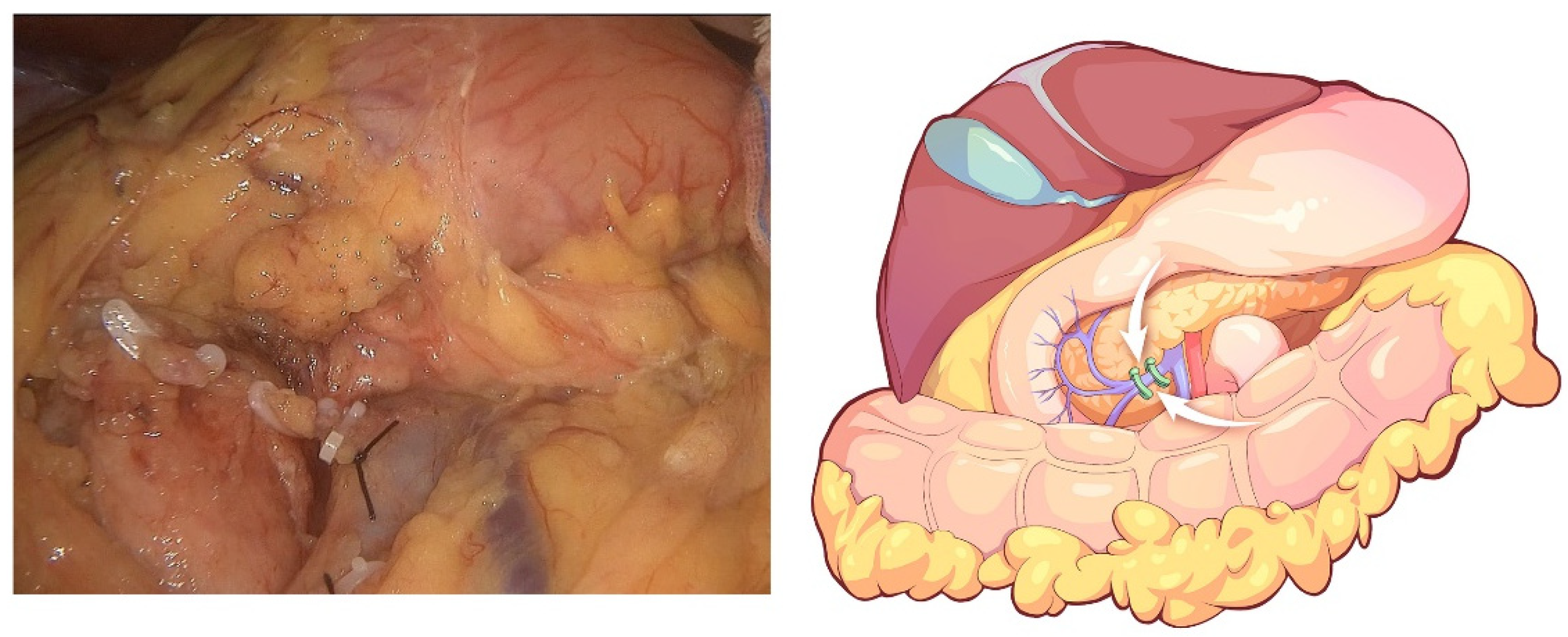
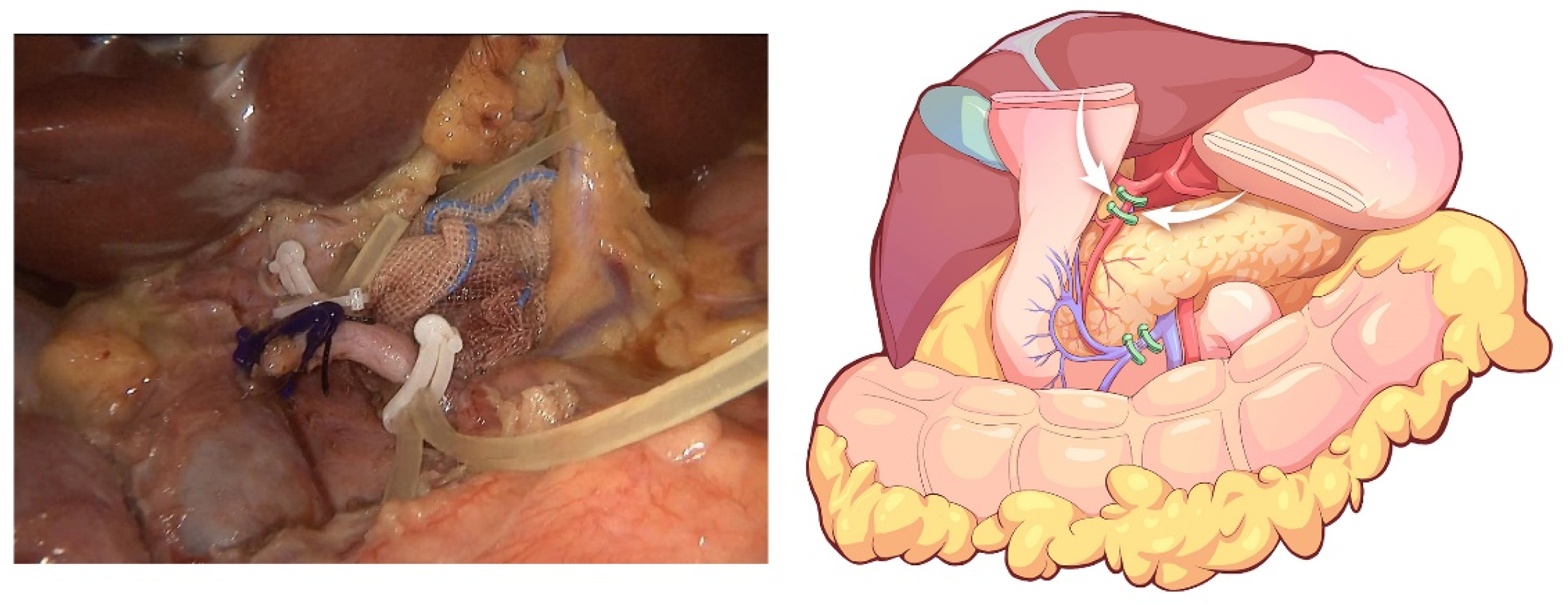
3.2.2. Procedures of the Inferior Infracolic Approach
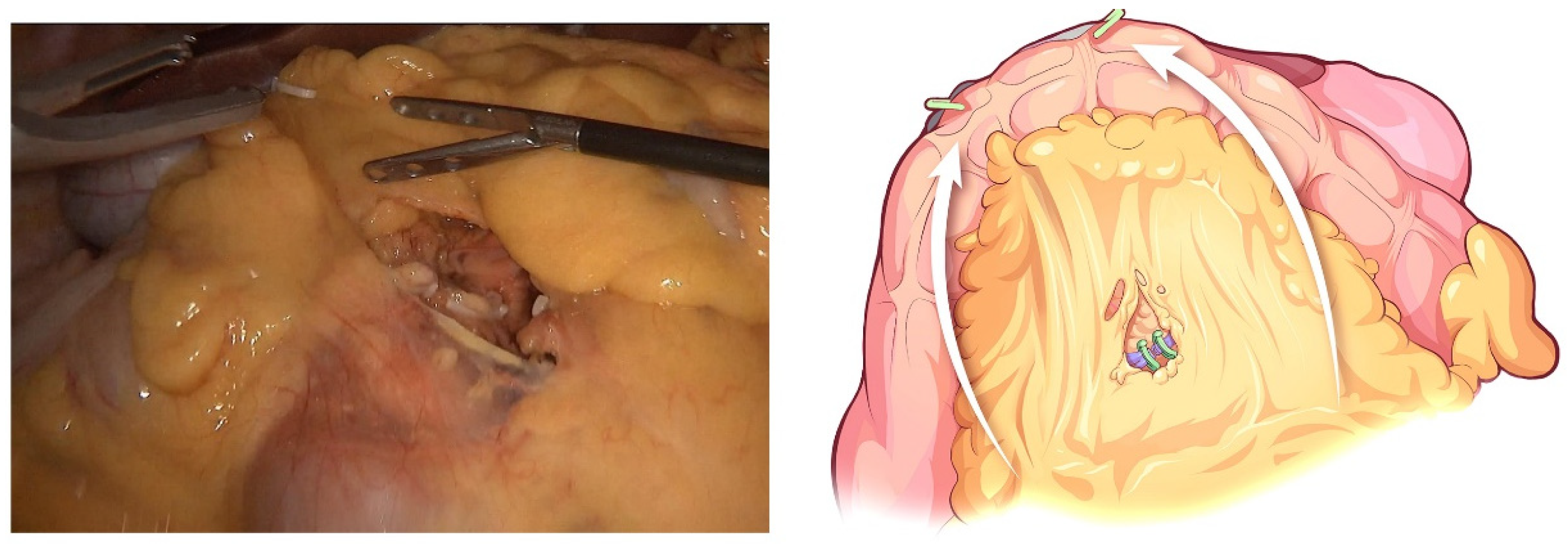
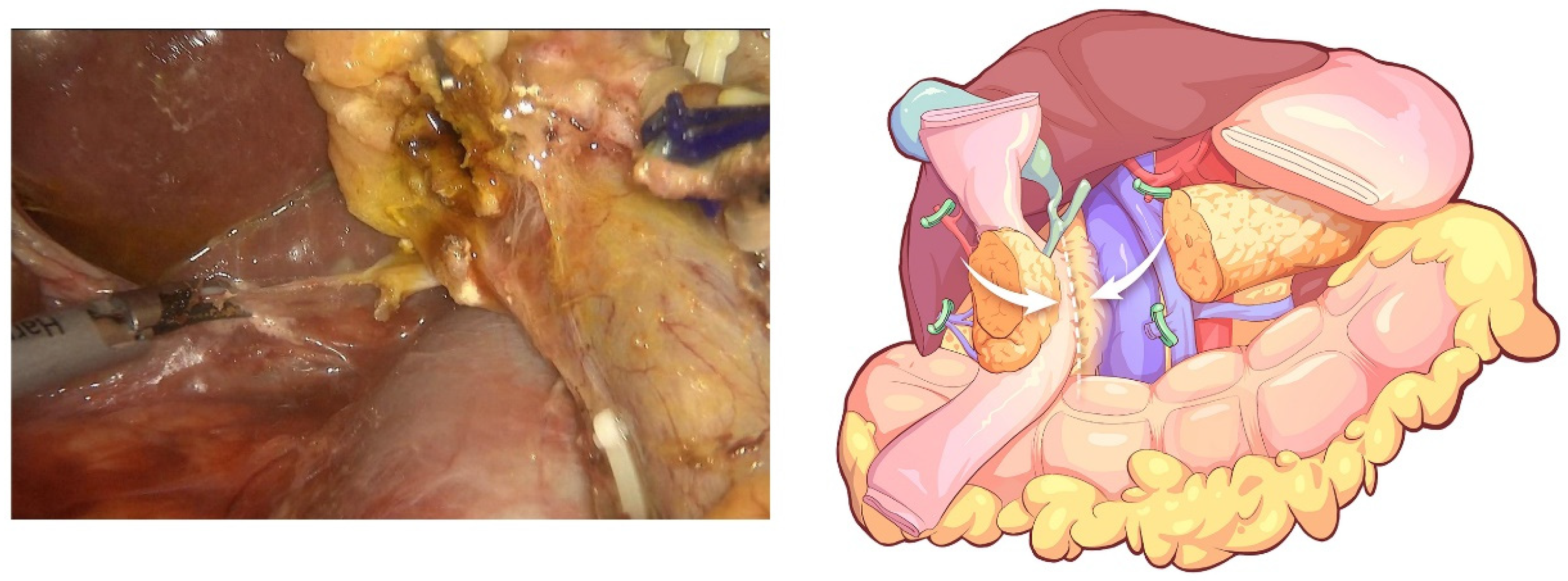
3.2.3. Reversed Kocher’s Maneuver and Lymphadenectomy
3.2.4. Reconstruction of Digestive Tract
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuroki, T.; Eguchi, S. No-touch isolation techniques for pancreatic cancer. Surg. Today 2017, 47, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Lyadov, V.K.; Milovanov, V.V. No-touch pancreatectomy and radical antegrade modular pancreatosplenectomy: A systematic review. Khirurgiia 2016, 12, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Lee, K.W.; Kim, H.C.; Yi, N.J.; Suh, K.S. No touch isolation technique for the prevention of postoperative recurrence of hepatocellular carcinoma after liver transplantation-combined with trans-arterial radioembolization. Surg. Oncol. 2020, 35, 189–190. [Google Scholar] [CrossRef] [PubMed]
- Hirota, M.; Hashimoto, D.; Ishiko, T.; Satoh, N.; Takamori, H.; Chikamoto, A.; Tanaka, H.; Sugita, H.; Sand, J.; Nordback, I.; et al. Distal pancreatectomy using a no-touch isolation technique. Scand. J. Surg. 2012, 101, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Fujita, J.; Uyama, I.; Sugioka, A.; Komori, Y.; Matsui, H.; Hasumi, A. Laparoscopic right hemicolectomy with radical lymph node dissection using the no-touch isolation technique for advanced colon cancer. Surg. Today 2001, 31, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Gall, T.M.; Jacob, J.; Frampton, A.E.; Krell, J.; Kyriakides, C.; Castellano, L.; Stebbing, J.; Jiao, L.R. Reduced dissemination of circulating tumor cells with no-touch isolation surgical technique in patients with pancreatic cancer. JAMA Surg. 2014, 149, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Ironside, N.; Barreto, S.G.; Loveday, B.; Shrikhande, S.V.; Windsor, J.A.; Pandanaboyana, S. Meta-analysis of an artery-first approach versus standard pancreatoduodenectomy on perioperative outcomes and survival. Br. J. Surg. 2018, 105, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Hilal, M.A.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years after. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, R.B., Jr.; Kyle, K.; Watson, F.R.; Spratt, J. Cancer of the colon: The influence of the no-touch isolation technic on survival rates. CA Cancer J. Clin. 1968, 18, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Wiggers, T.; Jeekel, J.; Arends, J.W.; Brinkhorst, A.P.; Kluck, H.M.; Luyk, C.I.; Munting, J.D.K.; Povel, J.A.C.M.; Rutten, A.P.M.; Volovics, A.; et al. No-touch isolation technique in colon cancer: A controlled prospective trial. Br. J. Surg. 1988, 75, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Han, D.; Li, X.; Pan, F.; Ma, J.; Kou, J.; Fan, H.; Lang, R.; He, Q. Inferior Infracolic ‘Superior Mesenteric Artery First’ Approach with a No-Touch Isolation Surgical Technique in Patients with a Borderline Resectable Cancer of the Pancreatic Head. Ann. Surg. Oncol. 2016, 23 (Suppl. 5), 976–980. [Google Scholar] [CrossRef] [PubMed]
- Hirota, M.; Shimada, S.; Yamamoto, K.; Tanaka, E.; Sugita, H.; Egami, H.; Ogawa, M. Pancreatectomy using the no-touch isolation technique followed by extensive intraoperative peritoneal lavage to prevent cancer cell dissemination: A pilot study. JOP 2005, 6, 143–151. [Google Scholar] [PubMed]
- Hirota, M.; Ogawa, M. No-touch pancreatectomy for invasive ductal carcinoma of the pancreas. JOP 2014, 15, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Wu, X.; Chen, G.; Liu, Y.; Zhu, C.; Huang, F.; Tan, Z.; Zhong, X. Laparoscopic Pancreatoduodenectomy for Pancreatic Cancer using In-Situ No-Touch Isolation Technique. J. Vis. Exp. 2022, 2, e63450. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z.J.; Zhong, X.S.; Shen, Z.T.; Huang, Y.X.; Chen, Y.C.; Qiu, C.J.; Chen, G.H.; Liu, Y.F.; Liu, Z.Y.Z.; Zhang, S.; et al. Clinical experience of laparoscopic pancreatoduodenectomy via orthotopic resection. Zhonghua Wai Ke Za Zhi 2020, 58, 782–786. [Google Scholar] [CrossRef]
- Kopchak, K.V.; Duvalko, A.V.; Pererva, L.A.; Davidenko, N.G.; Kvasivka, A.A.; Sukhachev, S.V. First experience of laparoscopic no-touch pancreatoduodenectomy. Klin. Khirurhiia 2013, 9, 73–74. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Cases | 41 |
| Age (median (interquartile range)) (y) | 56 (23–83) |
| Sex (male/female) | 20/21 |
| BMI (median (interquartile range)) (kg/m2) | 23.4 (16.6–28.6) |
| American Society of Anesthesiology | |
| II | 36 |
| III | 5 |
| Preoperative biliary drainage | 2 |
| Pathologic diagnosis | |
| Ampullary adenocarcinoma | 6 |
| Pancreatic ductal adenocarcinoma | 25 |
| Pancreatic neuroendocrine tumor | 4 |
| Distal cholangiocarcinoma | 3 |
| Solid pseudopapillary tumor | 2 |
| Other | 1 |
| Variables | |
|---|---|
| Conversion to open surgery (n, %) | 2(4.9) |
| Reoperation (n, %) | 1 (2.4) |
| Operative time (min) * | 335 (300–1055) |
| Estimated blood loss (mL) * | 300 (50–1250) |
| Combined with portal vein resection and reconstruction (n, %) | 2 (4.9) |
| Transfusion (n, %) | 6 (14.6) |
| Postoperative hospital stay (d) * | 12 (3–125) |
| Time to first passage of flatus (d) * | 3 (1–5) |
| Time to first out-of-bed (d) * | 3 (2–7) |
| Perioperative mortality (%) | 0 (0) |
| Complications (n, %) | |
| Clavien–Dindo classification (n, %) | |
| Grade I | 0(0) |
| Grade II | 3(7.3) |
| Grade IIIa | 3(7.3) |
| Grade IIIb | 1(2.4) |
| Grade IVa | 0(0) |
| Grade IVb | 0(0) |
| Grade V | 0(0) |
| Postoperative bleeding | |
| Grade A | 0(0) |
| Grade B | 1(2.4) |
| Grade C | 1(2.4) |
| Pancreatic fistula | |
| Biochemical leakage | 13(31.7) |
| Grade B | 2 (4.9) |
| Grade C | 0 (0) |
| Bile leakage | 1 (2.4) |
| Abdominal fluid collection | 3 (7.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, Y.; Xiong, J.; Wang, Z.; Wang, X.; Liu, X.; Ke, N. An Orthotopic Resection Surgical Technique Using an Inferior Infracolic Approach for Laparoscopic Pancreaticoduodenectomy. J. Clin. Med. 2023, 12, 590. https://doi.org/10.3390/jcm12020590
Yao Y, Xiong J, Wang Z, Wang X, Liu X, Ke N. An Orthotopic Resection Surgical Technique Using an Inferior Infracolic Approach for Laparoscopic Pancreaticoduodenectomy. Journal of Clinical Medicine. 2023; 12(2):590. https://doi.org/10.3390/jcm12020590
Chicago/Turabian StyleYao, Yutong, Junjie Xiong, Ziyao Wang, Xing Wang, Xubao Liu, and Nengwen Ke. 2023. "An Orthotopic Resection Surgical Technique Using an Inferior Infracolic Approach for Laparoscopic Pancreaticoduodenectomy" Journal of Clinical Medicine 12, no. 2: 590. https://doi.org/10.3390/jcm12020590
APA StyleYao, Y., Xiong, J., Wang, Z., Wang, X., Liu, X., & Ke, N. (2023). An Orthotopic Resection Surgical Technique Using an Inferior Infracolic Approach for Laparoscopic Pancreaticoduodenectomy. Journal of Clinical Medicine, 12(2), 590. https://doi.org/10.3390/jcm12020590