
Risk of Contrast-Associated Acute Kidney Injury in Patients Undergoing Peripheral Angiography with Carbon Dioxide Compared to Iodine-Containing Contrast Agents: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
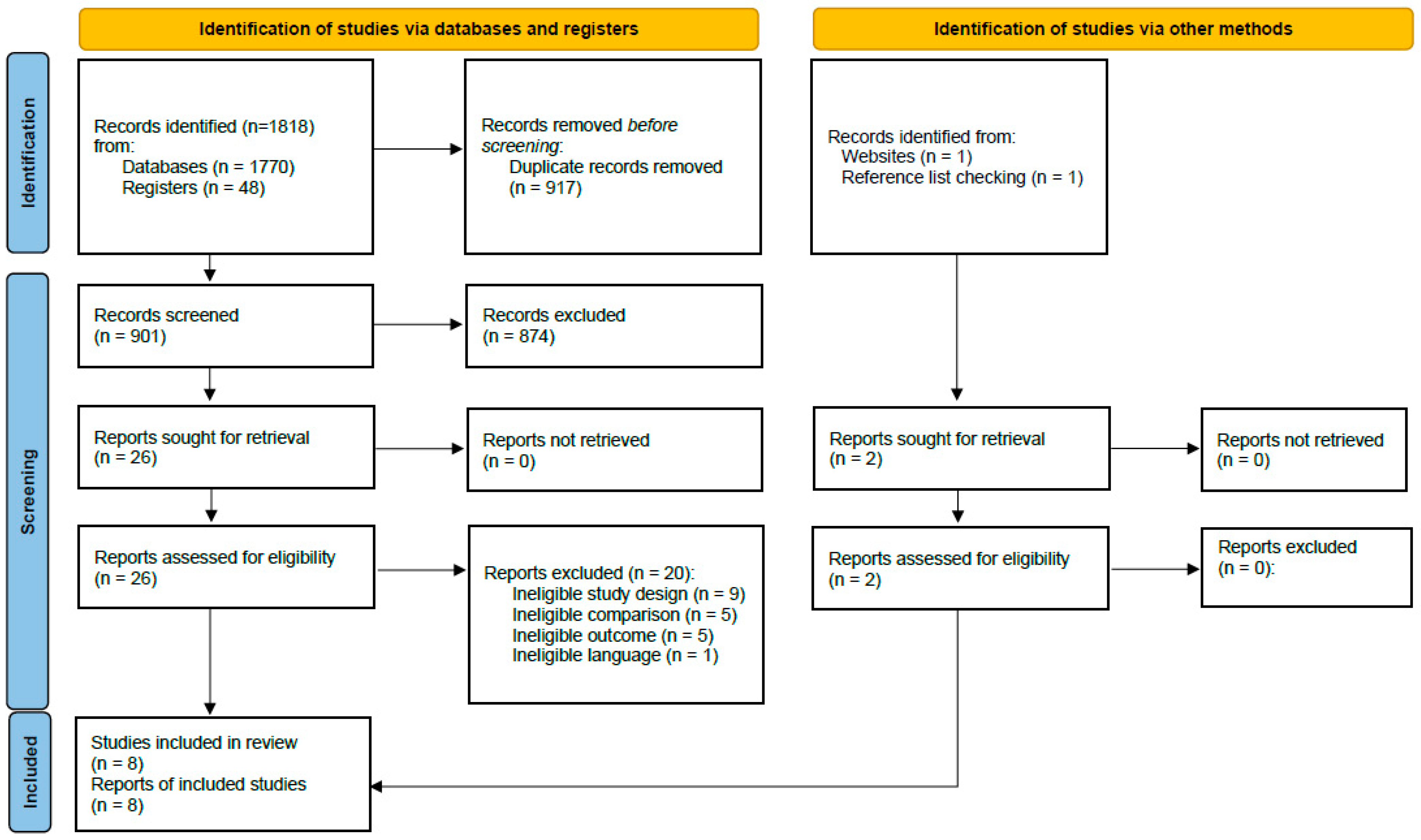
2.1. Literature Search
2.2. Eligibility Criteria and Study Selection
2.3. Risk of Bias and Certainty of Evidence
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Study Characteristics
3.2. Study Population
3.3. Risk of Bias and Certainty of Evidence
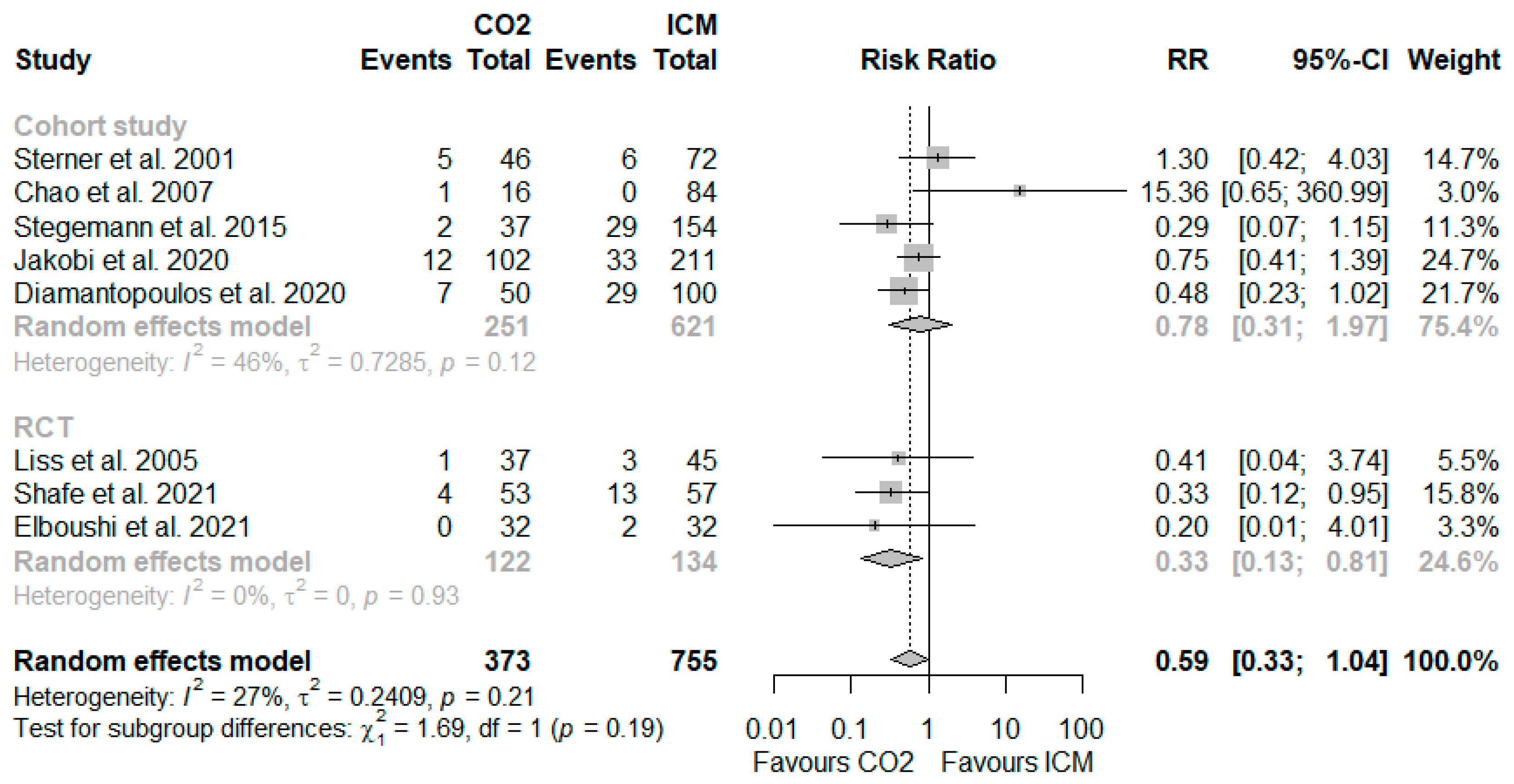
3.4. Risk of CA-AKI
3.5. Procedural Variables and Outcomes
3.6. Additional Adverse Events and CO2-Related Side Effects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Included | Excluded | |
|---|---|---|
| Populations | Adult patients undergoing angiography of the lower limb arteries, kidney arteries or infrarenal aorta with or without endovascular intervention | Children Angiography of other arteries (e.g., coronary angiography) Patients who required haemodialysis prior to the intervention |
| Intervention | Application of CO2 with or without supplemental use of a small amount of iodinated contrast medium | Any other intervention |
| Comparator | Application of conventional iodinated contrast medium only | Application of CO2 Any other comparator |
| Outcomes | Primary outcome: Risk of contrast-associated acute kidney injury as defined by study authors Secondary outcomes: Need for haemodialysis after the intervention Additional adverse events (e.g., vascular complications) CO2-related side effects (e.g., nausea, vomiting, limb pain) Procedural outcomes (e.g., technical success) | Post-procedural increase in creatinine/decrease in GFR without distinct definition or classification of contrast-associated acute kidney injury Other surrogate outcomes |
| Study designs | RCT Non-randomised controlled trials Controlled cohort studies | Cohort studies without control group Narrative and systematic reviews Case reports and case series |
| Publication type | Full publication | Abstracts only Letters and editorials |
| Publication language | English, German | All other languages |
| Author, Year, Country | Pre-Intervention, GFR, Serum Creatinine (Mean ± SD or Median [IQR]) | Procedure Time (Mean ± SD or Median [IQR]) | Fluoroscopy Time, Radiation Dose-Area Product (Mean ± SD or Median [IQR]) | Definition of Contrast-Induced Nephropathy | Additional Adverse Events, CO2-Related Side Effects and Procedural Outcome n/N (%) a | |
|---|---|---|---|---|---|---|
| Elboushi et al. 2021 [29] Saudi Arabia and Egypt | GFR, mL/min: CO2: NR ICM: NR Creatinine, mg/dL: CO2: 0.92 ± 0.16 ICM: 0.94 ± 0.2 | Procedure time, minutes: CO2: 87 ± 22 ICM: 77 ± 28 | Fluoroscopy time: NR Radiation dose-area product: NR | Increase in serum creatinine exceeding 25% or more than or equal to 0.5 mg/dL within 1 month. b | Technical success rate: CO2: 32/32 (100%) ICM: 32/32 (100%) No cardiac death, myocardial infarction, stroke and/or death within 3 months | Groin hematoma: CO2: 2/31c (6.5%) ICM: 2/32 (6.3%) Pseudoaneurysm: CO2: 1/31 c (3.2%) ICM: 0/32 Major amputation: CO2: 2/31 c (6.5%) ICM: 3/32 (9.4%) |
| Shafe et al. 2021 [31] Iran | GFR, mL/min: CO2: 60.9 ± 22.0 ICM: 74.7 ± 23.6 Creatinine, mg/dL: CO2: 1.46 ± 0.45 ICM: 1.13 ± 0.28 | Procedure time: NR | Fluoroscopy time: NR Radiation dose-area product: NR | Increase in serum creatinine exceeding 25% or 0.5 mg/dL within 72 h after the procedure | Technical success rate: CO2: 53/53 (100%) ICM: 57/57 (100%) Lower-limb pain: CO2: 12/53 (22.6%) ICM: 0/57 | Major vascular complications: CO2: 0/53 ICM: 0/57 Death: CO2: 0/53 ICM: 0/57 |
| Liss et al. 2005 [30] Sweden | GFR, mL/min: CO2: 54 ± 22 ICM: 59 ± 29 Creatinine, mg/dL: d CO2: 1.45 ± 0.43 ICM: 1.36 ± 0.42 | Procedure time: NR | Fluoroscopy time: NR Radiation dose-area product: NR | Increase in serum creatinine by >25% within one week after the procedure | Vomiting: CO2: 1/37 (27.0%) ICM: 0/45 | Nausea: CO2: 8/37 (21.6%) ICM: 1/45 (2.2%) |
| Sterner et al. 2001 [36] Sweden | GFR, mL/min: CO2: NR ICM: NR Creatinine, mg/dL e,f CO2: 2.57 [NR]; 3.71 [NR] ICM: 1.98 [NR] | Procedure time: NR | Fluoroscopy time: NR Radiation dose-area product: NR | Increase in serum creatinine by >25% within two weeks after the procedure | NR | |
| Chao et al. 2007 [32] USA | GFR, mL/min: CO2: 36 ± NR ICM: 81 ± NR Creatinine, mg/dL: CO2: 1.8 ± NR g ICM: 1.0 ± NR | Procedure time, hours: CO2: 3.0 ± 0.3 ICM: 2.3 ± 0.2 | Fluoroscopy time, minutes: CO2: 46 ± 7 ICM: 24 ± 1.5 Radiation dose-area product, cGy.cm2: CO2: 92,500 ± 13,800 ICM: 52,900 ± 4400 | Increase in serum creatinine by >20% within 24 h after the procedure | Morbidity: CO2: 2/16 (12%) ICM: 5/84 (6%) | Death: CO2: 0/16 ICM: 0/84 |
| Stegemann et al. 2015 [35] Germany | GFR, mL/min: CO2: 22 ± 34 ICM: 76 ± 28 Creatinine, mg/dL: CO2: 2.1 ± 1.3 ICM: 1.1 ± 0.6 | Procedure time, minutes: CO2: 83 + 32 ICM: 79 + 37 | Fluoroscopy time, minutes: CO2: 22 + 14 ICM: 23 + 17 Radiation dose-area product, cGy.cm2: CO2: 8054 + 12,764 ICM: 9359 + 11,474 | Increase in serum creatinine by >25% or >0.5 mg/dL within 48 h after the procedure | Technical success rate: CO2: 37/37 (100%) ICM: 148/154 (96%) | Nausea: CO2: 1/37 (2.7%) ICM: 0/154 Several patients described temporary acute ischaemic lower leg pain following both ICM and CO2 injection. |
| Diamantopoulus et al. 2020 [33] England | GFR, mL/min: CO2: 38.6 ± 13.2 ICM: 43.3 ± 12.2 Creatinine, mg/dL:f CO2: 1.7 ± 0.55 ICM: 1.54 ± 0.52 | Procedure time: NR | Fluoroscopy time: NR Radiation dose-area product: NR | Increase in serum creatinine by >25% or >0.5 mg/dL within 72 h after the procedure | There were no major complications associated with the use of CO2. Most of the CLI cases reported transient discomfort (seconds) at the level of the symptomatic foot. | Major complications: CO2: 0/50 ICM: NR |
| Jakobi et al. 2021 [34] Germany | GFR, mL/min: CO2: 32.4 ± 11.8 ICM: 33.1 ± 15.6 Creatinine, mg/dL: CO2: NR ICM: NR | Procedure time, minutes: CO2: 92.3 ± 35 ICM: 101.8 ± 47.2 | Fluoroscopy time: NR Radiation dose-area product, cGy.cm2: CO2: 6025 ± 6926 ICM: 4281 ± 4722 | Increase in serum creatinine by a factor of 1.5 to 1.9 or ≥0.3 mg/dL within 48 h after the procedure | Technical success rate: CO2: 99/102 (97%) ICM: 201/211 (95.3%) | Severe procedure-related complications: CO2: 0/102 ICM: 0/211 Transient leg pain: CO2: 15/102 (14.7%) ICM: 0/211 |
References
- Malyar, N.; Furstenberg, T.; Wellmann, J.; Meyborg, M.; Luders, F.; Gebauer, K.; Bunzemeier, H.; Roeder, N.; Reinecke, H. Recent trends in morbidity and in-hospital outcomes of in-patients with peripheral arterial disease: A nationwide population-based analysis. Eur. Heart J. 2013, 34, 2706–2714. [Google Scholar] [CrossRef] [PubMed]
- Latus, J.; Schwenger, V.; Schlieper, G.; Reinecke, H.; Hoyer, J.; Persson, P.B.; Remppis, B.A.; Mahfoud, F. Contrast medium-induced acute kidney injury-Consensus paper of the working group “Heart and Kidney” of the German Cardiac Society and the German Society of Nephrology. Internist 2021, 62, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R.; Zhuo, H.; Zhang, Y.; Dahl, N.; Dardik, A.; Ochoa Chaar, C.I. Risk factors and safe contrast volume thresholds for postcontrast acute kidney injury after peripheral vascular interventions. J. Vasc. Surg. 2020, 72, 603–610.e601. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.; Hughston, H.; Michalek, J.; Trevino, A.; Gupta, K.; Martinez, J.P.; Hoang, D.T.; Wu, P.B.; Banerjee, S.; Masoomi, R. Acute kidney injury in patients undergoing endovascular therapy for critical limb ischemia. Catheter. Cardiovasc. Interv. 2019, 94, 636–641. [Google Scholar] [CrossRef]
- Mehran, R.; Dangas, G.D.; Weisbord, S.D. Contrast-Associated Acute Kidney Injury. N. Engl. J. Med. 2019, 380, 2146–2155. [Google Scholar] [CrossRef]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-term risk of mortality and other adverse outcomes after acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 53, 961–973. [Google Scholar] [CrossRef]
- See, E.J.; Jayasinghe, K.; Glassford, N.; Bailey, M.; Johnson, D.W.; Polkinghorne, K.R.; Toussaint, N.D.; Bellomo, R. Long-term risk of adverse outcomes after acute kidney injury: A systematic review and meta-analysis of cohort studies using consensus definitions of exposure. Kidney Int. 2019, 95, 160–172. [Google Scholar] [CrossRef]
- Katsogridakis, E.; Lea, T.; Yap, T.; Batchelder, A.; Saha, P.; Diamantopoulos, A.; Saratzis, N.; Davies, R.; Zayed, H.; Bown, M.J.; et al. Acute kidney injury following endovascular intervention for peripheral artery disease. Br. J. Surg. 2021, 108, 152–159. [Google Scholar] [CrossRef]
- Prasad, A.; Ortiz-Lopez, C.; Khan, A.; Levin, D.; Kaye, D.M. Acute kidney injury following peripheral angiography and endovascular therapy: A systematic review of the literature. Catheter. Cardiovasc. Interv. 2016, 88, 264–273. [Google Scholar] [CrossRef]
- Safley, D.M.; Salisbury, A.C.; Tsai, T.T.; Secemsky, E.A.; Kennedy, K.F.; Rogers, R.K.; Latif, F.; Shammas, N.W.; Garcia, L.; Cavender, M.A.; et al. Acute Kidney Injury Following In-Patient Lower Extremity Vascular Intervention: From the National Cardiovascular Data Registry. JACC Cardiovasc. Interv. 2021, 14, 333–341. [Google Scholar] [CrossRef]
- Tsai, T.T.; Patel, U.D.; Chang, T.I.; Kennedy, K.F.; Masoudi, F.A.; Matheny, M.E.; Kosiborod, M.; Amin, A.P.; Messenger, J.C.; Rumsfeld, J.S.; et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: Insights from the NCDR Cath-PCI registry. JACC Cardiovasc. Interv. 2014, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fähling, M.; Seeliger, E.; Patzak, A.; Persson, P.B. Understanding and preventing contrast-induced acute kidney injury. Nat. Rev. Nephrol. 2017, 13, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Nijssen, E.C.; Rennenberg, R.J.; Nelemans, P.J.; Essers, B.A.; Janssen, M.M.; Vermeeren, M.A.; Ommen, V.V.; Wildberger, J.E. Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING): A prospective, randomised, phase 3, controlled, open-label, non-inferiority trial. Lancet 2017, 389, 1312–1322. [Google Scholar] [CrossRef]
- Weisbord, S.D.; Gallagher, M.; Jneid, H.; Garcia, S.; Cass, A.; Thwin, S.S.; Conner, T.A.; Chertow, G.M.; Bhatt, D.L.; Shunk, K.; et al. Outcomes after Angiography with Sodium Bicarbonate and Acetylcysteine. N. Engl. J. Med. 2018, 378, 603–614. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.S.; McDonald, R.J.; Comin, J.; Williamson, E.E.; Katzberg, R.W.; Murad, M.H.; Kallmes, D.F. Frequency of acute kidney injury following intravenous contrast medium administration: A systematic review and meta-analysis. Radiology 2013, 267, 119–128. [Google Scholar] [CrossRef]
- Wilhelm-Leen, E.; Montez-Rath, M.E.; Chertow, G. Estimating the Risk of Radiocontrast-Associated Nephropathy. J. Am. Soc. Nephrol. 2017, 28, 653–659. [Google Scholar] [CrossRef]
- Sharafuddin, M.J.; Marjan, A.E. Current status of carbon dioxide angiography. J. Vasc. Surg. 2017, 66, 618–637. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Veritas Health Innovation. Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2021; Available online: www.covidence.org (accessed on 20 October 2020).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- McMaster University and Evidence Prime. GRADEpro GDT: GRADEpro Guideline Development Tool; McMaster University and Evidence Prime: Hamilton, ON, CAN, 2022; Available online: gradepro.org (accessed on 20 October 2020).
- Paule, R.C.; Mandel, J. Consensus Values and Weighting Factors. J. Res. Natl. Bur. Stand. 1982, 87, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- RStudio Team. RStudio: Integrated Development Environment for R; RStudio, PBC: Boston, MA, USA, 2021. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Elboushi, A.; Tawfik, A.; Abouissa, A.; Harraz, M.; El-Laboudy, M. Carbon dioxide versus iodine contrast medium for endovascular revascularization of aortoiliac occlusive disease: A two-center randomized controlled trial. Egypt. J. Surg. 2021, 40, 264–271. [Google Scholar] [CrossRef]
- Liss, P.; Eklöf, H.; Hellberg, O.; Hägg, A.; Boström-Ardin, A.; Löfberg, A.M.; Olsson, U.; Orndahl, P.; Nilsson, H.; Hansell, P.; et al. Renal effects of CO2 and iodinated contrast media in patients undergoing renovascular intervention: A prospective, randomized study. J. Vasc. Interv. Radiol. 2005, 16, 57–65. [Google Scholar] [CrossRef]
- Shafe, O.; Samiee, E.; Moosavi, J.; Mohebbi, B.; Fakhrabadi, A.; Bakhshandeh, H.; Naghavi, B.; Tahivili, R.; Cheraghi, S.; Sadeghipour, P. Comparison Between Intra-Arterial Carbon Dioxide and Iodinated Contrast Agent Injections in Patients with Lower-Limb Peripheral Arterial Diseases and Mild-to-Moderate Renal Dysfunction: A Randomized Controlled Trial. J. Crit. Limb. Ischem. 2021, 1, E104–E109. [Google Scholar]
- Chao, A.; Major, K.; Kumar, S.R.; Patel, K.; Trujillo, I.; Hood, D.B.; Rowe, V.L.; Weaver, F.A. Carbon dioxide digital subtraction angiography-assisted endovascular aortic aneurys.sm.m repair in the azotemic patient. J. Vasc. Surg. 2007, 45, 451–458; discussion 458–460. [Google Scholar] [CrossRef]
- Diamantopoulos, A.; Patrone, L.; Santonocito, S.; Theodoulou, I.; Ilyas, S.; Dourado, R.; Game, D.; Karunanithy, N.; Patel, S.; Zayed, H.; et al. Carbon dioxide angiography during peripheral angioplasty procedures significantly reduces the risk of contrast-induced nephropathy in patients with chronic kidney disease. CVIR Endovasc. 2020, 3, 9. [Google Scholar] [CrossRef]
- Jakobi, T.; Meyborg, M.; Freisinger, E.; Gebauer, K.; Stella, J.; Engelbertz, C.; Reinecke, H.; Malyar, N.M. Feasibility and impact of carbon dioxide angiography on acute kidney injury following endovascular interventions in patients with peripheral artery disease and renal impairment. J. Nephrol. 2021, 8, 8. [Google Scholar] [CrossRef]
- Stegemann, E.; Tegtmeier, C.; Bimpong-Buta, N.Y.; Sansone, R.; Uhlenbruch, M.; Richter, A.; Stegemann, B.; Roden, M.; Westenfeld, R.; Kelm, M.; et al. Carbondioxide-Aided Angiography Decreases Contrast Volume and Preserves Kidney Function in Peripheral Vascular Interventions. Angiology 2016, 67, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Sterner, G.; Nyman, U.; Valdes, T. Low risk of contrast-medium-induced nephropathy with modern angiographic technique. J. Intern. Med. 2001, 250, 429–434. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ghumman, S.S.; Weinerman, J.; Khan, A.; Cheema, M.S.; Garcia, M.; Levin, D.; Suri, R.; Prasad, A. Contrast induced-acute kidney injury following peripheral angiography with carbon dioxide versus iodinated contrast media: A meta-analysis and systematic review of current literature. Catheter. Cardiovasc. Interv. 2017, 90, 437–448. [Google Scholar] [CrossRef]
- Weisbord, S.D.; Palevsky, P.M.; Kaufman, J.S.; Wu, H.; Androsenko, M.; Ferguson, R.E.; Parikh, C.R.; Bhatt, D.L.; Gallagher, M. Contrast-Associated Acute Kidney Injury and Serious Adverse Outcomes Following Angiography. J. Am. Coll. Cardiol. 2020, 75, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Dosekun, A.K.; Kumar, V. Carbon dioxide-angiography for patients with peripheral arterial disease at risk of contrast-induced nephropathy. World J. Cardiol. 2020, 12, 76–90. [Google Scholar] [CrossRef] [PubMed]


| Author, Year, Country | Study Design Risk of Bias Follow-Up | N | Age, Years, Mean (SD) | Women | Diabetes Mellitus | CKD Stage 3–5 | Condition/Site and Intervention | CO2 and ICM Amount, ICM Type, (Mean ± SD or Median [IQR]) | CA-AKI, Haemodialysis n/N (%) a |
|---|---|---|---|---|---|---|---|---|---|
| Elboushi et al. 2021 [29] Saudi Arabia and Egypt | RCT Low 3 months b | Total: 64 CO2: 32 ICM: 32 | Age: CO2: 54.3 ± 9.8 ICM: 56.3 ± 9.7 | Women: CO2: 29.0% ICM: 53.1% | Diabetes mellitus: All: 45.3% CO2: 55.0% ICM: 37.5% | CKD stage 3–5: CO2: 0 ICM: 0 | PAD Angiography with aortoiliac endovascular intervention | CO2 amount, mL: CO2: 171 [NR] ICM: 0 ICM amount, mL: CO2: 10 [NR] (N = 3) ICM: 78 [NR] ICM type: Iohexol | CA-AKI: CO2: 0/32 ICM: 2/32 (6.3%) Haemodialysis: NR |
| Shafe et al. 2021 [31] Iran | RCT Some concerns 1 month | Total: 110 CO2: 53 ICM: 57 | Age: CO2: 62.5 ± 8.4 ICM: 63.3 ± 11.7 | Women: CO2: 24.5% ICM: 19.3% | Diabetes mellitus: All: 45% CO2: 51% ICM: 40% | CKD stage 3–5: CO2: NR ICM: NR | PAD Angiography without (29%) or with aortoiliac, femoropopliteal or infrapopliteal endovascular intervention (71%) | CO2 amount, mL: CO2: NR ICM: 0 ICM amount, mL: CO2: 11.4 ± 6.1 ICM: 93.2 ± 43.0 ICM type: NR | CA-AKI: CO2: 4/53 (7.5%) ICM: 13/57 (22.8%) Haemodialysis: CO2: 0/53 ICM: 0/57 |
| Liss et al. 2005 [30] Sweden | RCT Some concerns 3 weeks | Total: 82 CO2: 37 ICM: 45 | Age: CO2: 67 ± 8 ICM: 63 ± 11 | Women: CO2: NR ICM: NR | Diabetes mellitus: All: 17% CO2: 27% ICM: 9% | CKD stage 3–5: CO2: NR ICM: NR | Renal arteries Angiography with or without endovascular intervention | CO2 amount, mL: CO2: 191 ± 118 ICM: 0 ICM amount, mL: CO2: 35.1 ± 6.4 ICM: 88.4 ± 42.9 ICM type: Ioxaglate | CA-AKI: CO2: 1/37 (2.7%) ICM: 3/45 (6.7%) Haemodialysis: CO2: 0/37 ICM: 1/45 (2.2%) |
| Sterner et al. 2001 [36] Sweden | Cohort study Serious 2 weeks | Total: 118 CO2: 46 c ICM: 72 d | Age: CO2: 71 ± NR ICM: 72 ± NR | Women: CO2: 15% ICM: 33% | Diabetes mellitus: All: 21% CO2: 20% ICM: 22% | CKD stage 3–5: CO2: NR ICM: NR | PAD, Renal and mesenteric arteries d Angiography with or without endovascular intervention | CO2 amount, mL: CO2: NR ICM: 0 ICM amount, mL: CO2: 5 [NR] ICM: 22 [NR] ICM type: Iohexol | CA-AKI: CO2: 5/46 (10.9%) ICM: 6/72 (8.3%) Haemodialysis: NR |
| Chao et al. 2007 [32] USA | Cohort study Serious 6 months | Total: 100 CO2: 16 ICM: 84 | Age: CO2: 77 ± NR ICM: 76 ± NR | Women: CO2: 6% ICM: 18% | Diabetes mellitus: All: 13% CO2: 20% ICM: 12% | CKD stage 3–5: CO2: 88% ICM: 34% | Abdominal aortic aneurysm EVAR | CO2 amount, mL: CO2: 50 ± NR ICM: 0 ICM amount, mL: CO2: 27 ± 5 ICM: 148 ± 20 ICM type: Iopamidol | CA-AKI: CO2: 1/16 (6.3%) ICM: 0/84 Haemodialysis: CO2: 0/16 ICM: 0/84 |
| Stegemann et al. 2015 [35] Germany | Cohort study Serious NR | Total: 191 CO2: 37 ICM: 154 | Age: CO2: 70 ± 10 ICM: 73 ± 12 | Women: CO2: 38% ICM: 23% | Diabetes mellitus: All: 51% CO2: 51% ICM: 51% | CKD stage 3–5: CO2: 86% ICM: 29% | PAD Endovascular intervention (aortoiliac, femoropopliteal, below-the-knee) | CO2 amount, mL: CO2: NR ICM: 0 ICM amount, mL: CO2: 34 ± 41 ICM: 112 ± 76 ICM type: Iodixanol | CA-AKI: CO2: 2/37 (5%) ICM: 29/154 (19%) Haemodialysis: CO2: 0/37 ICM: 0/154 |
| Diamantopoulus et al. 2020 [33] England | Cohort study Moderate 30 days | Total: 150 CO2: 50 ICM: 100 | Age: CO2: 77.5 ± 10.4 ICM: 76.5 ± 10.5 | Women: CO2: NR ICM: NR | Diabetes mellitus: All: 65% CO2: 66% ICM: 64% | CKD stage 3–5: CO2: 100% ICM: 100% | PAD Endovascular intervention (aortoiliac, femoropopliteal, below-the-knee) | CO2 amount, mL: CO2: NR ICM: 0 ICM amount, mL: CO2: 15.1 ± 14.0 ICM: 115.6 ± 58.1 ICM type: Iodixanol | CA-AKI: CO2: 7/50 (14%) ICM: 29/100 (29%) Haemodialysis: NR |
| Jakobi et al. 2021 [34] Germany | Cohort study Moderate 48 h | Total: 313 CO2: 102 ICM: 211 | Age: CO2: 74.8 ± 8.7 ICM: 72.4 ± 9.3 | Women: CO2: 36.3% ICM: 24.6% | Diabetes mellitus: All: 52% CO2: 51% ICM: 54% | CKD stage 3–5: CO2: 100% ICM: 100% | PAD Endovascular intervention (aortoiliac, femoropopliteal, below-the-knee) | CO2 amount, mL: CO2: 114.5 ± 53.4 ICM: 0 ICM amount, mL: CO2: 41.9 ± 31.6 (N = 86) ICM: 118.9 ± 51.1 ICM type: NR | CA-AKI: CO2: 12/102 (11.8%) ICM: 33/211 (15.6%) Haemodialysis: NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, G.; Glechner, A.; Persad, E.; Klerings, I.; Gartlehner, G.; Moertl, D.; Steiner, S. Risk of Contrast-Associated Acute Kidney Injury in Patients Undergoing Peripheral Angiography with Carbon Dioxide Compared to Iodine-Containing Contrast Agents: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7203. https://doi.org/10.3390/jcm11237203
Wagner G, Glechner A, Persad E, Klerings I, Gartlehner G, Moertl D, Steiner S. Risk of Contrast-Associated Acute Kidney Injury in Patients Undergoing Peripheral Angiography with Carbon Dioxide Compared to Iodine-Containing Contrast Agents: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(23):7203. https://doi.org/10.3390/jcm11237203
Chicago/Turabian StyleWagner, Gernot, Anna Glechner, Emma Persad, Irma Klerings, Gerald Gartlehner, Deddo Moertl, and Sabine Steiner. 2022. "Risk of Contrast-Associated Acute Kidney Injury in Patients Undergoing Peripheral Angiography with Carbon Dioxide Compared to Iodine-Containing Contrast Agents: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 23: 7203. https://doi.org/10.3390/jcm11237203
APA StyleWagner, G., Glechner, A., Persad, E., Klerings, I., Gartlehner, G., Moertl, D., & Steiner, S. (2022). Risk of Contrast-Associated Acute Kidney Injury in Patients Undergoing Peripheral Angiography with Carbon Dioxide Compared to Iodine-Containing Contrast Agents: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(23), 7203. https://doi.org/10.3390/jcm11237203