
Decline in Walking Independence and Related Factors in Hospitalization for Dialysis Initiation: A Retrospective Cohort Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
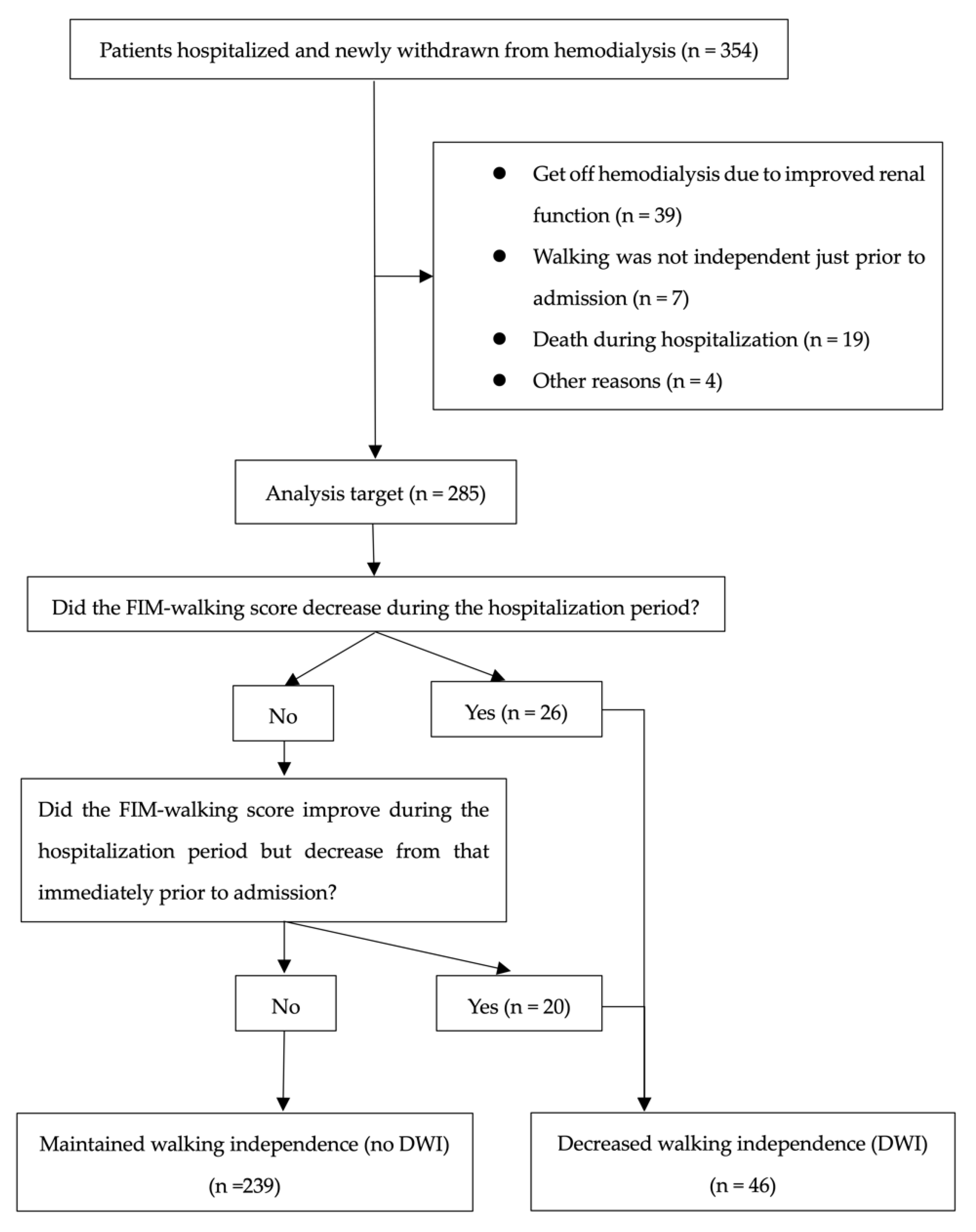
3. Results
3.1. Characteristics of Participants
3.2. Differences between Patients with and without DWI
3.3. Factors Associated with DWI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Isoyama, N.; Qureshi, A.R.; Avesani, C.M.; Lindholm, B.; Barany, P.; Heimburger, O.; Cederholm, T.; Stenvinkel, P.; Carrero, J.J. Comparative associations of muscle mass and muscle strength with mortality in dialysis patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1720–1728. [Google Scholar] [CrossRef] [PubMed]
- Reese, P.P.; Cappola, A.R.; Shults, J.; Townsend, R.R.; Gadegbeku, C.A.; Anderson, C.; Baker, J.F.; Carlow, D.; Sulik, M.J.; Lo, J.C.; et al. Physical performance and frailty in chronic kidney disease. Am. J. Nephrol. 2013, 38, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Hiraki, K.; Yasuda, T.; Hotta, C.; Izawa, K.P.; Morio, Y.; Watanabe, S.; Sakurada, T.; Shibagaki, Y.; Kimura, K. Decreased physical function in pre-dialysis patients with chronic kidney disease. Clin. Exp. Nephrol. 2013, 17, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Kurella Tamura, M.; Covinsky, K.E.; Chertow, G.M.; Yaffe, K.; Landefeld, C.S.; McCulloch, C.E. Functional status of elderly adults before and after initiation of dialysis. N. Engl. J. Med. 2009, 361, 1539–1547. [Google Scholar] [CrossRef]
- Goto, N.A.; van Loon, I.N.; Boereboom, F.T.J.; Emmelot-Vonk, M.H.; Willems, H.C.; Bots, M.L.; Gamadia, L.E.; van Bommel, E.F.H.; Van de Ven, P.J.G.; Douma, C.E.; et al. Association of initiation of maintenance dialysis with functional status and caregiver burden. Clin. J. Am. Soc. Nephrol. 2019, 14, 1039–1047. [Google Scholar] [CrossRef]
- Magalhaes, L.P.; Dos Reis, L.M.; Graciolli, F.G.; Pereira, B.J.; de Oliveira, R.B.; de Souza, A.A.; Moyses, R.M.; Elias, R.M.; Jorgetti, V. Predictive factors of one-year mortality in a cohort of patients undergoing urgent-start hemodialysis. PLoS ONE 2017, 12, e0167895. [Google Scholar] [CrossRef]
- Raffray, M.; Vigneau, C.; Couchoud, C.; Bayat, S. Predialysis care trajectories of patients with ESKD starting dialysis in emergency in France. Kidney Int. Rep. 2021, 6, 156–167. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Mahjoub, F.; Mizouri, R.; Ben Amor, N.; Bacha, M.M.; Khedher, A.; Lahmar, I.; Jamoussi, H. Prevalence of malnutrition for elderly hemodialysis patients. Tunis. Med. 2019, 97, 588–594. [Google Scholar]
- Yoshida, M.; Nakashima, A.; Doi, S.; Maeda, K.; Ishiuchi, N.; Naito, T.; Masaki, T. Lower geriatric nutritional risk index (GNRI) is associated with higher risk of fractures in patients undergoing hemodialysis. Nutrients 2021, 13, 2847. [Google Scholar] [CrossRef]
- Kono, K.; Moriyama, Y.; Yabe, H.; Hara, A.; Ishida, T.; Yamada, T.; Nishida, Y. Relationship between malnutrition and possible sarcopenia in the AWGS 2019 consensus affecting mortality in hemodialysis patients: A prospective cohort study. BMC Nephrol. 2021, 22, 378. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Visser, W.J.; Egmond, A.; Timman, R.; Severs, D.; Hoorn, E.J. Risk factors for muscle loss in hemodialysis patients with high comorbidity. Nutrients 2020, 12, 2494. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.T.; Wu, P.H.; Kuo, M.C.; Lin, M.Y.; Lee, T.C.; Chiu, Y.W.; Hwang, S.J.; Chen, H.C. High cost and low survival rate in high comorbidity incident elderly hemodialysis patients. PLoS ONE 2013, 8, e75318. [Google Scholar] [CrossRef] [PubMed]
- Bland, M.D.; Sturmoski, A.; Whitson, M.; Connor, L.T.; Fucetola, R.; Huskey, T.; Corbetta, M.; Lang, C.E. Prediction of discharge walking ability from initial assessment in a stroke inpatient rehabilitation facility population. Arch. Phys. Med. Rehabil. 2012, 93, 1441–1447. [Google Scholar] [CrossRef]
- Ii, T.; Hirano, S.; Tanabe, S.; Saitoh, E.; Yamada, J.; Mukaino, M.; Watanabe, M.; Sonoda, S.; Otaka, Y. Robot-assisted gait training using Welwalk in hemiparetic stroke patients: An effectiveness study with matched control. J. Stroke Cerebrovasc. Dis. 2020, 29, 105377. [Google Scholar] [CrossRef]
- Snowdon, D.A.; Sounthakith, V.; Kolic, J.; Brooks, S.; Scanlon, S.; Taylor, N.F. Many inpatients may not be physically prepared for community ambulation on discharge from a publicly funded rehabilitation centre: A cross-sectional cohort study. Disabil. Rehabil. 2021, 43, 3672–3679. [Google Scholar] [CrossRef]
- Souza, V.A.; Oliveira, D.; Barbosa, S.R.; Correa, J.; Colugnati, F.A.B.; Mansur, H.N.; Fernandes, N.; Bastos, M.G. Sarcopenia in patients with chronic kidney disease not yet on dialysis: Analysis of the prevalence and associated factors. PLoS ONE 2017, 12, e0176230. [Google Scholar] [CrossRef]
- Shimizu, Y.; Nakata, J.; Yanagisawa, N.; Shirotani, Y.; Fukuzaki, H.; Nohara, N.; Suzuki, Y. Emergent initiation of dialysis is related to an increase in both mortality and medical costs. Sci. Rep. 2020, 10, 19638. [Google Scholar] [CrossRef]
- Chang, J.; Hou, W.W.; Wang, Y.F.; Sun, Q.M. Main risk factors related to activities of daily living in non-dialysis patients with chronic kidney disease stage 3–5: A case-control study. Clin. Interv. Aging 2020, 15, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Bakkal, H.; Dizdar, O.S.; Erdem, S.; Kulakoglu, S.; Akcakaya, B.; Katircilar, Y.; Uludag, K. The relationship between hand grip strength and nutritional status determined by malnutrition inflammation score and biochemical parameters in hemodialysis patients. J. Ren. Nutr. 2020, 30, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; Glynn, L.G.; Murphy, A.W.; Mulqueen, J.; Canavan, M.; Reddan, D.N.; O’Donnell, M. Mild chronic kidney disease and functional impairment in community-dwelling older adults. Age Ageing 2013, 42, 488–494. [Google Scholar] [CrossRef]
- Sabatino, A.; Cuppari, L.; Stenvinkel, P.; Lindholm, B.; Avesani, C.M. Sarcopenia in chronic kidney disease: What have we learned so far? J. Nephrol. 2021, 34, 1347–1372. [Google Scholar] [CrossRef]
- Miyazaki, S.; Iino, N.; Koda, R.; Narita, I.; Kaneko, Y. Brain-derived neurotrophic factor is associated with sarcopenia and frailty in Japanese hemodialysis patients. Geriatr. Gerontol. Int. 2021, 21, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.R.; Kim, J.K.; Lee, H.S.; Kim, S.G.; Choi, E.K. Serum levels of protein carbonyl, a marker of oxidative stress, are associated with overhydration, sarcopenia and mortality in hemodialysis patients. BMC Nephrol. 2020, 21, 281. [Google Scholar] [CrossRef]
- Wang, D.X.M.; Yao, J.; Zirek, Y.; Reijnierse, E.M.; Maier, A.B. Muscle mass, strength, and physical performance predicting activities of daily living: A meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 3–25. [Google Scholar] [CrossRef]
- Vanden Wyngaert, K.; Van Craenenbroeck, A.H.; Van Biesen, W.; Dhondt, A.; Tanghe, A.; Van Ginckel, A.; Celie, B.; Calders, P. The effects of aerobic exercise on eGFR, blood pressure and VO2peak in patients with chronic kidney disease stages 3–4: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0203662. [Google Scholar] [CrossRef]
- Villanego, F.; Naranjo, J.; Vigara, L.A.; Cazorla, J.M.; Montero, M.E.; Garcia, T.; Torrado, J.; Mazuecos, A. Impact of physical exercise in patients with chronic kidney disease: Sistematic review and meta-analysis. Nefrologia 2020, 40, 237–252. [Google Scholar] [CrossRef]
- Cumming, T.B.; Thrift, A.G.; Collier, J.M.; Churilov, L.; Dewey, H.M.; Donnan, G.A.; Bernhardt, J. Very early mobilization after stroke fast-tracks return to walking: Further results from the phase II AVERT randomized controlled trial. Stroke 2011, 42, 153–158. [Google Scholar] [CrossRef]
- Iwai, K.; Hatanaka, Y.; Kawaguchi, T.; Araki, S.I. Evaluation of the safety, effectiveness, and health-related QOL impact of early rehabilitation in patients with nephrotic syndrome. Clin. Exp. Nephrol. 2019, 23, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Mori, K. Maintenance of skeletal muscle to counteract sarcopenia in patients with advanced chronic kidney disease and especially those undergoing hemodialysis. Nutrients 2021, 13, 1538. [Google Scholar] [CrossRef] [PubMed]
- Mitsutake, S.; Ishizaki, T.; Teramoto, C.; Shimizu, S.; Ito, H. Patterns of co-occurrence of chronic disease among older adults in Tokyo, Japan. Prev. Chronic Dis. 2019, 16, E11. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Yang, C.; Chu, H.; Wu, J.; Lin, K.; Shi, Y.; Wang, H.; Kong, G.; Zhang, L.; China Kidney Disease Network Working, G. Association between the Charlson Comorbidity Index and the risk of 30-day unplanned readmission in patients receiving maintenance dialysis. BMC Nephrol. 2019, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Fois, A.; Chatrenet, A.; Cataldo, E.; Lippi, F.; Kaniassi, A.; Vigreux, J.; Froger, L.; Mongilardi, E.; Capizzi, I.; Biolcati, M.; et al. Moderate protein restriction in advanced CKD: A feasible option in an elderly, high-comorbidity population. A stepwise multiple-choice system approach. Nutrients 2018, 11, 36. [Google Scholar] [CrossRef]
- Chae, J.W.; Song, C.S.; Kim, H.; Lee, K.B.; Seo, B.S.; Kim, D.I. Prediction of mortality in patients undergoing maintenance hemodialysis by Charlson Comorbidity Index using ICD-10 database. Nephron Clin. Pract. 2011, 117, c379–c384. [Google Scholar] [CrossRef] [PubMed]
- Di Iorio, B.; Cillo, N.; Cirillo, M.; De Santo, N.G. Charlson Comorbidity Index is a predictor of outcomes in incident hemodialysis patients and correlates with phase angle and hospitalization. Int. J. Artif. Organs 2004, 27, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.H.; Hsu, Y.J.; Tzeng, W.C. Correlation between physical activity and psychological distress in patients receiving hemodialysis with comorbidities: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 3972. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Zhang, D. Multimorbidity in the elderly: A systematic bibliometric analysis of research output. Int. J. Environ. Res. Public Health 2021, 19, 353. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Rajan, V.; Lin, E.; Hu, Z.; Han, H.Q.; Zhou, X.; Song, Y.; Min, H.; Wang, X.; Du, J.; et al. Pharmacological inhibition of myostatin suppresses systemic inflammation and muscle atrophy in mice with chronic kidney disease. FASEB J. 2011, 25, 1653–1663. [Google Scholar] [CrossRef]
- Sovatzidis, A.; Chatzinikolaou, A.; Fatouros, I.G.; Panagoutsos, S.; Draganidis, D.; Nikolaidou, E.; Avloniti, A.; Michailidis, Y.; Mantzouridis, I.; Batrakoulis, A.; et al. Intradialytic cardiovascular exercise training alters redox status, reduces inflammation and improves physical performance in patients with chronic kidney disease. Antioxidants 2020, 9, 868. [Google Scholar] [CrossRef] [PubMed]
- Michel, A.; Pladys, A.; Bayat, S.; Couchoud, C.; Hannedouche, T.; Vigneau, C. Deleterious effects of dialysis emergency start, insights from the French REIN registry. BMC Nephrol. 2018, 19, 233. [Google Scholar] [CrossRef] [PubMed]
- Arulkumaran, N.; Navaratnarajah, A.; Pillay, C.; Brown, W.; Duncan, N.; McLean, A.; Taube, D.; Brown, E.A. Causes and risk factors for acute dialysis initiation among patients with end-stage kidney disease-a large retrospective observational cohort study. Clin. Kidney J. 2019, 12, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Engberg, J.; Castle, N.G.; McCaffrey, D. Physical restraint initiation in nursing homes and subsequent resident health. Gerontologist 2008, 48, 442–452. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | N, Mean, Median |
|---|---|
| Sex | |
| Male [N, (%)] | 190 (66.7) |
| Female [N, (%)] | 95 (33.3) |
| Age (years) | 68.4 ± 14.4 |
| Median length of hospitalization (days) | 14 (12–28) |
| DWI [N, (%)] | 46 (16.1) |
| Hypertension [N, (%)] | 211 (74.0) |
| Diabetes mellitus [N, (%)] | 118 (41.4) |
| Hyperlipidemia [N, (%)] | 94 (33.0) |
| Previous history of CVD [N, (%)] | 123 (43.2) |
| Number of rehabilitations [N, (%)] | 84 (29.5) |
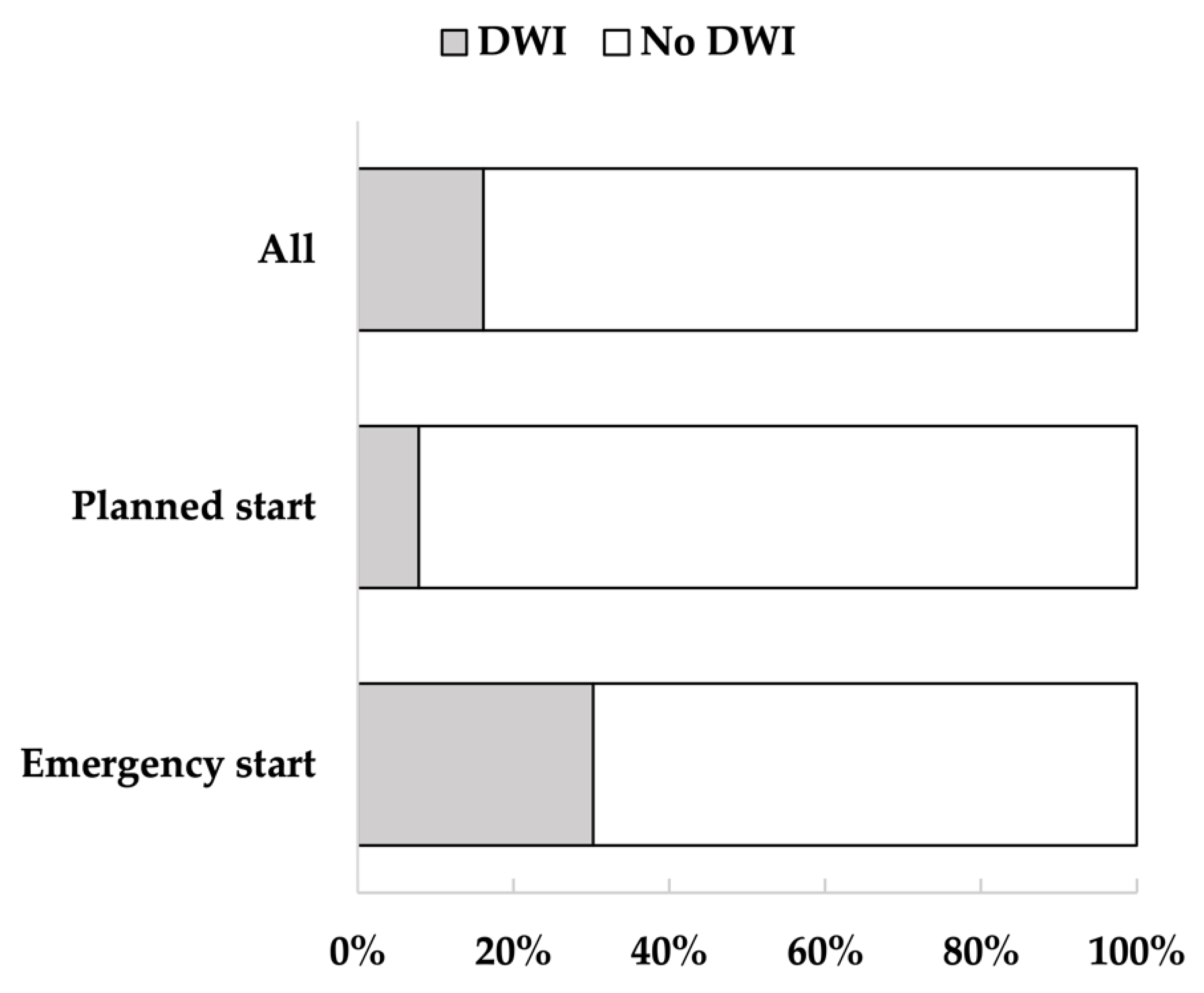
| Emergency dialysis start [N, (%)] | 106 (37.2) |
| Creatinine (mg/dL) | 7.7 ± 3.0 |
| eGFR (mL/min/1.73 m2) | 7.1 ± 6.3 |
| Geriatric Nutritional Risk Index | 78.2 ± 27.8 |
| Malnutrition | 159 (57.4) |
| DWI (N = 46) | No DWI (N = 239) | p-Value | |
|---|---|---|---|
| Male [N, (%)] | 35 (76.1) | 155 (64.9) | 0.139 |
| Age (years) | 78.5 ± 8.2 | 66.4 ± 14.6 | <0.001 * |
| Height (cm) | 158.0 ± 8.1 | 159.6 ± 9.4 | 0.287 |
| Body weight (kg) | 56.2 ± 10.0 | 61.2 ± 15.9 | 0.127 |
| BMI (kg/m2) | 22.5 ± 3.6 | 23.9 ± 5.1 | 0.213 |
| Median length of hospitalization (days) | 34 (26–64) | 13 (12–22) | <0.001 * |
| FIM-walking score at hospitalization < 6 [N, (%)] | 27 (58.7) | 31 (13.0) | <0.001 * |
| Number of rehabilitations [N, (%)] | 33 (71.7) | 51 (21.3) | <0.001 * |
| EDS [N, (%)] | 32 (69.6) | 74 (31.0) | <0.001 * |
| Malnutrition [N, (%)] | 31 (72.1) | 128 (54.7) | 0.034 * |
| High CCI [N, (%)] | 37 (80.4) | 108 (45.2) | <0.001* |
| CRP (mg/dL) | 0.43 (0.16–0.57) | 0.08 (0.03–0.17) | <0.001 * |
| Alb (g/dL) | 3.5 (3.1–3.8) | 3.5 (3.2–3.9) | 0.145 |
| Hb (g/dL) | 9.4 (9.1–10.0) | 9.6 (9.0–10.3) | 0.645 |
| Univariate Regression | Multiple Logistic | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | ||||||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age | 1.075 | 1.040–1.112 | <0.001 * | 1.089 | 1.045–1.135 | <0.001 * | 1.123 | 1.067–1.182 | <0.001 * |
| High CCI | 4.987 | 2.305–10.788 | <0.001 * | 4.540 | 1.874–11.001 | 0.001 * | 4.706 | 1.768–12.522 | 0.002 * |
| CRP | 1.296 | 1.142–1.471 | <0.001 * | 1.163 | 1.049–1.291 | 0.004 * | 1.180 | 1.057–1.317 | 0.003 * |
| EDS | 5.097 | 2.568–10.113 | <0.001 * | 2.720 | 1.217–6.080 | 0.015 * | 2.957 | 1.239–7.059 | 0.015 * |
| Sex (male) | 0.580 | 0.280–1.201 | 0.142 | 0.839 | 0.336–2.093 | 0.706 | |||
| Malnutrition | 2.139 | 1.047–4.370 | 0.037 * | 1.535 | 0.645–3.654 | 0.332 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirano, Y.; Fujikura, T.; Kono, K.; Ohashi, N.; Yamaguchi, T.; Hanajima, W.; Yasuda, H.; Yamauchi, K. Decline in Walking Independence and Related Factors in Hospitalization for Dialysis Initiation: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 6589. https://doi.org/10.3390/jcm11216589
Hirano Y, Fujikura T, Kono K, Ohashi N, Yamaguchi T, Hanajima W, Yasuda H, Yamauchi K. Decline in Walking Independence and Related Factors in Hospitalization for Dialysis Initiation: A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(21):6589. https://doi.org/10.3390/jcm11216589
Chicago/Turabian StyleHirano, Yuma, Tomoyuki Fujikura, Kenichi Kono, Naro Ohashi, Tomoya Yamaguchi, Wataru Hanajima, Hideo Yasuda, and Katsuya Yamauchi. 2022. "Decline in Walking Independence and Related Factors in Hospitalization for Dialysis Initiation: A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 21: 6589. https://doi.org/10.3390/jcm11216589
APA StyleHirano, Y., Fujikura, T., Kono, K., Ohashi, N., Yamaguchi, T., Hanajima, W., Yasuda, H., & Yamauchi, K. (2022). Decline in Walking Independence and Related Factors in Hospitalization for Dialysis Initiation: A Retrospective Cohort Study. Journal of Clinical Medicine, 11(21), 6589. https://doi.org/10.3390/jcm11216589