
Clinical Evaluation of Non-Contrast-Enhanced Radial Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography in Comparison to Contrast-Enhanced Computed Tomography Angiography for the Evaluation of Endoleaks after Abdominal Endovascular Aneurysm Repair
 , , ,
, , ,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Study Population
2.2. CE-CTA
2.3. Non-CE Radial Electrocardiogram Triggered QISS-MRA
2.4. Image Analysis
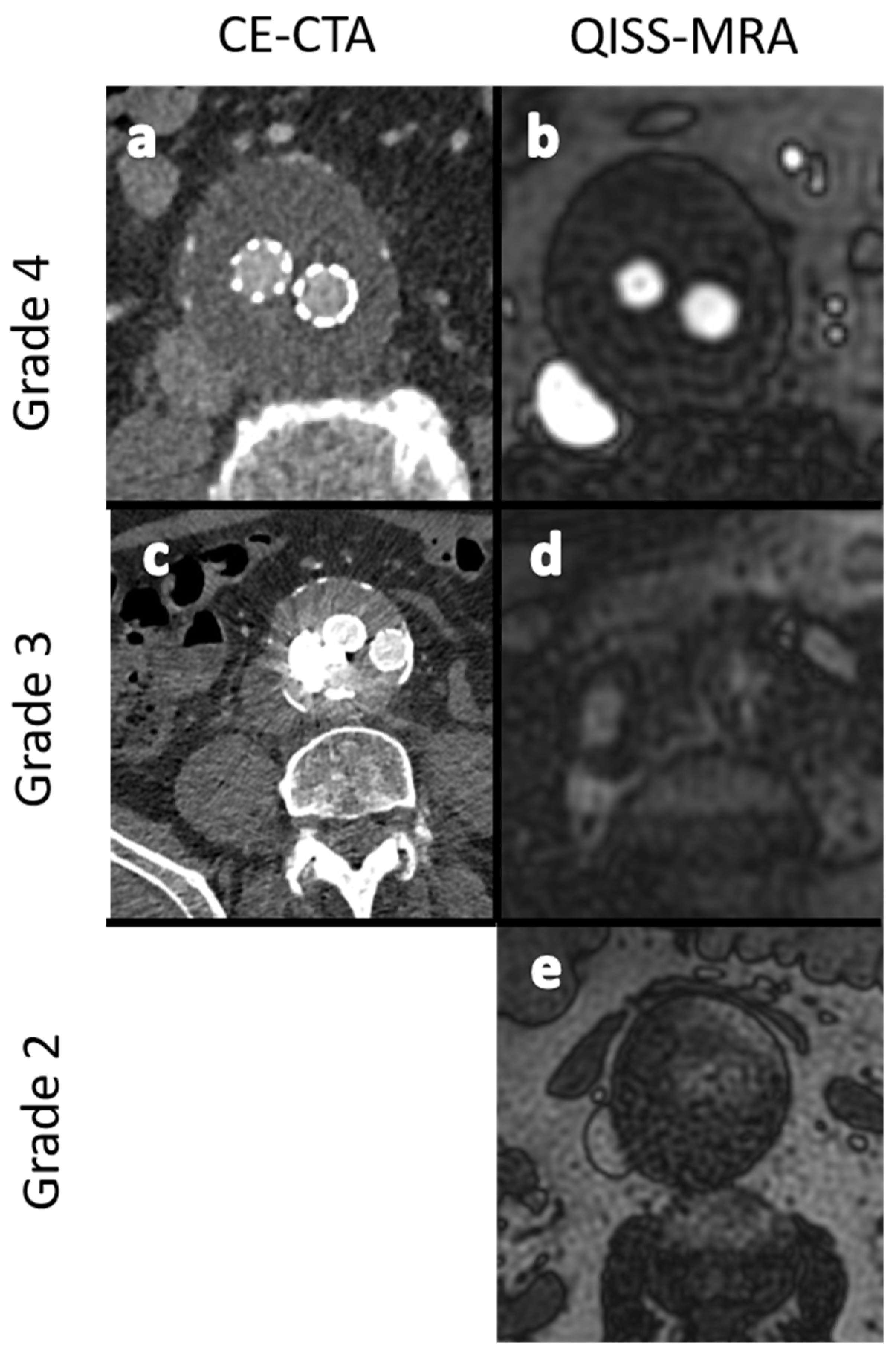
- Grade 1: Poor arterial signal and poor vascular contrast with undefinable outlining of aneurysm. Non-diagnostic.
- Grade 2: Ill-defined vessel-borders with suboptimal image quality for diagnosis.
- Grade 3: Minor inhomogeneities, and the vessel outlining is clearly visible.
- Grade 4: Excellent image without artifacts.
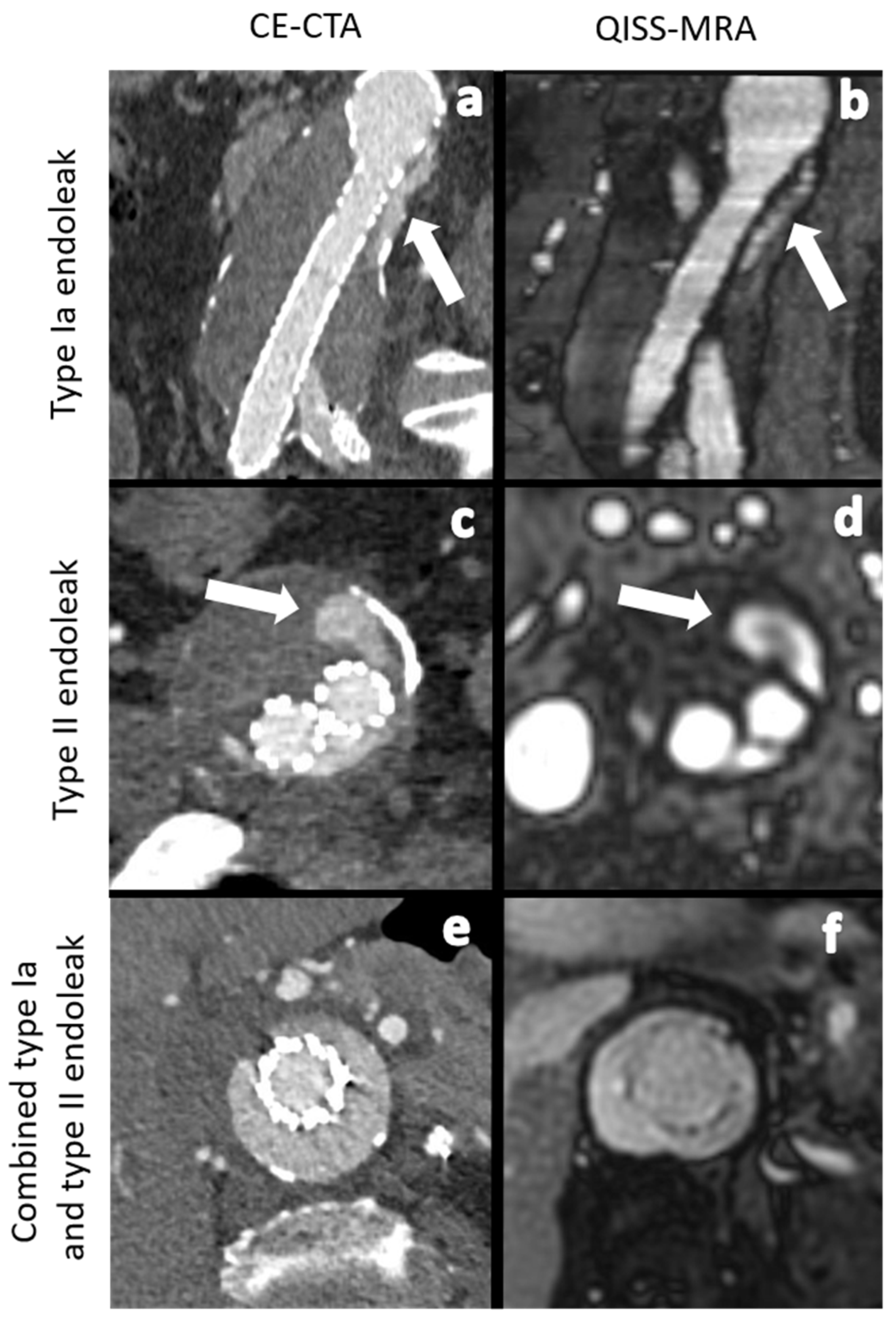
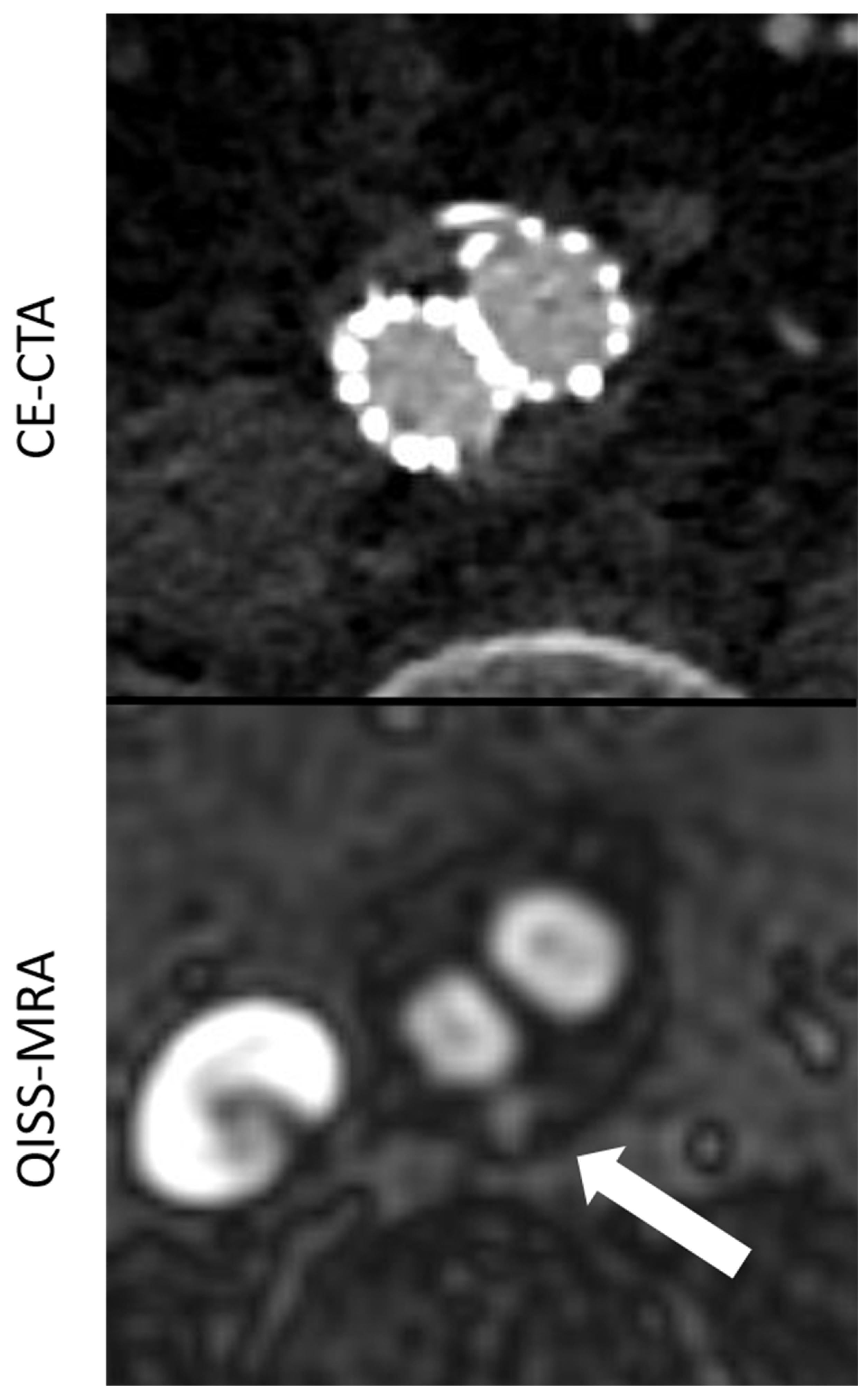
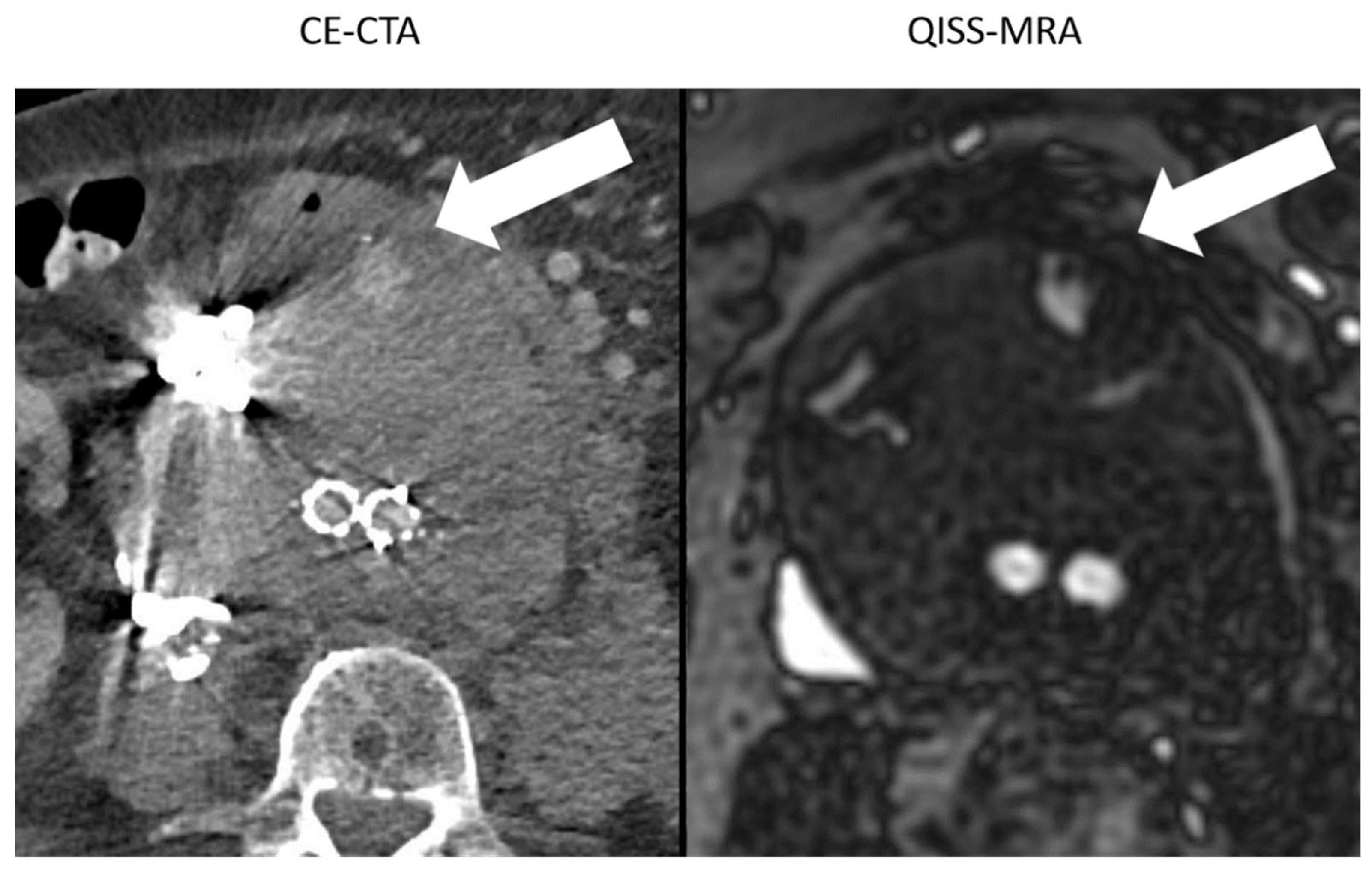
2.5. Modality-Specific Diagnosis of Endoleaks
2.6. Observer-Specific Intermodal Assessment of Endoleak and Endoleak Subtype Diagnosis
2.7. Observer-Specific Intermodal Assessment of Aneurysm Diameter
2.8. Statistical Analysis
3. Results
3.1. Image Quality Assessment
3.2. Comparison between the Imaging Modalities concerning Aneurysm Size
3.3. Number of Diagnosed Endoleaks and Endoleak Types
3.4. Observer-Specific Intermodal Assessment of Endoleaks and Endoleak-Subtype Diagnosis
3.5. Modality-Specific Agreement on Endoleak Diagnosis
4. Discussion
4.1. Aneurysm Diameter Measurement
4.2. Modality-Specific- and Observer-Specific Agreement on Endoleak Diagnosis and Image Quality
4.3. Visualization of Endoleaks and Image Quality
4.4. Avoidance of Radiation and Iodine-Based Contrast Agents
4.5. Clinically Efficient Measurement Time
4.6. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Patel, R.; Sweeting, M.J.; Powell, J.T.; Greenhalgh, R.M.; EVAR Trial Investigators. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): A randomised controlled trial. Lancet 2016, 388, 2366–2374. [Google Scholar] [CrossRef]
- Rand, T.; Uberoi, R.; Cil, B.; Munneke, G.; Tsetis, D. Quality improvement guidelines for imaging detection and treatment of endoleaks following endovascular aneurysm repair (EVAR). Cardiovasc. Intervent. Radiol. 2013, 36, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice-European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed]
- Eskandari, M.K.; Yao, J.S.; Pearce, W.H.; Rutherford, R.B.; Veith, F.J.; Harris, P.; Bernhard, V.M.; Becker, G.J.; Morasch, M.D.; Chrisman, H.B.; et al. Surveillance after endoluminal repair of abdominal aortic aneurysms. Cardiovasc. Surg. 2001, 9, 469–471. [Google Scholar] [CrossRef]
- Kazimierczak, W.; Serafin, Z.; Kazimierczak, N.; Ratajczak, P.; Leszczyński, W.; Bryl, Ł.; Lemanowicz, A. Contemporary imaging methods for the follow-up after endovascular abdominal aneurysm repair: A review. Videosurg. Other Miniinvasive Tech. 2019, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Manning, B.J.; Kristmundsson, T.; Sonesson, B.; Resch, T. Abdominal aortic aneurysm diameter: A comparison of ultrasound measurements with those from standard and three-dimensional computed tomography reconstruction. J. Vasc. Surg. 2009, 50, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Salehi Ravesh, M.; Langguth, P.; Pfarr, J.A.; Schupp, J.; Trentmann, J.; Koktzoglou, I.; Edelman, R.R.; Graessner, J.; Greiser, A.; Hautemann, D.; et al. Non-contrast-enhanced magnetic resonance imaging for visualization and quantification of endovascular aortic prosthesis, their endoleaks and aneurysm sacs at 1.5 T. Magn. Reson. Imaging 2019, 60, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Silvers, R.I.; Thakrar, K.H.; Metzl, M.D.; Nazari, J.; Giri, S.; Koktzoglou, I. Nonenhanced MR angiography of the pulmonary arteries using single-shot radial quiescent-interval slice-selective (QISS): A technical feasibility study. J. Cardiovasc. Magn. Reson. 2017, 19, 48. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Carr, J.C. QISS MR Angiography: An Alternative to CT Angiography for Peripheral Vascular Evaluation. JACC Cardiovasc. Imaging 2017, 10, 1125–1127. [Google Scholar] [CrossRef] [PubMed]
- Dobritz, M.; Engels, H.P.; Schneider, A.; Bauer, J.; Rummeny, E.J. Detection of intestinal bleeding with multi-detector row CT in an experimental setup. How many acquisitions are necessary? Eur. Radiol. 2009, 19, 2862–2869. [Google Scholar] [CrossRef]
- Cassagnes, L.; Pérignon, R.; Amokrane, F.; Petermann, A.; Bécaud, T.; Saint-Lebes, B.; Chabrot, P.; Rousseau, H.; Boyer, L. Aortic stent-grafts: Endoleak surveillance. Diagn. Interv. Imaging 2016, 97, 19–27. [Google Scholar] [CrossRef]
- Koike, Y.; Ishida, K.; Hase, S.; Kobayashi, Y.; Nishimura, J.; Yamasaki, M.; Hosaka, N. Dynamic volumetric CT angiography for the detection and classification of endoleaks: Application of cine imaging using a 320-row CT scanner with 16-cm detectors. J. Vasc. Interv. Radiol. 2014, 25, 1172–1180.e1. [Google Scholar] [CrossRef] [PubMed]
- Leisman, S. Radiocontrast Toxicity. Adv. Chronic. Kidney Dis. 2020, 27, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Bobadilla, J.L.; Suwanabol, P.A.; Reeder, S.B.; Pozniak, M.A.; Bley, T.A.; Tefera, G. Clinical implications of non-contrast-enhanced computed tomography for follow-up after endovascular abdominal aortic aneurysm repair. Ann. Vasc. Surg. 2013, 27, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Edelman, R.R.; Giri, S.; Dunkle, E.; Galizia, M.; Amin, P.; Koktzoglou, I. Quiescent-inflow single-shot magnetic resonance angiography using a highly undersampled radial k-space trajectory. Magn. Reason. Med. 2013, 70, 1662–1668. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protocol Parameters | |
|---|---|
| TR/TE (ms) | 993.9/1.7 |
| Acquisition matrix | 318 × 318 |
| Reconstructed voxel size (mm³) | 1.1 × 1.1 × 2.5 |
| BW (Hz/Px) | 1359 |
| Slice orientation | Transverse, sagittal, coronal |
| Distance factor (%) | −20 |
| FA (°) | 120 |
| GRAPPA acceleration factor/reference line | --- |
| Other |
|
| total acquisition time (min:sec) depending on the heart rate | 1:00 |
| Observer 1 | Observer 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| QISS-MRA | CE-CTA | κ-Value | p-Value | QISS-MRA | CE-CTA | κ-Value | p-Value | ||
| Type Ia | 1 (6.2%) | 1 (8.3%) | 1 | Type Ia | 1 (7.1%) | 1 (9.0%) | 1 | ||
| Type Ib | 3 (18.7%) | 3 (25.0%) | 1 | Type Ib | 3 (21.4%) | 3 (27.0%) | 1 | ||
| Type II | 11 (68.7%) | 8 (66.7%) | 0.71 | <0.01 | Type II | 9 (64.2%) | 7 (63.6%) | 0.79 | <0.01 |
| Type III | 0 (0%) | 0 (0%) | Type III | 0 (0%) | 0 (0%) | 1 | |||
| Type V | 1 (6.2%) | 0 (0%) | Type V | 1 (7.1%) | 0 (0%) | ||||
| Total number | 16 | 12 | Total number | 14 | 11 | ||||
| QISS-MRA | CE-CTA | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Observer 1 | Observer 2 | κ-Value | p-Value | Observer 1 | Observer 2 | κ-Value | p-Value | ||
| Type Ia | 1 (6.2%) | 1 (7.1%) | 1 | Type Ia | 1 (8.3%) | 1 (9.0%) | 1 | ||
| Type Ib | 3 (18.7%) | 3 (21.4%) | 1 | Type Ib | 3 (25.0%) | 3 (27.2%) | 1 | ||
| Type II | 11 (68.7%) | 9 (64.2%) | 0.80 | <0.01 | Type II | 8 (66.7%) | 7 (63.6%) | 0.89 | <0.01 |
| Type III | 0 (0%) | 0 (0%) | 1 | Type III | 0 (0%) | 0 (0%) | 1 | ||
| Type V | 1 (6.2%) | 1 (7.1%) | 1 | Type V | 0 (0%) | 0 (0%) | 1 | ||
| Total number | 16 | 14 | Total number | 12 | 11 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mostafa, K.; Pfarr, J.; Langguth, P.; Schäfer, J.P.; Trentmann, J.; Koktzoglou, I.; Edelman, R.R.; Bueno Neves, F.; Graessner, J.; Both, M.; et al. Clinical Evaluation of Non-Contrast-Enhanced Radial Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography in Comparison to Contrast-Enhanced Computed Tomography Angiography for the Evaluation of Endoleaks after Abdominal Endovascular Aneurysm Repair. J. Clin. Med. 2022, 11, 6551. https://doi.org/10.3390/jcm11216551
Mostafa K, Pfarr J, Langguth P, Schäfer JP, Trentmann J, Koktzoglou I, Edelman RR, Bueno Neves F, Graessner J, Both M, et al. Clinical Evaluation of Non-Contrast-Enhanced Radial Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography in Comparison to Contrast-Enhanced Computed Tomography Angiography for the Evaluation of Endoleaks after Abdominal Endovascular Aneurysm Repair. Journal of Clinical Medicine. 2022; 11(21):6551. https://doi.org/10.3390/jcm11216551
Chicago/Turabian StyleMostafa, Karim, Julian Pfarr, Patrick Langguth, Jost Philipp Schäfer, Jens Trentmann, Ioannis Koktzoglou, Robert R. Edelman, Fernando Bueno Neves, Joachim Graessner, Marcus Both, and et al. 2022. "Clinical Evaluation of Non-Contrast-Enhanced Radial Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography in Comparison to Contrast-Enhanced Computed Tomography Angiography for the Evaluation of Endoleaks after Abdominal Endovascular Aneurysm Repair" Journal of Clinical Medicine 11, no. 21: 6551. https://doi.org/10.3390/jcm11216551
APA StyleMostafa, K., Pfarr, J., Langguth, P., Schäfer, J. P., Trentmann, J., Koktzoglou, I., Edelman, R. R., Bueno Neves, F., Graessner, J., Both, M., Jansen, O., & Salehi Ravesh, M. (2022). Clinical Evaluation of Non-Contrast-Enhanced Radial Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography in Comparison to Contrast-Enhanced Computed Tomography Angiography for the Evaluation of Endoleaks after Abdominal Endovascular Aneurysm Repair. Journal of Clinical Medicine, 11(21), 6551. https://doi.org/10.3390/jcm11216551