
New Efficient Method for Hysteroscopic Isthmoplasty: Four Simple Steps Lead to a Significant Improvement in Bleeding Status
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
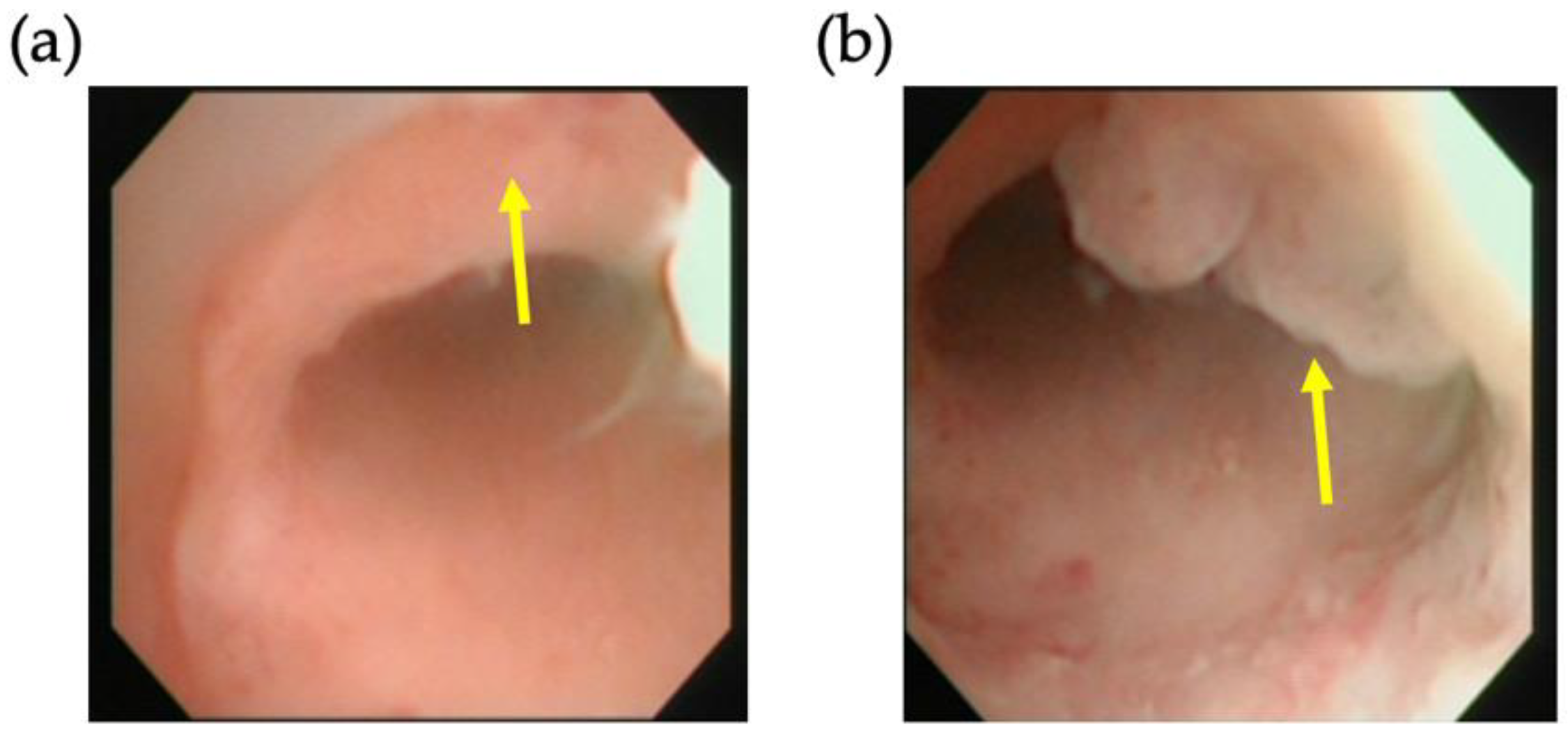
2.2. Performed Surgery
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients
3.2. Magnificent Modification of Procedure
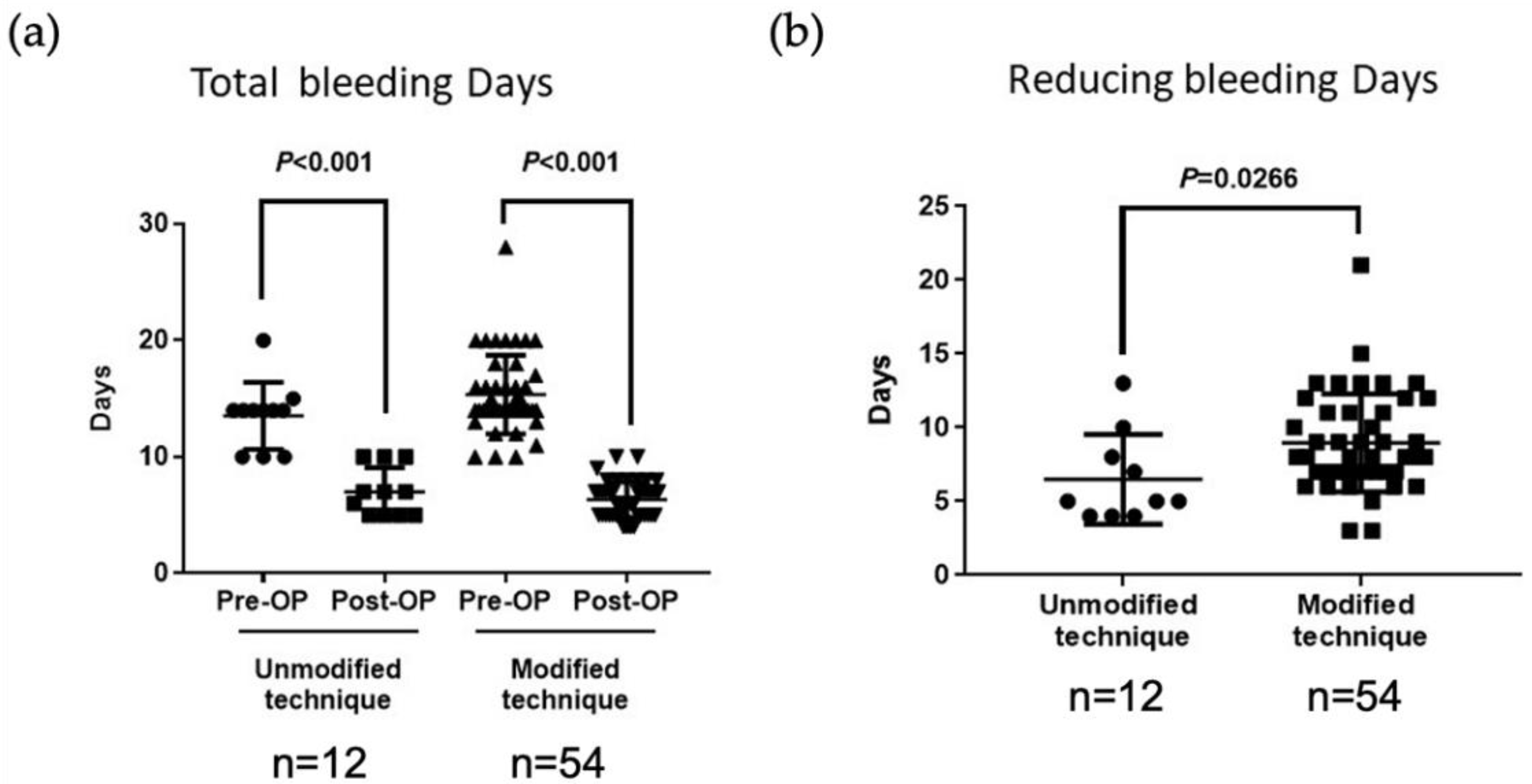
3.3. Significant Improvement of the Clinical Successful Rate
3.4. Minimal Invasion with Less Blood Loss and Short Admission
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nguyen, A.D.; Nguyen, H.T.T.; Duong, G.T.T.; Phan, T.T.H.; Do, D.T.; Tran, D.A.; Nguyen, T.K.; Nguyen, T.B.; Ville, Y. Improvement of symptoms after hysteroscopic isthmoplasty in women with abnormal uterine bleeding and expected pregnancy: A prospective study. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102326. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, F.; Torbati, L.; Akhbari, F.; Shahrzad, G. Appearance of Uterine Scar Due to Previous Cesarean Section on Hysterosalpingography: Various Shapes, Locations and Sizes. Iran. J. Radiol. 2013, 10, 103–110. [Google Scholar] [CrossRef]
- Allornuvor, G.F.N.; Xue, M.; Zhu, X.; Xu, D. The definition, aetiology, presentation, diagnosis and management of previous caesarean scar defects. J. Obstet. Gynaecol. 2013, 33, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Kremer, T.G.; Ghiorzi, I.B.; Dibi, R.P. Isthmocele: An overview of diagnosis and treatment. Rev. Assoc. Médica Bras. 2019, 65, 714–721. [Google Scholar] [CrossRef] [PubMed]
- De Vaate, A.J.M.B.; Van Der Voet, L.F.; Naji, O.; Witmer, M.; Veersema, S.; Brölmann, H.A.M.; Bourne, T.; Huirne, J.A.F. Prevalence, potential risk factors for development and symptoms related to the presence of uterine niches following Cesarean section: Systematic review. Ultrasound Obstet. Gynecol. 2014, 43, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Oehler, R.; Nirgianakis, K.; Mueller, M. The Rendez-vous technique for treatment of caesarean scar defects: A novel combined endoscopic approach. Surg. Endosc. 2016, 30, 770–771. [Google Scholar]
- Park, I.Y.; Kim, M.R.; Lee, H.N.; Gen, Y.; Kim, M.J. Risk factors for Korean women to develop an isthmocele after a cesarean section. BMC Pregnancy Childbirth 2018, 18, 162. [Google Scholar] [CrossRef]
- Feng, Y.-L.; Li, M.-X.; Liang, X.-Q.; Li, X.-M. Hysteroscopic Treatment of Postcesarean Scar Defect. J. Minim. Invasive Gynecol. 2012, 19, 498–502. [Google Scholar] [CrossRef]
- Futyma, K.; Gałczyński, K.; Romanek, K.; Filipczak, A.; Rechberger, T. When and how should we treat cesarean scar defect—Isthmocoele? Ginekol. Pol. 2016, 87, 664–668. [Google Scholar] [CrossRef]
- Setubal, A.; Alves, J.; Osório, F.; Guerra, A.; Fernandes, R.; Albornoz, J.; Sidiropoulou, Z. Treatment for Uterine Isthmocele, A Pouchlike Defect at the Site of a Cesarean Section Scar. J. Minim. Invasive Gynecol. 2018, 25, 38–46. [Google Scholar] [CrossRef]
- Chang, Y.; Tsai, E.M.; Long, C.Y.; Lee, C.L.; Kay, N. Resectoscopic treatment combined with sonohysterographic evaluation of women with postmenstrual bleeding as a result of previous cesarean delivery scar defects. Am. J. Obstet. Gynecol. 2009, 200, 370.e1–370.e4. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-J.; Huang, H.-J.; Chao, A.; Lin, Y.-P.; Pan, Y.-J.; Horng, S.-G. Challenges in the transvaginal management of abnormal uterine bleeding secondary to cesarean section scar defect. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 154, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Shapira, M.; Mashiach, R.; Meller, N.; Watad, H.; Baron, A.; Bouaziz, J.; Cohen, S.B. Clinical Success Rate of Extensive Hysteroscopic Cesarean Scar Defect Excision and Correlation to Histologic Findings. J. Minim. Invasive Gynecol. 2019, 27, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.L.; Chang, Y.Y.; Ho, M.; Wang, A.M.-H.; Lin, W.C. Hysteroscopic transcervical resection: A straightforward method corrects bleeding related to cesarean section scar defects. Am. J. Obstet. Gynecol. 2011, 204, 278.e1–278.e2. [Google Scholar] [CrossRef]
- Abacjew-Chmylko, A.; Wydra, D.G.; Olszewska, H. Hysteroscopy in the treatment of uterine cesarean section scar diverticulum: A systematic review. Adv. Med Sci. 2017, 62, 230–239. [Google Scholar] [CrossRef]
- Tsuji, S.; Kimura, F.; Yamanaka, A.; Hanada, T.; Hirata, K.; Takebayashi, A.; Takashi, M.; Seko-Nitta, A.; Murakami, T. Impact of hysteroscopic surgery for isthmocele associated with cesarean scar syndrome. J. Obstet. Gynaecol. Res. 2017, 44, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Ludwin, A.; Vilos, G.A.; Török, P.; Tesarik, J.; Vitagliano, A.; Lasmar, R.B.; Chiofalo, B. From hysteroscopy to laparoendoscopic surgery: What is the best surgical approach for symptomatic isthmocele? A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2020, 301, 33–52. [Google Scholar] [CrossRef]
- de Albornoz AV, C.; Carrasco, I.L.; Pastor, N.M.; Blanco, C.M.; Matos, M.M.; Pacheco, L.A.; Bartolomé, E.M. Outcomes after Hysteroscopic Treatment of Symptomatic Isthmoceles in Patients with Abnormal Uterine Bleeding and Pelvic Pain: A Prospective Case Series. Int. J. Fertil. Steril. 2019, 13, 108–112. [Google Scholar]
- Li, C.; Guo, Y.; Liu, Y.; Cheng, J.; Zhang, W. Hysteroscopic and laparoscopic management of uterine defects on previous cesarean delivery scars. J. Périnat. Med. 2014, 42, 363–370. [Google Scholar] [CrossRef]
- Fabres, C.; Arriagada, P.; Fernández, C.; MacKenna, A.; Zegers, F.; Fernández, E. Surgical treatment and follow-up of women with intermenstrual bleeding due to cesarean section scar defect. J. Minim. Invasive Gynecol. 2005, 12, 25–28. [Google Scholar] [CrossRef]
- Pérez-Medina, T.; Sauco, J.S.; Ríos, M.; Pereira, A.; Argila, N.; Cabezas, E.; Cayuela, E. Hysteroscopy in Pregnancy-Related Conditions: Descriptive Analysis in 273 Patients. J. Minim. Invasive Gynecol. 2014, 21, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Raimondo, G.; Grifone, G.; Raimondo, D.; Seracchioli, R.; Scambia, G.; Masciullo, V. Hysteroscopic Treatment of Symptomatic Cesarean-induced Isthmocele: A Prospective Study. J. Minim. Invasive Gynecol. 2015, 22, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Tanimura, S.; Funamoto, H.; Hosono, T.; Shitano, Y.; Nakashima, M.; Ametani, Y.; Nakano, T. New diagnostic criteria and operative strategy for cesarean scar syndrome: Endoscopic repair for secondary infertility caused by cesarean scar defect. J. Obstet. Gynaecol. Res. 2015, 41, 1363–1369. [Google Scholar] [CrossRef]
- Xie, H.; Wu, Y.; Yu, F.; He, M.; Cao, M.; Yao, S. A Comparison of Vaginal Surgery and Operative Hysteroscopy for the Treatment of Cesarean-Induced Isthmocele: A Retrospective Review. Gynecol. Obstet. Investig. 2014, 77, 78–83. [Google Scholar] [CrossRef]
- Zhang, Y. A Comparative Study of Transvaginal Repair and Laparoscopic Repair in the Management of Patients With Previous Cesarean Scar Defect. J. Minim. Invasive Gynecol. 2016, 23, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Gubbini, G.; Casadio, P.; Marra, E. Resectoscopic Correction of the “Isthmocele” in Women with Postmenstrual Abnormal Uterine Bleeding and Secondary Infertility. J. Minim. Invasive Gynecol. 2008, 15, 172–175. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, M.; Wang, Q.; Chen, J.; Ding, J.; Hua, K. Prospective evaluation of five methods used to treat cesarean scar defects. Int. J. Gynecol. Obstet. 2016, 134, 336–339. [Google Scholar] [CrossRef]
- Api, M.; Boza, A.; Gorgen, H.; Api, O. Should Cesarean Scar Defect Be Treated Laparoscopically? A Case Report and Review of the Literature. J. Minim. Invasive Gynecol. 2015, 22, 1145–1152. [Google Scholar] [CrossRef]
- Aimi, G.; Buggio, L.; Berlanda, N.; Vercellini, P. Laparoscopic repair of a symptomatic post–cesarean section isthmocele: A video case report. Fertil. Steril. 2017, 107, e17–e18. [Google Scholar] [CrossRef][Green Version]
- Ades, A.; Parghi, S. Laparoscopic Resection of Cesarean Scar Ectopic Pregnancy. J. Minim. Invasive Gynecol. 2017, 24, 533–535. [Google Scholar] [CrossRef]
- Mahmoud, M.S.; Nezhat, F.R. Robotic-assisted Laparoscopic Repair of a Cesarean Section Scar Defect. J. Minim. Invasive Gynecol. 2015, 22, 1135–1136. [Google Scholar] [CrossRef] [PubMed]
- Yalcinkaya, T.M.; Akar, M.E.; Kammire, L.D.; Johnston-MacAnanny, E.B.; Mertz, H.L. Robotic-assisted laparoscopic repair of symptomatic cesarean scar defect: A report of two cases. J. Reprod. Med. 2011, 56, 265–270. [Google Scholar] [PubMed]
- Armstrong, V.; Hansen, W.F.; Van Voorhis, B.J.; Syrop, C.H. Detection of cesarean scars by transvaginal ultrasound. Obstet. Gynecol. 2003, 101, 61–65. [Google Scholar] [PubMed]
- Wang, C.-B.; Chiu, W.-W.; Lee, C.-Y.; Sun, Y.-L.; Lin, Y.-H.; Tseng, C.-J. Cesarean scar defect: Correlation between Cesarean section number, defect size, clinical symptoms and uterine position. Ultrasound Obstet. Gynecol. 2009, 34, 85–89. [Google Scholar] [CrossRef]
- Florio, P.; Gubbini, G.; Marra, E.; Dores, D.; Nascetti, D.; Bruni, L.; Battista, R.; Moncini, I.; Filippeschi, M.; Petraglia, F. A retrospective case–control study comparing hysteroscopic resection versus hormonal modulation in treating menstrual disorders due to isthmocele. Gynecol. Endocrinol. 2010, 27, 434–438. [Google Scholar] [CrossRef]
- Sauerland, S.; Lefering, R.; Neugebauer, E.A.M. Retrospective clinical studies in surgery: Potentials and pitfalls. J. Hand Surg. 2002, 27, 117–121. [Google Scholar] [CrossRef]
- Kaji, A.H.; Schriger, D.; Green, S. Looking Through the Retrospectoscope: Reducing Bias in Emergency Medicine Chart Review Studies. Ann. Emerg. Med. 2014, 64, 292–298. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Age, years | 38.7 (27–49) |
| Prolonged uterine bleeding | 66 (100%) |
| Dysmenorrhea | 12 (18%) |
| Pelvic pain | 6 (9%) |
| Low back pain | 2 (3%) |
| Mean duration of symptoms (years) | 5.84 (1–17) |
| Number of previous caesarean sections | |
| 1 | 6 (10%) |
| 2 | 40 (60%) |
| 3 | 20 (30%) |
| Duration of operation (min) | 66 (30–215) |
| Blood loss (mL) | 10 (5–50) |
| Mean follow-up (years) | 8.5 (4–15) |
| References | Study Design | Numbers of Patients | Rates of Success (%) | Follow-Up Duration (months) | Pre-Op Bleeding Days | Post-Op Bleeding Days | Mean Operating Time (min) | Operative Blood Loss (mL) | Concept of Operations |
|---|---|---|---|---|---|---|---|---|---|
| Our study | |||||||||
| Overall | Retrospective | 66 | 92.4 | 102 | 15 ± 3.37 | 6.6 ± 2 | 66 | 10 | I, II, III, and IV |
| Unmodified | 12 | 75 | 13.2 ± 2.9 | 7.0 ± 2.0 | (I, not to the cervical outer orifice) | ||||
| Modified | 54 | 98.2 | 15.38 ± 3.3 | 6.29 ± 0.8 | (I, to the cervical outer orifice) | ||||
| Other studies | |||||||||
| [20] | Retrospective | 24 | 84 | 14 to 24 | - | - | - | - | |
| [26] | Prospective | 26 | 100 | 12 to 23 | 2 to 12 | - | - | - | II and III |
| [12] | Retrospective | 57 | 59.6 | 60 | 12.9 ± 2.9 | 9.4 ± 4.1 | 30.2 ± 6.6 | - | II (distal side only) and III |
| [8] | Retrospective | 57 | 66 | 12 | 9.6 | 6.6 to 7.6 | - | - | II (distal side only) and III |
| [19] | Retrospective | 24 | 79 | 3 to 16 | - | - | 23 ± 15 | 11 ± 6 | II and III |
| [21] | Retrospective | 22 | 68 | - | - | - | - | - | II (proximal side only) |
| [24] | Retrospective | 31 | 64.5 | 22.3 | 14 | - | 25 | 10 | III |
| [22] | Prospective | 120 | 80 | 35 | - | - | 8 | - | II (distal side only) |
| [23] | Prospective | 18 | 64 | 12 | - | - | - | - | - |
| [27] | Prospective | 19 | N/A | 21.2 | 11.9 ± 3.1 | 7.9 ± 2.2 | 25 ± 14 | 10.7 ± 16 | II (distal side only) |
| [18] | Prospective | 38 | 96.8 | 2 | - | - | - | - | II (distal side only) III |
| [18] | Prospective | 38 | 87.5 | 2 | - | - | - | - | II and III |
| [1] | Prospective | 23 | 68.8 | 6 | 7 | - | 17.4 ± 3.5 | - | II and III |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-C.; Chiu, S.-C.; Pan, C.-M.; Huang, C.-C.; Chang, C.Y.-Y.; Chao, S.-C.; Cho, D.-Y.; Lin, W.-C. New Efficient Method for Hysteroscopic Isthmoplasty: Four Simple Steps Lead to a Significant Improvement in Bleeding Status. J. Clin. Med. 2022, 11, 6541. https://doi.org/10.3390/jcm11216541
Huang C-C, Chiu S-C, Pan C-M, Huang C-C, Chang CY-Y, Chao S-C, Cho D-Y, Lin W-C. New Efficient Method for Hysteroscopic Isthmoplasty: Four Simple Steps Lead to a Significant Improvement in Bleeding Status. Journal of Clinical Medicine. 2022; 11(21):6541. https://doi.org/10.3390/jcm11216541
Chicago/Turabian StyleHuang, Chien-Chu, Shao-Chih Chiu, Chih-Ming Pan, Chun-Chung Huang, Cherry Yin-Yi Chang, Shih-Chi Chao, Der-Yang Cho, and Wu-Chou Lin. 2022. "New Efficient Method for Hysteroscopic Isthmoplasty: Four Simple Steps Lead to a Significant Improvement in Bleeding Status" Journal of Clinical Medicine 11, no. 21: 6541. https://doi.org/10.3390/jcm11216541
APA StyleHuang, C.-C., Chiu, S.-C., Pan, C.-M., Huang, C.-C., Chang, C. Y.-Y., Chao, S.-C., Cho, D.-Y., & Lin, W.-C. (2022). New Efficient Method for Hysteroscopic Isthmoplasty: Four Simple Steps Lead to a Significant Improvement in Bleeding Status. Journal of Clinical Medicine, 11(21), 6541. https://doi.org/10.3390/jcm11216541