

Intraoral Scanners for In Vivo 3D Imaging of the Gingiva and the Alveolar Process


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
- -
- No extremes of palatal shape and no visible edema in the attached or removable buccal or on the palatal mucosa (visual inspection by two investigators, with disagreements resolved by consensus).
- -
- No extreme malocclusion patterns, no crossbite, and no large asymmetries (visual inspection by two investigators, with disagreements resolved by consensus).
- -
- Participants of European (white) ancestry. This criterion was applied for consistency since this group was over-represented in the place of sample selection.
- -
- Before or more than 2 years after the end of any previous orthodontic treatment.
2.2. Data Acquisition
- 3D scans with CS 3600 (two times)
- 3D scans with TRIOS 3 (two times)
- 3D scan with CS 3600 (one time)
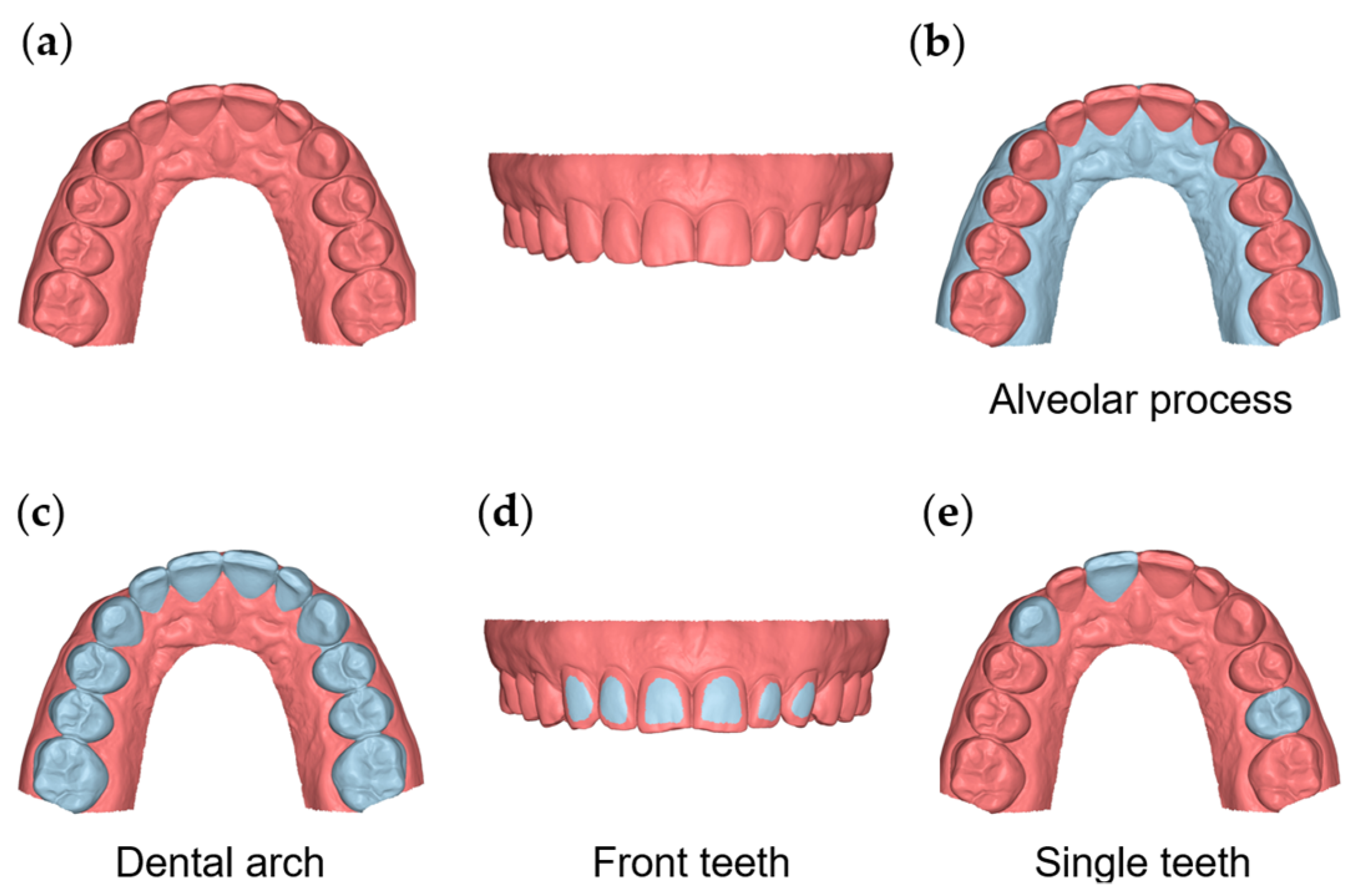
2.3. Assessment of Precision and Agreement between Scanners
2.4. Statistical Analysis
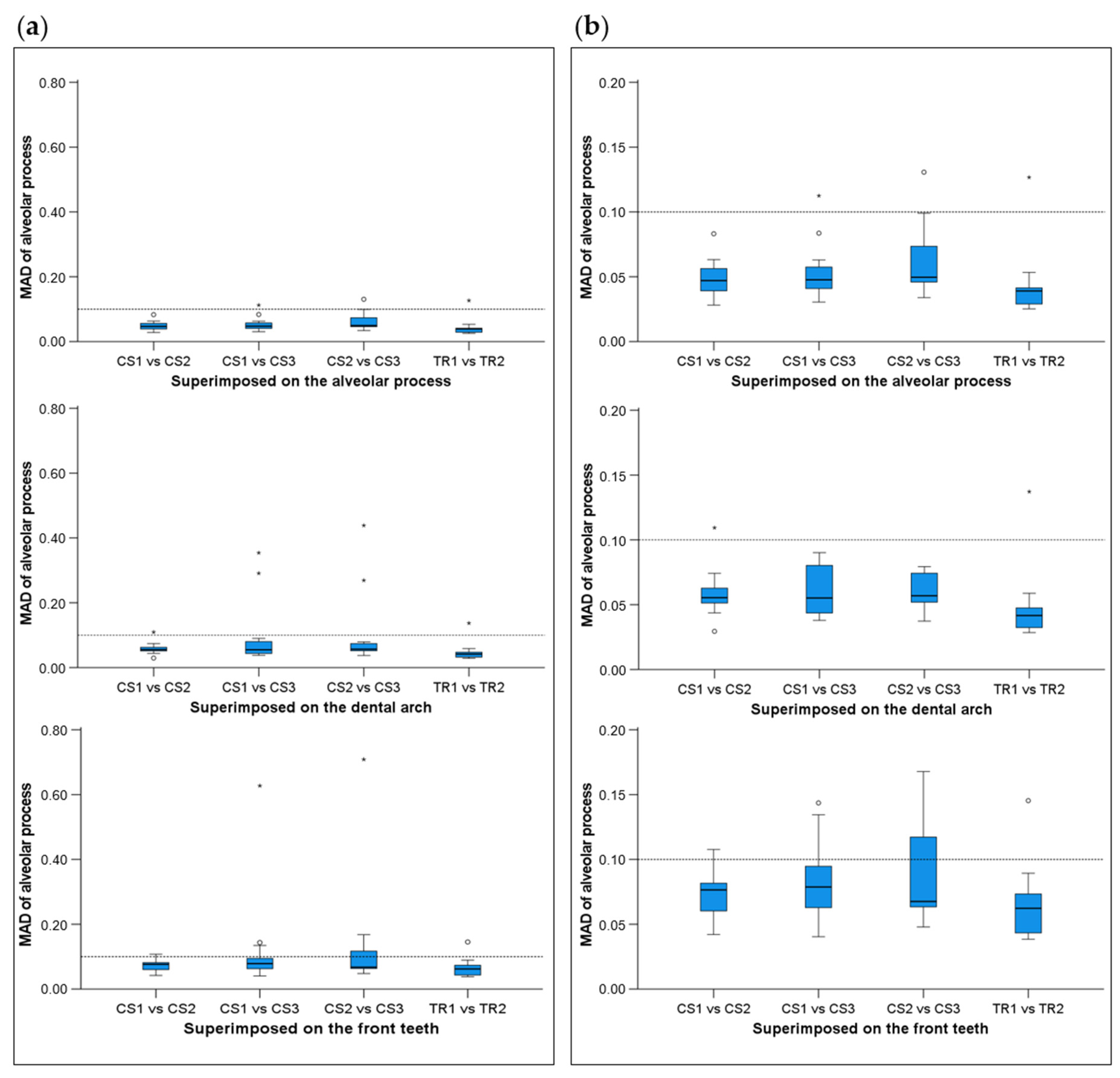
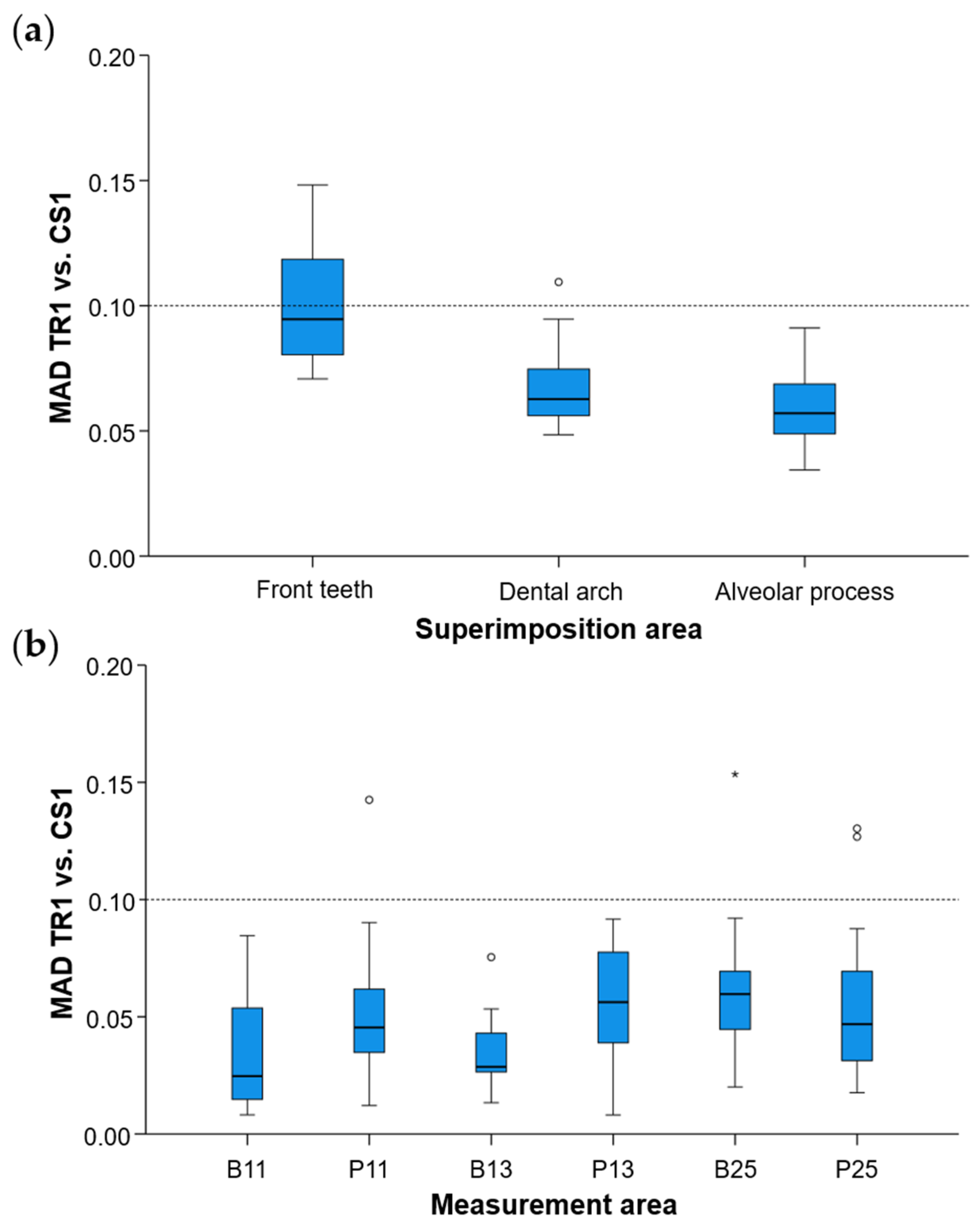
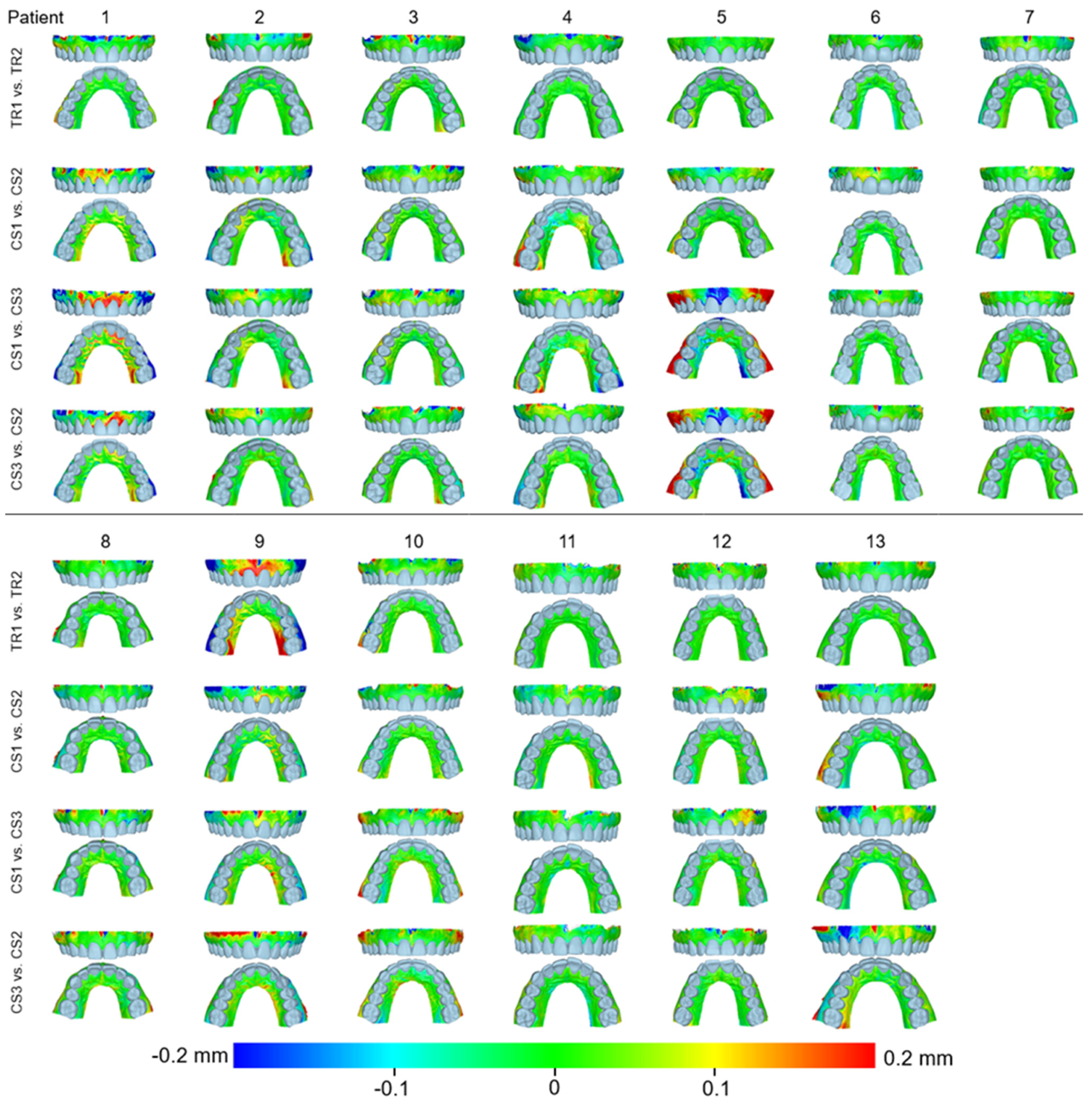
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Helal, O.; Göstemeyer, G.; Krois, J.; Fawzy El Sayed, K.; Graetz, C.; Schwendicke, F. Predictors for Tooth Loss in Periodontitis Patients: Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2019, 46, 699–712. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Christou, P.; Topouzelis, N. The Orthodontic-Periodontic Interrelationship in Integrated Treatment Challenges: A Systematic Review. J. Oral Rehabil. 2010, 37, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Kloukos, D.; Koukos, G.; Gkantidis, N.; Sculean, A.; Katsaros, C.; Stavropoulos, A. Transgingival Probing: A Clinical Gold Standard for Assessing Gingival Thickness. Quintessence Int. 2021, 52, 394–401. [Google Scholar] [CrossRef]
- Kloukos, D.; Koukos, G.; Doulis, I.; Sculean, A.; Stavropoulos, A.; Katsaros, C. Gingival Thickness Assessment at the Mandibular Incisors with Four Methods: A Cross-Sectional Study. J. Periodontol. 2018, 89, 1300–1309. [Google Scholar] [CrossRef] [PubMed]
- Stucki, S.; Gkantidis, N. Assessment of Techniques Used for Superimposition of Maxillary and Mandibular 3D Surface Models to Evaluate Tooth Movement: A Systematic Review. Eur. J. Orthod. 2020, 42, 559–570. [Google Scholar] [CrossRef]
- Winkler, J.; Gkantidis, N. Intraoral Scanners for Capturing the Palate and Its Relation to the Dentition. Sci. Rep. 2021, 11, 15489. [Google Scholar] [CrossRef]
- AlSamak, S.; Gkantidis, N.; Bitsanis, E.; Christou, P. Assessment of Potential Orthodontic Mini-Implant Insertion Sites Based on Anatomical Hard Tissue Parameters: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2012, 27, 875–887. [Google Scholar]
- Tsamis, C.; Rodiou, S.; Stratos, A.; Gkantidis, N. Removal of a Severely Impacted Mandibular Third Molar Minimizing the Risks of Compromised Periodontium, Nerve Injury, and Mandibular Fracture. Quintessence Int. 2018, 49, 41–48. [Google Scholar] [CrossRef]
- Mai, D.D.-P.; Stucki, S.; Gkantidis, N. Assessment of Methods Used for 3-Dimensional Superimposition of Craniofacial Skeletal Structures: A Systematic Review. PeerJ 2020, 8, e9263. [Google Scholar] [CrossRef]
- Kuralt, M.; Selmani Bukleta, M.; Kuhar, M.; Fidler, A. Bone and Soft Tissue Changes Associated with a Removable Partial Denture. A Novel Method with a Fusion of CBCT and Optical 3D Images. Comput. Biol. Med. 2019, 108, 78–84. [Google Scholar] [CrossRef]
- Winkler, J.; Gkantidis, N. Trueness and Precision of Intraoral Scanners in the Maxillary Dental Arch: An in vivo Analysis. Sci. Rep. 2020, 10, 1172. [Google Scholar] [CrossRef]
- Gkantidis, N.; Dritsas, K.; Katsaros, C.; Halazonetis, D.; Ren, Y. 3D Method for Occlusal Tooth Wear Assessment in Presence of Substantial Changes on Other Tooth Surfaces. J. Clin. Med. 2020, 9, E3937. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Dritsas, K.; Ren, Y.; Halazonetis, D.; Katsaros, C. An Accurate and Efficient Method for Occlusal Tooth Wear Assessment Using 3D Digital Dental Models. Sci. Rep. 2020, 10, 10103. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Dritsas, K.; Katsaros, C.; Halazonetis, D.; Ren, Y. 3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces. Diagnostics 2021, 11, 1033. [Google Scholar] [CrossRef] [PubMed]
- Vasilakos, G.; Schilling, R.; Halazonetis, D.; Gkantidis, N. Assessment of Different Techniques for 3D Superimposition of Serial Digital Maxillary Dental Casts on Palatal Structures. Sci. Rep. 2017, 7, 5838. [Google Scholar] [CrossRef] [PubMed]
- Goujat, A.; Abouelleil, H.; Colon, P.; Jeannin, C.; Pradelle, N.; Seux, D.; Grosgogeat, B. Marginal and Internal Fit of CAD-CAM Inlay/Onlay Restorations: A Systematic Review of In Vitro Studies. J. Prosthet. Dent. 2019, 121, 590–597.e3. [Google Scholar] [CrossRef]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Rydén, J.; Thor, A. Accuracy and Precision of 3 Intraoral Scanners and Accuracy of Conventional Impressions: A Novel in Vivo Analysis Method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In Vivo Precision of Conventional and Digital Methods for Obtaining Quadrant Dental Impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef]
- Kuralt, M.; Fidler, A. Assessment of Reference Areas for Superimposition of Serial 3D Models of Patients with Advanced Periodontitis for Volumetric Soft Tissue Evaluation. J. Clin. Periodontol. 2021, 48, 765–773. [Google Scholar] [CrossRef]
- Kuralt, M.; Fidler, A. A Novel Computer-Aided Method for Direct Measurements and Visualization of Gingival Margin Changes. J. Clin. Periodontol. 2022, 49, 153–163. [Google Scholar] [CrossRef]
- Wei, D.; Di, P.; Tian, J.; Zhao, Y.; Lin, Y. Evaluation of Intraoral Digital Impressions for Obtaining Gingival Contour in the Esthetic Zone: Accuracy Outcomes. Clin. Oral Investig. 2020, 24, 1401–1410. [Google Scholar] [CrossRef] [PubMed]
- Kanavakis, G.; Ghamri, M.; Gkantidis, N. Novel Anterior Cranial Base Area for Voxel-Based Superimposition of Craniofacial CBCTs. J. Clin. Med. 2022, 11, 3536. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.-C.; Lee, J.; Kang, D.-Y.; Cho, I.-W.; Shin, H.-S.; Park, J.-C. Digital Assessment of Gingival Dimensions of Healthy Periodontium. J. Clin. Med. 2021, 10, 1550. [Google Scholar] [CrossRef] [PubMed]
- Besl, P.J.; McKay, N.D. A Method for Registration of 3-D Shapes. IEEE Trans. Pattern Anal. Mach. Intell. 1992, 14, 239–256. [Google Scholar] [CrossRef]
- Schimmel, M.; Akino, N.; Srinivasan, M.; Wittneben, J.-G.; Yilmaz, B.; Abou-Ayash, S. Accuracy of Intraoral Scanning in Completely and Partially Edentulous Maxillary and Mandibular Jaws: An in Vitro Analysis. Clin. Oral Investig. 2021, 25, 1839–1847. [Google Scholar] [CrossRef]
- Tavelli, L.; Barootchi, S.; Majzoub, J.; Siqueira, R.; Mendonça, G.; Wang, H.-L. Volumetric Changes at Implant Sites: A Systematic Appraisal of Traditional Methods and Optical Scanning-Based Digital Technologies. J. Clin. Periodontol. 2021, 48, 315–334. [Google Scholar] [CrossRef]
- Häner, S.T.; Kanavakis, G.; Matthey, F.; Gkantidis, N. Voxel-Based Superimposition of Serial Craniofacial CBCTs: Reliability, Reproducibility and Segmentation Effect on Hard-Tissue Outcomes. Orthod. Craniofac. Res. 2020, 23, 92–101. [Google Scholar] [CrossRef]
- Kanavakis, G.; Häner, S.T.; Matthey, F.; Gkantidis, N. Voxel-Based Superimposition of Serial Craniofacial Cone-Beam Computed Tomographies for Facial Soft Tissue Assessment: Reproducibility and Segmentation Effects. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 343–351.e1. [Google Scholar] [CrossRef]
- Mennito, A.S.; Evans, Z.P.; Nash, J.; Bocklet, C.; Lauer Kelly, A.; Bacro, T.; Cayouette, M.; Ludlow, M.; Renne, W.G. Evaluation of the Trueness and Precision of Complete Arch Digital Impressions on a Human Maxilla Using Seven Different Intraoral Digital Impression Systems and a Laboratory Scanner. J. Esthet. Restor. Dent. 2019, 31, 369–377. [Google Scholar] [CrossRef]
- Rihani, A. Pressures Involved in Making Upper Edentulous Impressions. J. Prosthet. Dent. 1981, 46, 610–614. [Google Scholar] [CrossRef]
- Gkantidis, N.; Dritsas, K.; Gebistorf, M.; Halazonetis, D.; Ren, Y.; Katsaros, C. Longitudinal 3D Study of Anterior Tooth Wear from Adolescence to Adulthood in Modern Humans. Biology 2021, 10, 660. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-S.; Jeon, Y.-S.; Strauss, F.-J.; Jung, H.-I.; Gruber, R. Digital Scanning Is More Accurate than Using a Periodontal Probe to Measure the Keratinized Tissue Width. Sci. Rep. 2020, 10, 3665. [Google Scholar] [CrossRef]
- Marques, T.; Santos, N.M.; Fialho, J.; Montero, J.; Correia, A. A New Digital Evaluation Protocol Applied in a Retrospective Analysis of Periodontal Plastic Surgery of Gingival Recessions. Sci. Rep. 2021, 11, 20399. [Google Scholar] [CrossRef] [PubMed]
- Couso-Queiruga, E.; Tattan, M.; Ahmad, U.; Barwacz, C.; Gonzalez-Martin, O.; Avila-Ortiz, G. Assessment of Gingival Thickness Using Digital File Superimposition versus Direct Clinical Measurements. Clin. Oral Investig. 2021, 25, 2353–2361. [Google Scholar] [CrossRef] [PubMed]
- Probst, J.; Dritsas, K.; Halazonetis, D.; Ren, Y.; Katsaros, C.; Gkantidis, N. Precision of a Hand-Held 3D Surface Scanner in Dry and Wet Skeletal Surfaces: An Ex Vivo Study. Diagnostics 2022, 12, 2251. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winkler, J.; Sculean, A.; Gkantidis, N. Intraoral Scanners for In Vivo 3D Imaging of the Gingiva and the Alveolar Process. J. Clin. Med. 2022, 11, 6389. https://doi.org/10.3390/jcm11216389
Winkler J, Sculean A, Gkantidis N. Intraoral Scanners for In Vivo 3D Imaging of the Gingiva and the Alveolar Process. Journal of Clinical Medicine. 2022; 11(21):6389. https://doi.org/10.3390/jcm11216389
Chicago/Turabian StyleWinkler, Jonas, Anton Sculean, and Nikolaos Gkantidis. 2022. "Intraoral Scanners for In Vivo 3D Imaging of the Gingiva and the Alveolar Process" Journal of Clinical Medicine 11, no. 21: 6389. https://doi.org/10.3390/jcm11216389
APA StyleWinkler, J., Sculean, A., & Gkantidis, N. (2022). Intraoral Scanners for In Vivo 3D Imaging of the Gingiva and the Alveolar Process. Journal of Clinical Medicine, 11(21), 6389. https://doi.org/10.3390/jcm11216389