Abstract
Both surgical and non-surgical techniques are employed for implant site development. However, the efficacy of these methods has not been thoroughly evaluated and compared. This systematic review aims to compare the biologic, functional and esthetic outcomes of three different approaches before implant placement in both the maxillary and mandibular arches: orthodontic extrusion, regenerative surgery and spontaneous healing after extraction. The systematic research of articles was conducted up to January 2020 in Medline, Scopus and the Cochrane Library databases. Studies were selected in a three-stage process according to the title, the abstract and the inclusion criteria. The methodological quality and the risk of bias of the included studies were evaluated using ROBINS-I tools for non-randomized studies, Rob 2.0 for RCT. Quality evaluation of case reports was performed using CARE guidelines. Through the digital search, 1607 articles were identified, and 25 of them were included in the systematic review. The qualitative evaluation showed a good methodological quality for RCT, sufficient for non-randomized studies and poor for case reports. Based on the available results, both orthodontic extrusion and regenerative surgery allowed the development of the implant site with satisfying esthetic and functional outcomes. Studies about the spontaneous healing of the extraction socket showed resorption of the edentulous ridge, which complicated the implant insertion. No study referred to failures or severe complications. Most of the studies reported only qualitative results. The present systematic review demonstrated that there is a substantial lack of data and evidence to determine which of the presented methods is better for developing a future implant site. Both surgical and non-surgical procedures appear effective in the regeneration of hard tissue, whereas not all the techniques can improve soft tissue volume, too. The orthodontic technique simultaneously enhances both hard and soft tissue.
1. Introduction
The replacement of missing teeth using implants has become a routine practice in dentistry; the quality and quantity of alveolar bone and soft tissue in the future implant site are essential for proper tridimensional implant placement to achieve both esthetic and functional outcomes.
Because of the progressive vertical and horizontal resorption of the alveolar bone following tooth loss, it is often necessary to perform some pre, peri or post-implant tissue management to ensure a good esthetic, functional and predictable long-term result for the prosthetic rehabilitation [1,2].
Several surgical techniques have been employed to develop the implant site, including bone and soft tissue grafting, guided bone regeneration (GBR), distraction osteogenesis and ridge splitting [3,4,5,6,7,8,9,10,11,12,13,14,15].
For large defects, autogenous bone blocks remain the ‘gold standard’. Ideally, the autograft is taken from an intraoral site, either the ramus or symphysis. Selection depends on the defect morphology, location of the recipient site, available bone and the position of vital structures. The ramus is often preferable; however, the presence of third molars, lack of width between the lingual wall and the external oblique ridge, or reduced bone height above the inferior dental canal may prohibit its use [16,17,18].
Symphyseal donor sites are selected according to bone availability between the inferior border of the mandible and the apices of the lower incisors and canines. A minimum safe distance of 5 mm should be left to avoid injury to these teeth. If the amount of bone needed exceeds what is available intraorally, then extraoral sites can be considered, such as the iliac crest and calvarium [16].
Autogenous bone is the ideal biomaterial. As it is a genetic match, there are no issues with biocompatibility, carcinogenicity, disease transmission, or religious or ethical objections. Compared with the other graft materials, it is more resistant to infections and has a shorter healing time. However, its single most important and unique property is its osteogenicity [16]. While other graft materials merely act as a scaffold, into which the host bone eventually grows and substitutes, an autograft will stimulate bone apposition.
A complicating factor in the use of autologous grafts is the need for a donor site with its associated morbidity. As an alternative to this type of grafting, allogenic, xenographic and alloplastic materials have been developed. However, none guarantees the healing and bone replacement that autogenous block grafts can provide [18].
Techniques such as guided bone regeneration (GBR), ridge expansion and distraction osteogenesis have the advantage of removing the need for a donor site with its associated morbidity.
Guided bone regeneration (GBR) with particulate deproteinized bovine bone mineral (DBBM) and covered with resorbable collagen membranes is currently the best documented and most widely used method to augment peri-implant alveolar bone defects [19,20]. The major drawbacks of particulate bone grafting material and collagen membrane are their poor mechanical properties, which is a key issue in hard tissue regeneration, and their low resistance to tissue collapse. Limited evidence is available regarding the hard tissue volume stability of sites that are augmented by GBR, especially at the buccal–coronal region in the anterior maxilla area, where the tissue contour is esthetically significant.
The ridge-splitting technique can increase the width of bone by splitting and expanding the existing residual ridge. Indications of this technique include the ridge deficient in width with an adequate amount of height, with no vertical defects [21]. The maxilla is preferred over the mandible because bone expansion is easily achieved without complications, thanks to the bone’s cancellous nature. Advantages include no second surgery required to place implants, reduced overall treatment time and increased implant stability because of new bone formation between cortical plates. Disadvantages include more severe ridge defects in the case of procedure failure and primary closure being difficult to achieve.
Distraction osteogenesis is based on the principle of secondary wound healing. Osteotomy removes a bone segment from the basal bone, filling the distraction gap with a callus forming a new bone segment. This procedure demonstrates many advantages, such as decreased bone resorption, no donor site morbidity and simultaneous lengthening of the surrounding soft tissues. Therefore, there are also disadvantages, such as the risk of fracture of the mandible, fracture of the transport segment, difficulties in finishing the osteotomy on the lingual side, incorrect direction of distraction, perforation of the mucosa by the transport segment, suture dehiscence, bone formation defects and pain during the activation of the distraction device [22,23,24].
To correct gingival deficiencies at potential implant sites, conventional mucogingival surgical procedures, such as connective tissue grafts, free gingival grafts and coronally positioned flaps, are the most commonly used treatment modalities [3].
Currently, orthodontic extrusion, or forced eruption, is the only non-surgical procedure for pre-implant tissue management. This is a non-invasive technique based on the periodontum ability to respond to tooth movement. Salama and Salama, in 1993, suggested using orthodontic extrusion to create vertical bone and soft tissue at hopeless tooth sites before extraction and implant placement, without the use of surgery [4].
A basic tenet of osteophysiology is that the fibers of the periodontal membrane are secured to the bone by the formation of new bone around the ends of the fibers. Bone is in a constant state of transition. As elsewhere in the body, the bone of the alveolus is constantly being resorbed and rebuilt. Therefore, when tension is applied to the periodontal ligament, periodontal fibers bundles are elongated, and osteoblasts are induced to deposit new bone in the areas where periodontal attachment exists.
The same effects on alveolar bone height are seen when orthodontic treatment is carried out with controlled and low forces which do not tear apart the periodontal fibers. In other words, a tooth moved into the dental arch by controlled extrusive orthodontic forces will bring alveolar bone, and soft tissues will follow, too [5,6].
Orthodontic extrusion is an excellent way of using teeth that are hopeless but not useless: the advantage that these teeth offer resides in their remaining attachment apparatus. This orthodontic technique manipulates the remaining attachment to augment the gingival and osseous tissues in a vertical direction. The most important benefits are the creation of a greater volume of available bone to engage the future implant and the enhancement of soft tissue volume to achieve esthetic outcomes.
Both surgical and non-surgical techniques have been employed for implant site development. However, the efficacy of these methods has not been thoroughly evaluated and compared. Therefore, deciding which approach to use is sometimes difficult and often based on personal preference instead of scientific evidence.
The aim of this systematic review is to compare the biological, functional and esthetic outcomes of orthodontic extrusion and regenerative surgery prior to implant placement in both maxillary and mandibular arch, having the case of no type of treatment of the edentulous ridge before a delayed implant placement as a control group and point of reference. The authors have identified and compared studies that examined these three different approaches.
2. Materials and Methods
2.1. Search Strategy and Study Selection
The systematic research of articles was conducted up to January 2020. The digital research was performed in the following databases: Medline, Scopus and the Cochrane Library. The following limits were activated for the search: Human, English. The search strategy was assembled with a combination of Medical Subjects Headings (MESH terms) and free-text words, as reported below:
((“orthodontic extrusion” [Mesh] OR “orthodontic extraction” OR “orthodontic eruption” OR “forced eruption” OR “OISD” OR “OFE” OR “bone graft” OR “GBR” OR “tissue regeneration” OR “bone regeneration” OR “distraction”) AND (“implant site development” OR “enhancement hard tissue” OR “enhancement soft tissue” OR “implant site regeneration” OR “implant site enhancement”)) OR ((“ bone healing” OR “extraction wound repair” OR “healing extraction socket”) AND (“delayed implant”)).
Once the research was completed, studies were selected in a three-stage process. In the first stage, the reviewers screened the databases, read the article titles, and removed any duplicate studies that did not fit the purpose of the systematic review.
In the second stage, abstracts of all titles approved were downloaded and evaluated; if the abstract met the inclusion criteria, the full text was obtained. When neither the title nor the abstract contained sufficient information for the evaluation, the full text was obtained in any case, to avoid excluding any relevant article. In the last stage, after the collection of all full texts, the inclusion criteria were used to identify the studies that would have been used for the systematic review.
The reviewers performed each phase of this selection process independently, and any disagreement was resolved through discussion. All reviewers agreed on the final selection of the articles.
2.2. Inclusion Criteria
- Human studies;
- English language;
- Type of studies: case reports, case series, randomized controlled trials, prospective studies;
- Population (P): subjects needing ridge regenerative procedures prior to implant rehabilitation;
- Intervention (I): implant site development through orthodontic extrusion or regenerative surgery (ridge splitting, guided bone regeneration, distraction osteogenesis, bone and soft tissue grafting);
- Control (C): spontaneous bone healing after tooth loss and delayed implant placement;
- Outcome (O): primary outcome was changes in the amount of bone and soft tissue in the implant site.
2.3. Secondary Outcome
- Esthetic outcome;
- Implant survival rate;
- Complications.
2.4. Data Extraction
Data regarding the following parameters were extracted:
- Type of study;
- Year;
- Author;
- Patient age;
- Patient gender;
- Health conditions and smoking habit;
- Treated teeth;
- Reason for treatment need;
- Type of treatment (orthodontic, surgical, absent);
- Orthodontic technique: type of appliance, extrusion method, the intensity of the force, anchorage, extrusion ratio (mm/month), duration of the orthodontic treatment (months), frequency of follow-up (weeks), post-orthodontic retention (months), amount of tooth extrusion (mm), amount of bone augmentation (mm), amount of soft tissue augmentation (mm), efficacy of orthodontic extrusion in hard and soft tissue regeneration (%);
- Regenerative surgery: type of treatment (GTR, GBR, bone graft, distraction osteogenesis, ridge-splitting), materials and membranes used, and type of defects;
- Hard tissue changes;
- Soft tissue changes;
- Timing of implant placement;
- Type of implant;
- Treatment outcomes;
- Complications;
- Follow-up data;
- Implant survival rate.
2.5. Methodological Quality and Risk of Bias Evaluation
The methodological quality and the risk of bias of randomized and non-randomized studies were evaluated using specific tools designed by the Cochrane Library:
- ROBINS-I tools for non-randomized studies (Prospective studies, Case series);
- Rob 2.0 for Randomized Controlled Trials (RCT).
Quality evaluation of case reports was performed using CARE guidelines instead. Case report guidelines consist of a list of 13 key clinical components that should be present in a well-performed case report.
The reviewers decided to use this list to evaluate the studies. Each key component was given a score; to estimate the quality of each case report, the reviewers read the article evaluating the respect of these key components. For every component, the reviewers gave a score. Finally, all the points were added to obtain the final score of the study.
Four arbitrary numeric ranges were decided to give a qualitative description of the quality of case reports (excellent, good, sufficient or poor) (Figure 1).
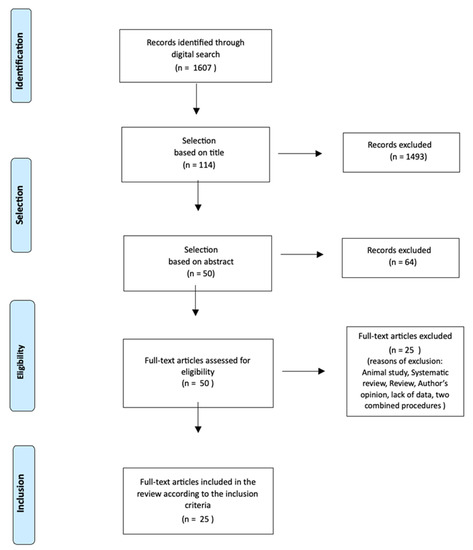
Figure 1.
Study flow chart.
3. Results
3.1. Characteristics of the Included Studies
In total, 25 studies were included in the review: 11 studies about orthodontic extrusion, 9 studies about regenerative procedures and 5 studies about spontaneous healing of the extraction socket and delayed implant placement.
Eleven studies (9 case reports and 2 case series) reported on orthodontic extrusion and nine studies (5 case reports, 3 case series and 1 RCT) reported on regenerative procedures for implant site development.
Five studies (4 RCT and 1 prospective study) reported on spontaneous healing of the extraction socket and delayed implant placement (Table 1).

Table 1.
Studies included in the systematic review. NR, not reported.
The studies were conducted in a private office or in a university setting.
In total, 27 patients were treated by orthodontic extrusion, 103 patients received regenerative procedures and 204 patients were included in the studies comparing spontaneous tissue healing after extraction with ridge preservation procedures.
3.2. Characteristics of the Participants
The age of patients treated with orthodontic extrusion ranged from 23 to 62 years. The two case series [5,11] reporting on orthodontic implant site development did not include any data on patients’ age.
The age of patients undergoing regenerative procedures ranged from 18 to 68 years. One case series [24] did not report any information about the patients’ age.
The age of patients included in the randomized studies comparing ridge preservation procedures with spontaneous healing after tooth loss ranged from 20 to 76 years.
In total, 16 patients (59.3%) treated with orthodontic extrusion were women, while only 6 (22.2%) were men; one study [5] did not report on patient sex.
In total, 47 patients (45.6%) treated with regenerative procedures were men, while 46 (44.6%) were women; one study [24] did not report on patient sex.
In total, 77 patients (37.2%) included in the studies comparing spontaneous tissue healing after extraction with ridge preservation procedures were men, while 127 (62.3%) were women (Table 2, Table 3 and Table 4).
Regarding the health of patients treated with orthodontic extrusion, it was reported that 17 patients were healthy, whereas there was no information about the remaining 10 patients’ health conditions.
In total, 91 of the patients treated with regenerative procedures were healthy, 1 patient had high blood pressure and 1 patient was asthmatic; there was no information about the health of the remaining 10 patients.
All the 204 patients included in the randomized studies comparing ridge preservation procedures with spontaneous healing after tooth loss were healthy.
The information provided about the smoking habit of most of the patients treated with orthodontic extrusion was insufficient. Regarding the patients treated with regenerative procedures, both smokers and nonsmokers were included in the studies, but not all studies provided enough information about that aspect.
Patients included in the randomized studies comparing ridge preservation procedures with spontaneous healing after tooth loss were smokers and nonsmokers; only one study [22] did not provide any information about patients smoking habit.
All teeth extruded orthodontically were identified concerning the location: 40 maxillary incisors, 3 maxillary canines, 5 maxillary premolars, 2 maxillary first molars, 4 mandibular incisors, and 1 mandibular first molar.
In the regenerative procedures, most treated teeth were maxillary incisors; two studies [18,19] reported regenerative procedures in the mandibular right posterior region and one study [24] in different mandibular areas, according to the patients’ need.
In the studies comparing spontaneous tissue healing after extraction with ridge preservation procedures, tooth extractions were performed both in maxillary and mandibular arches and in different areas, according to each patient’s need.
The most common reason for the extraction of teeth treated with orthodontic extrusion was severe periodontitis, followed by non-restorable tooth. The reasons for extraction in those patients treated with regenerative procedures were different: periodontitis, non-restorable teeth, fractures, endodontic complications, trauma; three studies [15,24,25] did not provide details regarding the reasons of tooth loss.
In the randomized studies comparing spontaneous tissue healing after extraction with ridge preservation procedures, no details were given about the reason for the extractions.
In the orthodontic extrusion group of studies, information about the type of bone defect affecting the tooth to be extruded was provided in just one case series [11], whereas the other studies only referred to the presence of horizontal and/or vertical defects due to periodontitis.
Most studies about regenerative procedures gave generic information about bone defects, just referring to the presence of severe alveolar bone defects; one study [16] provided the type of defect (Cadwood and Howell class V defect).
In the studies comparing spontaneous tissue healing after extraction with ridge preservation procedures, no details were given about bone defects.
3.3. Types of Treatment
3.3.1. Orthodontic Implant Site Development
Regarding the orthodontic implant site development, the most used appliance to perform orthodontic extrusion was a multi-bracket system; in only one study [9], a removable appliance was used. The multi-bracket approach was full bimaxillary in three studies [14,29,30] and partial in seven studies [5,7,8,10,11,12,13].
In one study [8], a lingual appliance was used; in another study [13], ceramic brackets were used (Table 2).
Different ways were employed to apply the extrusive force: three studies [8,13,29] used NiTi archwires and a more apical bonding of brackets on the teeth to be extruded; one study [9] used elastic bands from orthodontic hooks bonded to the cervical region of teeth to be extruded and a removable appliance; one study [14] first used NiTi archwires and a more apical bonding of brackets, then an SS archwire with extrusion steps and intermaxillary elastics; three studies [10,11,12] used SS archwires and extrusion steps; one study [7] used a Co-Cr archwire with extrusion steps, L-loops and inset component for palatal movement; and one study [30] used an SS archwire with L-shape loops.
A low extrusive force (<100 g) was applied in all studies, but five studies [5,8,12,29,30] did not report data about the intensity of the force used to perform the extrusion. Regarding the extrusion ratio, the extrusion was performed slowly (mean of 1 mm/month) in six studies [7,8,9,10,11,30], whereas the other five studies did not report any data.
Just two studies [7,11] reported the amount of tooth extrusion performed.
Most of the studies used an SS archwire as an anchorage during the extrusion; one study [9] used a removable appliance and one study [8] used a composite resin veneer pontic, while three studies did not report information about the anchorage used.
The frequency of follow-up varied from 2 to 4 weeks in all studies.
In all studies but one [14], a stabilization period followed the orthodontic extrusion. The retention period lasted from 1.5 to 6 months, depending on each study.
Tooth extraction was followed by immediate post-extractive implant placement in all studies, except two [9,12], where a delayed implant placement was performed 4–6 weeks after extraction.
All studies but one [5] gave details about the type of implants used.
Eight studies performed a follow-up from a minimum of 6 months [10] to a maximum of 6 years [29]; three studies [5,8,12] did not report information about the duration of follow-up. No complications emerged in all studies except two: in one study [11], one implant failed and gingival recessions (0.1–0.2 mm) were observed, whereas in another study [9], external root resorption and an interdental papillae deficiency were observed.
Table 2.
Studies on orthodontic implant site development. NR: Not reported.
Two studies [7,11] only reported the implant survival rate (100% and 96% respectively).
All studies referred to good treatment outcomes, with satisfying esthetic and biological results and a successful implant osteointegration, but only a few [5,7,11,12,30] gave quantitative data about the amount of bone and/or soft tissue augmentation and only one study [11] indicated the percentage of efficacy of the technique in the regeneration of bone and soft tissue in the future implant site (70% and 65%, respectively).
3.3.2. Regenerative Procedures for Implant Site Development
For implant site development, different regenerative procedures were used: four studies [15,17,19,20] performed a guided bone regeneration (GBR), in particular, two studies [15,19] used a one-stage GBR (implant placement and simultaneous bone regeneration), one study [20] used a two-stage GBR (bone regeneration and delayed implant placement in the regenerated bone) and another study [17] divided the patients in two groups and used both types of GBR, one-stage GBR in one group and two-stage GBR in the other one; three studies [16,18,25] performed a bone graft procedure, in particular, one study [18] used an allogenic block graft, whereas the other two studies [16,25] used autogenous bone grafts from an intra-oral site; finally two studies [24,27] performed an alveolar distraction osteogenesis (Table 3).
All studies gave information about the materials used for the regenerative procedures: for GBR procedures, one study [15] used a deproteinized bovine bone mineral (Bio-Oss), one study [17] used a freeze-dried mineralized bone allograft, and the other two studies [19,20] used demineralized freeze-dried bone particles (Dembone); for bone grafting, one study [18] used a Puros block allograft rehydrated with platelet-rich plasma and additional Puros particulate mineralized bone graft material, and the other two studies used autogenous bone grafts from symphysis [25] and from retromolar area [16]; and the studies [24,27] performing alveolar distraction osteogenesis used the same type of distraction device (Modus distractor, Medartis).
All studies performing GBR or bone graft procedures used barrier membranes: three studies [15,16,18] used resorbable membranes and the other four studies [17,19,20,25] used non-resorbable membranes.
Regarding the timing of implant placement, two studies [15,19] performed a regenerative procedure with simultaneous implant placement, two studies [17,25] performed a regenerative procedure with simultaneous or delayed implant placement, depending on each patient’s clinical condition, and five studies [16,18,20,24,27] performed a regenerative procedure with delayed implant placement in the regenerated bone.
All studies except two [16,20] gave details about the type of implants used.
The follow-up period ranged from a minimum of 6 months [15] to a maximum of 3 years [16,24,25], depending on each study.
All studies reported good outcomes, with an enhancement of hard tissue, but none of them gave quantitative data about the amount of regenerated bone. Regarding soft tissue changes, no study reported data, except one [24], using an alveolar distraction osteogenesis procedure which referred to a simultaneous lengthening of soft tissues surrounding the distracted bone segment.
Table 3.
Studies on regenerative surgery procedures for implant site development.
Only three studies [17,24,25] indicated the implant survival rate (100%, 97.3% and 97.1%, respectively).
Only three studies [20,24,25] reported complications: one study [24] using alveolar distraction osteogenesis referred to a lingual inclination of the distracted bone segment occurred during distraction in one patient and a post-operative infection in another patient; one study [20] using a GBR technique reported an early exposure of the e-PTFE membrane; finally, one study [25] using an onlay bone graft from the mandibular symphysis reported four cases of paresthesia at the donor site immediately following the graft surgery.
3.3.3. Spontaneous Healing of the Extraction Socket and Delayed Implant Placement
Regarding the delayed implant placement in an untreated edentulous ridge, five studies were included in the systematic review: one prospective study [21] analyzed the spontaneous healing of the extraction socket and a delayed implant placement; the other four randomized controlled studies [22,23,26,28] compared extraction alone with ridge preservation procedures before delayed implant placement (Table 4).
Table 4.
Studies on spontaneous healing of the extraction socket and delayed implant placement.
In the prospective study [21], no ridge preservation procedure was performed after tooth extraction, but the extraction was as atraumatic as possible, and the granulation tissue was left in situ to help the healing process. Implants were placed three months after tooth extraction.
In the RCT studies ridge preservation procedures were performed after tooth extraction to limit the resorption of hard and soft tissues: one study [22] used a freeze-dried bone allograft and a collagen membrane; one study [23] used a xenograft; one study [26] used a cortical or collagenated corticocancellous porcine bone graft; finally, one study [28] used a corticocancellous porcine bone graft and a collagen membrane, which remained exposed in the oral environment for an intentional secondary soft tissue healing. A delayed implant placement followed all these ridge preservation procedures: in one study [26], implants were inserted 3 months after tooth extraction; in two studies [22,28] implants were placed 4 months after extraction; and in another study [23], implants were inserted 7 months after tooth extraction.
Two studies [21,26] only reported data about the type of implants used.
The follow-up period was different: in three studies [22,23,28], it was 6, 7, and 8 months long, respectively, 3 years in the prospective study [21], and 4 years in another randomized study [26].
Regarding complications, only one study [22] reported the presence of little dehiscences at the time of implant placement in the group of patients treated with ridge preservation procedures. The other studies reported no complications.
All studies reported data about hard tissue changes. In the prospective study [21], no statistically significant differences were found in the ridge width before the extraction and 3 years after implant placement (11.44 ± 1.80 mm and 11.59 ± 1.61 mm, respectively), whereas the vertical ridge dimension showed a statistically significant increase (from 8.05 ± 2.12 mm to 12.48 ± 2.04 mm). The RCT studies showed that all ridge preservation procedures limited the horizontal and vertical resorption of hard tissue after tooth extraction, compared to extraction alone. In one study [22], the ridge width decreased from 9.2 ± 1.2 mm to 8.0 ± 1.4 mm in the group treated with ridge preservation procedures (RP), while it decreased from 9.1 ± 1.0 mm to 6.4 ± 2.2 mm in the extraction-alone (EXT) group, a difference of 1.6 mm. Most of resorption occurred from the buccal. The vertical change for the RP group was a gain of 1.3 ± 2.0 mm versus a loss of 0.9 ± 1.6 mm for the EXT group. Histologic analysis revealed more bone in the RP group.
In another study [23], a significantly greater horizontal resorption was observed at EXT sites (4.3 ± 0.8 mm) compared to RP sites (2.5 ± 1.2 mm). The ridge height reduction at the buccal side was 3.6 ± 1.5 mm for the EXT group, whereas it was 0.7 ± 1.4 mm for the RP group. Moreover, the vertical change at the lingual sites was 0.4 mm in the RP group and 3 mm in the EXT group. The histologic analysis showed a significantly higher percentage of trabecular bone and total mineralized tissue in ridge-preservation sites compared to extraction-alone sites.
One study [28] reported that in the grafted group changes in horizontal dimension showed an average resorption of 1.6 ± 0.55 mm. Vertical bone resorption was 0.3 ± 0.76 mm, 1.1 ± 0.96 mm, 0.3 ± 0.85 mm, 0.9 ± 0.98 mm at the mesial, buccal, distal and lingual sites, respectively. In the non-grafted group, horizontal bone resorption was significantly higher (3.6 ± 0.72 mm). Vertical measurements indicated an average resorption of 1 ± 0.7 mm, 2.1 ± 0.6 mm, 1 ± 0.8 mm and 2 ± 0.73 mm respectively, at the mesial, buccal, distal and lingual sites.
Finally, another study [26] reported that there were no differences regarding marginal bone change between the collagenated (COLL) and the cortical (CORT) corticocancellous porcine bone groups. Both grafts seemed to preserve the peri-implant marginal bone better than the natural healing. The total amount of marginal bone loss from T0 to T4-year was 1.14 ± 0.23 mm in the CORT group, 1.13 ± 0.29 mm in the COLL group and 1.92 ± 0.07 mm in the EXT group.
Regarding soft tissue changes, two studies [21,23] did not report data, and one study [22] reported a gain in soft tissue thickness in the group of patients treated with extraction alone and a loss of thickness in the group of patients treated with ridge preservation procedures; the other two studies [26,28] reported a better-preserved width of keratinized gingiva in the groups of patients subjected to ridge preservation procedures.
Only two studies [21,26] reported the implant survival rate (100% both).
3.4. Methodological Quality and Risk of Bias Evaluation
Regarding the methodological quality of studies included in the review, different tools were used to perform the evaluation. For randomized studies [15,22,23,26,28] (RCT), Rob 2.0 tool was used: all studies had good quality and a low risk of bias (Table 5).
Table 5.
Risk of bias for the included randomized clinical trials (RCT) using Rob 2.0 tool.
For non-randomized studies [11,17,21,24,25] (case series and prospective study) ROBINS-I tool was used: two studies [11,24] only had a low risk of bias, whereas the other three studies [17,21,25] had a moderate risk of bias (Table 6).
Table 6.
Risk of bias for the included non-randomized studies using ROBINS-I tool.
For the evaluation of case reports, the CARE guidelines were used: two studies [10,27] only had a good quality, three studies [9,29,30] had sufficient quality, and the remaining studies [7,8,12,13,14,16,18,19,20] had a poor methodological quality (Table 7).
Table 7.
Quality evaluation of the included case reports using CARE guidelines.
4. Discussion
Regarding orthodontic extrusion for implant site development, most studies [7,8,9,10,12,13,14,29,30] were case reports, except two, which were case series [5,11]. The studies reporting on regenerative procedures for implant site development included five case reports [16,18,19,20,27], three case series [17,24,25] and one RCT [15]. The majority of studies comparing ridge preservation procedures with spontaneous healing after tooth loss were RCT [22,23,26,28,31], except one, which was a prospective study [21].
Patients undergoing orthodontic extrusion ranged from 23 to 62 years old; patients treated with regenerative surgery ranged from 18 to 68 years old; and, finally, patients included in the studies comparing spontaneous tissue healing versus extraction alone ranged from 20 to 76 years old.
The mean age of patients treated with orthodontic extrusion or regenerative procedures was 40 years, and it was a little lower than the one of patients included in the studies about spontaneous tissue healing after tooth loss and delayed implant placement (52 years); it is not known if this was due to the fact that older patients prefer not to submit to surgery or orthodontic procedures prior to implant placement, or to the clinician’s preference. In all studies, most of the patients were women.
The presence of a systematic disease before Implant placement has been discussed in the literature. A retrospective study [31] that investigated the correlation between systemic diseases and implant treatment found a failure rate of 3.6% and concluded that osteoporosis and Crohn’s disease were significantly associated with early implant failure. Furthermore, the same authors [32] concluded that these factors were not associated with late implant loss. The literature suggests that the level of evidence regarding the association between systemic diseases and implant loss is low [33], but the control of any systemic disease before an implant therapy is considered important [34], and any systemic disease in the patients included in the study should be reported. Regarding health conditions, most patients of the studies included in the systematic review were in good health, but not all studies provided enough information on this subject.
Two retrospective studies [35,36] identified a correlation between smoking and implant complications. For what concerns the smoking habit, both smokers and nonsmokers were included in the studies about regenerative procedures and in the studies comparing ridge preservation procedures with spontaneous healing after tooth loss, as soon as the smoking addiction was moderate (fewer than 10 cigarettes per day). The information provided about patient smoking habits in the group of patients treated with orthodontic extrusion was insufficient.
The biological and functional result of implant treatment is very important regardless of the implant’s position; however, the esthetic outcome is fundamental in the anterior maxilla, especially in patients with a high lip line. The quality and quantity of alveolar bone and soft tissue in the future implant site is essential for proper tridimensional implant placement to achieve esthetic and functional outcomes; therefore, several techniques have been employed to develop the implant site. Both mandibular and maxillary anterior and posterior teeth were treated with orthodontic extrusion or regenerative procedures to enhance the implant site, but the majority were anterior maxillary teeth.
Periodontitis was the primary reason for tooth extraction in the studies reporting on orthodontic extrusion, whereas in the studies reporting on regenerative procedures, many causes can be identified, such as periodontitis, non-restorable tooth, traumas, fractures and endodontic complications. The randomized studies comparing spontaneous tissue healing after extraction with ridge preservation procedures provided no details about the reason for the extractions.
Most of studies did not report any data about the type of bone defects affecting the teeth to be treated, except two: one case series [11] about orthodontic extrusion, which reported a classification of the different types of osseous defects based on the amount of the residual periodontal attachment, and another study [16] about regenerative surgery, which reported the type of defect (Cadwood and Howell class V defect). In the studies comparing spontaneous tissue healing after extraction with ridge preservation procedures, no details were given about bone defects.
Although it has been suggested an association between patient’s gingival biotype and the tendency toward gingival recessions after surgical procedures [37,38,39], only three studies [11,17,22] included information on this subject.
The articles reviewed provided detailed information regarding the treatment procedures and materials used. Different methods were employed to apply the extrusive force: NiTi archwire and a more apical bonding of brackets on the teeth to be extruded, SS archwire with extrusion steps, SS archwire with L-shape loops or elastic bands from orthodontic hooks bonded to the cervical region of teeth to be extruded and a removable appliance. The most used appliance to perform orthodontic extrusion was a multi-bracket system; in only one study [9], a removable appliance was used. The multi-bracket approach was full bimaxillary in three studies [14,29,30] and partial in seven studies [5,7,8,10,11,12,13]. In one study [8], a lingual appliance was used; in another study [13], ceramic brackets were used.
No clinical study has proved the ”uper’ority of extrusive biomechanics versus another, but it is mandatory to use low and controlled extrusive forces. A low extrusive force (<100 g) was applied in all studies, but five studies [5,8,12,29,30] did not report data about the intensity of the force used to perform the extrusion. It is important to understand that when tension is applied to the periodontal ligament, periodontal fibers bundles are elongated, and osteoblasts are induced to deposit new bone in the areas where periodontal attachment exists. The same effects on alveolar bone height can be seen when orthodontic treatment is carried out with controlled forces which do not tear apart the periodontal fibers. In other words, a tooth moved into the dental arch by controlled extrusive orthodontic forces will bring alveolar bone, and soft tissues will follow, too [5,6]. Therefore, using low and controlled extrusive forces is fundamental to enhance hard and soft tissues through orthodontic extrusion.
Regarding the extrusion ratio, the extrusion was performed slowly (mean of 1 mm/month) in six studies [7,8,9,10,11,30] whereas the other five studies did not report any data.
Just two studies [7,11] reported the amount of tooth extrusion performed.
Another important aspect has sufficient anchorage to limit the risk of adverse side effects on the teeth adjacent to those planned to be extruded. Most of the studies used an SS archwire as an anchorage during the extrusion; one study [9] used a removable appliance and one study [8] used a composite resin veneer pontic, while three studies did not report information about the anchorage used.
The orthodontic extrusion should be performed according to the tooth’s long axis to avoid generating any apical compression against the buccal cortical bone, which is likely to cause bone fenestrations.
The frequency of follow-up varied from 2 to 4 weeks; during each control visit, hygiene conditions were checked, the orthodontic extrusion device was activated, and progressive occlusal adjustments were performed in order to maintain the teeth extruded out of the occlusal plane.
In all studies except one [14], a stabilization period followed the orthodontic extrusion to ensure a complete maturation of the newly formed bone; the retention period lasted from 1.5 to 6 months, depending on each study and retention was ensured in most of cases by the multibracket system, which was left in place. Tooth extraction was followed by immediate post-extractive implant placement in all studies, except two [9,12], where a delayed implant placement was performed 4–6 weeks after extraction. Immediate post-extractive implant placement is suggested to keep the hard and soft tissue volume obtained through the orthodontic technique.
All studies showed good treatment outcomes, with satisfying esthetic and biological results and successful implant osteointegration, but two studies [7,11] only reported the implant survival rate (100% and 96%, respectively).
Regarding the amount of bone and/or soft tissue augmentation obtained through the orthodontic extrusion, only a few studies [5,7,11,12,30] gave quantitative data, and only one study [11] indicated the percentage of the efficacy of the technique in the regeneration of bone and soft tissue in the future implant site (70% and 65%, respectively). Most studies reported qualitative results, and for this reason, it is not possible to calculate the real efficacy of the orthodontic technique in the regeneration of hard and soft tissues in a future implant site.
No complications emerged in almost all studies. Nevertheless, we must keep in mind that some bias of non-published data may occur in cases with technical failures, and that makes it difficult to establish an accurate success/failure ratio of the employed technique.
At the moment, based on the available results, it is only possible to say that orthodontic extrusion appears as an interesting non-surgical technique to develop a future implant site using hopeless teeth, with apparently fewer disadvantages and risks than the traditional surgical techniques (GBR, ridge splitting, distraction osteogenesis, and bone grafting). The only constraints to the use of this technique are the presence of hopeless teeth to be extruded with a sufficient quantity of residual periodontal attachment and a sufficient anchorage unit [31,32,33,34,35,36,37].
Some recommendations to optimize the clinical results can be given: low and controlled (<100 g) extrusive forces must be used; an extrusion ratio < 1 mm/month should be performed; it is important to use an anchorage on the teeth adjacent to the ones planned to be extruded; the extrusion should be performed according to the long tooth axis; regular follow-up of patients should be scheduled every month; a post-extrusion retention period is suggested; immediate post-extractive implants are suggested to keep the hard and soft tissues volume obtained through the orthodontic technique.
Further studies are necessary to evaluate the efficacy of the technique in the regeneration of hard and soft tissues, to compare the different extrusive biomechanics and to create an evidence-based clinical protocol. Another aspect to investigate is the resorption rate of the orthodontically regenerated bone to compare the quality and quantity of bone regenerated through orthodontic extrusion with that obtained using regenerative procedures.
For implant site development, different regenerative procedures were used: four studies [15,17,19,20] performed a one-stage or two-stage guided bone regeneration (GBR), three studies [16,18,25] performed a bone graft procedure, and two studies [24,27] performed alveolar distraction osteogenesis.
A wide variety of materials were employed for the regenerative procedures, and all studies gave information about the materials used: for GBR procedures, one study [15] used a deproteinized bovine bone mineral (Bio-Oss), one study [17] used a freeze-dried mineralized bone allograft and the other two studies [19,20] used demineralized freeze-dried bone particles (Dembone); for bone grafting, one study [18] used a Puros block allograft rehydrated with platelet-rich plasma and additional Puros particulate mineralized bone graft material, and the other two studies used autogenous bone grafts from symphysis [25] and from the retromolar area [16]; and the studies [24,27] performing alveolar distraction osteogenesis used the same type of distraction device (Modus distractor, Medartis).
All studies performing GBR or bone graft procedures used barrier membranes: three studies [15,16,18] used resorbable membranes and the other four studies [17,19,20,25] used non-resorbable membranes.
Regarding the timing of implant placement, two studies [15,19] performed a regenerative procedure with a simultaneous implant placement, two studies [17,25] performed a regenerative procedure with a simultaneous or delayed implant placement, depending on each patient clinical condition and five studies [16,18,20,24,27] performed a regenerative procedure with a delayed implant placement in the regenerated bone.
All studies except two [16,20] gave details about the type of implants used.
The follow-up period ranged from a minimum of 6 months [15] to a maximum of 3 years [16,24,25], depending on each study.
All studies reported good outcomes, with an enhancement of hard tissue, but few of them gave quantitative data about the amount of regenerated bone; therefore it is not possible to evaluate the efficacy of the different techniques in bone regeneration. Regarding soft tissue changes, no study reported data, except one [24].
Each regenerative surgical procedure showed some limits; one randomized study [15] reported that GBR with resorbable membranes and particulate bone substitutes undergoes some horizontal volume reduction during the healing stage. Greater reduction occurs at the coronal region and the use of different implant healing strategies (transmucosal or submerged) does not make a significant difference. This volume instability could result in the shrinkage of the grafted area and alteration of the ridge contour. To compensate for the volume reduction during the healing stage of GBR, over augmentation has been recommended by some clinicians [40]. In the coronal region, new bone formation may be predictably expected only within the bony envelope of the defect, but further studies are needed to confirm this result. The regenerated hard tissue, determined by the radiographic observation of a radiopacity, may not be true new bone in a histological sense, because not always the biomaterial is resorbed and replaced by new bone, but it can remain as a “foreign body” within the graft [41,42,43,44,45].
Another difficulty with GBR techniques is associated to the use of membranes: non-resorbable membranes have good mechanical properties but they also have a lower biocompatibility, request a second surgery for their removal and there is always a risk of early exposure during the healing process, which can compromise the result. Resorbable membranes have higher biocompatibility and do not request a second surgery, but they have unfavorable mechanical properties, volume instability due to their soft consistency and low resistance to pressure from the surrounding tissues, which may result in membrane collapse and the compromise of the new bone formation due to the loss of tissue volume during the healing stage of the GBR procedure.
Finally, the GBR technique can only regenerate hard tissue, to ease an implant placement, but the soft tissue volume is often inadequate to provide an esthetic result, and it is difficult to simultaneously graft the ridge-augmentation site with soft tissue because of poor vascular support over a GBR membrane. Therefore, the esthetic result sometimes may be unsatisfactory [46].
Autogenous bone is the ideal biomaterial, thanks to its biocompatibility and osteogenicity. Regarding bone graft procedures, autogenous bone blocks remain the ‘gold standard’; intraoral block grafts harvested from the symphysis or the mandibular ramus can be used to reconstruct horizontal and vertical ridge deficiencies prior to implant placement. If the amount of bone needed exceeds what is available intraorally, extraoral sites, such as the iliac crest and calvarium, can be considered [47,48]. The main disadvantage of autologous bone grafts is the morbidity of the donor site; another complicating factor is the additional surgical time necessary to harvest the bone block. As an alternative to this type of grafting, allogenic, xenographic and alloplastic materials have been developed, but they can only provide osteoconduction or osteoinduction, not osteogenesis, and none of them guarantee the healing and bone replacement that autogenous block grafts can provide [49,50,51,52,53,54,55].
The successful integration of a bone graft depends on numerous factors, which are all associated with a good surgical technique. In the receiving site, the cortical plate should be perforated to induce bleeding, which is fundamental to the healing process. There should be intimate contact between the bone block and the recipient site; precise measurements or a template of the recipient site can help to ensure that the harvested bone block is adequate in size and form. The bone graft must be completely still during the healing process, because any movement causes its failure: for this reason, the blocks should be secured through mini screws to the host site. Once the block is screwed, a tension free flap closure and a primary healing must be obtained. Strict asepsis protocols must be respected [56].
Implant primary stability, whenever possible, should be researched in the native bone of the patient, even basal bone: when the native bone ensures the primary stability and the graft only works as a coverage for the implant, implants can be placed 4 months after the graft procedure; otherwise, when there is no residual native bone, it is recommended to wait 6–8 months from the graft procedure before placing the implants, because new bone must form inside the graft in order to have primary stability for the implant. Bone augmentation could also be performed simultaneously with implant placement, but it is associated with increased failure rates [57].
Ridge splitting technique can increase the width of bone by splitting and expanding the existing residual ridge. Indications of this technique include the ridge deficient in width with an adequate amount of height, with no vertical defects. The maxilla is preferred over the mandible because the expansion of bone is easily achieved without any complications thanks to the cancellous nature of bone. Advantages include no second surgery required to place implants simultaneously inserted during the ridge splitting procedure, reduced overall treatment time and increased implant stability because of new bone formation between cortical plates. Disadvantages include more severe ridge defects in case of procedure failure and primary closure being difficult to achieve [58,59,60].
Distraction osteogenesis is based on the principle of secondary wound healing. Osteotomy removes a bone segment from the basal bone, and the distraction gap is filled with callus that forms a new bone segment. This procedure demonstrates many advantages such as decreased bone resorption, no donor site morbidity and simultaneous lengthening of the surrounding soft tissues. This technique requires a delayed implant placement (at least 4 months from the end of the distraction) to wait for the consolidation of distracted bone segments. Therefore, there are also disadvantages, such as the risk of fracture of the mandible, fracture of the transport segment, difficulties in finishing the osteotomy on the lingual side, incorrect direction of distraction, perforation of the mucosa by the transport segment, suture dehiscence, bone formation defects and pain during the activation of the distraction device.
In conclusion, based on the available results, all these regenerative procedures allow an enhancement of a future implant site, with satisfying esthetic and functional outcomes. No study reported a failure and no complications emerged in almost all studies. Nevertheless, we must keep in mind that some bias of non-published data may occur in cases with technical failures, and that makes it difficult to establish an accurate success/failure ratio of the employed techniques [61,62].
Compared to orthodontic extrusion, the regenerative surgical techniques appear more complex, with a higher risk of complications and with a limited ability to develop soft tissues. Regarding the regeneration of hard tissue, most studies reported qualitative results, and for this reason, it is not possible to calculate the real efficacy of the different techniques in the formation of new bone and it is not possible to compare the results with those obtained through orthodontic extrusion [63,64].
Finally, the authors have evaluated randomized studies comparing ridge preservation procedures with spontaneous healing of the edentulous ridge after tooth loss and a delayed implant placement. Overall, the different ridge preservation procedures reduced post-extraction alveolar ridge dimensional changes, compared to extraction alone, but they were unable to prevent resorption. Another systematic review [65] confirmed these results, but also suggested the use of barrier membranes, flap surgical procedures and full flap closure to achieve better results. The obtained results, however, could not indicate which type of surgical procedure or biomaterial is most suitable for this approach.
Regarding hard tissue volume, even if ridge preservation procedures appear to be better than extraction alone followed by a delayed implant placement, one prospective study [21] showed that, if tooth extraction is atraumatic and the granulation tissue is left in situ, both horizontal and vertical dimension could be maintained, because the granulation tissue contains new small blood vessels and pluripotent stem cells that contribute to tissue healing. Regarding soft tissue volume, the authors found discordant results. One study [22] reported a loss of soft tissue thickness on the buccal aspect in the ridge preservation group of patients. Kirkland et al. previously showed that using a resorbable membrane for ridge augmentation decreased soft tissue thickness; the same phenomenon occurred in this study. Soft tissue thickness loss occurs together with hard tissue loss; the greatest loss is on the buccal side; therefore, it has important relevance in the esthetic zone. This loss of soft tissue thickness is most likely due to the interference with flap vascularity by the membrane and the graft; since the membrane is interposed between the flap and the bone surface, the vascular supply for the flap comes only from the flap base rather than the dual blood supply from the underlying osseous and flap base found in non-grafted sites. On the contrary, two other studies [26,28] reported a greater soft tissue volume in the grafted groups. Further studies are needed to confirm these results, and split-mouth studies would be the most indicative to compare these different approaches.
Study Limitations
The methodological quality evaluation showed that most of studies regarding orthodontic extrusion are case reports, which correspond to the lowest level of scientific evidence; moreover, the lack of quantitative data about the outcomes of the different approaches limits the strength of the conclusion that can be drawn and does not allow the creation of an evidence-based protocol for the development of the implant site. In this perspective, different methods under different conditions could lead to difficult comparison evaluation.
5. Conclusions
The present systematic review demonstrated that there is a substantial lack of data and evidence to determine which of the presented methods is better to develop a future implant site; the main problem is the absence of randomized controlled trials and multicenter studies comparing the two implant site development approaches: orthodontic extrusion versus regenerative surgery. On the contrary, in the literature, there are many RCT studies comparing ridge preservation procedures and extraction alone, but further studies are needed to identify the best materials and procedures to use and to create an evidence-based protocol for clinicians.
Based on the available results, both surgical and non-surgical procedures appear effective in the regeneration of hard tissue in a future implant site, whereas not all the techniques can improve soft tissue volume, too.
Regarding orthodontic extrusion, no clinical study has proved the superiority of extrusive biomechanics versus another yet, but some useful recommendations can be given to clinicians:
- Low and controlled (<100 g) extrusive forces;
- Extrusion ratio < 1 mm/month;
- Extrusion according to the tooth long axis;
- A post-extrusion retention period is suggested to wait for the maturation of the regenerated bone;
- Immediate post-extractive implants are suggested to keep the hard and soft tissues volume obtained through the orthodontic technique; a guided insertion could be beneficial for aesthetic and patient comfort.
Author Contributions
Conceptualization, M.M. and G.I.; Methodology, A.U.; Formal Analysis, R.N.; Investigation, A.D.M.; Resources, S.D.; Data Curation, S.D. and A.U.; Writing—Original Draft Preparation, S.D.; Writing—Review and Editing, R.N., M.M. and G.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available upon reasonable request. Review registration: PROSPERO (CRD42020162718).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chappuis, V.; Araujo, M.G.; Buser, D. Clinical relevance of dimensional bone and soft tissue alterations post-extraction in esthetic sites. Periodontology 2000 2017, 73, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Moya-Villaescusa, M.J.; Sanchez-Perez, A. Measurement of ridge alterations following tooth removal: A radiographic study in humans. Clin. Oral Implant. Res. 2010, 21, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Seibert, J.S.; Salama, H. Alveolar ridge preservation and reconstruction. Periodontology 2000 1996, 11, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Salama, H.; Salama, M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: A systematic approach to the management of extraction site defects. Int. J. Periodontics Restor. Dent. 1993, 13, 312–333. [Google Scholar]
- Mantzikos, T.; Shamus, I. Forced eruption and implant site development: An osteophysiologic response. Am. J. Orthod. Dentofac. Orthophedics 1999, 115, 583–591. [Google Scholar] [CrossRef]
- Mantzikos, T.; Shamus, I. Forced eruption and implant site development: Soft tissue response. Am. J. Orthod. Dentofac. Orthophedics 1997, 112, 596–606. [Google Scholar] [CrossRef]
- Watanabe, T.; Marchack, B.W.; Takei, H. Creating labial bone for immediate implant placement: A minimally invasive approach by using orthodontic therapy in the esthetic zone. J. Prosthet. Dent. 2013, 110, 435–441. [Google Scholar] [CrossRef]
- Paolone, M.; Kaitsas, R.; Paolone, G.; Kaitsas, V. Lingual orthodontics and forced eruption: A means for osseous and tissue regeneration. Case Report. Prog. Orthod. 2008, 9, 90–110. [Google Scholar]
- Hyun Kim, S.; Tramontina, V.A.; Papalexiou, V.; Luczyszyn, S.M. Orthodontic extrusion and implant site development using an interocclusal appliance for a severe mucogingival deformity: A clinical report. J. Prosthet. Dent. 2011, 105, 72–77. [Google Scholar] [CrossRef]
- Joo, J.Y.; Son, S.; Lee, J.Y. Implant site development for enhancing esthetics of soft and hard tissue and simplification of implant surgery using a forced eruption. Int. J. Periodontics Restor. Dent. 2016, 36, 583–589. [Google Scholar] [CrossRef]
- Amato, F.; Mirabella, D.; Macca, U.; Tarnow, D.P. Implant site development by orthodontic forced extraction: A preliminary study. Int. J. Oral Maxillofac. Implant. 2012, 27, 411–420. [Google Scholar]
- Mantzikos, T.; Shamus, I. Case report: Forced eruption and implant site development. Angle Orthod. 1998, 68, 179–186. [Google Scholar] [PubMed]
- Holst, S.; Hegenbarth, E.; Schlegel, K.A.; Holst, A.I. Restoration of a nonrestorable central incisor using forced orthodontic eruption, immediate implant placement and an all-ceramic restoration: A clinical report. J. Prosthet. Dent. 2007, 98, 251–255. [Google Scholar] [CrossRef]
- Erkut, S.; Arman, A.; Gulsahi, A.; Uckan, S.; Gulsahi, K. Forced eruption and implant treatment in posterior maxilla: A clinical report. J. Prosthet. Dent. 2007, 97, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zhang, Y.; Mi, P.; Lin, Y. Hard tissue volume stability of guided bone regeneration during the healing stage in the anterior maxilla: A clinical and radiographic study. Clin. Implant. Dent. Relat. Res. 2018, 20, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.P. Implant placement in the esthetic zone following an autogenous bone graft from an intraoral site: A Case Study. Prim. Dent. J. 2013, 2, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Fagan, M.C.; Owens, H.; Smaha, J.; Kao, R.T. Simultaneous hard and soft tissue augmentation for implants in the esthetic zone: Report of 37 consecutive cases. J. Periodontol. 2008, 79, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Petrungaro, P.; Salomon, A. Localized ridge augmentation with allogenic block grafts prior to implant placement: Case reports and histologic evaluations. Implant. Dent. 2005, 14, 139–148. [Google Scholar] [CrossRef]
- Artzi, Z.; Nemcovsky, C. Bone regeneration in extraction sites. Part I: The simultaneous approach. Implant. Dent. 1997, 6, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Artzi, Z.; Nemcovsky, C.; Rosenblat, O.; Zohar, R.; Kozak, D. Bone regeneration in extraction sites. Part II: The staged approach. Implant. Dent. 1997, 6, 183–187. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Crespi, G.; Gastaldi, G.; Gherlone, E.F. Delayed implants outcome in maxillary molar region. Clin. Implant. Dent. Relat. Res. 2017, 19, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Iasella, J.M.; Greenwell, H.; Miller, R.L.; Hill, M.; Drisko, C.; Bohra, A.A.; Scheetz, J.P. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: A clinical and histologic study in human. J. Periodontol. 2003, 74, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Aldini, N.N.; Fini, M.; Giardino, R.; Calvo Guirado, J.L.; Covani, U. Xenograft versus extraction alone for ridge preservation after tooth removal: A clinical and histomorphometric study. J. Periodontol. 2008, 79, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Sezer, B.; Koyuncu, B.O.; Gunbay, T.; Sezak, M. Alveolar distraction osteogenesis in the human mandible: A clinical and histomorphometric study. Implant. Dent. 2012, 21, 317–322. [Google Scholar] [CrossRef]
- McCarthy, C.; Patel, R.R.; Wragg, P.F.; Brook, I.M. Dental implants and onlay bone grafts in the anterior maxilla: Analysis of clinical outcome. Int. J. Oral Maxillofac. Implant. 2003, 18, 238–241. [Google Scholar]
- Marconcini, S.; Giammarinaro, E.; Derchi, G.; Alfonsi, F.; Covani, U.; Barone, A. Clinical outcomes of implants placed in ridge-preserved versus nonpreserved sites: A 4-year randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2018, 20, 906–914. [Google Scholar] [CrossRef]
- Gozneli, R.; Ozkan, Y.; Akalin, Z.F. Rehabilitation of maxillary anterior esthetics by alveolar distraction osteogenesis with immediate implant placement: A case report. Implant. Dent. 2010, 19, 468–476. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implant. Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef]
- de Barros, L.A.; de Almeida Cardoso, M.; de Avila, E.D.; de Molon, R.S.; Sigueira, D.F.; Mollo-Junior Fde, A. Six-year follow-up of maxillary anterior rehabilitation with forced orthodontic extrusion: Achieving esthetic excellence with a multidisciplinary approach. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 607–615. [Google Scholar] [CrossRef]
- Chou, Y.H.; Du, J.K.; Chou, S.T.; Hu, K.F.; Tsai, C.C.; Ho, K.Y.; Wu, Y.M.; Ho, Y.P. An interdisciplinary treatment approach combining orthodontic forced eruption with immediate implant placement to achieve a satisfactory treatment outcome: A case report. Clin. Implant. Dent. Relat. Res. 2013, 15, 113–120. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Komarek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of oral implant failure, up to abutment connection. J. Clin. Periodontol. 2007, 34, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, G.; Quirynen, M.; Komarek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin. Oral Implant. Res. 2008, 19, 670–676. [Google Scholar] [CrossRef]
- Bornestein, M.M.; Cionca, N.; Mombelli, A. Systemic conditions and treatments as risk for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 12–27. [Google Scholar]
- Diz, P.; Scully, C.; Sanz, M. Dental implants in the medically compromised patient. J. Dent. 2013, 41, 195–206. [Google Scholar] [CrossRef]
- Vervaeke, S.; Collaert, B.; Cosyn, J.; Deschepper, E.; De Bruyn, H. A multifactorial analysis to identify predictors of implant failure and peri-implant bone loss. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 1), 298–307. [Google Scholar] [CrossRef]
- Rondriguez-Arqueta, O.F.; Figueiredo, R.; Valmaseda-Castellon, E.; Gay-Escoda, C. Postoperative complications in smoking patients treated with implants. A retrospective study. J. Oral Maxillofac. Surg. 2011, 69, 2152–2157. [Google Scholar] [CrossRef]
- Kois, J.C.; Kan, J.Y. Predictable peri-implant gingival esthetics: Surgical and prosthodontics rationales. Pract. Proced. Aesthetic Dent. 2001, 13, 691–698. [Google Scholar]
- Koke, U.; Sander, C.; Heinecke, A.; Muller, H.P. A possible influence of gingival dimensions on attachment loss and gingival recession following placement of artificial crowns. Int. J. Periodontics Restor. Dent. 2003, 23, 439–445. [Google Scholar]
- Kan, J.Y.; Morimoto, T.; Rungcharassaeng, K.; Roe, P.; Smith, D.H. Gingival biotype assessment in the esthetic zone: Visual versus direct measurement. Int. J. Periodontics Restor. Dent. 2010, 30, 237–243. [Google Scholar]
- Hammerle, C.H.; Lang, N.P. Single stage surgery combining transmucosal implant placement with guided bone regeneration and bioresorbable materials. Clin. Oral Implant. Res. 2001, 12, 9–18. [Google Scholar] [CrossRef]
- Jung, R.E.; Fenner, N.; Hammerle, C.H.; Zitzmann, N.U. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12–14 years. Clin. Oral Implant. Res. 2013, 24, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Zaniboni, M. Clinical of GBR procedures to correct peri-implant dehiscences and fenestrations: A systematic review. Clin. Oral Implant. Res. 2009, 20, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Holst, A.I.; Nkenke, E.; Blatz, M.B.; Geiselhoringer, H.; Holst, S. Prosthetic considerations for orthodontic implant site development in the adult patient. J. Oral Maxillofac. Surg. 2009, 67, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Kaitsas, R.; Paolone, M.G.; Paolone, G. Guided orthodontic regeneration: A tool to enhance conventional regenerative techniques in implant surgery. Int. Orthod. 2015, 13, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Paolone, M.G.; Kaitsas, R. Orthodontic-periodontal interactions: Orthodontic extrusion in interdisciplinary regenerative treatments. Int. Orthod. 2018, 16, 217–245. [Google Scholar] [CrossRef]
- Taskonak, B.; Ozkan, Y. An alveolar bone augmentation technique to improve esthetics in anterior ceramic FPDs: A clinical report. J. Prosthodont. 2006, 15, 32–36. [Google Scholar] [CrossRef]
- Uribe, F.; Taylor, T.; Shafer, D.; Nanda, R. A novel approach for implant site development through root tipping. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 649–655. [Google Scholar] [CrossRef]
- Hof, M.; Pommer, B.; Strbac, G.D.; Suto, D.; Watzek, G.; Zechner, W. Esthetic evaluation of single-tooth implants in the anterior maxilla following autologous bone augmentation. Clin. Oral Implant. Res. 2013, 24 (Suppl. A), 88–93. [Google Scholar] [CrossRef]
- Bauer, C.; Boileau, M.J.; Bazert, C. Implementation of orthodontic extraction for pre-implant soft tissue management: A systematic review. Int. Orthod. 2019, 17, 20–37. [Google Scholar] [CrossRef]
- Almurtadha, R.H.; Alhammadi, M.S.; Fayed, M.M.S.; Abou-El-Ezz, A.; Halboub, E. Changes in soft tissue profile after orthodontic treatment with and without extraction: A systematic review and meta-analysis. J. Evid.-Based Dent. Pract. 2018, 18, 193–202. [Google Scholar] [CrossRef]
- Alsahhaf, A.; Att, W. Orthodontic extrusion for pre-implant site enhancement: Principles and clinical guidelines. J. Prosthodont. Res. 2016, 60, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, C.; Linde, A.; Gottlow, J.; Nyman, S. Healing of bone defects by guided tissue regeneration. Plast. Recostructive Surg. 1998, 81, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Devlin, H.; Sloan, P. Early bone healing events in the human extraction socket. Int. J. Oral Maxillofac. Surg. 2002, 31, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Magkavali-Trikka, P.; Kirmanidou, Y.; Michalakis, K.; Gracis, S.; Kalpidis, C.; Pissiotis, A.; Hirayama, H. Efficacy of two site-development procedures for implants in the Maxillary esthetic region: A systematic review. Int. J. Oral Maxillofac. Implant. 2015, 30, 73–94. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Morjaria, K.R.; Wilson, R.; Palmer, R.M. Bone healing after tooth extraction with or without an intervention: A systematic review of randomized controlled trials. Clin. Implant. Dent. Relat. Res. 2014, 16, 1–20. [Google Scholar] [CrossRef]
- Lekholm, U.; Wannfors, K.; Isaksson, S.; Adielsson, B. Oral implants in combination with bone grafts. A 3 year retrospective multicenter study using Branemark implant system. Int. J. Oral Maxillofac. Surg. 1999, 28, 181–187. [Google Scholar] [CrossRef]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ridge preservation after tooth extraction. A systematic review. Clin. Oral Implant. Res. 2011, 23, 22–38. [Google Scholar] [CrossRef]
- Pietrokovski, J.; Massler, M. Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Wang, R.E.; Lang, N.P. Ridge preservation after tooth extraction. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 147–156. [Google Scholar] [CrossRef]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Ingber, J.S. Forced eruption part II: A method of treating non-restorable teeth—Periodontal and restorative considerations. J. Periodontol. 1976, 47, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Ingber, J.S. Forced eruption part I: A method of treating isolated one and two wall infrabony osseous defects—Rationale and case report. J. Periodontol. 1974, 45, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Somar, M.; Mohadeb, J.V.; Huang, C. Predictability of orthodontic forced eruption in developing an implant site: A systematic review. J. Clin. Orthod. 2016, 50, 485–492. [Google Scholar] [PubMed]
- Korayem, M.; Flores-Mir, C.; Nassar, U.; Olfert, K. Implant site development by orthodontic extrusion: A systematic review. Angle Orthod. 2008, 78, 752–760. [Google Scholar] [CrossRef]
- Misch, C.M. Implant site development using ridge splitting techniques. Oral Maxillofac. Surg. Clin. N. Am. 2004, 16, 65–74. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).