
Respiratory Physiology of COVID-19 and Influenza Associated Acute Respiratory Distress Syndrome

 and
and
Abstract
1. Background
2. Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Basic Patient Characteristics
3.2. Horizontal Comparison of Ventilation Parameters
3.3. Longitudinal Comparison of Ventilation Parameters
3.4. Subgroup Analysis–ECMO vs. Non-ECMO
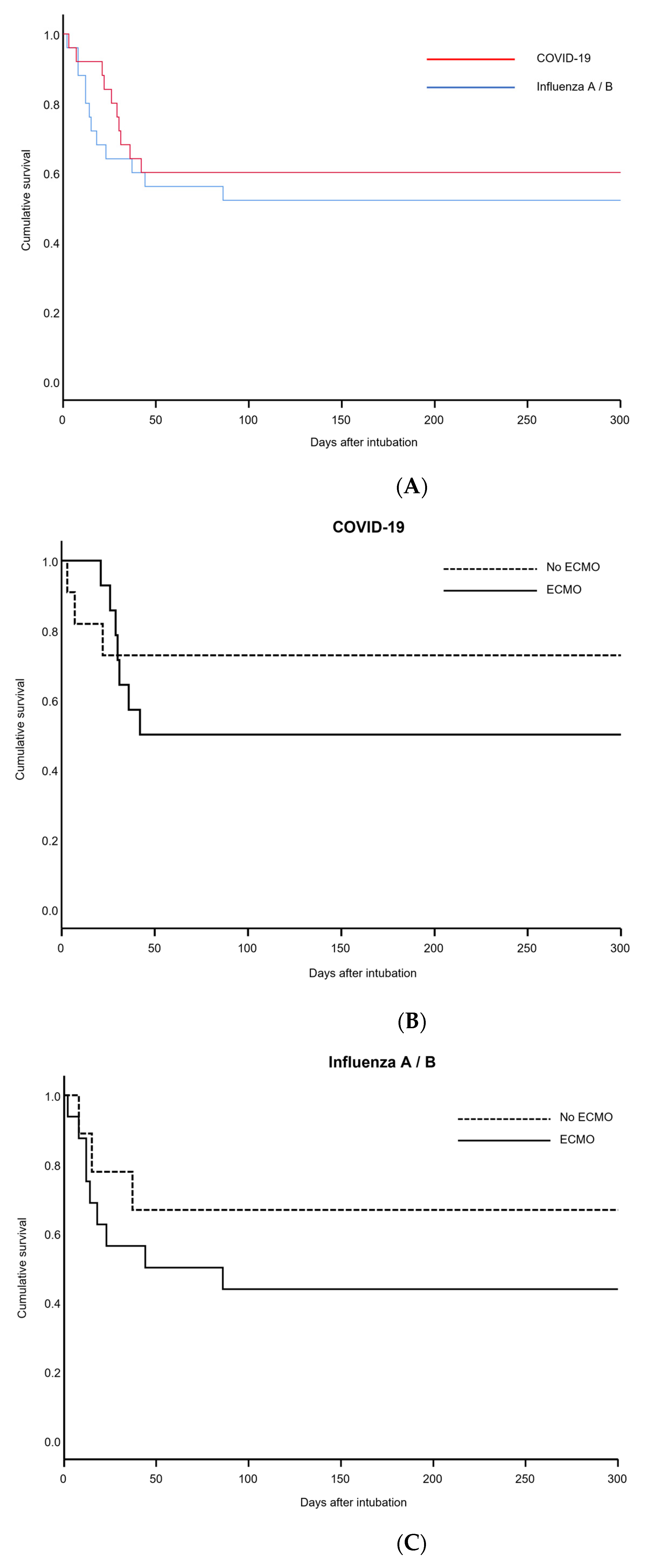
3.5. Outcome
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | Acute respiratory distress syndrome |
| COPD COVID-19 | Chronic Obstructive Pulmonary Disease Coronavirus disease 2019 |
| ΔP | driving pressure |
| ECMO | Extracorporeal membrane oxygenation |
| HFNC | High-Flow Nasal Cannula |
| PEEP | positive end-expiratory pressure |
| PP | plateau pressure |
| RR | Respiratory Rate |
| VILI | Ventilator induced lung injury |
| VR | Ventilatory ratio |
References
- Hozhabri, H.; Piceci Sparascio, F.; Hamidreza, S.; Mousavifar, L.; Roy, R.; Scribano, D.; De Luca, A.; Ambrosi, C.; Sarshar, M. The Global Emergency of Novel Coronavirus (SARS-CoV-2): An Update of the Current Status and Forecasting. Int. J. Environ. Res. Public Health 2020, 17, 5648. [Google Scholar] [CrossRef] [PubMed]
- Raoult, D.; Zumla, A.; Locatelli, F.; Ippolito, G.; Kroemer, G. Coronavirus infections: Epidemiological, clinical and immunological features and hypotheses. Cell Stress 2020, 4, 66–75. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extracorporeal Life Support Organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef]
- Ramanathan, K.; Shekar, K.; Ling, R.R.; Barbaro, R.P.; Wong, S.N.; Tan, C.S.; Rochwerg, B.; Fernando, S.M.; Takeda, S.; MacLaren, G.; et al. Extracorporeal membrane oxygenation for COVID-19: A systematic review and meta-analysis. Crit. Care 2021, 25, 211. [Google Scholar] [CrossRef]
- Gattinoni, L.; Coppola, S.; Cressoni, M.; Busana, M.; Rossi, S.; Chiumello, D. COVID-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome. Am. J. Respir Crit Care Med. 2020, 201, 1299–1300. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Bongiovanni, F.; Chen, L.; Menga, L.S.; Cutuli, S.L.; Pintaudi, G.; Carelli, S.; Michi, T.; Torrini, F.; Lombardi, G.; et al. Respiratory physiology of COVID-19-induced respiratory failure compared to ARDS of other etiologies. Crit. Care 2020, 24, 529. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Chiumello, D.; Rossi, S. COVID-19 pneumonia: ARDS or not? Crit. Care 2020, 24, 154. [Google Scholar] [CrossRef]
- Ferrando, C.; Suarez-Sipmann, F.; Mellado-Artigas, R.; Hernández, M.; Gea, A.; Arruti, E.; Aldecoa, C.; Martínez-Pallí, G.; Martínez-González, M.A.; Slutsky, A.S.; et al. Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. 2020, 46, 2200–2211. [Google Scholar] [CrossRef]
- Marini, J.J.; Gattinoni, L. Management of COVID-19 Respiratory Distress. JAMA 2020, 323, 2329–2330. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Caironi, P.; Cressoni, M.; Chiumello, D.; Ranieri, V.M.; Quintel, M.; Russo, S.; Patroniti, N.; Cornejo, R.; Bugedo, G. Lung recruitment in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2006, 354, 1775–1786. [Google Scholar] [CrossRef] [PubMed]
- Dhont, S.; Derom, E.; van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir. Res. 2020, 21, 198. [Google Scholar] [CrossRef] [PubMed]
- Santamarina, M.G.; Boisier, D.; Contreras, R.; Baque, M.; Volpacchio, M.; Beddings, I. COVID-19: A hypothesis regarding the ventilation-perfusion mismatch. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.; Seiler, F.; Muellenbach, R.M.; Danziger, G.; Kamphorst, M.; Lotz, C.; PACovid Study Group; Bals, R.; Lepper, P.M. Pulmonary Hemodynamics and Ventilation in Patients With COVID-19-Related Respiratory Failure and ARDS. J. Intensive Care Med. 2021, 36, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: Is it “typical” ARDS? Crit. Care 2020, 24, 198. [Google Scholar] [CrossRef]
- Chiumello, D.; Busana, M.; Coppola, S.; Romitti, F.; Formenti, P.; Bonifazi, M.; Pozzi, T.; Palumbo, M.M.; Cressoni, M.; Herrmann, P.; et al. Physiological and quantitative CT-scan characterization of COVID-19 and typical ARDS: A matched cohort study. Intensive Care Med. 2020, 46, 2187–2196. [Google Scholar] [CrossRef]
- Mang, S.; Kalenka, A.; Broman, L.M.; Supady, A.; Swol, J.; Danziger, G.; Becker, A.; Hörsch, S.I.; Mertke, T.; Kaiser, R.; et al. Extracorporeal Life Support in COVID-19-related Acute Respiratory Distress Syndrome—A EuroELSO international survey. Artif. Organs 2021, 45, 495–505. [Google Scholar] [CrossRef]
- Hong, X.; Xiong, J.; Feng, Z.; Shi, Y. Extracorporeal membrane oxygenation (ECMO): Does it have a role in the treatment of severe COVID-19? Int. J. Infect. Dis. 2020, 94, 78–80. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G. Poor survival with extracorporeal membrane oxygenation in acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19): Pooled analysis of early reports. J. Crit. Care 2020, 58, 27. [Google Scholar] [CrossRef]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.aerztekammer-saarland.de/files/164CC10E4F3/GV-0005%20Saarl%E4ndisches%20Krankenhausgesetz.pdf (accessed on 15 October 2022).
- Haudebourg, A.-F.; Perier, F.; Tuffet, S.; de Prost, N.; Razazi, K.; Dessap, M.A.; Carteaux, G. Respiratory Mechanics of COVID-19- versus Non-COVID-19-associated Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 202, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Choron, R.L.; Butts, C.A.; Bargoud, C.; Krumrei, N.J.; Teichman, A.L.; Schroeder, M.E.; Manderski, M.T.B.; Cai, J.; Song, C.; Rodricks, M.B.; et al. Fever in the ICU: A Predictor of Mortality in Mechanically Ventilated COVID-19 Patients. J. Intensive Care Med. 2021, 36, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef]
- Stawicki, S.P.; Jeanmonod, R.; Miller, A.C.; Paladino, L.; Gaieski, D.F.; Yaffee, A.Q.; De Wulf, A.; Grover, J.; Papadimos, T.J.; Bloem, C.; et al. The 2019–2020 Novel Coronavirus (Severe Acute Respiratory Syndrome Coronavirus 2) Pandemic: A Joint American College of Academic International Medicine-World Academic Council of Emergency Medicine Multidisciplinary COVID-19 Working Group Consensus Paper. J. Glob. Infect. Dis. 2020, 22, 47–93. [Google Scholar] [CrossRef]
- Rola, P.; Farkas, J.; Spiegel, R.; Kyle-Sidell, C.; Weingart, S.; Duggan, L.; Garrone, M.; Thomas, A. Rethinking the early intu-bation paradigm of COVID-19: Time to change gears? Clin. Exp. Emerg. Med. 2020, 7, 78–80. [Google Scholar] [CrossRef]
- Gattinoni, L.; Marini, J.J.; Camporota, L. The Respiratory Drive: An Overlooked Tile of COVID-19 Pathophysiology. Am. J. Respir. Crit. Care Med. 2020, 202, 1079–1080. [Google Scholar] [CrossRef]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar] [CrossRef]
- Mang, S.; Reyher, C.; Mutlak, H.; Natanov, R.; Lotz, C.; Gill-Schuster, D.; Bals, R.; Danziger, G.; Meybohm, P.; Combes, A.; et al. Awake Extracorporeal Membrane Oxygenation for COVID-19-induced Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2022, 205, 847–851. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| COVID (n = 25) | Influenza (n = 25) | p | |
|---|---|---|---|
| Age on admission [years] | 61.7 [53.1–68.1] | 55.7 [45.5–65.4] | p = 0.082 * |
| Male/female | 20/5 | 16/9 | p = 0.210 |
| Height [m] | 1.77 [1.73–1.81] | 1.73 [1.70–1.76] | p = 0.105 |
| Weight [kg] | 100.4 [91.6–109.2] | 95.9 [81.3–110.5] | p = 0.573 |
| Body-Mass Index (BMI) [kg/m2] | 32.3 [29.0–35.5] | 31.5 [27.0–36.0] | p = 0.781 |
| Comorbidities: | Adiposity (19) Arterial Hypertension (13) Diabetes mellitus Type II (3) Coronary Heart Disease (3) Congestive Heart Failure (3) Past pulmonary embolism (3) Past stroke (4) Myasthenia gravis (1) | Adiposity (10) Arterial Hypertension (10) Diabetes mellitus Type II (9) Coronary Heart Disease (6) COPD (4) Chronic kidney disease (3) Epilepsy (2) Atrial fibrillation Cystic fibrosis Asthma | p = 0.010 ** p = 0.400 p = 0.047 ** p = 0.270 |
| COVID-19 | Influenza A/B | Significance | |
|---|---|---|---|
| Arterial oxygen partial pressure [mmHg] | 84.4 [76.8–92.1] n = 14 | 93.3 [71.8–114.8] n = 9 | p = 0.313 |
| Inspiratory oxygen fraction during non-invasive ventilation/HFNC | 0.6 [0.49–0.70] n = 14] | 0.75 [0.53–0.84] n = 9 | p = 0.227 |
| Arterial carbon dioxide partial pressure [mmHg] | 42.1 [38.1–46.0] n = 14 | 45.0 [38.1–51.9] n = 9 | p = 0.384 |
| pH | 7.39 [7.37–7.41] n = 14 | 7.34 [7.30–7.39] n = 8 | p = 0.03 |
| Horovitz-Index | 127.9 [112.8–161.3] n = 14 | 135.4 [100.3–180.4] n = 9 | p = 0.557 |
| Positive end-expiratory pressure (PEEP) [cmH2O/mbar] | 12.0 [9.6–13.5] n = 14 | 13.0 [9.0–15.5] n = 9 | p = 0.369 |
| Plateau pressure [cmH2O/mbar] | 23.5 [20.8–29.0] n = 14 | 25.0 [24.0–28.5] n = 9 | p = 0.561 |
| Delta-P [cmH2O/mbar] | 13.5 [10.8–16.0] n = 14 | 12.0 [11.0–14.5] n = 9 | p = 0.643 |
| Tidal volume [mL] | 551 [434.5–593.8] n = 14 | 431 [210–572] n = 9 | p = 0.124 |
| Tidal volume per kg predicted body weight [mL/kg] | 7.69 [7.12–8.12] n = 14 | 5.12 [3.14–8.40] n = 8 | p = 0.059 |
| Respiratory Rate * [min−1] | 20.0 [15.5–21.3] n = 14 | 14.0 [12.5–17.5] n = 9 | p = 0.011 |
| Minute ventilation [L/min] | 10.7 [7.2–12.2] n = 14 | 6.0 [2.5–10.1] n = 9 | p = 0.013 |
| COVID-19 | Influenza A/B | Significance | |
|---|---|---|---|
| Ventilatory system compliance [mL/mbar] | 40.7 [31.8–46.7]; n = 14 | 31.4 [13.7–42.8]; n = 9 | p = 0.198 |
| Ventilatory system compliance/kg idealized body weight [mL/mbar/kg] | 0.57 [0.48–0.70]; n = 14 | 0.41 [0.20–0.59]; n = 8 | p = 0.150 |
| Ventilatory Ratio | 1.57 [1.31–1.84]; n = 14 | 0.91 [0.44–1.38]; n = 7 | p = 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kronibus, N.; Seiler, F.; Danziger, G.; Muellenbach, R.M.; Reyher, C.; Becker, A.P.; Kamphorst, M.; Rixecker, T.M.; Metz, C.; Bals, R.; et al. Respiratory Physiology of COVID-19 and Influenza Associated Acute Respiratory Distress Syndrome. J. Clin. Med. 2022, 11, 6237. https://doi.org/10.3390/jcm11216237
Kronibus N, Seiler F, Danziger G, Muellenbach RM, Reyher C, Becker AP, Kamphorst M, Rixecker TM, Metz C, Bals R, et al. Respiratory Physiology of COVID-19 and Influenza Associated Acute Respiratory Distress Syndrome. Journal of Clinical Medicine. 2022; 11(21):6237. https://doi.org/10.3390/jcm11216237
Chicago/Turabian StyleKronibus, Niklas, Frederik Seiler, Guy Danziger, Ralf M. Muellenbach, Christian Reyher, André P. Becker, Maren Kamphorst, Torben M. Rixecker, Carlos Metz, Robert Bals, and et al. 2022. "Respiratory Physiology of COVID-19 and Influenza Associated Acute Respiratory Distress Syndrome" Journal of Clinical Medicine 11, no. 21: 6237. https://doi.org/10.3390/jcm11216237
APA StyleKronibus, N., Seiler, F., Danziger, G., Muellenbach, R. M., Reyher, C., Becker, A. P., Kamphorst, M., Rixecker, T. M., Metz, C., Bals, R., Lepper, P. M., & Mang, S. (2022). Respiratory Physiology of COVID-19 and Influenza Associated Acute Respiratory Distress Syndrome. Journal of Clinical Medicine, 11(21), 6237. https://doi.org/10.3390/jcm11216237