
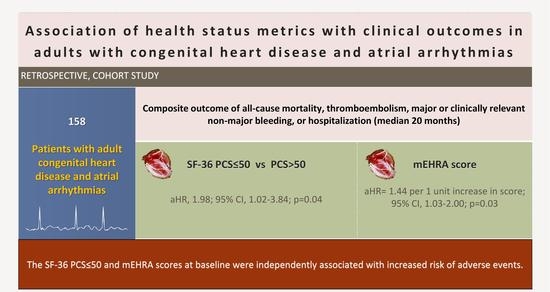
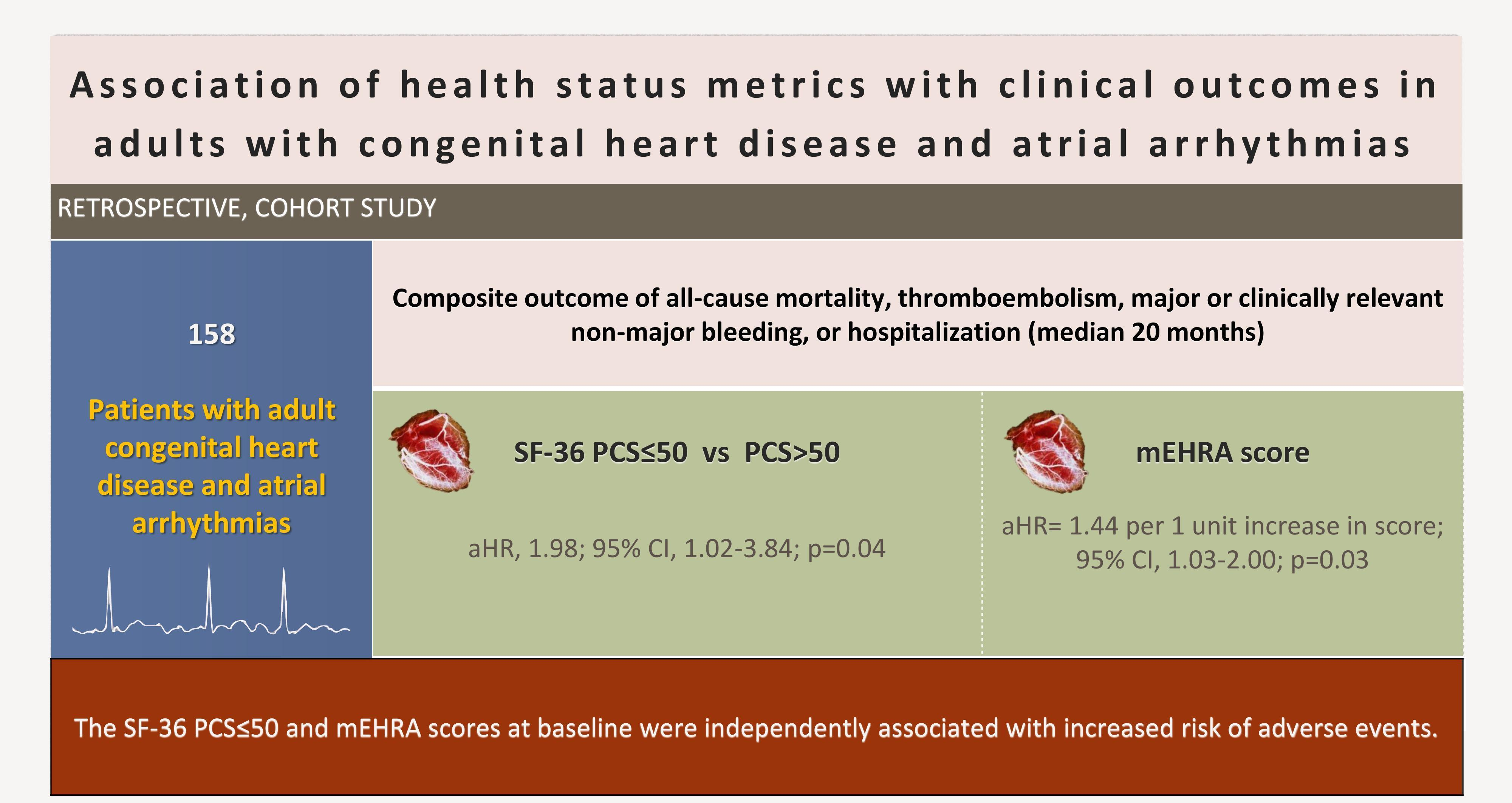
Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias
 , , ,
, , ,  , , ,
, , ,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Outcomes
2.4. Data Sources and Measures
2.5. Statistical Analysis
3. Results
3.1. Study Population
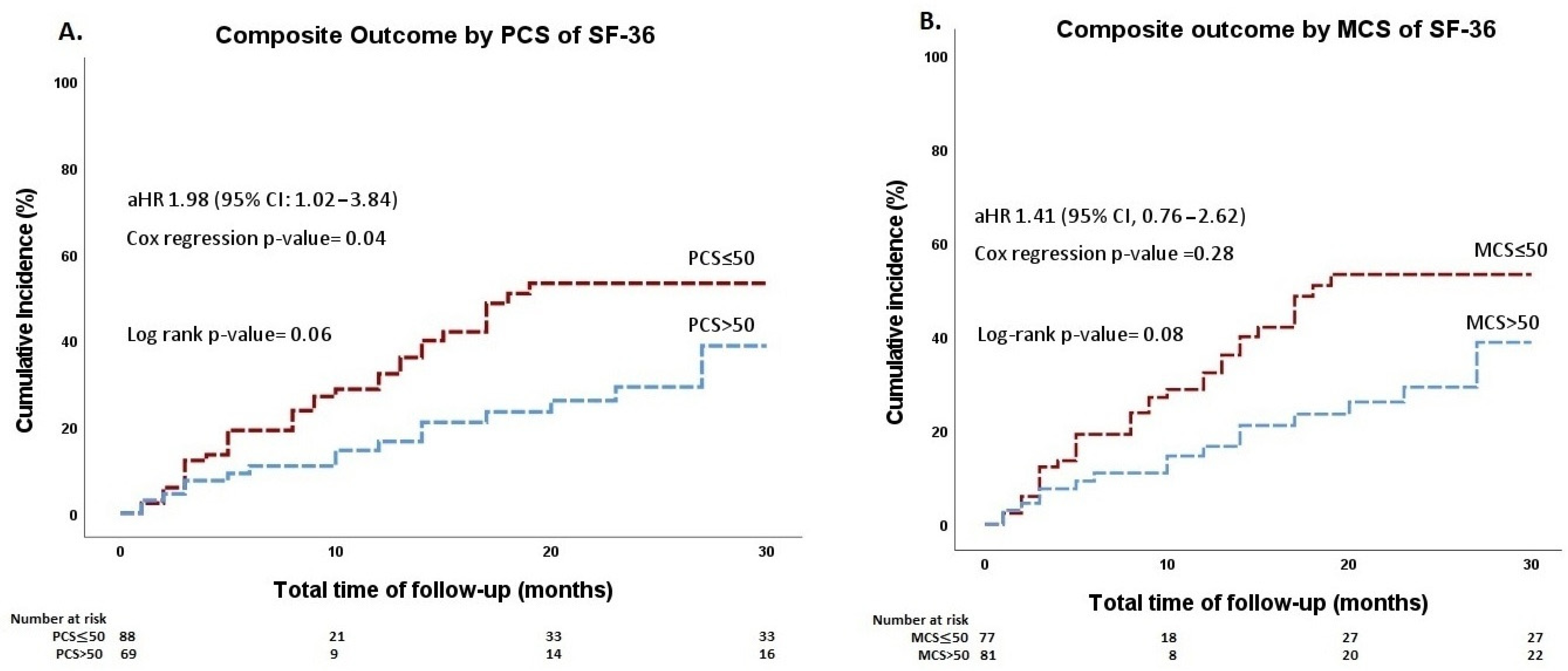
3.2. Prognostic Significance of SF-36 PCS and MCS
3.3. Prognostic Significance of mEHRA Score
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kempny, A.; Dimopoulos, K.; Uebing, A.; Moceri, P.; Swan, L.; Gatzoulis, M.A.; Diller, G.P. Reference values for exercise limitations among adults with congenital heart disease. Relation to activities of daily lifesingle centre experience and review of published data. Eur. Heart J. 2012, 33, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Ntiloudi, D.; Giannakoulas, G.; Parcharidou, D.; Panagiotidis, T.; Gatzoulis, M.A.; Karvounis, H. Adult congenital heart disease: A paradigm of epidemiological change. Int. J. Cardiol. 2016, 218, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Koyak, Z.; Achterbergh, R.C.A.; De Groot, J.R.; Berger, F.; Koolbergen, D.R.; Bouma, B.J.; Lagrand, W.K.; Hazekamp, M.G.; Blom, N.A.; Mulder, B.J.M. Postoperative arrhythmias in adults with congenital heart disease: Incidence and risk factors. Int. J. Cardiol. 2013, 169, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Negishi, J.; Ohuchi, H.; Yasuda, K.; Miyazaki, A.; Norifumi, N.; Yamada, O. Unscheduled hospitalization in adults with congenital heart disease. Korean Circ. J. 2015, 45, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Madrid, A.; Paul, T.; Abrams, D.; Aziz, P.F.; Blom, N.A.; Chen, J.; Chessa, M.; Combes, N.; Dagres, N.; Diller, G.; et al. Arrhythmias in congenital heart disease: A position paper of the European Heart Rhythm Association (EHRA), Association for European Paediatric and Congenital Cardiology (AEPC), and the European Society of Cardiology (ESC) Working Group on Grown-up Congeni. Europace 2018, 20, 1719–1720. [Google Scholar] [CrossRef]
- Kartas, A.; Papazoglou, A.S.; Kosmidis, D.; Moysidis, D.V.; Baroutidou, A.; Doundoulakis, I.; Despotopoulos, S.; Vrana, E.; Koutsakis, A.; Rampidis, G.P.; et al. The Adult Congenital Heart Disease Anatomic and Physiological Classification: Associations with Clinical Outcomes in Patients with Atrial Arrhythmias. Diagnostics 2022, 12, 466. [Google Scholar] [CrossRef]
- Anker, S.D.; Agewall, S.; Borggrefe, M.; Calvert, M.; Caro, J.J.; Cowie, M.R.; Ford, I.; Paty, J.A.; Riley, J.P.; Swedberg, K.; et al. The importance of patient-reported outcomes: A call for their comprehensive integration in cardiovascular clinical trials. Eur. Heart J. 2014, 35, 2001–2009. [Google Scholar] [CrossRef]
- Casteigt, B.; Samuel, M.; Laplante, L.; Shohoudi, A.; Apers, S.; Kovacs, A.H.; Luyckx, K.; Thomet, C.; Budts, W.; Enomoto, J.; et al. Atrial arrhythmias and patient-reported outcomes in adults with congenital heart disease: An international study. Heart Rhythm 2021, 18, 793–800. [Google Scholar] [CrossRef]
- Yang, H.; Kuijpers, J.M.; de Groot, J.R.; Konings, T.C.; van Dijk, A.; Sieswerda, G.T.; Post, M.C.; Mulder, B.J.M.; Bouma, B.J. Impact of atrial arrhythmias on outcome in adults with congenital heart disease. Int. J. Cardiol. 2017, 248, 152–154. [Google Scholar] [CrossRef]
- Egbe, A.C.; Najam, M.; Banala, K.; Vojjini, R.; Bonnichsen, C.; Ammash, N.M.; Faizee, F.; Khalil, F.; Deshmukh, A.J.; Connolly, H.M. Impact of atrial arrhythmia on survival in adults with tetralogy of Fallot. Am. Heart J. 2019, 218, 1–7. [Google Scholar] [CrossRef]
- Kartas, A.; Doundoulakis, I.; Ntiloudi, D.; Koutsakis, A.; Kosmidis, D.; Rampidis, G.; Apostolopoulou, S.; Frogoudaki, A.; Tzifa, A.; Avramidis, D.; et al. Rationale and design of a prospective, observational, multicentre study on the safety and efficacy of apixaban for the prevention of thromboembolism in adults with congenital heart disease and atrial arrhythmias: The PROTECT-AR study. BMJ Open 2020, 10, e038012. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.; Ware, J.; Raczek, A. The MOS 36-item short-form health survey (SF-36): II. Psychometric. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Farivar, S.S.; Cunningham, W.E.; Hays, R.D. Correlated physical and mental health summary scores for the SF-36 and SF-12 Health Survey, V.1. Health Qual. Life Outcomes 2007, 5, 54. [Google Scholar] [CrossRef] [PubMed]
- Wynn, G.J.; Todd, D.M.; Webber, M.; Bonnett, L.; McShane, J.; Kirchhof, P.; Gupta, D. The European Heart Rhythm Association symptom classification for atrial fibrillation: Validation and improvement through a simple modification. Europace 2014, 16, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Dawood, Z.S.; Janjua, M.; Chauhan, S.S.B.; Ladak, L.A. Health-related quality of life in adults with tetralogy of Fallot repair: A systematic review and meta-analysis. Qual. Life Res. 2021, 30, 2715–2725. [Google Scholar] [CrossRef]
- Marshall, K.H.; D’Udekem, Y.; Sholler, G.F.; Opotowsky, A.R.; Costa, D.S.J.; Sharpe, L.; Celermajer, D.S.; Winlaw, D.S.; Newburger, J.W.; Kasparian, N.A. Health-Related Quality of Life in Children, Adolescents, and Adults with a Fontan Circulation: A Meta-Analysis. J. Am. Heart Assoc. 2020, 9, e014172. [Google Scholar] [CrossRef]
- Lane, D.A.; Lip, G.Y.H.; Millane, T.A. Quality of life in adults with congenital heart disease. Heart 2002, 88, 71–75. [Google Scholar] [CrossRef]
- Kamphuis, M.; Ottenkamp, J.; Vliegen, H.W.; Vogels, T.; Zwinderman, K.H.; Kamphuis, R.P.; Verloove-Vanhorick, S.P. Health related quality of life and health status in adult survivors with previously operated complex congenital heart disease. Heart 2002, 87, 356–362. [Google Scholar] [CrossRef]
- Soufi, A.; Gouton, M.; Metton, O.; Mitchell, J.; Bernard, Y.F.; Bozio, A.; Ninet, J.; Di Filippo, S. Quality of life of adult Fontan patients. Cardiol. Young 2021, 31, 97–104. [Google Scholar] [CrossRef]
- Gratz, A.; Hess, J.; Hager, A. Self-estimated physical functioning poorly predicts actual exercise capacity in adolescents and adults with congenital heart disease. Eur. Heart J. 2009, 30, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Müller, J.; Hess, J.; Hager, A. Minor symptoms of depression in patients with congenital heart disease have a larger impact on quality of life than limited exercise capacity. Int. J. Cardiol. 2012, 154, 265–269. [Google Scholar] [CrossRef]
- Pravda, N.S.; Zusman, O.; Richter, I.; Blieden, L.; Vig, S.; Marchushamer, I.; Dadashev, A.; Razon, Y.; Kornowski, R.; Hirsch, R. Self-Reported Mental and Physical Measures in Adult Fontan Patients. J. Clin. Med. 2022, 11, 3969. [Google Scholar] [CrossRef] [PubMed]
- Müller, J.; Berner, A.; Ewert, P.; Hager, A. Reduced health-related quality of life in older patients with congenital heart disease: A cross sectional study in 2360 patients. Int. J. Cardiol. 2014, 175, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Van Den Bosch, A.E.; Roos-Hesselink, J.W.; Van Domburg, R.; Bogers, A.J.J.C.; Simoons, M.L.; Meijboom, F.J. Long-term outcome and quality of life in adult patients after the Fontan operation. Am. J. Cardiol. 2004, 93, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Schron, E.; Friedmann, E.; Thomas, S.A. Does health-related quality of life predict hospitalization or mortality in patients with atrial fibrillation? J. Cardiovasc. Electrophysiol. 2014, 25, 23–28. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the Europe. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Pecen, L.; Rzayeva, N.; Lucerna, M.; Purmah, Y.; Ojeda, F.M.; Caterina, R.; Kirchhof, P. Symptom Burden of Atrial Fibrillation and Its Relation to Interventions and Outcome in Europe. J. Am. Heart Assoc. 2021, 7, e007559. [Google Scholar] [CrossRef]
- Rienstra, M.; Vermond, R.A.; Crijns, H.J.G.M.; Tijssen, J.G.P.; Van Gelder, I.C.; RACE Investigators. Asymptomatic persistent atrial fibrillation and outcome: Results of the RACE study. Heart Rhythm 2014, 11, 939–945. [Google Scholar] [CrossRef]
- Vermond, R.A.; Crijns, H.J.G.M.; Tijssen, J.G.P.; Alings, A.M.; Van Den Berg, M.P.; Hillege, H.L.; Van Veldhuisen, D.J.; Van Gelder, I.C.; Rienstra, M.; Ii, R. Symptom severity is associated with cardiovascular outcome in patients with permanent atrial fibrillation in the RACE II study. Europace 2014, 16, 1417–1425. [Google Scholar] [CrossRef]
- Flaker, G.C.; Belew, K.; Beckman, K.; Vidaillet, H. Asymptomatic atrial fibrillation: Demographic features and prognostic information from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am. Heart J. 2005, 149, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Laroche, C.; Diemberger, I.; Fantecchi, E.; Popescu, M.I.; Rasmussen, L.H.; Sinagra, G.; Petrescu, L.; Tavazzi, L.; Maggioni, A.P.; et al. Asymptomatic atrial fibrillation: Clinical correlates, management and outcomes in the EORP-AF Pilot General Registry. Am. J. Med. 2015, 128, 509–518.e2. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Stroke | Determined as a new-onset neurological deficit provoked by central nervous system injury due to haemorrhage or infarction (symptoms lasting at least 24 h or clear matching CT or MRI lesion for symptoms lasting <24 h), excluding any other nonvascular cause. Strokes will be categorized as “ischemic“, “primary hemorrhagic”, or “undetermined cause” if there are no available imaging data, according to the following definitions. Ischemic stroke
|
| Systemic embolism | Acute blood stoppage in a peripheral artery or embolism from other causes (e.g., surgical specimens, angiography, vascular imaging), localized in the lower or upper limb, intraocular, intra-abdominal viscera or elsewhere. |
| Pulmonary embolism | PE symptoms accompanied by one of the following:
|
| Intracardiac thrombus | Determined as a distinguished echo-dense mass in one of the cardiac chambers that is discovered by echocardiography or cardiac MRI, has well-demarcated borders, and is present both in systole and diastole. |
| Major bleeding (isth) | Determined as apparent bleeding accompanied by:
|
| Clinically relevant non-major bleeding | Determined as overt bleeding not satisfying the aforementioned criteria for major bleeding requiring intervention:
|
| Minor bleeding | Determined as other overt bleeding not satisfying the criteria of a major bleeding event or a clinically relevant non-major bleeding event. |
| Transient ischemic attack | Determined as new neurologic symptoms or deficit of <24 h in the absence of acute infarction on CT or MRI. |
| Myocardial infarction (4th universal definition) | A rise and/or fall of cardiac Troponin levels (≥1 value above the 99th percentile URL) and accompanied by at least one of the above:
|
| Death | The cause of death will be classified as follows: Cardiovascular
|
| Overall n = 158 | PCS ≤ 50 n = 89 | PCS > 50 n = 69 | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years), mean ± SD | 52 ± 17 | 52 ± 17 | 51 ± 17 | 0.62 |
| Female sex | 85 (54%) | 49 (55%) | 36 (53%) | 0.92 |
| BMI, (kg/m2), median (IQR) | 26.2 (5.7) | 26.4 (7.2) | 25.9 (4.9) | 0.32 |
| Systolic blood pressure (mmHg), median (IQR) | 120 (16) | 120 (20) | 115 (10) | 0.07 |
| Diastolic Blood pressure (mmHg), median (IQR) | 70 (15) | 70 (15) | 70 (11) | 0.56 |
| Smoking | 11 (8.0%) | 4 (4.9%) | 7 (13%) | 0.12 |
| Atrial arrhythmia | 1 | |||
| Atrial fibrillation | 101 (77%) | 61 (77%) | 40 (77%) | |
| Atrial flutter | 20 (15%) | 12 (15%) | 8 (15%) | |
| Intra-atrial reentry tachycardia | 10 (7.6%) | 6 (7.6%) | 4 (7.7%) | |
| Pattern of arrhythmia | 0.4 | |||
| First diagnosed | 10 (7.9%) | 5 (6.6%) | 5 (10%) | |
| Paroxysmal | 73 (58%) | 43 (57%) | 30 (60%) | |
| Persistent | 7 (5.6%) | 3 (3.9%) | 4 (8.0%) | |
| Permanent | 36 (29%) | 25 (33%) | 11(22%) | |
| Medical history | ||||
| Major bleeding | 5 (3.6%) | 2 (2.4%) | 3 (5.5%) | 0.38 |
| Clinically relevant non-major bleeding | 19 (14%) | 14 (17%) | 5 (9.1%) | 0.30 |
| Minor bleeding | 41 (31%) | 29 (36%) | 12 (23%) | 0.13 |
| Thromboembolism | 3 (2.2%) | 2 (2.5%) | 1 (1.8%) | 1 |
| Dyslipidemia | 26 (19%) | 17 (21%) | 9 (16%) | 0.51 |
| Hypertension | 40 (29%) | 26 (32%) | 14 (25%) | 0.48 |
| Diabetes | 22 (16%) | 14 (17%) | 8 (15%) | 0.92 |
| Heart failure | 74 (54%) | 48 (59%) | 26 (46%) | 0.14 |
| Chronic kidney disease | 9 (6.5%) | 6 (7.1%) | 3 (5.6%) | 1 |
| NT-proBNP (pg/mL), median (IQR) | 756 (1611) | 725 (1585) | 924 (1020) | 0.34 |
| NYHA functional class | <0.001 | |||
| 1 | 44 (33%) | 15 (18%) | 29 (59%) | |
| 2 | 59 (45%) | 44 (53%) | 15 (31%) | |
| 3 | 26 (20%) | 21 (25%) | 5 (10%) | |
| 4 | 3 (2.3%) | 3 (3.6%) | 0 (0%) | |
| Stroke–bleeding risk | ||||
| CHA2DS2-VASc score, median (IQR) | 2 (1) | 2 (2) | 1 (1) | 0.07 |
| HAS-BLED score, median (IQR) | 1 (1.75) | 1 (2) | 1 (1) | 0.07 |
| Echocardiography | ||||
| Systemic ventricular fraction (%), median (IQR) | 53 (8) | 50 (8) | 55 (12) | 0.07 |
| LA diameter (cm), median (IQR) | 4.45 (1.15) | 4.50 (0.77) | 4.30 (1.20) | 0.15 |
| Electrocardiogram | ||||
| QRS, median (IQR) | 110 (25) | 109 (30) | 116 (22) | 0.34 |
| Health status metrics | ||||
| mEHRA score, mean ± SD | 1.24 ± 1.07 | 1.33 ± 1.13 | 1.10 ± 0.98 | 0.20 |
| Medication | ||||
| Class I antiarrhythmic | 10 (6.3%) | 4 (4.5%) | 6 (8.7%) | 0.3 |
| Class III antiarrhythmic | 41 (26%) | 23 (26%) | 18 (26%) | 1 |
| beta-blocker | 82 (60%) | 52 (65%) | 30 (54%) | 0.2 |
| Overall N = 158 | MCS ≤ 50 N = 89 | MCS > 50 N = 69 | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years), mean ± SD | 52 (17) | 52 (17) | 51 (17) | 0.77 |
| Female sex | 85 (54%) | 39 (51%) | 46 (57%) | 0.48 |
| BMI, (kg/m2), median (IQR) | 26.2 (5.7) | 26.6 (5.7) | 26.0 (5.1) | 0.49 |
| Systolic blood pressure (mmHg), median (IQR) | 120 (16) | 120 (20) | 120 (14) | 0.30 |
| Diastolic Blood pressure (mmHg), median (IQR) | 70 (15) | 70 (15) | 70 (14) | 0.88 |
| Smoking | 11 (8.0%) | 5 (7.1%) | 6 (9.0%) | |
| Atrial arrhythmia | 0.37 | |||
| Atrial fibrillation | 101 (77%) | 53 (82%) | 48 (73%) | |
| Atrial flutter | 20 (15%) | 7 (11%) | 13 (20%) | |
| Intra-atrial reentry tachycardia | 10 (7.6%) | 5 (7.7%) | 5 (7.6%) | |
| Pattern of arrhythmia | 0.28 | |||
| First diagnosed | 10 (7.9%) | 4 (6.6%) | 6 (9.2%) | |
| Paroxysmal | 73 (58%) | 43 (57%) | 30 (60%) | |
| Persistent | 7 (5.6%) | 3 (3.9%) | 4 (8.0%) | |
| Permanent | 36 (29%) | 25 (33%) | 11 (22%) | |
| Medical history | ||||
| Major bleeding | 5 (3.6%) | 1 (1.4%) | 4 (5.8%) | 0.21 |
| Clinically relevant non-major bleeding | 19 (14%) | 8 (12%) | 11 (16%) | 0.62 |
| Minor bleeding | 41 (31%) | 24 (35%) | 17 (26%) | 0.34 |
| Thromboembolism | 3 (2.2%) | 2 (3.0%) | 1 (1.4%) | 0.62 |
| Dyslipidemia | 26 (19%) | 13 (19%) | 13 (19%) | 1 |
| Hypertension | 40 (29%) | 24 (35%) | 16 (24%) | 0.15 |
| Diabetes | 22 (16%) | 13 (18%) | 9 (13%) | 0.56 |
| Heart failure | 74 (54%) | 43 (61%) | 31 (46%) | 0.08 |
| Chronic kidney disease | 9 (6.5%) | 7 (9.9%) | 2 (3.0%) | 0.17 |
| NT-proBNP (pg/mL), median (IQR) | 756 (1611) | 642 (1131) | 782 (1756) | 0.61 |
| NYHA functional class | 0.16 | |||
| 1 | 44 (33%) | 18 (25%) | 26 (43%) | |
| 2 | 59 (45%) | 34 (48%) | 25 (41%) | |
| 3 | 26 (20%) | 17 (24%) | 9 (15%) | |
| 4 | 3 (2.3%) | 2 (2.8%) | 1 (1.6%) | |
| Stroke–bleeding risk | ||||
| CHA2DS2-VASc score, median (IQR) | 2 (1) | 2 (2) | 1 (1) | 0.04 |
| HAS-BLED score, median (IQR) | 1 (1.75) | 1 (2) | 1 (1) | 0.31 |
| Echocardiography | ||||
| Systemic ventricular fraction (%), median (IQR) | 53 (8) | 54 (8) | 53 (7) | 0.78 |
| LA diameter (cm), median (IQR) | 4.45 (1.15) | 4.55 (1.20) | 4.30 (1.00) | 0.31 |
| Electrocardiogram | ||||
| QRS, Median (IQR) | 110 (25) | 114 (32) | 110 (20) | 0.79 |
| Health status metrics | ||||
| mEHRA score, mean ± SD | 1.24 ± 1.07 | 1.41 ± 1.47 | 1.06 ± 0.97 | 0.05 |
| Medication | ||||
| Class I antiarrhythmic | 10 (6.3%) | 4 (5.2%) | 6 (7.4%) | 0.75 |
| Class III antiarrhythmic | 41 (26%) | 20 (26%) | 21 (26%) | 1 |
| beta-blocker | 82 (60%) | 41 (59%) | 41 (61%) | 0.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baroutidou, A.; Kartas, A.; Papazoglou, A.S.; Kosmidis, D.; Moysidis, D.V.; Otountzidis, N.; Doundoulakis, I.; Despotopoulos, S.; Vrana, E.; Koutsakis, A.; et al. Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias. J. Clin. Med. 2022, 11, 6181. https://doi.org/10.3390/jcm11206181
Baroutidou A, Kartas A, Papazoglou AS, Kosmidis D, Moysidis DV, Otountzidis N, Doundoulakis I, Despotopoulos S, Vrana E, Koutsakis A, et al. Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias. Journal of Clinical Medicine. 2022; 11(20):6181. https://doi.org/10.3390/jcm11206181
Chicago/Turabian StyleBaroutidou, Amalia, Anastasios Kartas, Andreas S. Papazoglou, Diamantis Kosmidis, Dimitrios V. Moysidis, Nikolaos Otountzidis, Ioannis Doundoulakis, Stefanos Despotopoulos, Elena Vrana, Athanasios Koutsakis, and et al. 2022. "Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias" Journal of Clinical Medicine 11, no. 20: 6181. https://doi.org/10.3390/jcm11206181
APA StyleBaroutidou, A., Kartas, A., Papazoglou, A. S., Kosmidis, D., Moysidis, D. V., Otountzidis, N., Doundoulakis, I., Despotopoulos, S., Vrana, E., Koutsakis, A., Rampidis, G. P., Ntiloudi, D., Liori, S., Avramidis, D., Karagiannidis, E., Nikolopoulos, T. T., Apostolopoulou, S., Frogoudaki, A., Tzifa, A., ... Giannakoulas, G. (2022). Association of Health Status Metrics with Clinical Outcomes in Patients with Adult Congenital Heart Disease and Atrial Arrhythmias. Journal of Clinical Medicine, 11(20), 6181. https://doi.org/10.3390/jcm11206181