

Visualization of Peripheral Blood Vessels on the Lingual Aspect of the Mandible Using a Balanced Steady-State Free-Precession Sequence with a Time–Spatial Labeling Inversion Pulse: Usefulness for Prevention of Severe Complications of Dental Implantation

Abstract
1. Introduction
2. Subjects and Methods
2.1. Study Subjects
2.2. Image Analysis
2.3. Statistical Analysis
3. Results
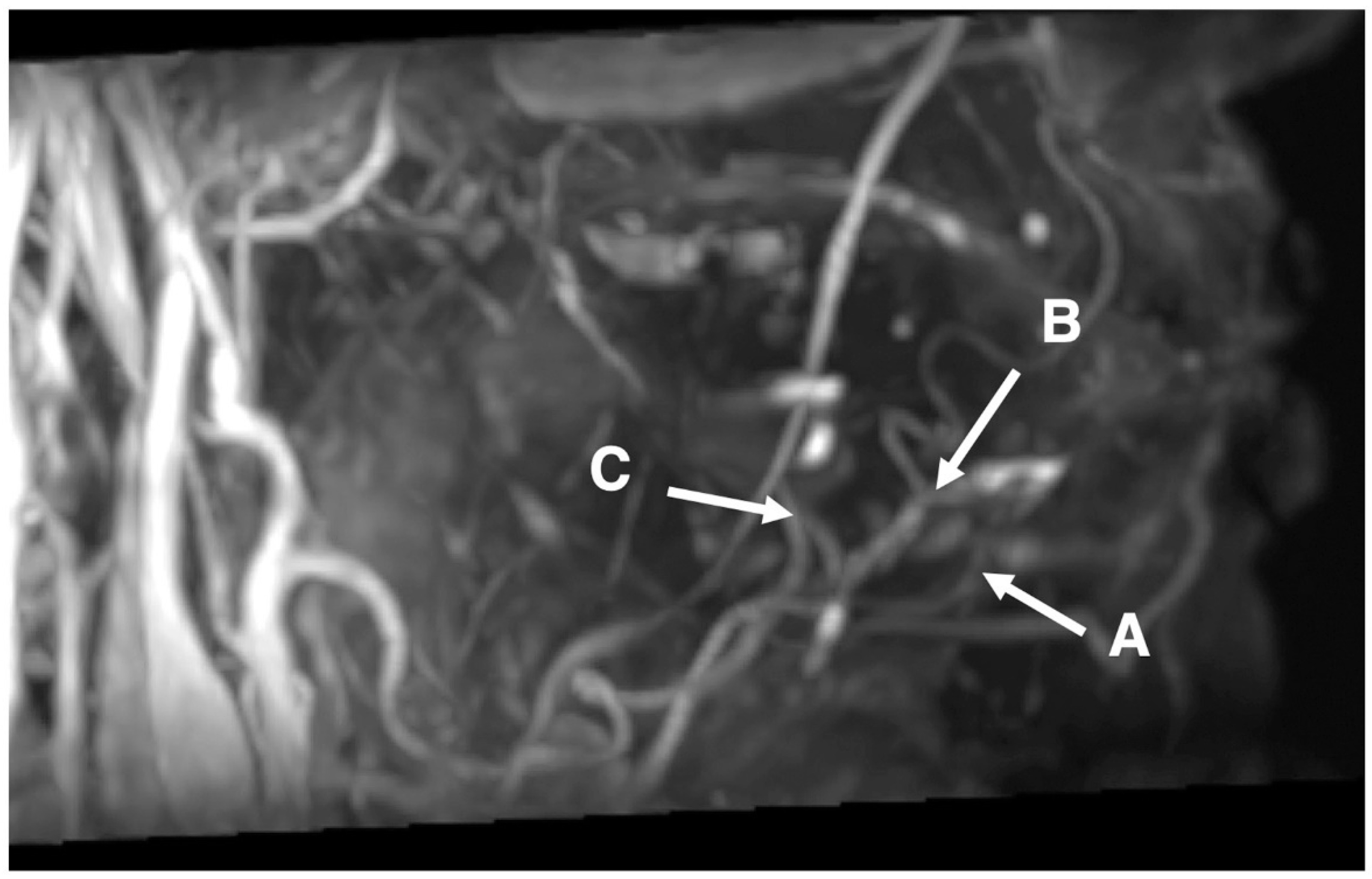
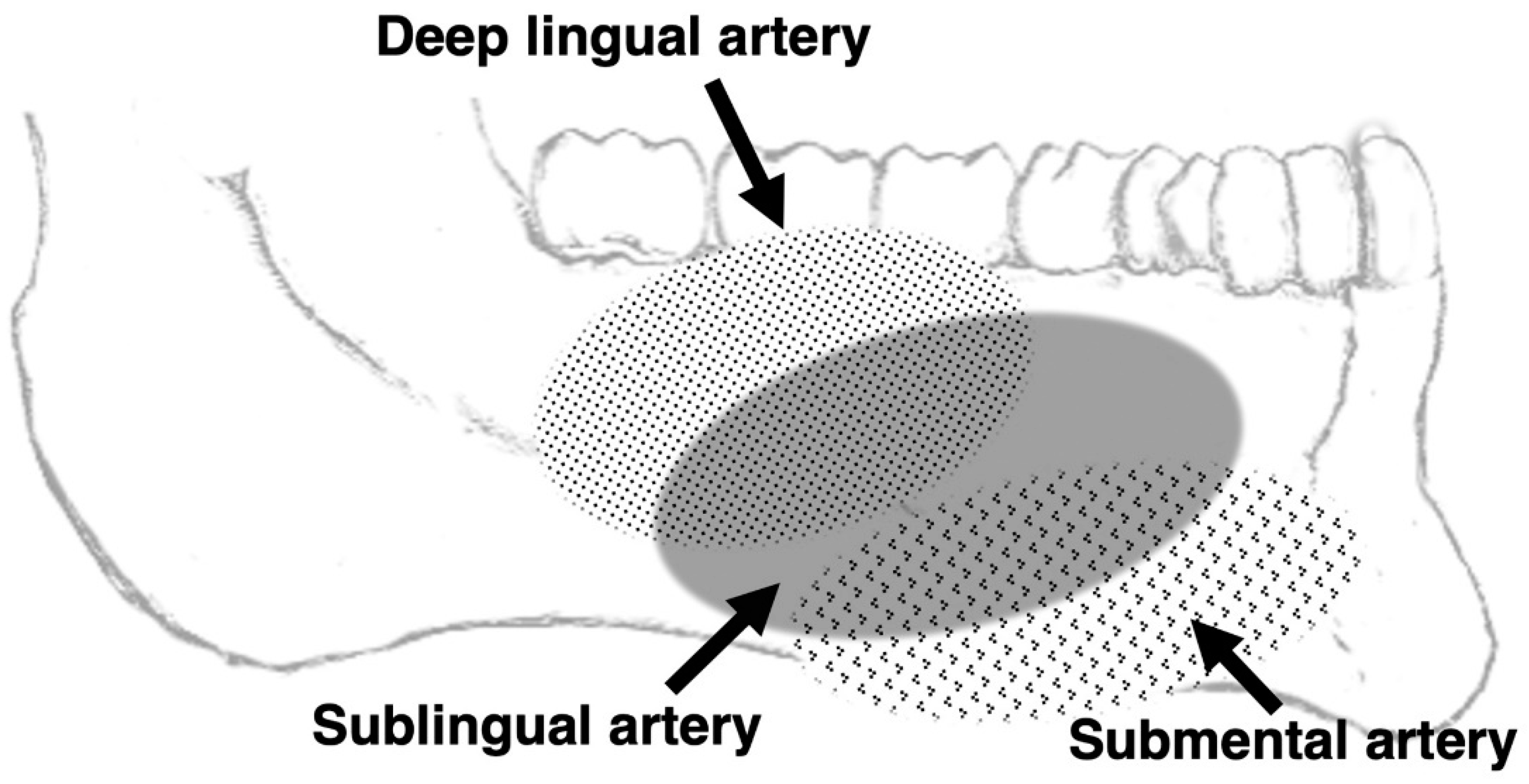
3.1. Conspicuity in the Visualization of the Branches of Lingual and Facial Arteries around the Lingual Sides of Mandibles Using SSFP with a Time–SLIP
3.2. Detectable Rate and Major Axis in the Visualization of the Branches of Lingual and Facial Arteries around the Lingual Sides of Mandibles Using SSFP with a Time–SLIP
3.3. Characteristics of Branches of Lingual and Facial Arteries Using SSFP with a Time–SLIP
4. Discussion
4.1. Applicability to Preoperative Consultation for Dental Implants
4.2. Efficacy of MRA Technique Using SSFP with a Time–SLIP
4.3. Limitations of MRA Technique Using SSFP with a Time–SLIP
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- French, D.; Grandin, H.M.; Ofec, R. Retrospective cohort study of 4591 dental implants: Analysis of risk indicators for bone loss and prevalence of peri-implant mucositis and peri-implantitis. J. Periodontol. 2019, 90, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Olmedo-Gaya, M.V.; Manzano-Moreno, F.J.; Cañaveral-Cavero, E.; de Dios Luna-del Castillo, J.; Vallecillo-Capilla, M. Risk factors associated with early implant failure: A 5-year retrospective clinical study. J. Prosthet Dent. 2016, 115, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Sergio, B.L.; Esperanza, L.G.D.; José, M.B.; Josep, B.T.; Carles, M.F.; Coro, B.A.; Javier, M.B.; Josep, A.M. Twenty four years of oral and maxillofacial surgery malpractice claims in Spain: Patient safety lessons to learn. Oral Maxillofac. Surg. 2019, 23, 187–192. [Google Scholar]
- Corte-Real, A.; Caetano, C.; Alves, S.; Pereira, A.D.; Rocha, S.; Nuno Vieira, D. Patient Safety in Dental Practice: Lessons to Learn About the Risks and Limits of Professional Liability. Int. Dent. J. 2021, 71, 378–383. [Google Scholar] [CrossRef]
- de Souza, J.G.; Schuldt, F.G.; Pereira, N.A.R.; Lyra, H.F., Jr.; Bianchini, M.A.; Cardoso, A.C. Accident in implant dentistry: Involuntary screwdriver ingestion during surgical procedure. A clinical report. J. Prosthodont. 2012, 21, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Eric, W.B.; Johanna, W. Atlas of Oral and Maxillofacial Anatomy; Iwanaga, J., Tubbs, R.S., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Michael, S.; Erik, S.; Udo, S. THIEME Atlas of Anatomy: Head, Neck, and Neuroanatomy; Thieme Medical Publishers: Leipzig, Germany, 2020. [Google Scholar]
- Oda, M.; Tanaka, T.; Kito, S.; Habu, M.; Kodama, M.; Kokuryo, S.; Miyamoto, I.; Yoshiga, D.; Yamauchi, K.; Nogami, S.; et al. Magnetic Resonance Angiography Using Fresh Blood Imaging in Oral and Maxillofacial Regions. Int. J. Dent. 2012, 2012, 865369. [Google Scholar] [CrossRef] [PubMed]
- Urata, J.; Miyazaki, M.; Wada, H.; Nakaura, T.; Yamashita, Y.; Takahashi, M. Clinical evaluation of aortic diseases using nonenhanced MRA with ECG-triggered 3D half-Fourier FSE. J. Magn. Reson. Imaging 2001, 14, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Shonai, T.; Takahashi, T.; Ikeguchi, H.; Miyazaki, M.; Amano, K.; Yui, M. Improved arterial visibility using short-tau inversionrecovery (STIR) fat suppression in non-contrast-enhanced time-spatial labeling inversion pulse (Time-SLIP) renal MR angiography. J. Magn. Reson. Imaging 2009, 29, 1471–1477. [Google Scholar] [CrossRef]
- Satogami, N.; Okada, T.; Koyama, T.; Gotoh, K.; Kamae, T.; Togashi, K. Visualization of external carotid artery and its branches: Noncontrast-enhanced MR angiography using balanced steady-state free-precession sequence and a time-spatial labeling inversion pulse. J. Magn. Reson. Imaging. 2009, 30, 678–683. [Google Scholar] [CrossRef][Green Version]
- Tanaka, T.; Oda, M.; Kito, S.; Wakasugi-Sato, N.; Matsumoto-Takeda, S.; Otsuka, K.; Yoshioka, I.; Habu, M.; Kokuryo, S.; Kodama, M.; et al. Noninvasive identification of peripheral vessels of oral and maxillofacial regions using electrocardiography-triggered three-dimensional fast asymmetric spin-echo sequences. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Oda, M.; Tanaka, T.; Kito, S.; Matsumoto-Takeda, S.; Otsuka, K.; Hayashi, Y.; Wakasugi-Sato, N.; Yoshioka, I.; Habu, M.; Kokuryo, S.; et al. Magnetic resonance angiography with fresh blood imaging for identification of hemangiomas and blood vessels around hemangiomas in oral andmaxillofacial regions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Sumi, T.; Sumi, M.; van Cauteren, M.; Kimura, Y.; Nakamura, T. Parallel imaging technique for the external carotid artery and its branches: Comparison of balanced turbo field echo, phase contrast, and time-of-flight sequences. J. Magn. Reson. Imaging. 2007, 25, 1028–1034. [Google Scholar] [CrossRef]
- van den Berg, R.; Wasser, M.N.; van Glis, A.P.; van den Mey, A.G.; Hermans, J.; van Buchem, M.A. Vascularization of head and neck paragangliomas: Comparison of three MR angiographic techniques with digital subtraction angiography. Am. J. Neuroradiol. 2000, 21, 162–170. [Google Scholar] [PubMed]
- Tanaka, T.; Morimoto, Y.; Takano, H.; Tominaga, K.; Kito, S.; Okabe, S.; Takahashi, T.; Fukuda, J.; Ohba, T. Three-dimensional identification of hemangiomas and feeding arteries in the head and neck region using combined phase-contrast MR angiography and fast asymmetric spin-echo sequences. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2005, 100, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, A.P.; Jovin, T.G. Vascular imaging of the head and neck. Semin Neurol. 2012, 32, 401–410. [Google Scholar] [PubMed]
- Kami, Y.N.; Chikui, T.; Shiraishi, T.; Inadomi, D.; Nishioka, M.; Yuasa, K.; Yoshiura, K.A. New method for displaying the lingual artery using high-resolution three-dimensional phase-contrast magnetic resonance angiography. Int. J. Oral Maxillofac. Surg. 2013, 42, 1494–1498. [Google Scholar] [CrossRef] [PubMed]
- Garcia, D.M.; Duhamel, G.; Alsop, D.C. Efficiency of inversion pulses for background suppressed arterial spin labeling. Mag. Reson. Med. 2005, 54, 366–372. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sequences | |||
|---|---|---|---|
| SSFP with a Time–SLIP | T1WI | STIR | |
| TR (ms) | 5 | 820 | 4700 |
| TE (ms) | 2.5 | 15 | 75 |
| Flip angle (°) | 120 | 90 | 90 |
| FOV (mm) | 300 × 300 | 250 × 225 | 250 × 225 |
| Section thickness (mm) | 3 | 6 | 6 |
| Intersection gap (mm) | 0 | 1.2 | 1.2 |
| Matrix (pixels) | 256 × 256 | 224 × 320 | 272 × 272 |
| Male (n = 20) | Female (n = 20) | Total (n = 40) | |
|---|---|---|---|
| Submental artery | 1.95 ± 1.19 | 1.65 ± 1.27 | 1.80 ± 1.22 |
| Sublingual artery | 2.20 ± 1.10 | 1.75 ± 1.25 | 1.98 ± 1.19 |
| Deep lingual artery | 2.00 ± 1.17 | 1.65 ± 1.18 | 1.83 ± 1.17 |
| Facial artery | 2.55 ± 0.89 | 2.40 ± 0.88 | 2.48 ± 0.88 |
| Lingual artery | 2.50 ± 0.76 | 2.45 ± 0.76 | 2.48 ± 0.75 |
| Maxillary artery | 2.55 ± 0.69 | 2.35 ± 0.93 | 2.45 ± 0.81 |
| Male (n = 20) | Female (n = 20) | Total (n = 40) | |
|---|---|---|---|
| Submental artery | 9 (45%) | 7 (35%) | 16 (40%) |
| Sublingual artery | 12 (60%) | 8 (40%) | 20 (50%) |
| Deep lingual artery | 10 (50%) | 6 (30%) | 16 (40%) |
| Male (n = 20) | Female (n = 20) | Total (n = 40) | |
|---|---|---|---|
| Submental artery (mm) | 25.2 ± 6.3 | 21.8 ± 6.0 | 23.7 ± 6.3 |
| Sublingual artery (mm) | 26.9 ± 9.0 | 20.6 ± 8.9 | 24.4 ± 9.3 |
| Deep lingual artery (mm) | 16.3 ± 9.7 | 14.3 ± 2.6 | 15.5 ± 7.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, T.; Kawashima, Y.; Oda, M.; Wakasugi-Sato, N.; Matsumoto-Takeda, S.; Nishimura, S.; Morimoto, Y. Visualization of Peripheral Blood Vessels on the Lingual Aspect of the Mandible Using a Balanced Steady-State Free-Precession Sequence with a Time–Spatial Labeling Inversion Pulse: Usefulness for Prevention of Severe Complications of Dental Implantation. J. Clin. Med. 2022, 11, 6137. https://doi.org/10.3390/jcm11206137
Tanaka T, Kawashima Y, Oda M, Wakasugi-Sato N, Matsumoto-Takeda S, Nishimura S, Morimoto Y. Visualization of Peripheral Blood Vessels on the Lingual Aspect of the Mandible Using a Balanced Steady-State Free-Precession Sequence with a Time–Spatial Labeling Inversion Pulse: Usefulness for Prevention of Severe Complications of Dental Implantation. Journal of Clinical Medicine. 2022; 11(20):6137. https://doi.org/10.3390/jcm11206137
Chicago/Turabian StyleTanaka, Tatsurou, Yusuke Kawashima, Masafumi Oda, Nao Wakasugi-Sato, Shinobu Matsumoto-Takeda, Shun Nishimura, and Yasuhiro Morimoto. 2022. "Visualization of Peripheral Blood Vessels on the Lingual Aspect of the Mandible Using a Balanced Steady-State Free-Precession Sequence with a Time–Spatial Labeling Inversion Pulse: Usefulness for Prevention of Severe Complications of Dental Implantation" Journal of Clinical Medicine 11, no. 20: 6137. https://doi.org/10.3390/jcm11206137
APA StyleTanaka, T., Kawashima, Y., Oda, M., Wakasugi-Sato, N., Matsumoto-Takeda, S., Nishimura, S., & Morimoto, Y. (2022). Visualization of Peripheral Blood Vessels on the Lingual Aspect of the Mandible Using a Balanced Steady-State Free-Precession Sequence with a Time–Spatial Labeling Inversion Pulse: Usefulness for Prevention of Severe Complications of Dental Implantation. Journal of Clinical Medicine, 11(20), 6137. https://doi.org/10.3390/jcm11206137